
Abstract
To investigate sex differences in liver disease development and prognosis in individuals with HIV and HBV co-infection. This study comprised 752 HIV/HBV co-infected people who were diagnosed with HIV and started on combination antiretroviral therapy (cART) between January 31st, 2015 and January 31st, 2023. Their clinical data, including CD4+ T lymphocyte counts, HBV-DNA, and FIB-4 scores, were tracked once a year. The prognosis was determined during the long-term surveillance period. Risk factors related with the progression of liver diseases were included in both univariable and multivariable logistic regression. Then, sex differences in CD4+ T lymphocyte counts, HBV-DNA, FIB-4 scores, changes in liver fibrosis levels, and prognosis were investigated. Multivariable logistic regression analysis identified male as an independent risk factor for liver disease progression. Compared to the male group, the female group had a significantly greater decline of HBV DNA levels at years 1, 2, 3, 3–5, and > 5 post-cART. At each assessment point, the female group showed a significantly greater rise in CD4+ T lymphocyte counts than the male group based on their respective baseline values. Furthermore, females had greater CD4+ T lymphocyte counts and a lower prevalence of liver cirrhosis than males throughout the study period. Compared to female, higher incidence of end-stage-liver disease (1.190/100 person-years vs 0.714/100 person-years), higher all-cause mortality (0.440/100 person-years vs 0.148/100 person-years) and higher mortality associated with end-stage-liver diseases (0.273/100 person-years vs 0.074/100 person-years) were found in male. Among individuals with HIV and HBV coinfection, males had a worse therapeutic effect of HBV-active therapy and poorer prognosis than females.
Similar content being viewed by others


Introduction
Hepatitis B virus (HBV) and human immunodeficiency virus (HIV) infection are both major public health issues worldwide. Co-infections of HBV and HIV are common due to similar routes of transmission1, which varied markedly from 5 to 30% in different regions of the world2,3,4. Studies found that co-infection with HIV and HBV was associated with an increased risk of mortality and liver-related consequences5.
Chronic hepatitis B is a condition that affects men more than women6. Males are at least two to three times more likely to develop HCC than females7. Males had HCC at a younger age than females, and they had a higher proportion of early-stage tumors when diagnosis8. Furthermore, the clinical course and prognosis of HCC caused by HBV infection appear to be significantly worse in men than in women. Male HCC progresses more aggressively than female HCC, resulting in a worse prognosis and a mortality rate that is 2–3 times higher7,8. The causes of sex disparities in HBV infection-related liver illness have already been reported. The inhomogeneous distribution between male and female had been explained by the varied prevalence of risk factors (e.g., alcoholism). Furthermore, because the liver is now recognized as a sexually dimorphic that is very vulnerable to interactions with estrogens and androgens9, sex hormones may play a substantial role. However, data on the role of sex in disease progression and outcome among individuals with HIV and HBV coinfection in resource-limited locations areas remains limited.
The goal of this study was to determine whether sex differences were an independent predictor of liver disease progression in HIV/HBV co-infected individuals. Then, using long-term follow-up, we attempted to investigate sex differences in HBV replication, immunological reconstruction, liver fibrosis, and prognostic alterations.
Methods
Study design and population
This was a retrospective study conducted at Zhongnan Hospital of Wuhan University. All data were collected from patients at Zhongnan Hospital of Wuhan University. For at least 6 months, all of the participants had tested positive for anti-HIV and hepatitis B surface antigen (HBsAg). Patients with HAV, HCV or HEV infections were excluded. Other exclusion criteria were any complications from severe heart, lung, kidney, brain, or blood diseases, as well as other serious systemic diseases; severe neurological or psychological illness; and pregnancy or lactation. A consort chart was used to display the objects and data collected for this investigation (Fig. 1).

A consort chart of this study.
This study was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was approved by the Institutional Review Board of Zhongnan Hospital of Wuhan University. Informed consent was obtained from all participants.
Data collection
Demographic data (such as age, sex, marital and financial status, height and weight), medical history (such as history of chronic disease, family history of liver disease), alcohol consumption history, HIV related indexes (such as baseline CD4+ T lymphocyte counts, changes in CD4+ T lymphocyte counts, antiretroviral drugs), HBV related indexes (such as HBeAg status, levels of HBV DNA, ALT and platelet, imaging findings of the liver), and compliance were collected.
Laboratory testing
In a stable situation, HBV DNA and CD4+ T lymphocyte counts were measured every 6–12 months, whereas alanine aminotransferase (ALT), aspartate aminotransferase (AST), and platelets were measured every 3–6 months. If there is a medical requirement, the detection frequency of specific indications will be increased accordingly. The average values of HBV DNA, CD4+ T lymphocyte counts and transaminase levels in the current year were taken for analysis.
