
Abstract
To assess the clinical outcomes of robot-assisted proximal femoral nail antirotation (PFNA) surgery in elderly patients with unstable femoral intertrochanteric fractures (UFIFs). 151 patients who underwent UFIF and PFNA surgery between January 2020 and May 2024 were analyzed retrospectively. Of these, 78 patients were treated with traditional PFNA surgery (control group), and 73 patients were treated with robot-assisted PFNA surgery (observation group). The observed indicators included visual analog pain scale (VAS) score, surgery time, PFNA operation time, tip-apex distance (TAD), intraoperative blood loss (IBL), perioperative hidden blood loss (PHBL), postoperative allogeneic blood transfusion rate (PABTR), hospital stay, time to first independent walking with crutches postoperatively, time to independent walking without crutches, and Harris hip function score (HHFS). There were no statistically significant differences in general condition between the two groups before surgery. Surgery time, PFNA operation time, IBL, PHBL, PABTR, TAD, hospital stay, time to first independent walking with crutches postoperatively, time to independent walking without crutches, VAS score, and HHFS were significantly improved in the observation group compared with the control group. Thus, compared with traditional PFNA surgery for UFIF in elderly patients, robot-assisted PFNA yields better outcomes in terms of the quality of PFNA surgery, surgical trauma, conserving clinical blood resources, and patient recovery.
Similar content being viewed by others
Introduction
Senile femoral intertrochanteric fractures are a common type of limb fracture and account for approximately 50% of hip fractures1. Given the poor recovery of hip joint function after conservative treatment and the high rates of complications and mortality2,3, femoral intertrochanteric fractures are referred to as “the last fracture in life,” and most doctors recommend that patients undergo surgical treatment as soon as possible. However, perioperative blood loss, especially hidden blood loss, is a common fatal factor in these patients4,5,6. Reducing perioperative blood loss and transfusion, minimizing surgical trauma, and ensuring the quality and effectiveness of surgery remain clinical challenges.
In 2015, orthopedic surgical robots began to be used in trauma orthopedic surgery. In 2019, scholars reported the application of orthopedic surgical robots in proximal femoral nail antirotation (PFNA) surgery for unstable femoral intertrochanteric fractures (UFIFs), achieving good clinical results7. Further improvement and development of orthopedic surgical robots have led to their widespread clinical application because of their minimal invasiveness and precise, flexible, and stable characteristics. This study assessed the impact of using orthopedic surgical robots to assist PFNA surgery on surgical trauma and quality, postoperative complications, and recovery in elderly patients with UFIFs. We hypothesized that the employment of orthopedic surgical robot in PFNA surgery would enhance the quality of conventional PFNA surgery, diminish the volume of blood loss throughout the perioperative phase, and expedite the recuperation of patients.
Materials and methods
This study was performed following the principles of the Declaration of Helsinki. All experimental protocols were approved by Shaoguan Hospital Affiliated to Southern Medical University. All patients provided informed consent.
General Information
Inclusion criteria were: (1) patients who were at least 60 years old with unilateral closed intertrochanteric fractures; (2) patients who had undergone PFNA assisted by orthopaedic robot navigation or traditional PFNA; (3) main evaluation indicators included intraoperative blood loss, perioperative hidden blood loss, postoperative allogeneic blood transfusion rate, the operation time, and the Harris score of hip function, etc.
Exclusion criteria were: (1) pathological fractures such as bone metastasis of cancer, primary bone tumor, and metabolic bone disease; (2) history of fractures in the affected hip; (3) bilateral femoral intertrochanteric fracture; (4) the affected side of the hip suffered from moderate to severe arthritis or femoral head necrosis; (5) postoperative follow-up time of less than 1 year.
A retrospective analysis was conducted on 151 patients who were diagnosed with senile UFIF and who underwent surgical treatment at two hospitals between January 2020 and May 2024. All patients had unilateral fractures. Among these patients, 78 patients were treated with traditional PFNA surgery (control group), and 73 patients underwent PFNA surgery assisted by orthopedic surgical robots (observation group). All patients underwent diagnostic classification and surgical preplanning based on hip X-rays and CT scans upon admission. After assessing the basic tolerance for surgery and anesthesia risks, surgeries were scheduled to ensure stable preoperative vital signs, including hemoglobin levels ≥ 100 g/L, albumin levels ≥ 35 g/L, and blood glucose ≤ 11.1 g/L.
