
Abstract
Intracerebral hemorrhage (ICH) represents one of the most devastating forms of stroke, characterized by spontaneous bleeding into the brain parenchyma. This neurological emergency carries a substantial burden of mortality and long-term disability worldwide. A comprehensive understanding of ICH’s evolving global impact from 1990 to 2021 remains essential for healthcare planning and resource allocation. We conducted a systematic analysis of ICH burden utilizing data from the Global Burden of Disease (GBD) Study 2021. Key epidemiological indicators were extracted, including prevalence, incidence, mortality, and disability-adjusted life-years (DALYs). Temporal trends were quantified through estimated annual percentage changes (EAPCs) in age-standardized rates of prevalence (ASPR), incidence (ASIR), mortality (ASDR), and DALYs across the study period. The association between disease burden and socioeconomic development was examined using the sociodemographic index (SDI) as a metric of societal development. This analytical framework enabled assessment of ICH burden across global, regional, and national scales while accounting for demographic and socioeconomic variations. From 1990 to 2021, while absolute ICH cases increased globally, age-standardized incidence rates declined. Our novel geographic analysis revealed East Asia bearing the highest burden, with Eastern Europe showing the highest age-standardized rates. Gender analysis identified distinct age-specific patterns, with males above 35 showing higher risk, particularly in Eastern Europe, while South Asia demonstrated minimal gender differences. Our innovative analysis during COVID-19 revealed healthcare system strength significantly impacted ICH outcomes, with well-resourced countries maintaining better outcomes. Regional risk factor assessment showed varying impacts of high systolic blood pressure across regions, highest in Southern Sub-Saharan Africa and lowest in Oceania. Future projections through 2030 indicate improving survival rates in most regions, except in low-income areas, highlighting persistent healthcare disparities. While the absolute number of ICH cases, deaths, and DALYs increased globally from 1990 to 2021, age-standardized rates showed a decreasing trend. This suggests improvements in prevention and management strategies over time. However, the burden of ICH remains substantial and unevenly distributed across regions, with lower SDI areas facing a disproportionately higher burden. These findings highlight the need for targeted interventions and resource allocation, particularly in regions with higher ICH burden, to further reduce the global impact of this devastating condition.
Similar content being viewed by others


Introduction
Intracerebral hemorrhage (ICH) remains a significant global health challenge, representing a major cause of mortality and disability worldwide. According to the GBD 2021 study, stroke was the third most common cause of death (7.3 million deaths; 10.7% of all deaths) after ischemic heart disease and COVID-19, and the fourth leading cause of DALYs (160.5 million DALYs; 5.6% of all DALYs). In 2021, there were 93.8 million prevalent and 11.9 million incident strokes globally1. Of these, ICH constituted 28.8% of all incident strokes, representing a substantial portion of the overall stroke burden.
While the GBD 2021 study provided comprehensive stroke data, detailed ICH-specific analyses remain limited. Our study extends beyond the GBD 2021 findings in several innovative ways. First, we conduct an in-depth analysis of ICH-specific temporal trends and risk factor patterns across different regions and healthcare systems. Second, we provide the first systematic assessment of how healthcare system resilience affected ICH outcomes during the COVID-19 pandemic, revealing significant disparities in mortality increases between regions with robust versus limited healthcare infrastructure. Third, our gender-stratified analysis identifies previously unreported age-specific patterns, with males above 35 showing higher risk and the gender gap progressively widening with age. Finally, we develop novel regional risk factor attribution patterns, particularly focusing on high systolic blood pressure’s variable impact across regions, ranging from 64% attribution in Southern Sub-Saharan Africa to 45% in Oceania.
Our detailed ICH-specific approach, incorporating stratification by sex, age groups, and socio-demographic index (SDI) quintiles, enables precise identification of vulnerable populations and high-burden regions. This comprehensive analysis, covering the period from 1990 to 2021, includes future projections through 2030 and examines how the COVID-19 pandemic affected ICH care delivery patterns. The findings from this systematic analysis are intended to inform evidence-based health policies and guide the development of targeted prevention strategies and therapeutic interventions.