HBV DNA quantification was performed by using PCR-Fluorescence detection kits for hepatitis B viral nucleotides (QIAGEN, Hilden, Germany), and the minimum detection limit was 20 IU/ml. Detectable HBV DNA was defined as ≥ 20 IU/mL.
CD4+ T lymphocyte counts (cells/μL) was measured by multiple-color flow cytometry with human monoclonal anti-CD3-fluorescein isothiocyanate (FITC), anti-CD4-phycoerythrin (PE) and anti-CD8-allophycocyanin (APC) antibodies (BD Multitest) according to the manufacturer’s instructions. The cells were autoanalyzed on a BD FACS Canto II flow cytometry system (BD Biosciences).
Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were measured using Architect c8000 (Abbott Laboratories, USA), and platelet count were measured using the ABX Pentra XL80 (Horiba, Japan). Age was calculated based on date of birth.
Definitions
End-stage-liver diseases (ESLD) were liver cirrhosis, hepatocellular carcinoma and severe reactivation of apreexisting chronic hepatitis B in this study. Reference standards for ESLD diagnosis were similar to those in Matthews’ study10. Liver disease progression was defined as the emergence of an ESLD event in this study.
The following published serum models were used to assess liver fibrosis11. FIB-4: Age (years) × AST (U/L) / ALT (U/L)1/2 × PLT × 109. Refer to prior study12, FIB-4 score > 3.25 was representative of advanced fibrosis or cirrhosis.
Causes of death were ascertained according to medical documents and death certificates. An ESLD-related death was defined as one that happened after ESLD hospitalization or was listed on a death certificate. Mortality associated with ESLD = Number of deaths due to ESLD in a given period ÷ Total observation person-years in the same period × 100%.
Statistical analysis
Categorical variables were described as frequency rates and percentages, and quantitative data were expressed as mean ± SD. Comparisons between groups were analyzed by chi-square test or Fisher’s exact test for categorical variables and by Student’s t-test for quantitative variables.
All variables as potential predictors for the development of liver diseases were analyzed using univariable and stepwise multivariable logistic regression models. The conventional ART regimen includes three medications with anti-HIV activity, some of which also have anti-HBV activity, such as TDF, 3TC, and FTC. In the analysis of risk factors related with the progression of liver diseases, HBV-active therapy and antiretroviral medicines were chosen as two distinct variables to minimize the unpredictable effects of patients’ pharmaceutical choices on liver disease outcomes. Variables with a P-value < 0.10 in univariable logistic regression models were considered for inclusion in the multivariable model. Each covariate was assigned an odds ratio (OR) and a 95% confidence interval (95% CI). A factor with an OR > 1 is a risk factor for liver disease development, while an OR < 1 indicates a protective factor. The 95% CI is an estimate of the population mean based on the mean of the specimen data.
Changes in HBV DNA levels, CD4 counts, and FIB-4 scores at various ART time points by sex were expressed as mean ± SD. To control for other confounding factors, the generalized estimating equations (GEE) model was employed to evaluate longitudinal changes in the aforementioned outcomes. Based on the assumption that the P-value was statistically significant, OR > 1 showed that the observation measure increased at a treatment time point relative to the prior treatment time point. OR < 1 implies a decrease in the observed indication. The 95% CI is an estimate of the population mean based on the mean of the specimen data.
Kaplan–Meier analysis was used to estimate the incidence of end-stage liver diseases (ESLD), mortality of all-cause and ESLD-related death by sex. The log-rank test was used to assess the difference between the survival curves. All tests were two-sided and a P-value < 0.05 was taken as significant.
All the analysis were performed using SPSS Statistics version 27.0 software. GraphPad Prism Version 8 was used to analyze and generate figures from the clinical follow-up data.
Results
Characteristics of HBV/HIV co-infected individuals grouped by sex
A total of 752 HIV/HBV co-infected persons were enrolled in the study, with 588 (78.2%) males and 164 (21.8%) females. The median age was 42 (IQR: 35–58) years, the baseline CD4+ T lymphocyte counts was 140 (IQR, 35–367) cells/mm3, 18.8% (141/752) were HBeAg positive, the proportion of detectable HBV DNA was 61.2% (460/752). The median follow-up time was 4(2–6) years in this study. Of all participants, 86.8% (653/752) were on combination antiretroviral therapy (cART) during the follow-up time, 86.2% (648/752) had complete suppression of HIV RNA, 84.4% (635/752) had suppressed HBV DNA(< 20 IU/mL), 40.4% (304/752) had Lamivudine (3TC)-based ART regimen, 46.4% (349/752) had Tenofovir disoproxil fumarate (TDF)/3TC-based ART regimen.