Robot-assisted PFNA surgical procedure
Step 1 was obtaining informed consent. Patients signed both the surgery informed consent form and the orthopedic surgical robot-assisted informed consent form.
Step 2 was anesthesia and positioning. Patients received either combined spinal–epidural anesthesia or general anesthesia with endotracheal intubation. Once anesthesia was effective, patients were placed in a supine position on a traction bed, with the body bent toward the healthy side using the affected hip as a pivot point. The healthy limb was positioned with the knee and hip flexed on an abduction rack, facilitating C-arm fluoroscopy during the procedure.
Step 3 was traction and reduction of the C-arm flu, which was performed with the assistance of a C-arm fluoroscope (Siemens). Traction and reduction were carried out until satisfactory repositioning was achieved. In cases where reduction was difficult, a small incision was made on the anterior superior aspect of the hip on the opposite side to assist repositioning.
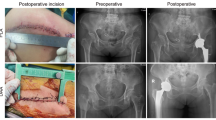
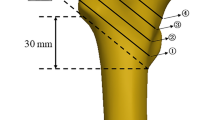
Step 4 was the activation and operation of the orthopedic robot (TiRobot, Tianzhihang Medical Technology) to complete PFNA surgery. Standard disinfection procedures were followed, and sterile drapes were used. The orthopedic surgical robot system was positioned, the machine was debugged and calibrated, and the C-arm machine was connected. After completion, fluoroscopy was performed to obtain anteroposterior and lateral images of the affected hip, which were subsequently transmitted to the robot workstation for four guide-pin placement planning. The general operation is detailed in reference7. The general operation was modified to include the planning of the placement and depth of the four guide pins (Fig. 1a, b). The 1st guide pin was used to temporarily fix both ends of the fracture to maintain stability and locate the femur calcar. The 2nd guide pin, if necessary, was used to fix the lesser trochanteric bone block and locate the posterior upper of the lesser trochanter. The 3rd guide pin was used to guide the drilling of the bone tunnel of the spiral blade and locate the femur calcar in the lower 1/3 of the femur neck. Finally, the 4th guide pin was used to guide the drill in drilling a hole at the insertion point for placement of the PFNA main nail at the apex and upper part of the greater trochanter of the femur. During the planning process, temporary fixation of the fracture ends and the lesser trochanter was necessary to avoid affecting the placement of the PFNA main nail. After the planning was completed, the robot machine arm was started, and the four guide pins (2.5 mm) were drilled into the bone in sequence under the guidance of the machine arm. After confirming that the positions of the guide pins were correct by fluoroscopy (Fig. 1c, d), the bone tunnel was predrilled with a hollow drill based on the position of the 3rd guide pin, which was temporarily withdrawn from the outer femoral cortex of the tunnel until the insertion of the main nail. Under the guidance of the 4th guide pin, the entry point in the greater trochanter of the femur was expanded into a hole by using a hollow drill. Next, guided by the 4th guide pin, a PFNA main nail was inserted at the hole in the proximal femur. When the hole in the spiral blade of the main nail overlapped with the predrilled bone tunnel of the spiral blade in a straight line, the 3rd guide pin was reinserted by hand, and the spiral blade was inserted and pressurized under guidance. Finally, under the guidance of the PFNA guide set, a distal screw was placed, the tail cap was installed, and the results were verified by fluoroscopy (Fig. 1e, f). After irrigation, the surgical incision was sutured.

Technical methods involving four guide pins by orthopedic robot-assisted PFNA surgery.(a, b), Planning the placement of the 1st guide pin (White) used to temporarily fix the fracture ends, planning the placement of the 2nd guide pin (blue) used to fix the lesser trochanter bone block, planning the placement of the 3rd guide pin (pink) used to guide the spiral blade, and planning the placement of the 4th guide pin (red) used to guide the main pin position. (c, d), With the assistance of the robot mechanical arm, these guide pins were placed under the guidance of anteroposterior and lateral fluoroscopy of the hip joint as needed. (e, f), Finally, under the guidance, PFNA was implanted and the results were verified by fluoroscopy.
Traditional PFNA operation
A skin incision was made over the lateral aspect of the hip at the level of the greater trochanter and extended proximally. The soft tissues were dissected by hand to palpate the tip of the greater trochanter. Under guidance by C-arm fluoroscopy, the main nail guidewire and the PFNA main nail were inserted. Subsequently, under the guidance of the PFNA aiming device, the main nail, helical blade guidewire, helical blade, and distal screws were sequentially positioned.
