
Abstract
This study aimed to assess the exact location, size, and clinical significance of prostatic calcification using computed tomography (CT). We retrospectively analyzed data from 5,492 patients who underwent CT at the Department of Urology in our hospital between January 2010 and December 2020. After applying exclusion criteria (prostate cancer, post-prostatectomy, indwelling urethral catheter, severe artifacts, and software errors), 4,805 patients were included in the final analysis. Patient age, medical history, laboratory findings, and the International Prostate Symptom Score (IPSS) were collected, with linear regression used to identify predictors of IPSS. Of the 4,805 patients, 1,525 had no calcification, 285 had calcification with a Hounsfield unit (HU) < 100, and 2,995 had calcification with HU ≥ 100. The average age of patients with calcification was significantly higher than that of patients without calcification. Total IPSS scores were significantly elevated in the calcification group, particularly in those with calcifications of HU ≥ 100. The majority of calcifications were located in the central zone (79.3%), followed by the periurethral (48.6%) and transitional zones (42.0%). Only a small number of calcifications were observed in the peripheral zone (0.9%). Multivariate analysis revealed that both age and prostate calcification were significant predictors of urinary symptoms. CT can be effectively utilized to accurately assess the exact location, size, and number of prostate calcifications. Prostate calcification increases with age and is associated with worsened lower urinary tract symptoms.
Similar content being viewed by others

Introduction
As the global population ages, interest in urological conditions has grown, leading to an increased utilization of transrectal ultrasonography (TRUS) in health promotion centers and urology departments. This rise in the application of TRUS has correspondingly increased the diagnosis of prostate calcifications, which are reported in 7.4–76.6% of cases, depending on the patient’s age1,2,3. Prostate calcifications are commonly associated with benign prostatic hyperplasia (BPH) and prostate cancer, although their precise etiology remains unclear4,5. Chemical analyses of prostatic calcifications have identified calcium phosphate—distinct from the calcium oxalate typically found in urinary stones—as the predominant component6,7. This finding supports hypotheses suggesting that stasis of prostatic secretions or dilation of prostatic ducts are key mechanisms in the formation of prostatic calcifications. Most calcifications are localized at the junction where the urethra meets the ejaculatory duct2,8,9.
Despite advancements in imaging techniques, most studies on prostate calcifications have been limited by technical challenges. Small calcifications often become indistinguishable within ultrasound noise, and accurate measurements are hindered by acoustic shadows cast behind the calcifications. Furthermore, prior research has analyzed prostate calcifications without precise classification methods, leading to inaccuracies. The assessment of calcification burden has also been insufficient, as many studies only documented the presence or absence of calcifications without quantifying their extent. In studies that attempted to evaluate the calcification burden using transrectal ultrasound, reliance on the longest axis of the calcifications introduced significant limitations. This method often failed to provide an accurate representation of the true burden, further complicating efforts to establish reliable quantitative measurements.
Unlike ultrasound, computed tomography (CT) is unaffected by ultrasound noise and provides imaging quality comparable to magnetic resonance imaging (MRI), the gold standard for prostate imaging in the diagnosis of prostatic calcifications10. CT not only allows precise identification of the calcification’s location within the prostate but also facilitates accurate measurement of its size. This study aims to leverage the advantages of CT imaging to determine the exact location and size of prostatic calcifications. Additionally, it seeks to assess the clinical significance of various factors associated with prostate calcifications, offering insights into their diagnostic and prognostic implications.
Methods
Study participants
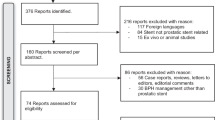
This retrospective study analyzed data from 5,492 male patients aged ≥ 18 years (range: 18–93 years) who underwent both enhanced and non-enhanced abdominal pelvic computed tomography (APCT) at the Department of Urology in our hospital between January 2010 and December 2020. Patients were excluded if they had a history of prostate cancer, previous prostatectomy, indwelling urethral catheter, severe imaging artifacts, or errors in imaging software. After applying these exclusion criteria, a total of 4,805 patients were included in the final analysis (Fig. 1).

Overview of patients.