As shown in Table 1, there was no significant difference in age, baseline CD4+ T lymphocyte counts, ART coverage, HBeAg positive rate, proportion of complete suppression of HIV RNA and HBV DNA, proportion of 3TC and TDF/3TC-based ART regimen, or median duration of ART between male and female groups, whereas males had a higher proportion of detectable HBV DNA at baseline (63.6% vs 52.4%).
Risk factors associated with the progression of liver diseases
Univariable logistic regression identified risk factors for liver disease progression, including age > 50 years at baseline, male gender, BMI > 24 kg/m2, alcohol consumption, baseline CD4+ T lymphocyte counts < 200 cells/ul, detectable HBV DNA, baseline ALT more than twice the upper limit of normal values, hypoplatelet count at baseline, virological rebound of HBV DNA, and poor compliance. In contrast, CD4+ T lymphocyte counts change ≥ 150 cells/ul within 3 months, undetectable HBV DNA levels at year 1 following HBV-active therapy, HBV-active therapy, 3TC-containing therapy, and TDF/3TC-containing therapy were protective factors for progression of liver disease (Table 2).
Multivariable logistic regression further identified male, BMI > 24 kg/m2, baseline CD4+ T lymphocyte counts < 200 cells/ul, detectable HBV DNA at baseline as independent risk factors related to the progression of liver disease. Conversely, CD4+ T lymphocyte counts change ≥ 150 cells/ul within 3 months, TDF/3TC-containing therapy, and undetectable HBV DNA levels at year 1 post HBV-active therapy had a favorable effect against the progression of liver disease (Table 2).
Sex difference of the changes of HBV replication during cART
Table 3 shows how the GEE was used to compare the differences in detectable HBV DNA levels between the female and male groups at different study time periods. In comparison to the male group, the female group exhibited a considerably higher reduction throughout all evaluation time points, with a between-group difference in changes from baseline to T1 (at year 1) of 0.15 times (95% CI, 0.11 to 0.21; P < 0.001); to T2 (at year 2), 0.17 times (95% CI, 0.11 to 0.27; P < 0.001), to T3 (at year 3), 0.27 times (95% CI, 0.13 to 0.58; P = 0.001); to T4 (at year 3–5), 0.31 times (95% CI, 0.18 to 056; P < 0.001); and to T5 (at year > 5), 0.42 times(95% CI, 0.18 to 0.95; P = 0.038).
Sex difference of the changes of CD4+ T lymphocyte counts during cART
As indicated in Table 3, CD4+ T lymphocyte counts grew in both groups over time and showed significant differences. The female group demonstrated a considerably larger augmentation than the male group during the cART period, with a between-group difference in changes from baseline to T1 (OR 1.44; 95% CI 1.36 to 1.53, P < 0.001); to T2 (OR 1.56; 95% CI 1.45 to 1.68, P < 0.001); T3 (OR 1.63; 95% CI 1.50 to 1.78, P < 0.001); T4 (OR 1.75; 95% CI 1.61 to 1.89, P < 0.001); T5 (OR 2.00; 95% CI 1.84 to 2.18, P < 0.001).
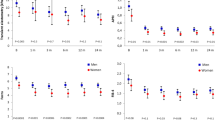
Figure 2A and B show variations in CD4+ T lymphocyte counts over time in males and females, respectively. Then, in Fig. 2C, a male–female comparison was shown, revealing that the trend line of CD4+ T lymphocyte counts in female was higher than in male at all time points without crossover.

Sex difference of the changes of CD4+ T lymphocyte counts during cART. (A) Changes in male CD4+ T lymphocyte counts during ART; (B) Changes in female CD4+ T lymphocyte counts during ART; (C) A trend test comparison of changes in male and female CD4+ T lymphocyte counts during ART.
Sex difference of the changes of FIB-4 scores and liver fibrosis levels during cART
As demonstrated in Table 3, although FIB-4 scores decreased at all time points when compared to the baseline, there was no significant difference in the rate of decline between males and females. However, liver fibrosis was detected in 42.8% of males and 33.3% of females who had not received cART. As illustrated in Fig. 3A and B, the difference was large. Among cART patients, the overall proportion of liver fibrosis fell to 22.1% and 12.2% in males and females, respectively, with a significant difference between the two groups, as shown in Fig. 3C and D. Males exhibited a higher proportion of liver fibrosis than females at years 1, 2, 3, 3–5, and > 5 after cART (Fig. 3E).