Methods
Data source
The foundational methodology for estimating stroke burden and associated risk factors in GBD 2021 builds upon previously established GBD protocols, which have been extensively documented in prior publications2,3,4.The GBD study employed sophisticated modeling techniques to estimate the burden of ICH. The DisMod-MR 2.1 (disease-model-Bayesian meta-regression) tool was utilized to calculate incidence and prevalence. This Bayesian geospatial software integrates diverse disease parameters, epidemiological relationships, and geospatial data to generate robust estimates2,3,4. For mortality estimation, the Cause of Death Ensemble modeling (CODEm) framework was applied2,3,4. This method systematically incorporates vital registration and verbal autopsy data, including those with non-specific codes. The data underwent rigorous adjustment processes to ensure accuracy before analysis1. CODEm combines multiple models to estimate death rates with improved precision. These models were applied to the 2021 database, producing comprehensive estimates of ICH burden. The approach accounts for methodological heterogeneity across multiple data sources, ensuring consistent and accurate estimates of ICH incidence, prevalence, and mortality. To calculate the DALYs due to ICH, we summed two components: Years Lived with Disability (YLD), which quantifies the burden of living with the effects of ICH, and Years of Life Lost (YLL), which measures the impact of premature death2,3,4. The detailed methodology for these calculations is provided in the Supplementary Methods section.
The GBD estimation process is based on identifying multiple relevant data sources for each disease or injury, including censuses, household surveys, civil registration and vital statistics, disease registries, health service use, air pollution monitors, satellite imaging, disease notifications, and other sources2,3,4. These data are identified from a systematic review of published studies, searches of government and international organization websites, published reports, primary data sources such as the Demographic and Health Surveys, and datasets contributed by GBD collaborators. For ICH specifically, the analysis incorporated 121 sources reporting prevalence, 355 sources reporting incidence, and 127 sources reporting excess mortality rate. Each newly identified and obtained data source is given a unique identifier by a team of librarians and included in the Global Health Data Exchange (GHDx). The GHDx makes publicly available the metadata for each source included in GBD, as well as the data where allowed by the data provider. The detailed classification and characteristics of these data sources are provided in the Supplementary Methods section.
Sociodemographic index
The SDI serves as a comprehensive metric of societal development, incorporating three fundamental dimensions: total fertility rate, average educational attainment, and per capita income. This composite measure is scaled from 0 to 1, where higher values reflect greater levels of socioeconomic development7,8. Countries and territories were categorized into quintiles based on their 2021 SDI value: low SDI (≤ 0.46), low-middle SDI (0.46–0.54), middle SDI (0.54–0.63), high-middle SDI (0.63–0.74), and high SDI (> 0.74)2,3,4. Previous research has demonstrated robust correlations between SDI values and various health outcomes, including disease occurrence and mortality patterns across different populations. In our analysis, we categorized countries and regions into five distinct SDI quintiles: low, low-medium, medium, medium–high, and high. This stratified approach enabled us to systematically investigate the association between ICH burden and socioeconomic development status, providing insights into how social and economic factors influence disease patterns across different development contexts.
Definition of ICH
In the GBD 2021 study, ICH was defined according to World Health Organization clinical criteria5,6. Specifically, ICH was characterized as a stroke resulting in a focal collection of blood within the brain parenchyma, not attributable to trauma. The corresponding disease codes include ICD-9: 431–432.9, 437.2 and ICD-10: I61-I62, I62.1-I62.9, I68.1-I68.2, I69.1-I69.2. The methodologies employed by the GBD to attribute cause of death to stroke and its subtypes in regions where neuroimaging facilities were unavailable have been extensively documented in previous publications6,7.
Risk factors
In addition to the primary metrics of prevalence, incidence, mortality, and DALYs, this study also examined the impact of specific risk factors on ICH burden. Our analysis included data on ICH-related DALYs and deaths attributable to these factors, with additional stratification by region to elucidate geographical variations in their impact. To quantify the influence of these risk factors, we employed sophisticated methodologies, including DisMod-MR 2.1 and spatiotemporal Gaussian process regression8. These approaches enabled us to model exposure distributions for each risk factor across various demographics and locations. We then established the theoretical minimum risk exposure level (TMREL) for each factor, based on epidemiological evidence, representing the optimal exposure level for minimizing LCH risk9. By integrating exposure data, relative risk estimates, and TMRELs, we calculated population attributable fractions (PAFs) for each risk factor. These PAFs, stratified by location, age, sex, and year, quantify the potential reduction in ischemic stroke burden if exposure to a given risk factor were reduced to its TMREL9. To translate these fractions into meaningful health outcomes, we multiplied the PAFs by DALYs. This calculation provided estimates of the risk-attributable burden, offering valuable insights into how modifying these risk factors could potentially impact ICH outcomes across different populations. This comprehensive approach not only highlights the direct burden of ICH but also illuminates the contribution of modifiable risk factors, providing a more nuanced understanding of the disease’s impact and potential avenues for intervention.