Protocol for assessment of prostate calcification on APCT
Prostate calcifications were evaluated using multiple CT scanners (Brilliance iCT 256, Somatom Definition AS+, Somatom Definition Flash, and Somatom Force) with imaging parameters set to 100–120 kVp and slice thicknesses ranging from 2 to 3 mm. Calcifications were identified and measured in non-contrast abdominal pelvic computed tomography (APCT) axial images using a threshold value of ≥ 100 Hounsfield units (HU) through three-dimensional reconstruction with imaging software (SyngoVia, Siemens Healthineers, Germany)11,12. Only highlighted pixels within the prostate boundary were selected for analysis. Lesions with HU values < 100 were not classified as calcifications; however, these lesions were identified and classified separately if their boundaries were distinct from surrounding tissues. The locations of prostate calcifications were categorized into periurethral, central, transitional, and peripheral zones. Non-contrast APCT was utilized to determine the presence and volume of calcifications, while contrast-enhanced APCT was used to differentiate the transitional and peripheral zones for precise localization. To ensure diagnostic accuracy, two experienced specialists—a urologist (S. C. Kim) and a radiologist (T. Y. Lee)—independently reviewed the images. Diagnoses were made through cross-reading of another observer’s interpretations and double-reading of their own, performed under strict blinding to prior results. In cases of discrepancies, reexaminations were conducted to achieve consensus. The prostate calcification locations are illustrated in Fig. 2.

Zone classification for prostatic calcifications.
Clinical and laboratory measurements
Patient demographics, including age, medical history, and laboratory findings, were recorded. Urinary symptoms were assessed using the International Prostate Symptom Score (IPSS), which incorporates a quality-of-life (QoL) component to evaluate the impact of symptoms on patients’ daily lives. Prostate size was measured using TRUS. Prostatic calcifications were measured using a Picture Archiving and Communication System (PACS) measurement tool. Dimensions were reported in millimeters to one decimal place. The maximum anteroposterior diameter was measured on axial images, while the length and width were obtained from midsagittal images. Stone volume was calculated using the prolate ellipsoid formula (0.524 × height × width × length).13
Statistical analysis
Nominal variables were summarized as frequencies and percentages, while continuous variables were presented as mean values and interquartile ranges. The frequency of calcifications by location was illustrated using a Venn diagram. Differences based on calcification location and number were analyzed using either analysis of variance (ANOVA) or the Kruskal–Wallis test for continuous variables, depending on data distribution. Predictors of the IPSS were evaluated using linear regression analysis. Variables with a p-value < 0.2 in univariate analysis were included in the multivariate analysis to adjust for potential confounders. Statistical significance was set at p < 0.05. All statistical analyses were performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA).
Ethics statement
This retrospective observational study was approved by the Institutional Review Board (IRB) of Ulsan University Hospital (approval number: 2021-07-0732) and adhered to the principles outlined in the Declaration of Helsinki. Due to the retrospective nature of the study and the anonymization of included data, the IRB waived the requirement for informed consent.
Results
Participants
Among the 4,805 patients included in the analysis, 1,525 had no calcifications, 285 had calcifications with a Hounsfield unit (HU) < 100, and 2,995 had calcifications with HU ≥ 100. Table 1 presents the differences in age and clinical characteristics based on the presence or absence of prostate calcifications as observed on CT imaging. Patients with calcifications were, on average, older than those without calcifications. Notably, the group with calcifications of HU ≥ 100 had the highest mean age at 60.5 years (p < 0.001). No significant differences were observed in prostate-specific antigen (PSA) levels or prostate size among the groups. However, total, storage, and voiding scores on the International Prostate Symptom Score (IPSS) were significantly higher in patients with calcifications, with the highest scores recorded in the HU ≥ 100 group.
Characteristics of prostate calcification
The majority of calcifications, including duplicates, were located in the central zone (N = 2,375; 79.3%). The periurethral (N = 1,475; 48.6%) and transitional zones (N = 1,257; 42.0%) followed as the most frequently observed sites, while a small number were found in the peripheral zone (N = 28; 0.9%) (Fig. 3). One calcification was the most common, observed in 1,366 patients (45.6%), followed by two calcifications in 1,137 patients (38.0%), and three calcifications in 491 patients (16.4%). The average HU for calcifications was 172 ± 75.7, and the average calcification size was 187.6 mm2 (Table 2).