Sex difference of the changes of liver fibrosis levels during cART. (A) A comparison of liver fibrosis percentage in ART-naive male and female using Peason Chi-Square; (B) A comparison of liver fibrosis percentage in ART-treated male and female using Peason Chi-Square; (C) Distribution of different degrees of liver fibrosis in male and female during ART treatment using descriptive analysis.
Sex difference of the prognosis of persons with HIV/HBV co-infection
The median follow-up time was 4(2–6) years in this study. The person-years of follow-up observation were 13,191 and 4064 in male and female, respectively. The number of ESLD events in males was 157, whereas females had 29. The incidence of ESLD was greater in males than in females (1.190/100 person-years vs 0.714/100 person-years). All-cause deaths were 58 and 6 in males and females, respectively, and ESLD caused 36 and 3 deaths. Males had greater mortality of all-cause and ESLD-related death than females (0.440/100 and 0.273/100 person-years vs 0.148/100 and 0.074/100 person-years). The result of survival analysis was shown in Fig. 4.

Sex difference in the prognosis of persons with HIV/HBV co-infection. (A) Comparison of the incidence of end-stage liver disease in male and female using Kaplan–Meier analysis; (B) Comparison of all-cause mortality in male and female using Kaplan–Meier analysis; (C) Comparison of mortality associated with end-stage liver disease in male and female using Kaplan–Meier analysis.
Discussion
Studies have shown that males have a higher incidence of AIDS than females in many countries13,14. According to a study conducted in Zhejiang, China, newly infected males with HIV are 4.64 times more common than females, and males have a higher overall AIDS incidence15. In this HIV/HBV coinfection cohort during 4 years of median follow-up time, males were found to have a significantly less decline of HBV DNA levels, a significantly less rise in CD4+ T lymphocyte counts, more liver fibrosis, and higher all-cause and liver-related mortality than females. The sex difference of the diseases progression was significant.
It was discovered that 10% of HIV/HBV co-infected individuals had persistently detectable HBV DNA after a short follow-up period16, although persistent HBV was extremely rare after 5 years of cART17. Previous studies found that 3TC-resistance mutations occurred at an annual rate of 15–20% in HIV/HBV co-infected patients using cART18,19,20,21. Due to limited resources, several patients in this study were given cART with only one anti-HBV activity. In this context, we can clearly see that HBV replication levels following therapy are significantly lowered in both male and female groups, while they are still not entirely controlled below the detection threshold. The failure to reduce HBV replication may attribute to the disadvantage of 3TC as a single anti-HBV medication. Some studies have demonstrated that the baseline level of HBV-DNA should be taken into account when deciding on treatment options for patients with HIV/HBV co-infection22,23. We anticipated that our study’s reduced proportion of HBeAg-negative disease and HBV DNA levels < 20,000 IU/ml, relative to resource-rich settings24,25,26,27, could explain treatment outcomes in this cohort. This study revealed that males had a slower reduction in HBV levels than females. The topic of whether males’ reactions to anti-HBV medicines were delayed, or whether resistance to 3TC developed earlier due to other reasons such as compliance, merits more investigation.
Previous studies found that HIV might infect hepatocytes and activate hepatic stellate cells28,29, potentially causing liver damage. Furthermore, CD4+ T cell concentration has been found to be negatively associated with liver fibrosis30. A study indicated that immunodeficiency, defined as a CD4+ T cell count < 350/mm3, results in a higher overall fibrosis score and worse chances of fibrosis reversal when on cART31. Based on these findings, the CD4+ T cell count in males was lower than in females at various stages of cART in this study, resulting in a higher incidence of liver fibrosis and ESLDs, as well as liver-related mortality in males. The majority of studies found that males had a more advanced clinical stage and immunosuppression than females32, and gender can influence the proportion of patients treated late33,34. In this study, the baseline CD4+ T cell count in males was substantially identical to that in females, contradicting the majority of previous studies. Nonetheless, males showed a smaller rise in CD4+ T cell count in this study, showing that they were less efficient than females in immunological reconstitution following cART. Some studies found that antiviral efficacy and safety differed between males and females35,36,37,38. In a prospective research37, males were four times more likely than females to attain a study endpoint, which was defined as the time from baseline to a 50% decline in CD4+ T lymphocyte counts,AIDS onset, or death. Furthermore, females appeared to do slightly better in terms of CD4+ T lymphocyte counts response than males on ZDV and ZDV/ddI treatment37, which is consistent with our findings, despite the fact that the two studies used different cART regimens. As previously noted, sex inequalities in response to cART can be related to differences in absorption, blood flow, sex-specific cytochrome p450 isoenzymes, drug half-life, and pharmacokinetics differences caused by hormonal changes during the menstrual cycle39,40. The effect of androgen/estrogen on cART medication absorption and metabolism is unknown at the moment and will be researched further. In the future, personalized treatment methods will incorporate sex-specific antiviral regimen recommendations.