Statistical analyses
To assess the trends in age-standardized rates (ASR) of ICH incidence, mortality, DALYs, and prevalence, the study utilized the Estimated Annual Percentage Change (EAPC). The ASR was computed per 100,000 individuals utilizing the subsequent formula:
(\({a}_{ i}\): the age-specific rate in ith the age group; w: the number of people in the corresponding ith age group among the standard population; A: the number of age groups)
The calculation of EAPCs was based on a regression model that characterizes the pattern of age-standardized rates during a specified period12. The equation employed was: Y = α + βX + e, where Y represents the natural logarithm of the ASR, X indicates the calendar year, α is the intercept term, β denotes the slope or trend, and e is the error term. The EAPC is calculated as 100 × [exp(β)–1], representing the annual percentage change. The linear regression model was used to compute the 95% confidence interval (CI) for the EAPC. An ASR is deemed to have an increasing trend if both the EAPC and the lower bound of its 95% CI are positive. In contrast, if both the EAPC and the upper bound of its 95% CI are negative, the ASR is considered to have a decreasing trend. If neither condition is satisfied, the ASR is regarded as stable. Spearman correlation was used to assess associations between the SDI and the ASR of ICH.
In this study, we utilized a Bayesian age-period-cohort (BAPC) model incorporating integrated nested Laplace approximations to project future trends in ICH burden. Previous research has demonstrated that BAPC offers superior coverage and precision compared to alternative prediction methods10,11,12,13. The computational process was implemented using the R-package BAPC, following established protocols from prior studies13. Additionally, risk factors for ICH were assessed. Statistical analyses and data visualizations were conducted using R software (version 4.2.1; https://www.r-project.org/), a free environment for statistical computing and graphics. Several specialized R packages were employed: BAPC (version 0.0.36) for Bayesian Age-Period-Cohort modeling, INLA (version 24.05.011) for integrated nested Laplace approximations, and ggplot2 (version 3.4.2) for data visualization. Geographic visualizations were created using the rworldmap package (version 1.3.6).
Results
Global level
The global prevalence cases of ICH increased from 11.2 million (95% UI: 10.2–12.3) in 1990 to 16.6 million (95% UI: 15.2–18.2) in 2021 (Table1). However, the age-standardized rates of ICH prevalence (ASPR) per 100,000 population decreased from 250.2 (95% UI: 228.0–275.1) to 194.5 (95% UI: 178.0–212.5) (Fig. 1). The EAPC was -0.97 (95% CI: -1.04 to -0.90), indicating a significant decrease in the ASPR over the study period. With respect to age distribution, the prevalence of ICH is relatively low in both males and females under 30 years of age. However, a notable increase in prevalence is observed in males aged 35 and above. Overall, the data demonstrate a trend of increasing prevalence with advancing age. Across all age groups, males consistently exhibit higher prevalence rates compared to females of the same age (FigS1). The global incidence cases of ICH rose from 2.4 million (95% UI: 2.1–2.6) cases in 1990 to 3.4 million (95% UI: 3.1–3.8) cases in 2021. The ASIR per 100,000 population decreased from 59.5 (95% UI: 51.4–66.6) to 40.8 (95% UI: 36.2–45.2). The EAPC was -1.52 (95% CI: -1.67 to -1.38). On a global scale, the incidence rate of ICH generally increases with age, with a particularly marked elevation observed in individuals aged 65 and above (Fig. 2).

Trends in intracerebral hemorrhage prevalence, incidence, deathes and disability-adjusted life-years from 1990 to 2021.

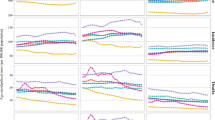
The age-specific numbers and ASIRs of intracerebral hemorrhage by SDI regions in 2021.
Global deaths due to ICH increased from 2.3 million (95% UI: 2.2–2.5) in 1990 to 3.3 million (95% UI: 3.0–3.6) in 2021. The ASR per 100,000 population decreased from 61.6 (95% UI: 57.0–66.1) to 39.1 (95% UI: 35.6–42.5). The EAPC was -1.40 (95% CI: -1.51 to -1.30), indicating a significant reduction in the age-standardized mortality rate (Fig. 1,Table1).
In 1990, the global DALYs attributed to ICH were estimated at 63.2 million (95% UI: 59.2–67.1). The age-standardized DALYs rate per 100,000 population was 1,516.8 (95% UI: 1,421.0–1,613.3). By 2021, the absolute number of DALYs had increased to 79.5 million (95% UI: 72.7–85.5). However, the age-standardized DALYs rate decreased substantially to 923.6 per 100,000 population (95% UI: 844.8–993.2) (Fig. 1,Table1).