Venn diagram showing proportions by location of calcifications.
When calcifications were located in the peripheral zone, the mean age of patients was the highest, but the HU value was the lowest. Additionally, while calcifications in the peripheral zone had the largest size, there was no significant difference in the International Prostate Symptom Score (IPSS), suggesting that urinary symptoms are not influenced by the calcification location. As the number of calcifications increased, the mean age, HU, and calcification size showed a significant increase. However, there was no corresponding change in IPSS scores (Table 3).
Clinical significance of prostate calcification
Total International Prostate Symptom Score (IPSS) was significantly higher with increasing age and the presence of prostate calcifications. In the univariate analysis, Storage lower urinary tract symptoms (LUTS) also showed a significant increase with both age and calcifications. However, in the multivariate analysis, only age emerged as a significant factor influencing Storage LUTS. Voiding LUTS, on the other hand, significantly increased with both age and calcification in both the univariate and multivariate analyses. Therefore, both age and prostate calcification were identified as significant factors influencing urinary symptoms (Table 4).
Discussion
Prostate calcification is a common finding in middle-aged and older men, with incidence rates ranging from 7 to 70%, largely depending on the age of the study population3,14,15. In our study, the mean age of participants was 59 years, and approximately two-thirds of the cohort exhibited prostate calcifications. Notably, both the size and number of calcifications increased with age, which aligns with findings from previous studies9,16,17. Prostate calcification is most commonly associated with benign prostatic hyperplasia or chronic inflammation. The relationship between calcification and LUTS has been well-documented, though the underlying mechanism remains incompletely understood. One possible explanation is an inflammatory response. Histopathological studies often reveal lymphocytic and histiocytic infiltration of the prostate acinar glands in areas of calcification, which may create a microenvironment that perpetuates further inflammatory changes18,19. Prostate calcification causes inflammation by blocking the intraprostatic ducts, and this chronic inflammation is ultimately associated with calcification in the surrounding tissues. This can cause fibrosis, leading to tissue stiffness and LUTS19,20. In the multivariate analysis, age and calcification were significant factors affecting urinary symptoms.
Numerous studies have reported that the presence of prostate calcifications and their characteristics can influence urinary symptoms. In particular, calcifications located around the prostatic urethra can cause tissue stiffness, which exacerbates urinary symptoms8. Additionally, increasing calcification size has been shown to correlate with worsening urinary symptoms5. In our analysis, both the HU value and size of the calcifications varied according to their location within the prostate. However, no significant correlation was found between these characteristics and the IPSS. As age increased, there was a higher incidence of multiple calcifications, and the size of the calcifications also increased. Despite this, no correlation between the number or size of the calcifications and urinary symptoms was observed. This lack of correlation is likely due to the fact that not all participants in the study presented with urinary symptoms, leading to a smaller variation in IPSS scores, which made it difficult to detect significant differences. Similarly, it was difficult to identify a relationship between prostate volume and IPSS, likely because not all participants had benign prostatic hyperplasia or LUTS, resulting in minimal differences in prostate volume.
To date, most studies on prostate calcification have relied on TRUS for diagnosis8,9,16,21. However, TRUS is operator-dependent and may be limited in its ability to accurately diagnose and localize calcifications due to the noise generated behind them. In contrast, this study employed CT, which offers a standardized imaging modality that is independent of the operator. CT enables precise evaluation of not only the location, size, and number of calcifications but also the HU, which provides valuable information regarding the density of the lesions. MRI has limitations in detecting intraprostatic calcifications due to its sensitivity to variations in signal intensity and the small size of the lesions. Given these constraints, CT may offer a distinct advantage over MRI in identifying prostate calcifications, providing clearer, more accurate imaging for both diagnostic and clinical purposes10,22.