Observation indicators
Surgery time and PFNA operation time
The surgery time was recorded from the incision, after the sterile towel was laid out following disinfection, until the completion of skin suturing. The PFNA operation time was recorded from the insertion of the main nail guidewire for the intramedullary nail until the completion of tail cap installation.
Tip-apex distance (TAD)
The position of the helical blade TAD was observed and recorded according to postoperative X-ray images.
Intraoperative blood loss (IBL) volume, perioperative hidden blood loss (PHBL) volume, and postoperative allogeneic blood transfusion rate (PABTR). The IBL volume was calculated by calculating the total volume of blood collected via intraoperative suction and in drainage bags and the amount of blood absorbed by gauze. The volume of PHBL was based on the difference between the lowest hemoglobin value obtained from the patient’s routine blood examination at admission and the patient’s routine blood re-examination after surgery minus the IBL volume. Patients who received allogeneic blood transfusions after surgery were included.
2.4.4 Visual analog-pain score (VAS). The VAS score was calculated and recorded at admission, on the 1st, 2nd, and 3rd postoperative days, and on the discharge day.
Postoperative follow up and related complications
All patients underwent anterior and lateral X-ray examinations of the affected hip before discharge and at the 1st, 2nd, 3rd, 6th, 9th, and 12th months postoperatively to assess fracture healing. The time required for patients to walk independently with crutches and the time required to walk independently without crutches were recorded. The patient’s hip Harris functional score (HHFS) on the operated limb was obtained at 1, 2, and 3 months postoperatively and at the last follow-up. Additionally, the incidence rates of other related surgical complications and mortality were recorded.
Statistical analysis
SPSS 25.0 (IBM, Corporation) was used to perform statistical analyses. The sample size requirement was based on the primary outcome of HBL determined by previous studies. According to previous literature reports, the HBL in UFIFs in elderly patients can reach about 700 ml ± 300 ml. Setting the sample allocation ratio, significance level (α), and power (1 -β) as 1.0, 0.05, and 0.90, respectively, indicated that 40 patients were needed for subgroup analysis. To compensate for the expected dropouts which were 10%, the sample size was 45 cases in each group, and the dropout rate was preset to 20%. The final calculation resulted in a sample size of 120 cases at least. The quantitative data are presented as the means ± standard deviations. A t test was used for comparisons of quantitative variables, and the chi-square test or Fisher’s exact test was used for comparisons of categorical variables. The values of VAS and HHFS at different time points were analyzed using repeated-measures ANOVA. P < 0.05 indicated a significant difference.
Results
General results (Table 1)
The PFNAs ranged from 170 mm to 200 mm in length and 9 mm to 11 mm in diameter. The control group included 47 males and 31 females with an age range of 59 to 91 years (average 77.8 ± 7.95 years). According to the International Orthopedic Association (AO) classification, there were 10 patients with type A1, 42 patients with type A2 and 26 patients with type A3. Regarding the causes of injury, there were 25 cases due to traffic accidents, 45 cases from falls, and 8 cases from other causes. The time interval from hospital admission to surgery ranged from 2 to 8 days (average 3.23 ± 1.28). The observation group included 40 males and 33 females aged 62 to 88 years (average 75.7 ± 6.73); there were 8 patients with type A1, 37 patients with type A2 and 28 patients with type A3 according to the AO classification. There were 21 cases of traffic accident injuries, 41 cases of falls, and 11 other cases. The time interval from hospital admission to surgery ranged from 1 to 7 days (average 3.01 ± 1.32). All patients had at least two comorbidities and underlying diseases, including anemia, hypertension, diabetes, osteoporosis, syphilis, hypoproteinemia, uremia, hyperuricemia, chronic obstructive pulmonary disease (COPD), Colles’ fracture, osteoarthritis of the knee, history of contralateral hip surgery, history of knee replacement, sequelae of polio, history of heart failure, history of myocardial infarction, history of venous thrombosis, history of lumbar compression fractures, and lumbar spine surgery. There were no statistically significant differences between the two groups in sex, age, AO classification, cause of injury, time from admission to surgery, or complication status.
Clinical observation indicator results (tables 2 and 3)
All patients had a minimum of 2 and a maximum of 5 skin incisions requiring suturing (ranging from 1 to 10 cm in length). The total length of incisions in the control group was 13.27 ± 1.79 cm, and that in the observation group was 12.97 ± 2.12 cm, with no statistically significant difference (t = 0.9416, P > 0.05). All wounds healed.