Regional level
The global burden of ICH demonstrates marked regional heterogeneity, with patterns closely linked to socioeconomic development status. ASPR exhibit substantial variation across SDI regions. The highest ASPR is observed in Low SDI areas (222 per 100,000 population; 95% UI: 205–242), with Low-middle SDI regions showing comparable rates (220 per 100,000; 95% UI: 200–241). In contrast, High SDI regions report significantly lower rates (154 per 100,000; 95% UI: 142–165) (Table 1, Fig. 1). The most pronounced decrease is observed in High-middle SDI regions (EAPC: -1.37; 95% CI: -1.48 to -1.25), followed by Low SDI regions (EAPC: -1.11; 95% CI: -1.16 to -1.06). ASIR further highlight these regional disparities. Low SDI regions experience the highest incidence (58 per 100,000; 95% UI: 52–63), contrasting sharply with High SDI regions (16 per 100,000; 95% UI: 15–18). Similarly, ASDR show marked variation, with Low SDI regions reporting substantially higher mortality (59 per 100,000; 95% UI: 49–68) compared to High SDI regions (10 per 100,000; 95% UI: 9–11). The burden of disease, measured by age-standardized DALY rates, reflects these disparities most dramatically. Low SDI regions bear nearly six times the burden of High SDI regions, with rates of 1,428 per 100,000 (95% UI: 1,216–1,643) and 243 per 100,000 (95% UI: 227–258), respectively.
Among GBD super-regions, East Asia recorded the highest number of ICH incidence cases (1.2 million; 95% UI: 1.0–1.4) in 2021. The temporal trends in ASDR demonstrated marked regional variations, with Southern Sub-Saharan Africa experiencing an increase (EAPC: 0.94, 95% CI: 0.47–1.42), while High-income Asia Pacific achieved significant reduction (EAPC: -4.76, 95% CI: -4.91 to -4.60). Analysis of age-standardized DALYs rates revealed significant regional disparities, with the highest burden observed in Southeast Asia and Sub-Saharan Africa. All super-regions demonstrated a decline in age-standardized DALYs rates since 1990, with Central Europe showing the most substantial improvement, achieving a reduction of about 64% between 1990 and 2021.
National level
Country-specific analyses revealed substantial variations in ICH burden across nations. The ASPR ranged from 67.1 to 592.5 per 100,000 population, with Pacific Island nations showing particularly high rates. Kiribati demonstrated the highest ASPR (592.5 per 100,000; 95% UI: 560.7–625.1), followed by Solomon Islands (581.6 per 100,000; 95% UI: 548.4–620.7) and Nauru (473.6 per 100,000; 95% UI: 448–502.7) (Fig. 3A, Table S1). Notable temporal changes included the Philippines, which exhibited the most substantial increase in ASPR (EAPC: 1.13, 95% CI: 0.9–1.37). The ASIR demonstrated similar geographical disparities (Fig. 3B, Table S2). Solomon Islands recorded the highest ASIR (198.1 per 100,000; 95% UI: 184.5–211.6), contrasting markedly with Switzerland, which reported the lowest rate (9.9 per 100,000; 95% UI: 8.6–11.2). Mortality patterns, measured by ASDR, showed considerable variation across nations, ranging from 4.3 to 160.7 per 100,000 population in 2021. The highest mortality rates were observed in Solomon Islands (160.7 per 100,000; 95% UI: 129.6–198.9), Montenegro (159.3 per 100,000; 95% UI: 137.3–184.4), and Nauru (147.2 per 100,000; 95% UI: 117.7–183.5) (Fig. 3C, Table S3).While most countries demonstrated declining mortality trends between 1990 and 2021, the magnitude of improvement varied substantially. The most pronounced reductions in ASDR were achieved by the Republic of Korea (EAPC: -7.29, 95% CI: -7.56 to -7.02), Hungary (EAPC: -5.36, 95% CI: -5.62 to -5.1), and Singapore (EAPC: -5.07, 95% CI: -5.24 to -4.91) (Table S3) Conversely, Zimbabwe showed a increase (EAPC 1.94, 95% CI 1.33–2.56). The age-standardized DALYs rates due to ICH varies widely across countries, ranging from approximately 84.5 to 3998.5 per 100,000 people. Among all countries, Nauru (3998.5 per 100,000 persons; 95% UI: 3121.7–5096.9), Solomon Islands (3737.7 per 100,000 persons; 95% UI: 2942.4–4694.8), and Marshall Islands (3450.4 per 100,000 persons; 95% UI: 2651.9–4450.8) exhibit the highest ASR of DALYs for ICH in 2021 (Fig. 3D; Table S4). The most significant decrease in the ASR of DALYs for ICH was observed in Republic of Korea (EAPC -7.08, 95% CI -7.35–6.81) (Table S4).

The global disease burden of intracerebral hemorrhage for both sexes in 204 countries and territories. (A) Prevalence rate. (B) Incidence rate. (C) Death rate. (D) DALYs rate. Maps were generated using R software (version 4.2.1, https://www.r-project.org/) with the ‘rworldmap’ package (version 1.3.6).