Liver fibrosis is the normal progression of chronic liver disease into liver cirrhosis. The FIB-4 score was used as a non-invasive fibrosis marker in patients with HBV monoinfection and HIV/HBV co-infection. Males showed a higher rate of advanced liver fibrosis than females, both before and after cART. As seen in HBV-monoinfected patients, higher HBV DNA replication levels were associated with a higher overall fibrosis score41,42. The finding was likewise confirmed in the HIV/HBV co-infected group. Furthermore, in HBV-monoinfected patients, a connection between body mass index (BMI) and liver fibrosis was established43. The fact that males have a higher BMI than females may contribute to the higher prevalence of male liver fibrosis, which has yet to be shown in the context of HIV. Alcohol consumption, which is more common among males, is also a major factor to liver fibrosis. Although all HIV-infected patients are advised to avoid alcohol throughout cART, perfect compliance is rarely guaranteed. According to recent findings, HIV can stimulate hepatic stellate cells and may infect hepatocytes28,29. Another study found that HIV infection was independently associated with an increased marker of liver fibrosis30. As a result, male participants in this study had reduced CD4 levels caused directly by HIV infection, which contributed to greater liver fibrosis.
Since the advent of cART, mortality rates for AIDS-related events have declined significantly, while there has been a discernible shift towards a higher proportion of fatalities due to non-AIDS-related illnesses, such as liver ailments, over time44,45,46,47. People with chronic HBV and HIV infections are more likely to develop liver cirrhosis and hepatocellular carcinoma, resulting in higher mortality rates than those infected with just HIV or HBV48,49. The complex relationship between HIV and hepatic viral infections is one of the major contributors to the increased cancer burden, as well as the morbidity and mortality of HIV patients, but the mechanisms underlying this interaction are still being investigated50,51. People living with HIV have much higher liver-related death rates than the general population52. Males experienced worse outcomes than females in terms of ESLD-related morbidity and death, as well as all-cause mortality. The results were similar with those of a nationwide population-based study in Brazil53. Males were more likely to have behavioral factors such as problematic drug use, heavy alcohol consumption and smoking, and obesity, which may explain the difference in disease prognosis between males and females. We considered that the more relevant and directly associated rationale was the greater incidence of liver fibrosis caused by delayed full suppression of HBV replication and slower CD4+ T cell count exansion after cART in males compared to females , as discussed earlier in this study.
In conclusion, given the findings of this study on the course and prognosis of liver disease in HIV/HBV coinfected males during ART period compared to females, we hold the opinion that in medical resources limited areas, personalized treatment options for HIV/HBV coinfected males should be considered. For male HIV/HBV co-infected individuals, drugs with strong anti-HBV and HIV properties should be considered as the optimal option for the initial treatment strategy, and non-invasive liver fibrosis evaluation indexes such as the FIB-4 score should be used to appropriately increase the frequency of liver disease monitoring. It can be viewed as a technique for lowering the incidence and fatality rates of end-stage liver disease in HIV/HBV co-infected males. Especially for patients whose HBV DNA is still not controlled below the detection limit after one year of ART treatment and/or CD4+ T lymphocyte counts have increased by less than 150 cells/ul, the ART combination regimen with stronger anti-HBV and anti-HIV effects should be adjusted as soon as possible.
This study provides some valuable clinical insights, particularly in the rarely addressed sex differences in HIV and HBV coinfection population. More than half of the individuals in this study were born during a period when there was no active hepatitis B active immunization, and more than 80% of the subjects had a clear family history of hepatitis B infection, indicating that the majority of the subjects contracted HBV as children. One of the study’s highlights is that the duration of HBV infection was long enough to see the differential influence of sex on the prognosis of liver disease. Another strength is the comparison of males and females in terms of the dynamic evolution of HBV DNA, CD4+ T lymphocyte levels, and FIB-4 scores throughout cART durations. However, we acknowledge that our study has certain limitations. First, because this was a retrospective cohort study, we were unable to provide complete data for all participants during the monitoring period, which reduced the continuity of a few data points to some extent. Second, due to the low acceptability of liver biopsy and the economic burden, the FIB-4 index was used to assess liver fibrosis in this study, which may not adequately reflect the liver’s pathological condition. Finally, despite the small sample size, this study did not include the objective presence of occult hepatitis B infections that tested negative for HBsAg but positive for HBV DNA.