This study has several limitations. First, it was retrospective in nature, which inherently restricts the ability to establish causality and may introduce selection bias. Second, while we used the IPSS to assess the clinical significance of prostate calcification, it is important to note that calcifications can have varying clinical implications. LUTS can be caused by factors other than calcifications, which may have confounded our findings. Third, the study exclusively included patients who underwent CT scans in the urology department, regardless of their reason for seeking care. This limited our ability to detect significant differences in urinary symptoms, as the patient population may not have been fully representative of the broader group with prostate calcifications. Finally, we were unable to perform pathological evaluations to assess fibrosis or tissue stiffness surrounding the calcifications, which we hypothesize to be a major contributor to the worsening of LUTS in our study participants. Despite these limitations, our study provides valuable insights as one of the few to use CT for the assessment of prostate calcification. It represents a significant advancement in the accurate evaluation of prostate calcifications. Future large-scale, prospective studies are essential to further investigate the potential for preventing calcification by controlling the underlying inflammation, as well as to assess the efficacy of treatments aimed at removing calcifications.
Conclusions
CT can be effectively utilized to accurately assess the exact location, size, and number of prostate calcifications. Our findings indicate that the prevalence of prostate calcifications increases with age and that these calcifications are associated with worsening LUTS. However, further prospective studies are needed to validate the effectiveness of preventive strategies and treatment options for prostate calcification, particularly in alleviating associated symptoms.
Data availability
The data that support the findings of this study are available from the authors, but restrictions apply to the availability of these data, which were used under license from the Ulsan University Hospital for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission from the Ulsan University Hospital. If necessary, please contact the corresponding author by email (Taekmin Kwon; tmkwon@uuh.ulsan.kr).
References
Dell’Atti, L., Galosi, A. B. & Ippolito, C. Prostatic calculi detected in peripheral zone of the gland during a transrectal ultrasound biopsy can be significant predictors of prostate cancer. Arch. Ital. Urol. Androl. 88, 304–307. https://doi.org/10.4081/aiua.2016.4.304 (2016).
Park, B. & Choo, S. H. The burden of prostatic calculi is more important than the presence. Asian J. Androl. 19, 482–485. https://doi.org/10.4103/1008-682X.181193 (2017).
Hyun, J. S. Clinical significance of prostatic calculi: A review. World J. Mens. Health 36, 15–21. https://doi.org/10.5534/wjmh.17018 (2018).
Hong, C. G. et al. The prevalence and characteristic differences in prostatic calcification between health promotion center and urology department outpatients. Korean J. Urol. 53, 330–334. https://doi.org/10.4111/kju.2012.53.5.330 (2012).
Kim, W. B., Doo, S. W., Yang, W. J. & Song, Y. S. Influence of prostatic calculi on lower urinary tract symptoms in middle-aged men. Urology 78, 447–449. https://doi.org/10.1016/j.urology.2010.12.056 (2011).
Chen, T. et al. Clinical correlation of prostatic calculi with semen parameters in adult men with fertility intention. Am. J. Mens. Health 13, 1557988319852018. https://doi.org/10.1177/1557988319852018 (2019).
Dessombz, A., Meria, P., Bazin, D. & Daudon, M. Prostatic stones: evidence of a specific chemistry related to infection and presence of bacterial imprints. PLoS One 7, e51691. https://doi.org/10.1371/journal.pone.0051691 (2012).
Han, J. H. et al. Is periurethral calcification associated with urinary flow rate and symptom severity in men with lower urinary tract symptoms-benign prostatic hyperplasia? A retrospective review. Urology 85, 1156–1161. https://doi.org/10.1016/j.urology.2015.01.038 (2015).
Meng, J. et al. The prevalence and risk factors of prostatic calculi in Han Chinese: A cross-sectional study based on health examinations. Aging Male 23, 887–892. https://doi.org/10.1080/13685538.2019.1620203 (2020).
Straub, S. et al. Potential of quantitative susceptibility mapping for detection of prostatic calcifications. J. Magn. Reson. Imaging 45, 889–898. https://doi.org/10.1002/jmri.25385 (2017).
Adams, L. C. et al. Assessment of intracranial meningioma-associated calcifications using susceptibility-weighted MRI. J. Magn. Reson. Imaging 46, 1177–1186. https://doi.org/10.1002/jmri.25614 (2017).