Age and sex patterns
The ASPR of ICH in 2021 exhibited an age-dependent increase, culminating in the 95 + age bracket (Fig. 4). While ASPR ratios were comparable between genders at ages 40–44, men consistently showed higher rates than women in subsequent age groups. Concurrently, the ASIR displayed a similar age-related upward trend, peaking among nonagenarians and centenarians. Notably, in the 90 + cohort, females surpassed males in incidence rates (Fig. 2). Comparing 2021 to 1990, the ASDR for ICH decreased across both sexes, yet maintained an age-associated rise. Men generally experienced elevated ASDRs compared to women across most age categories (Supplementary Fig. S6). DALYs also demonstrated a reduction in 2021 relative to 1990, with ASR surpassing that of women in men aged 55 and above (Supplementary Fig. S7).

Age-standardized prevalence rates of intracerebral hemorrhage by sex, age group, and socio-demographic index, 1990 and 2021.
Risk factors for ICH
Analysis of risk factors contributing to ICH burden focused on several major modifiable factors: alcohol use, high body-mass index, high fasting plasma glucose, high systolic blood pressure, and smoking (Supplementary Fig. S8, TableS5). High systolic blood pressure emerged as the predominant risk factor globally, accounting for 57.9% of ICH-related DALYs in 2021. The impact of this risk factor showed marked regional variation, with Central Europe reporting the highest attribution (63.3%) and Andean Latin America the lowest (44.7%).
Regional analysis revealed distinct patterns for other risk factors. Smoking-attributable DALYs were most pronounced in Eastern Europe (22.5%) and minimal in Western Sub-Saharan Africa (4.4%). Alcohol-attributable DALYs peaked in Western Europe (11.7%) and were lowest in North Africa and Middle East (0.5%). High fasting plasma glucose showed the greatest impact in High-income North America (7.5%) and the least in Eastern Sub-Saharan Africa (3%).
Age-specific analysis revealed that DALYs attributable to these risk factors increased progressively with age until 65–69 years, reaching a peak in this age group before declining gradually (Supplementary Fig. S8). The contribution of risk factors varied across SDI regions, with High-middle SDI regions showing greater proportions attributable to smoking, alcohol use, and high fasting plasma glucose compared to Low SDI regions, underscoring the complex interaction between socioeconomic development and risk factor profiles in ICH burden.
Future forecasts of global burden of ICH
Projections of ICH burden from 2021 to 2030 reveal divergent trends across different epidemiological measures (Supplementary Fig S9). ASPR demonstrate an anticipated increase from 194 per 100,000 population in 2021 to 210 per 100,000 by 2030, with consistently higher rates observed in males compared to females.
In contrast, ASIR show a projected decline from 40.8 per 100,000 population in 2021 to 38.2 per 100,000 by 2030. Similarly, ASDR are expected to decrease modestly from 39 per 100,000 in 2021 to 36 per 100,000 by 2030, potentially reflecting improvements in acute care and management strategies.
The burden of disease, measured by age-standardized DALY rates, follows this downward trend, with projected reduction from 923.6 per 100,000 population in 2021 to 855 per 100,000 by 2030. Notably, among all epidemiological indicators, only prevalence shows an upward trajectory, while the gender disparity persists across all measures, with males consistently experiencing higher disease burden than females.
In terms of absolute numbers, our projections indicate by 2030, prevalent cases will reach 10.1 million in males and 8.0 million in females, while incident cases will be 1.9 million in males and 1.4 million in females. Deaths are projected to reach 1.9 million in males and 1.2 million in females, with total DALYs reaching 45.6 million in males and 28.5 million in females.
Discussion
This comprehensive analysis of the global, regional, and national burden of ICH from 1990 to 2021 reveals significant trends and disparities in prevalence, incidence, mortality, and DALYs. Our findings provide crucial insights into the evolving landscape of ICH burden worldwide and highlight areas requiring targeted interventions and resource allocation.
The global decrease in ASPR of ICH, with an EAPC of -0.97, suggests overall progress in ICH prevention and control. This trend aligns with findings from the most recent GBD 2021 stroke study1. Our results extend these observations specifically to ICH, highlighting the need for continued efforts in stroke prevention and management. The observed reduction in ASIR of ICH, with an EAPC of -1.52, is particularly encouraging. This decline may be attributed to improved control of key risk factors for ICH, such as hypertension, which has been identified as the most significant modifiable risk factor for ICH. A meta-analysis by O’Donnell et al. demonstrated that hypertension accounts for approximately 73.6% of the population-attributable risk for ICH. The global efforts to enhance hypertension awareness, treatment, and control, as reported by Mills et al., may have contributed substantially to the declining incidence of ICH observed in our study14.