Conclusions
In conclusion, we found illness progression and prognosis in HIV/HBV co-infected persons during the course of the study, with a clear sex difference. Males experienced a smaller reduction in HBV DNA levels, a narrower growth range for CD4+ T lymphocyte counts, and a higher incidence of liver cirrhosis. Furthermore, males had a worse prognosis than females in terms of morbidity and mortality from ESLD, as well as overall mortality.
Data availability
Data is provided within the manuscript.
References
Koziel, M. J. & Peters, M. G. Viral hepatitis in HIV infection. N Engl. J. Med. 356(14), 1445–1454. https://doi.org/10.1056/NEJMra065142 (2007).
Rong-Rong, Y., Xi-En, G., Shi-Cheng, G. & Yong-Xi, Z. Interaction of hepatitis B and C viruses in patients infected with HIV. J. Acquir. Immune Defic. Syndr. 48(4), 505–506. https://doi.org/10.1097/QAI.0b013e31816de23c (2008).
Singh, K. P. et al. HIV-hepatitis B virus coinfection: Epidemiology, pathogenesis, and treatment. AIDS 31, 2035–2052. https://doi.org/10.1097/QAD.0000000000001574 (2017).
Coffie, P. A. et al. Prevalence of hepatitis B and delta according to HIV-type: A multi-country cross-sectional survey in West Africa. BMC Infect. Dis. 17, 466. https://doi.org/10.1186/s12879-017-2568-5 (2017).
Thio, C. L. et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 360(9349), 1921–1926. https://doi.org/10.1016/s0140-6736(02)11913-1 (2002).
Nevola, R. et al. Gender differences in the pathogenesis and risk factors of hepatocellular carcinoma. Biology (Basel) 12(7), 984. https://doi.org/10.3390/biology12070984 (2023).
Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249. https://doi.org/10.3322/caac.21660 (2021).
Rich, N. E. et al. Sex disparities in presentation and prognosis of 1110 patients with hepatocellular carcinoma. Aliment. Pharmacol. Ther. 52(4), 701–709. https://doi.org/10.1111/apt.15917 (2020).
Roy, A. K. & Chatterjee, B. Sexual dimorphism in the liver. Annu. Rev. Physiol. 45, 37–50. https://doi.org/10.1146/annurev.ph.45.030183.000345 (1983).
Matthews, G. V., Cooper, D. A. & Dore, G. J. Improvements in parameters of end-stage liver disease in patients with HIV/HBV-related cirrhosis treated with tenofovir. Antivir. Ther. 12, 119–122 (2007).
Sterling, R. K. et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 43, 1317–1325. https://doi.org/10.1002/hep.21178 (2006).
Vallet-Pichard, A. et al. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection comparison with liver biopsy and fibrotest. Hepatology 46(1), 32–36. https://doi.org/10.1002/hep.21669 (2007).
Cornell, M., Myer, L., Kaplan, R., Bekker, L. G. & Wood, R. The impact of gender and income on survival and retention in a south African antiretroviral therapy programme. Trop. Med. Int. Health 14(7), 722–731 (2009).
Takarinda, K. C. et al. Gender-related differences in outcomes and attrition on antiretroviral treatment among an HIV-infected patient cohort in Zimbabwe: 2007–2010. Int. J. Infect. Dis. 30, 98–105 (2015).
Lu, Z. et al. Analysis on the trend of AIDS incidence in Zhejiang, China based on the age-period-cohort model (2004–2018). BMC Public Health 21(1), 1077 (2021).
Audsley, J. et al. Effects of long-term tenofovir-based combination antiretroviral therapy in HIV-hepatitis B virus coinfection on persistent hepatitis B virus viremia and the role of hepatitis B virus quasispecies diversity. AIDS 30(10), 1597–1606. https://doi.org/10.1097/QAD.0000000000001080 (2016).
Audsley, J. et al. Long-term TDF-inclusive ART and progressive rates of HBsAg loss in HIV-HBV coinfection-lessons for functional HBV cure?. J. Acquir. Immune Defic. Syndr. 84(5), 527–533. https://doi.org/10.1097/QAI.0000000000002386 (2020).
Wensing, A. M. et al. 2022 update of the drug resistance mutations in HIV-1. Top Antivir. Med. 30(4), 559–574 (2022).
Liaw, Y. F. et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2012 update. Hepatol. Int. 6, 531–561. https://doi.org/10.1007/s12072-012-9365-4 (2012).
Iser, D. M. & Sasadeusz, J. J. Current treatment of HIV/hepatitis B virus coinfection. J. Gastroenterol. Hepatol. 23, 699–706. https://doi.org/10.1111/j.1440-1746.2008.05382.x (2008).