The average surgery time was 79.48 min for the control group and 62.26 min for the observation group, a statistically significant difference (t = 14.0217, P < 0.01). Moreover, the average time for the traditional PFNA operation was 60.64 min in the control group and 20.27 min in the observation group, a significant difference (t = 35.2531, P < 0.01). These results suggest that the use of orthopedic surgical robots in performing PFNA surgeries can significantly reduce the duration of surgery.
In terms of perioperative blood loss, the average IBL in the observation group was 86.78 ml, significantly less than the average of 147.95 ml in the control group (t = 7.0906, P < 0.01). The average PHBL in the control group was 744.23 ml, significantly greater than the average of 504.66 ml in the observation group (t = 4.7635, P < 0.05). Consistent with these results, the PABTR was significantly greater in the control group (61.54%) than in the observation group (34.25%) (χ2 = 11.2472, P < 0.01). This indicates that the use of orthopedic surgical robots in performing PFNA surgeries can reduce perioperative blood loss, particularly PHBL, thereby reducing the need for allogeneic blood transfusions.
Postoperative X-ray follow-up revealed that the average TAD of the helical blade was 17.17 mm in the observation group, significantly greater than average of 19.38 mm in the control group (t = 4.0278, P < 0.01). The control group required an average of 5.22 days to first walk with crutches postoperatively, which was significantly longer than the time for the observation group (4.03 days) (t = 3.5501, P < 0.01). The average hospital stay was 13.31 days for the control group and 11.12 days for the observation group, a statistically significant difference (t = 4.9424, P < 0.01). After discharge, patients in the control group needed an average of 5.13 months to walk independently without crutches, significantly longer than the time for patients in the observation group (3.88 months) (t = 5.5552, P < 0.01). These data suggest that orthopedic surgical robots improve the quality and stability of PFNA surgeries, benefiting patient functional recovery.
In terms of perioperative pain, the preoperative VAS score did not differ significantly between the control and observation groups; in both groups, the postoperative VAS score gradually decreased. On the first, second, and third days after surgery, the VAS score was greater in the control group than in the observation group, which experienced faster pain relief. However, there was no statistically significant difference in the VAS score between the two groups at the time of discharge. Regarding hip joint function, both groups showed progressive improvement in HHFSs from the first month postoperatively until the last follow-up. However, compared to the control group, the observation group achieved higher HHFSs starting from the first postoperative month until the final follow-up. These findings indicate that the observation group recovered more quickly in terms of postoperative pain and hip joint function rehabilitation than did the control group.
Regarding the incidence of postoperative complications, the control group had 7 cases of lower limb venous thrombosis and 1 case of acute cerebral infarction (which resolved after endovascular treatment), 8 cases where internal fixation failed leading to 4 cases undergoing hip arthroplasty and 4 cases revision, and 3 case of multiple organ failure resulting in death. In the observation group, 3 patient developed deep vein thrombosis postoperatively, which resolved after anticoagulant and other conservative treatments. 4 cases where internal fixation failed leading to hip arthroplasty, and 1 case of multiple organ failure resulting in death. The postoperative complication rate was 24.36% (19/78) in the control group and 10.96% (8/73) in the observation group; however, the difference between the two groups was not statistically significant (χ2 = 4.6113, P < 0.05).
Discussion
For the surgical treatment of UFIFs in elderly patients, minimally invasive PFNA intramedullary fixation is the preferred choice. Elderly patients often have underlying diseases and complications, such as anemia, osteoporosis, cardiopulmonary diseases, and thrombosis, that lead to a compensatory state of physiological functions. Intraoperative bleeding during surgery and perioperative blood loss can often cause decompensation in elderly patients, endangering their lives8,9. This retrospective analysis revealed that orthopedic robot-assisted PFNA surgery improved clinical outcomes in the treatment of UFIFs in elderly patients compared with traditional PFNA surgery.
Theoretically, for elderly UFIF patients, shorter surgery times and higher PFNA quality will lead to reduced surgical trauma and faster recovery10. The main trauma of PFNA surgery is intraoperative and postoperative bleeding. PFNA surgery itself is a minimally invasive procedure, and actual clinical surgeries rarely involve significant intraoperative bleeding. Reports in the literature4,5,6,11 indicate that the average surgery time for traditional PFNA in elderly patients with UFIFs is approximately 50–120 min, with an average IBL of approximately 50–400 ml. However, PHBL can reach 400–3000 ml12. These values are consistent with the data from this study. Surgery is a significant factor in PHBL. The data from this study indicate that, compared to traditional PFNA operations, robot-assisted surgery reduced not only the surgery time but also the actual PFNA operation time, which averaged only about 20 min. As a result, IBL and PHBL were significantly reduced in the robot-assisted group, significant decreasing the rate of patient allogeneic blood transfusion and conserving clinical blood resources.