Although there has been a general decrease in the age-standardized rates, our analysis highlights considerable regional differences in the incidence of ICH. Regions with a low SDI consistently show higher age-standardized rates in terms of prevalence, incidence, mortality, and DALYs when compared to regions with a high SDI. These disparities are likely even larger than observed, since many cases from low-income countries may be underdocumented due to substantially lower rates of hospitalization and postmortem examinations in low-SDI compared to high-SDI regions. This phenomenon aligns with the epidemiological transition theory, which posits that as nations advance through various stages of socioeconomic development, they undergo a transition in their disease profile, transitioning from a predominance of infectious diseases to a predominance of non-communicable diseases, such as stroke.
The higher burden of ICH in low SDI regions can be attributed to several factors. First, these regions often have limited access to quality healthcare and advanced diagnostic technologies, leading to delayed or missed diagnoses and suboptimal management of ICH cases. A study by Magwood et al. highlighted the disparities in stroke care quality between high- and low-income countries, emphasizing the need for improved healthcare infrastructure and resources in less developed regions15. Second, the prevalence of key risk factors for ICH, such as uncontrolled hypertension and unhealthy lifestyles, tends to be higher in low SDI regions. A systematic review by Adeloye et al. reported a higher prevalence of hypertension in low- and middle-income countries compared to high-income countries, particularly in urban areas undergoing rapid socioeconomic changes16.
The observed gender differences in ICH prevalence, with males consistently exhibiting higher prevalence rates across all age groups, warrant further investigation. This gender disparity may be partly explained by differences in risk factor profiles between men and women. For instance, a meta-analysis by Peters et al. found that smoking, a known risk factor for ICH, confers a 25% higher risk of stroke in women compared to men17. However, men generally have a higher prevalence of smoking and alcohol consumption, which may contribute to their increased ICH risk. Additionally, hormonal factors and differences in healthcare-seeking behaviors between genders may play a role in these disparities.
The age-related increase in ICH prevalence and incidence observed in our study is consistent with previous research on stroke epidemiology. The GBD 2016 Stroke Collaborators reported a similar age-related increase in stroke incidence and prevalence globally18. This trend can be attributed to the cumulative effect of risk factors over time, as well as age-related changes in cerebral vasculature that increase susceptibility to ICH. The particularly marked elevation in ICH incidence observed in individuals aged 65 and above underscores the importance of targeted prevention strategies for this high-risk population.
Our analysis of risk factors revealed distinct regional variations that reflect complex interactions between geography, culture, and socioeconomic conditions. High systolic blood pressure, while consistently the leading risk factor globally (57.9% of ICH-related deaths), showed substantial regional variation. Its higher attribution in Southern Sub-Saharan Africa (64.2%) compared to Oceania (44.7%) likely reflects differences in healthcare accessibility, dietary habits, and salt consumption patterns across regions. The pronounced variation in smoking-attributable burden between Eastern Europe (16.6%) and Western Sub-Saharan Africa (3.3%) mirrors regional differences in tobacco control policies, affordability, and social norms around smoking. Alcohol-attributable burden showed striking regional contrasts, from 11.2% in Australasia to 0.5% in North Africa and Middle East, primarily reflecting religious and cultural influences on alcohol consumption patterns. High body-mass index contributions varied notably between High-income North America (7.5%) and High-income Asia Pacific (1.2%), suggesting the influence of westernized diets, urbanization patterns, and differing cultural attitudes toward obesity. These findings emphasize the need for culturally sensitive and economically appropriate interventions that consider local risk factor profiles and societal contexts.