Matthews, G. V. et al. Characteristics of drug resistant HBV in an international collaborative study of HIV-HBV-infected individuals on extended lamivudine therapy. AIDS 20, 863–870. https://doi.org/10.1097/01.aids.0000218550.85081.59 (2006).
Thio, C. L. et al. Comparison of HBV-active HAART regimens in an HIV-HBV multinational cohort: Outcomes through 144 weeks. AIDS 29(10), 1173–1182. https://doi.org/10.1097/QAD.0000000000000686 (2015).
Li, Y. et al. Lamivudine monotherapy-based cART is efficacious for HBV treatment in HIV/HBV coinfection when baseline HBV DNA <20,000 IU/mL. J. Acquir. Immune Defic. Syndr. 72(1), 39–45. https://doi.org/10.1097/QAI.0000000000000927 (2016).
Thio, C. L. et al. Characterization of HIV-HBV coinfeciton in a multinational HIV-infected cohort. AIDS 27, 191–201. https://doi.org/10.1097/QAD.0b013e32835a9984 (2010).
Idoko, J. et al. Impact of hepatitis B virus infection on human immunodeficiency virus response to antiretroviral therapy in Nigeria. Clin. Infect. Dis. 49, 1268–1273. https://doi.org/10.1086/605675 (2009).
Hoffmann, C. J. et al. Hepatitis B virus infection and response to antiretroviral therapy (ART) in a South African ART program. Clin. Infect. Dis. 47, 1479–1485. https://doi.org/10.1086/593104 (2008).
Ive, P. et al. Low prevalence of liver disease but regional differences in HBV treatment characteristics mark HIV/HBV co-infection in a South African HIV clinical trial. PLoS One 8, e74900. https://doi.org/10.1371/journal.pone.0074900 (2013).
Blackard, J. T. & Sherman, K. E. HCV/HIV co-infection: time to re-evaluate the role of HIV in the liver?. J. Viral Hepat. 15, 323–330. https://doi.org/10.1111/j.1365-2893.2008.00970.x (2008).
Tuyama, A. C. et al. Human immunodeficiency virus (HIV)-1 infects human hepatic stellate cells and promotes collagen I and monocyte chemoattractant protein-1 expression: Implications for the pathogenesis of HIV/hepatitis C virus-induced liver fibrosis. Hepatology 52, 612–622. https://doi.org/10.1002/hep.23679 (2010).
Price, J. C. et al. HIV monoinfection is associated with increased aspartate aminotransferase-to-platelet ratio index, a surrogate marker for hepatic fibrosis. J. Infect. Dis. 205(6), 1005–1013. https://doi.org/10.1093/infdis/jir885 (2012).
Boyd, A. et al. Liver fibrosis changes in HIV-HBV-coinfected patients: clinical, biochemical and histological effect of long-term tenofovir disoproxil fumarate use. Antivir. Ther. 15(7), 963–974. https://doi.org/10.3851/IMP1649 (2010).
Ngongo, N. M. et al. Longitudinal analysis of sociodemographic, clinical and therapeutic factors of HIV-infected individuals in Kinshasa at antiretroviral therapy initiation during 2006–2017. PLoS One 16(11), e0259073. https://doi.org/10.1371/journal.pone.0259073 (2021).
Luma, H. N. et al. Late presentation to HIV/AIDS care at the Douala general hospital, Cameroon: Its associated factors, and consequences. BMC Infect. Dis. 18(1), 298. https://doi.org/10.1186/s12879-018-3204-8 (2018).
Benzekri, N. A. et al. Prevalence, predictors, and management of advanced HIV disease among individuals initiating ART in Senegal, West Africa. BMC Infect. Dis. 19(1), 261. https://doi.org/10.1186/s12879-019-3826-5 (2019).
Campbell, T. B. et al. Efficacy and safety of three antiretroviral regimens for initial treatment of HIV-1: A randomized clinical trial in diverse multinational settings. PLoS Med. 9(8), e1001290. https://doi.org/10.1371/journal.pmed.1001290 (2012).
Moore, R. D., Fortgang, I., Keruly, J. & Chaisson, R. E. Adverse events from drug therapy for human immunodeficiency virus disease. Am. J. Med. 101, 34–40. https://doi.org/10.1016/s0002-9343(96)00077-0 (1996).
Currier, J. S. et al. Differences between women and men in adverse events and CD4+ responses to nucleoside analogue therapy for HIV infection. The AIDS Clinical Trials Group 175 Team. J. Acquir. Immune Defic. Syndr. 24, 316–324. https://doi.org/10.1097/00126334-200008010-00003] (2000).