The advantages of robot-assisted surgery include not only the precise temporary fixation of bone fragments during surgery through the use of guide needles but also the direct simulation and measurement of depth and length data, which ensure the precision of the surgical procedure. Precision is particularly advantageous when fixing the lesser trochanter fragments during surgery13. In traditional PFNA surgery, the surgeon’s experience is an important factor affecting the degree of surgical trauma and the quality of the PFNA procedure14,15. Common issues with traditional PFNA surgery include instability at the fracture site, loss of reduction leading to an improper entry point for the main nail, incorrect positioning of the spiral blade, and difficulties in fixing the lesser trochanter. These problems can result in prolonged postoperative surgery time, increased bleeding, extended hospital stays, suboptimal recovery, increased surgical complications, multiple revision surgeries, and even death due to exacerbation of underlying diseases16. Additionally, during traditional PFNA procedures, inaccuracies in the entry point for the main nail may require repeated adjustments and fluoroscopy to correct the angle and position of the guide pin, loss of reduction due to prenail insertion reaming, and loss of reduction when inserting a main nail with too large a diameter, which can lead to increased surgery time and bleeding due to surgical trauma17. Therefore, multiple adjustments may be necessary, and even after several attempts, the ideal position may still not be achieved, which could be a major factor in increasing surgery time and intraoperative bleeding.
Undoubtedly, clinical evidence suggests that traditional PFNA surgery for elderly UFIF patients can effectively alleviate pain, control the progression of underlying diseases and complications, improve hip joint function, and enhance quality of life. However, if the quality of the PFNA surgery is poor, resulting in persistent postoperative pain, implant-related complications, and other disease complications, then postoperative ambulation, clinical healing of the fracture, recovery of hip joint function, and quality of life can be severely affected. Although there was no statistically significant difference in the incidence of perioperative complications between the two groups before and after surgery and although local pain gradually subsided and was significantly alleviated at discharge, the pain relief in the robot-assisted group occurred earlier and was more effective than that in the traditional PFNA group. This may be a factor influencing the faster recovery of hip joint function and earlier ambulation without crutches in these patients postoperatively. Consistently, recent comparative studies have provided direct evidence that navigation system-assisted PFNA surgery, compared to traditional PFNA surgery, can ensure surgical bleeding and significantly improve patients’ hip function7,14.
However, robot-assisted PFNA surgery also has several limitations. The preparation time before the start of surgery is longer for robot-assisted surgery, which increases the anesthesia time about 10 min (The data is not shown). This was a two-center retrospective study, and the number of patients was limited.
In summary, combining the precision and stability of orthopedic surgical robots with the assistance of guide-pin techniques ensures the quality of PFNA surgical procedures, thereby reducing surgical trauma, decreasing the need for allogeneic blood transfusions, conserving blood resources, and accelerating patient revovery.
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions or privacy.
References
Chen, P. et al. A biomechanical investigation of a novel intramedullary nail used to salvage failed internal fixations in intertrochanteric fractures. J. Orthop. Surg. Res. 18 (1), 632–641 (2023).
Adeyemi, A. & Delhougne, G. Incidence and economic burden of intertrochanteric fracture: a Medicare Claims Database Analysis. JB JS Open. Access. 4 (1), e0045 (2019).
Liu, P. et al. Artificial intelligence to detect the femoral intertrochanteric fracture: the arrival of the intelligent-medicine era. Front. Bioeng. Biotechnol. 10 (2), 927–936 (2022).
Stacey, J., Bush, C. & DiPasquale, T. The hidden blood loss in proximal femur fractures is sizeable and significant. J. Clin. Orthop. Trauma. 18, 16:239–243 (2021).
Guo, J., Zhang, Y. & Hou, Z. Intramedullary fixation does not cause a large amount of hidden blood loss in Elderly patients with intertrochanteric fractures. Clin. Interv Aging. 17, 16:475–486 (2021).