Our analysis of regional trends reveals notable variations in the burden of ICH. The high ASPR observed in Western Sub-Saharan Africa, Southeast Asia, and Oceania may be related to a combination of genetic, environmental, and socioeconomic factors. For instance, the high prevalence of ICH in Southeast Asia has been previously reported and linked to a higher prevalence of intracranial arterial stenosis in this population, as discussed by Kim et al.19. The significant decrease in ASPR observed in Tropical Latin America (EAPC -2.95) is encouraging and may reflect successful public health interventions in this region. However, further research is needed to elucidate the specific factors contributing to these regional variations. The substantial reduction in ASIR observed in East Asia, with the highest EAPC of -2.23, is particularly noteworthy. This improvement may be attributed to concerted efforts in stroke prevention and management in countries like China, which has implemented large-scale public health initiatives targeting stroke risk factors. A study by Wang et al. reported significant improvements in hypertension awareness, treatment, and control in China between 2002 and 2012, which may have contributed to the declining ICH incidence observed in our study20. The persistent high burden of ICH in regions such as Oceania, Southeast Asia, and Central Sub-Saharan Africa, as evidenced by their high age-standardized mortality rates and DALYs, highlights the urgent need for targeted interventions in these areas. The complex interplay of genetic susceptibility, environmental factors, and healthcare system limitations in these regions may contribute to their disproportionate ICH burden. For example, a study by Mehndiratta et al. highlighted the challenges in stroke care in Sub-Saharan Africa, including limited access to neuroimaging facilities and acute stroke units, which can significantly impact ICH outcomes21. The improvement observed in Central Europe, where age-standardized DALYs rates decreased by 63.6% between 1990 and 2021, is encouraging and may serve as a model for other regions. This progress could be attributed to improvements in healthcare systems, increased awareness of stroke risk factors, and implementation of evidence-based prevention and treatment strategies. At the national level, the striking variations in ASPR and ASIR of ICH underscore the importance of tailored, country-specific approaches to ICH prevention and management. While our analysis shows varying rates across different countries, these estimates should be interpreted with caution, particularly for smaller nations where high-quality epidemiological data may be limited. The different trends observed between countries, such as varying patterns in ASPR, likely reflect broader regional differences in healthcare system development, public health infrastructure, and the implementation of preventive strategies. These variations may be influenced by multiple factors including the pace of epidemiological transition, healthcare resource availability, and the effectiveness of public health interventions across different settings. To address regional disparities, we recommend targeted strategies for low-SDI regions. Cost-effective interventions, such as community health worker programs for blood pressure management, should be prioritized. Mobile health technologies and telemedicine can bridge healthcare gaps, particularly in remote areas of Sub-Saharan Africa and Southeast Asia. For regions with limited neuroimaging access, investing in basic diagnostic equipment and training healthcare workers at district hospitals can improve ICH detection and management. Partnerships between high- and low-SDI regions can support knowledge transfer in areas like stroke unit organization and emergency care. Strengthening primary healthcare infrastructure and implementing region-specific public health campaigns are essential, with interventions tailored to local budgets and resources to ensure sustainability.
Building on our findings, we propose several key clinical and public health implications. First, the regional variations in ICH burden suggest the need for differentiated prevention strategies. In high-burden regions like Western Sub-Saharan Africa and Southeast Asia, strengthening primary healthcare systems for early detection and management of hypertension should be prioritized. Implementation of community-based blood pressure screening programs and improving access to affordable antihypertensive medications could significantly reduce ICH incidence. Second, the success observed in regions like Central Europe, with its 63.6% reduction in age-standardized DALYs, provides valuable lessons for clinical practice. Their model of integrated stroke care, combining primary prevention, rapid emergency response, and comprehensive rehabilitation services, could be adapted for other healthcare systems. The significant improvements seen in East Asia, particularly China’s success in hypertension management, demonstrate the effectiveness of large-scale public health initiatives in reducing ICH burden. Third, our findings on risk factor variations across regions suggest the need for culturally tailored interventions. Healthcare providers should consider regional and cultural contexts when developing prevention strategies, such as dietary recommendations for blood pressure management or smoking cessation programs. In areas with limited healthcare resources, mobile health technologies and community health worker programs could help extend the reach of preventive services. These clinical implications emphasize the importance of translating epidemiological findings into actionable strategies for healthcare providers and public health practitioners, ultimately aiming to reduce the global burden of ICH through targeted, evidence-based interventions.
Limitation
Several key limitations should be considered when interpreting our findings. First, data quality and availability vary substantially across regions, particularly in low- and middle-income countries where epidemiological surveillance systems may be less robust. The lower rates of hospitalization and postmortem examinations in these settings likely lead to significant underreporting of ICH cases, affecting the accuracy of burden estimates. Second, while the GBD methodology employs sophisticated modeling techniques to address data gaps, the estimation of risk factor attributions faces specific challenges. The complex interactions between multiple risk factors and limited data on risk factor exposure in many regions may affect the precision of attributable burden calculations. Third, our analysis relies heavily on age-standardized rates, which while useful for comparing populations, may mask important variations in absolute burden and specific age group trends. Finally, the broad scope of this study, while providing valuable global insights, cannot capture detailed local variations or identify specific high-risk subpopulations that might require targeted interventions.
Conclusion
Our comprehensive analysis of the global burden of ICH from 1990 to 2021 reveals a complex landscape of epidemiological trends, characterized by an overall decrease in age-standardized rates but significant regional and national disparities. These findings underscore the need for tailored, context-specific approaches to ICH prevention and management, particularly in low SDI regions and countries with persistently high ICH burden. Future research should focus on elucidating the specific factors contributing to these disparities and evaluating the effectiveness of targeted interventions across different populations. By addressing these challenges, we can work towards reducing the global burden of ICH and improving outcomes for affected individuals worldwide.
Data availability
GBD study 2021 data resources were available online from the Global Health Data Exchange (GHDx) query tool ( http://ghdx.healthdata.org/gbd-results-tool).