Clark, R. Sex differences in antiretroviral therapy-associated intolerance and adverse events. Drug Saf. 28, 1075–1083. https://doi.org/10.2165/00002018-200528120-00003 (2005).
Fletcher, C. V., Acosta, E. P. & Strykowski, J. M. Gender differences in human pharmacokinetics and pharmacodynamics. J. Adolesc. Health 15, 619–629. https://doi.org/10.1016/s1054-139x(94)90628-9 (1994).
Knupp, C. A., Milbrath, R. L. & Barbhaiya, R. H. Effect of metoclopramide and loperamide on the pharmacokinetics of didanosine in HIV seropositive asymptomatic male and female patients. Eur. J. Clin. Pharmacol. 45, 409–413. https://doi.org/10.1007/BF00315510 (1993).
Iloeje, U. H. et al. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 130, 678–686. https://doi.org/10.1053/j.gastro.2005.11.016] (2006).
Chen, C. J. et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 295, 65–73. https://doi.org/10.1001/jama.295.1.65 (2006).
Wong, G. L. et al. Metabolic syndrome increases the risk of liver cirrhosis in chronic hepatitis B. Gut. 58, 111–1117. https://doi.org/10.1136/gut.2008.157735 (2009).
Schwarcz, S. K., Vu, A., Hsu, L. C. & Hessol, N. A. Changes in causes of death among persons with AIDS: San Francisco, California, 1996–2011. AIDS Patients Care 28, 517–523. https://doi.org/10.1089/apc.2014.0079 (2014).
Hernando, V. et al. All-cause and liver-related mortality in HIV positive subjects compared to the general population: Differences by HCV co-infection. J. Hepatol. 57, 743–751. https://doi.org/10.1016/j.jhep.2012.06.010 (2012).
Croxford, S. et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Health 2, e35–e46. https://doi.org/10.1016/S2468-2667(16)30020-2 (2017).
Pettit, A. C. et al. Increased non-AIDS mortality among persons with AIDS-defining events after antiretroviral therapy initiation. J. Int. AIDS Soc. 21, e25031. https://doi.org/10.1002/jia2.25031 (2018).
Mak, D., Babb de Villiers, C., Chasela, C., Urban, M. I. & Kramvis, A. Analysis of risk factors associated with hepatocellular carcinoma in black South Africans: 2000–2012. PLoS One 13, e0196057. https://doi.org/10.1371/journal.pone.0196057] (2018).
Ioannou, G. N. et al. The prevalence of cirrhosis and hepatocellular carcinoma in patients with human immunodeficiency virus infection. Hepatology 57, 249–257. https://doi.org/10.1002/hep.25800 (2013).
Pinato, D. J., Dalla Pria, A., Sharma, R. & Bower, M. Hepatocellular carcinoma: An evolving challenge in viral hepatitis and HIV coinfection. AIDS 31, 603–611. https://doi.org/10.1097/QAD.0000000000001422 (2017).
Hu, J., Liu, K. & Luo, J. HIV-HBV and HIV-HCV coinfection and liver cancer development. Cancer Treat. Res. 177, 231–250. https://doi.org/10.1007/978-3-030-03502-0_9 (2019).
Taborelli, M. et al. Excess liver-related mortality among people with AIDS compared to the general population: an Italian nationwide cohort study using multiple causes of death. HIV Med. 21(10), 642–649. https://doi.org/10.1111/hiv.12937 (2020).
Lima, M. D., Firmo, A. A. & Martins-Melo, F. R. Trends in AIDS-related mortality among people aged 60 years and older in Brazil: A nationwide population-based study. AIDS Care 28(12), 1533–1540. https://doi.org/10.1080/09540121.2016.1191608 (2016).
Acknowledgements
We thank the patients, the nurses and physicians who provided care for the patients, and the investigators at Zhongnan Hospital of Wuhan University.
Funding
This study was supported by National Natural Science Foundation of China (82003511), Discipline and Platform Construction Project of Center for AIDS Research, Wuhan University (PTPP2023002).
Author information
Authors and Affiliations
Contributions
R.Y. contributed to the data analysis and implementation of study. R.Y. wrote the original manuscript. Q.C and F.J. contributed to the data collection and data interpretation. X.Y. and Y.X. contributed to the conception and study design. X.Y. and Y.X. contributed to the review and revision. AI-assisted copyediting was not used.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was approved by the Institutional Review Board of Zhongnan Hospital of Wuhan University. Informed consent was obtained from all participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, R., Chen, Q., Jiao, F. et al. The sex differences in diseases progression and prognosis among persons with HIV and HBV coinfection. Sci Rep 15, 4018 (2025). https://doi.org/10.1038/s41598-025-88530-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88530-2