Luo, X., He, S., Li, Z. & Li, Q. Quantification and influencing factors of perioperative hidden blood loss during intramedullary fixation for intertrochanteric fractures in the elderly. Arch. Orthop. Trauma. Surg. 140 (10), 1339–1348 (2020).
Lan, H. et al. Intramedullary nail fixation assisted by Orthopaedic Robot Navigation for Intertrochanteric Fractures in Elderly patients. Orthop. Surg. 11 (2), 255–262 (2019).
Yang, X., Wu, Q. & Wang, X. Investigation of perioperative hidden blood loss of unstable intertrochanteric fracture in the elderly treated with different intramedullary fixations. Injury 48 (8), 1848–1852 (2017).
Zhao, K. et al. Incidence of and risk factors for pre-operative deep venous thrombosis in geriatric intertrochanteric fracture patients. Int. Orthop. 46 (2), 351–359 (2022).
Haidukewych, G. J. Intertrochanteric fractures: ten tips to improve results. Instr Course Lect. 59, 503–509 (2010).
Cui, Y. et al. Clinical application effects of different preoperative blood management schemes in older patients with delayed intertrochanteric fracture surgery. Clin. Interv Aging. 17, 825–835 (2022).
Obada, B. et al. Clinical outcomes of total hip arthroplasty after femoral neck fractures vs. osteoarthritis at one year follow up-A comparative, retrospective study. Int. Orthop. Sep;48 (9), 2301–2310 (2024).
Liu, X. et al. Does integrity of the lesser trochanter influence the surgical outcome of intertrochanteric fracture in elderly patients? BMC Musculoskelet. Disord. 16, 47 (2015).
Coviello, M. et al. Computer-assisted navigation for intramedullary nailing of intertrochanteric femur fractures: a preliminary result. Med. Glas (Zenica), 201 (2023).
Mereddy, P. et al. The AO/ASIF proximal femoral nail antirotation (PFNA): a new design for the treatment of unstable proximal femoral fractures. Injury 40 (4), 428–432 (2009).
Simmermacher, R. K. et al. The new proximal femoral nail antirotation (PFNA) in daily practice: results of a multicentre clinical study. Injury 39 (8), 932–939 (2008).
Hwang, J. H. et al. Mismatch between PFNa and medullary canal causing difficulty in nailing of the pertrochanteric fractures. Arch. Orthop. Trauma. Surg. 128 (12), 1443–1446 (2008).
Acknowledgements
Chaolong Lu and Xiao Wei contributed equally to this work. Zhengbo Hu Qiang Wu, Wenhu Li and Yunze Kang were as an equally senior author. The authors thank all of the patients who participated in the study.
Funding
This project was supported by the National Key Research and Development Program of China (Project Nos. 2022YFC2407500), Shaoguan Health and Wellness Scientic Research (Project Nos.Y25119), Guangdong Provincial Medical Scientific Research Fund (Project Nos. 2024111915152526).The funders had no role in study design,data collection and analysis, dedision to publish or preparation of the manuscripts.
Author information
Authors and Affiliations
Contributions
Conceived and designed the analysis: Zhengbo Hu, Qiang Wu, Wenhu Li, Chaolong Lu.Collected the data: Chaolong Lu, Xiao Wei, Lugen Li, Wenxing Lan, Yunze Kang, Qingyang Hu.Contributed data or analysis tools: Xiao Wei, Lugen Li, Zhengbo Hu, Qiang Wu, Wenxing Lan.Performed the analysis: Chaolong Lu, Xiao Wei, Penghuan Wu, Wenhu Li, Yunze Kang .Wrote the paper: Chaolong Lu, Xiao Wei, Zhengbo Hu, Qingyang Hu, Wenxing Lan.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
The study related to patients was followed by the principles of the Declaration of Helsinki. The approval was obtained from the ethics committee of Shaoguan Hospital Affiliated to Southern Medical University, and written informed consent was obtained from the patients.
Consent to participate
Consent to publish was obtained from all participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lu, C., Wei, X., Li, L. et al. Robot-assisted PFNA surgery improves clinical outcomes in the treatment of unstable femoral intertrochanteric fractures in elderly patients compared with traditional PFNA surgery. Sci Rep 15, 3836 (2025). https://doi.org/10.1038/s41598-025-88229-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88229-4
Keywords
This article is cited by
-
Robot-assisted versus conventional percutaneous screw fixation in calcaneal fractures: a retrospective analysis
European Journal of Trauma and Emergency Surgery (2025)