References
Feigin, V. L. et al. Global, regional, and national burden of stroke and its risk factors, 1990–2021: a systematic analysis for the global burden of disease study 2021. The Lancet. Neurology 23, 973–1003 (2024).
Ferrari, A. J. et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet (London, England) 403, 2133–2161 (2024).
Brauer, M. et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet (London, England) 403, 2162–2203 (2024).
Murray, C. J. L. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet (London, England). 396, 1223–1249 (2020).
Aho, K. et al. Cerebrovascular disease in the community: results of a WHO collaborative study. Bulletin World Health Organization 58, 113–130 (1980).
Feigin, V. L. et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. Neurol. 20, 795–820 (2021).
Roth, G. A. et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet (London, England). 392, 1736–1788 (2018).
Liane, K. et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet (London, England). 402, 203–234 (2023).
Clegg, L. X., Hankey, B. F., Tiwari, R., Feuer, E. J. & Edwards, B. K. Estimating average annual per cent change in trend analysis. Stat. Med. 28, 3670–3682. https://doi.org/10.1002/sim.3733 (2009).
Knoll, M. et al. An R package for an integrated evaluation of statistical approaches to cancer incidence projection. Bmc Med. Res. Methodol. 20, 257. https://doi.org/10.1186/s12874-020-01133-5 (2020).
Li, S. et al. Changing trends in the disease burden of esophageal cancer in China from 1990 to 2017 and its predicted level in 25 years. Cancer Med. 10, 1889–1899. https://doi.org/10.1002/cam4.3775 (2021).
Liu, N. et al. Burden, trends, and risk factors for breast cancer in China from 1990 to 2019 and its predictions until 2034: an up-to-date overview and comparison with those in Japan and South Korea. Bmc Cancer 22, 826. https://doi.org/10.1186/s12885-022-09923-4 (2022).
Wu, B. et al. Temporal trends of breast cancer burden in the western pacific region from 1990 to 2044: implications from the global burden of disease study 2019. J. Adv. Res. https://doi.org/10.1016/j.jare.2023.07.003 (2023).
Mills, K. T., Stefanescu, A. & He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 16, 223–237. https://doi.org/10.1038/s41581-019-0244-2 (2020).
Magwood, G. S. et al. Barriers and facilitators of stroke recovery: perspectives from african americans with stroke, caregivers and healthcare professionals. J. Stroke Cerebrovascular Dis : Official J. Nat. Stroke Assoc. 28, 2506–2516. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.06.012 (2019).
Adeloye, D., Basquill, C., Aderemi, A. V., Thompson, J. Y. & Obi, F. A. An estimate of the prevalence of hypertension in Nigeria: a systematic review and meta-analysis. J. Hypertension 33, 230–242. https://doi.org/10.1097/HJH.0000000000000413 (2015).
Peters, S. A. E., Huxley, R. R. & Wooard, M. Smoking as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 81 cohorts, including 3,980,359 individuals and 42,401 strokes. Stroke 44, 2821–2828. https://doi.org/10.1161/STROKEAHA.113.002342 (2013).
Owens, C. et al. Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the global burden of disease study.2016. Lancet Neurol. https://doi.org/10.1016/S1474-4422(19)30034-1 (2019).
Bang, O. Y. Intracranial atherosclerosis: current understanding and perspectives. J. Stroke 16, 27–35. https://doi.org/10.5853/jos.2014.16.1.27 (2014).
Wang, Z. et al. Status of hypertension in china: results from the china hypertension survey, 2012–2015. Circulation 137, 2344–2356. https://doi.org/10.1161/CIRCULATIONAHA.117.032380 (2018).
Mehndiratta, M. M., Khan, M., Mehndiratta, P. & Wasay, M. Stroke in Asia: geographical variations and temporal trends. J. Neurol. Neurosurg. Psychiatry 85, 1308–1312. https://doi.org/10.1136/jnnp-2013-306992 (2014).
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82470510) and the early warning systems and rehabilitation research for cognitive impairment after stroke. Hubei Provincial Key Research and Development Plan Project. 2022.8–2024.6,provincial projects,Project approval number 2022BCE062.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
All participants in this study consented to publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Zw., Wan, Mp., Tai, Jh. et al. Global regional and national burden of intracerebral hemorrhage between 1990 and 2021. Sci Rep 15, 3624 (2025). https://doi.org/10.1038/s41598-025-88017-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88017-0
Keywords
This article is cited by
-
Global, regional and national burden of intracerebral hemorrhage attributable to dietary and metabolic risks from 1990 to 2021 and projections to 2050: a systematic analysis based on the Global Burden of Disease 2021 comparative risk assessment framework
European Journal of Medical Research (2025)
-
Incidence of intracerebral hemorrhage in Shangdong province, East China, 2012-2021: a population-based study
Scientific Reports (2025)