Azad, R., Mittal, P., Malhotra, A. & Gangrade, S. Detection and differentiation of focal intracranial calcifications and chronic microbleeds using MRI. J. Clin. Diagn. Res. 11, TC19–TC23. https://doi.org/10.7860/JCDR/2017/24076.9846 (2017).
Park, M. C. et al. Effects of metabolic syndrome on renal stone progression. World J. Urol. 40, 1845–1851. https://doi.org/10.1007/s00345-022-04047-7 (2022).
Sfanos, K. S., Wilson, B. A., De Marzo, A. M. & Isaacs, W. B. Acute inflammatory proteins constitute the organic matrix of prostatic corpora amylacea and calculi in men with prostate cancer. Proc. Natl. Acad. Sci. U. S. A. 106, 3443–3448. https://doi.org/10.1073/pnas.0810473106 (2009).
Shoskes, D. A., Lee, C. T., Murphy, D., Kefer, J. & Wood, H. M. Incidence and significance of prostatic stones in men with chronic prostatitis/chronic pelvic pain syndrome. Urology 70, 235–238. https://doi.org/10.1016/j.urology.2007.04.008 (2007).
Yu, S. H., Lim, D. G. & Kim, S. O. Clinical significance of distally located periurethral calcification in patients with lower urinary tract symptoms of benign prostate hyperplasia. Asian J. Androl. 25, 361–365. https://doi.org/10.4103/aja202245 (2023).
Zhang, X. M. et al. Prevalence of and associated factors for prostate calcification in >/=40-year-old males with benign prostatic enlargement. Zhonghua Nan Ke Xue 28, 579–584 (2022).
Untergasser, G., Madersbacher, S. & Berger, P. Benign prostatic hyperplasia: Age-related tissue-remodeling. Exp. Gerontol. 40, 121–128. https://doi.org/10.1016/j.exger.2004.12.008 (2005).
Bianchi-Frias, D. et al. The effects of aging on the molecular and cellular composition of the prostate microenvironment. PLoS One https://doi.org/10.1371/journal.pone.0012501 (2010).
Gandaglia, G. et al. The role of chronic prostatic inflammation in the pathogenesis and progression of benign prostatic hyperplasia (BPH). BJU Int. 112, 432–441. https://doi.org/10.1111/bju.12118 (2013).
Cai, T. et al. Prostate calcifications: A case series supporting the microbial biofilm theory. Investig. Clin. Urol. 59, 187–193. https://doi.org/10.4111/icu.2018.59.3.187 (2018).
Kan, H. et al. Delineation of prostatic calcification using quantitative susceptibility mapping: Spatial accuracy for magnetic resonance-only radiotherapy planning. J. Appl. Clin. Med. Phys. 23, e13469. https://doi.org/10.1002/acm2.13469 (2022).
Author information
Authors and Affiliations
Contributions
Research conception and design: Seong Cheol Kim and Taekmin Kwon. Data acquisition: Ji Hyung Yoon, Sungchan Park, Kyung Hyun Moon, and Sang Hyeon Cheon. Statistical analysis: Tae Young Lee, Seong Cheol Kim and Taekmin Kwon. Data analysis and interpretation: Seong Cheol Kim and Tae Young Lee Drafting of the manuscript: Seong Cheol Kim and Taekmin Kwon. Critical revision of the manuscript: Seong Cheol Kim and Taekmin Kwon Administrative, technical, or material support: Woocheol Kang, Hoyoung Bae Supervision: Tae Young Lee and Taekmin Kwon. All authors reviewed the manuscript Approval of the final manuscript: Seong Cheol Kim and Taekmin Kwon.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
The requirement for informed consent was waived by the Institutional Review Board of Ulsan University Hospital given the retrospective study design and the anonymization of the data included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kim, S.C., Lee, T.Y., Kang, W. et al. Diagnosis and clinical significance of prostate calcification using computed tomography. Sci Rep 15, 4689 (2025). https://doi.org/10.1038/s41598-025-88320-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88320-w
