
Abstract
Infertility is a significant global issue affecting millions of couples, and increased body fat is considered a major contributing factor. Traditional assessment methods, such as body mass index (BMI) and waist circumference (WC), are limited in accurately reflecting body fat composition. The relative fat mass (RFM) index, a newer tool, provides a more precise assessment of fat content, but its relationship with infertility remains unclear. This study aimed to investigate the correlation between relative fat mass and a history of infertility by analyzing data from the National Health and Nutrition Examination Survey (NHANES). The study included 3915 women aged 18 to 45 years. Infertility status was self-reported, and RFM was calculated using a specific formula. Logistic regression models were employed, adjusting for multiple covariates, to investigate the relationship between RFM and infertility. Women with a history of infertility had a significantly higher RFM when compared to those who were not infertile. Specifically, women in the highest RFM quartile had almost three-fold higher odds of history of infertility than those in the lowest quartile (odds ratio [OR]: 2.87; 95% confidence interval [CI]: 1.85–4.44). Subgroup analyses indicated a stronger association between RFM and a history of infertility; this relationship was predominantly observed in women under 35 years-of-age. Sensitivity analyses confirmed the robustness of these findings. Higher RFM is more likely to be associated with a history of infertility. While RFM provides a more accurate assessment of body fat distribution compared to BMI and WC, making it a valuable tool for evaluating infertility, further research is now needed to determine the impact of interventions based on RFM measurements.
Similar content being viewed by others

Introduction
Female infertility is characterized by a failure to establish a clinical pregnancy after 12 months of regular and unprotected sexual intercourse or due to the impairment of a subject’s capacity to reproduce either as an individual or with his/her partner1,2. Female infertility is a pervasive global issue affecting approximately 48.5 million couples, imposing significant emotional and financial burdens on individuals and healthcare systems3. Up to 12% of women of reproductive age suffer from infertility4. The primary etiologies underlying female infertility include ovulatory dysfunction and tubal disease, while lifestyle factors, such as smoking, age, drinking and obesity, are known to represent risk factors for infertility, although the specific mechanisms involved have yet to be fully elucidated. Addressing these factors is crucial if we are to improve reproductive outcomes and reduce the global impact of infertility.
The intricate interplay between obesity and infertility has gained significant attention as obesity rates among women of childbearing age have risen globally. Obesity, characterized by the excessive accumulation of body fat, is a significant risk factor for infertility, and can exert adverse effects on all aspects of reproductive health5. Projections indicate that by 2025, approximately 20% of women of reproductive age will be affected by obesity6,7. Therefore, women who are overweight and planning a pregnancy may find it difficult to achieve successful conception5. Obesity is associated with an elevated likelihood of developing menstrual disorders, polycystic ovary syndrome (PCOS), gestational diabetes (GDM), and pathological changes in the endothelium of the uterus8,9,10. Obesity is traditionally evaluated by body mass index (BMI) and waist circumference (WC)11; however, these metrics have notable limitations. For example, BMI cannot distinguish between fat and muscle mass, or accurately reflect the distribution of body fat, thus causing obesity to be misclassified12. Furthermore, while WC is a reliable indicator of abdominal obesity, this index cannot provide a comprehensive evaluation of total body fat13. When compared to BMI and WC, relative fat mass (RFM) provides a more precise assessment of adiposity14. Previous studies have demonstrated that RFM exhibits superior accuracy when estimating the percentage of fat over the entire body of obese women when compared to BMI15,16,17. Unlike BMI, which does not differentiate between lean mass and fat mass, RFM provides a direct reflection of the percentage of body fat, providing a clearer indicator of adiposity and its metabolic implications18. Recent research has highlighted the critical role of obesity and body fat distribution in infertility, primarily by causing hormonal imbalances and metabolic disruptions19. Large cohort studies, conducted in Danish women planning pregnancies, demonstrated a negative correlation between fecundability ratios and increasing BMI21,22. An cohort of over 7,000 American women identified reduced fecundity in eumenorrheic obese women, while a substantial cohort of more than 3,000 Dutch women with regular menstrual cycles revealed a linear decline in the likelihood of spontaneous conception when BMI exceeded 29 kg/m223,24. Furthermore, women with a higher BMI and undergoing in vitro fertilization (IVF) are known to face a higher risk of cycle cancellation, implantation failure and reduced pregnancy success rates25. WC has been associated with insulin resistance and inflammation, which further exacerbate risks to reproductive health26. Recent research has also highlighted the close relationship between body fat distribution and reproductive health27. Little is known as to how RFM can specifically exert influence on reproductive health, particularly with regards to infertility. We hypothesize that RFM is associated with infertility.
In this study, we investigated the specific correlation between RFM and a history of infertility using a nationally representative sample from the National Health and Nutrition Examination Survey (NHANES). Findings could enhance our understanding of body fat distribution in infertile females and provide more targeted recommendations for clinical management.
Methods
Study design and participants
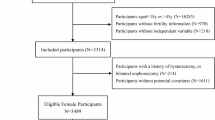
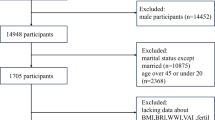
The NHANES is an ongoing cross-sectional study authorized and sponsored by the National Center for Health Statistics (NCHS) in the US. This national study aims to evaluate detailed health information and comprehensive nutritional data relating to the population of the United States. The NHANES employs a complex, multi-stage and probabilistic sampling methodology to guarantee the collection of representative data from diverse demographic groups. In this study, we analyzed NHANES data collected between 2013 and 2020. Participants were women aged 18 to 45 years with data relating to infertility status, RFM and relevant covariates. The exclusion criteria were as follows: age < 18 years or > 45 years, and missing data relating to infertility status, RFM or all covariates. The selection and inclusion procedures for participants are illustrated in the flowchart presented in Fig. 1.

Flow chart showing the procedures used to the selection and inclusion of participants.
Assessment of infertility history
Due to the lack of medical data relating to the diagnosis of female infertility in the NHANES, data relating to self-reported infertility were collected by a Reproductive Health Questionnaire (RHQ) from the NHANES. A history of infertility was determined by the participants’ responses to two questions: RHQ074 (Women were asked, ‘Have you ever attempted to become pregnant over a period of at least a year without becoming pregnant?’), and RHQ076 (Have you ever been to a doctor or other medical provider because you have been unable to become pregnant?” Those who answered ‘yes’ for either of these questions were categorized as having a history of infertility. Conversely, those who responded “no” were classified as fertile.
Assessment of relative fat mass (RFM)
RFM was determined as follows: RFM = 64 - (20 × height / waist circumference) + (12 × sex), where sex = 0 for men and sex = 1 for women15. Height was measured with participants standing barefoot and their heads aligned horizontally against a height measuring device. WC was recorded at the end of normal exhalation, immediately above the iliac crest along the mid-axillary line, with a precision of 0.1 cm29.
Covariates
To investigate the specific association between RFM and infertility, we included a range of covariates in our analysis, encompassing demographic information, physical examination data, health habits and co-morbidities. A comprehensive explanation of the measurement procedures is available on the NHANES website (https://www.cdc.gov/nchs/nhanes/). Demographic characteristics included age, race, poverty income ratio (PIR), education level and marital status. Race was categorized as White (non-Hispanic), Mexican American, Black (non-Hispanic), Hispanic (Other Hispanic), and Other Race (including multi-racial). Education was classified as under high school or above high school. Marital status was classified as never married, married (including living with a partner) or divorced (including those who were separated or widowed). Physical examination data included weight, height, WC and BMI. Health habits included smoking status (yes: regular smoker or having smoked more than 100 cigarettes over the course of a lifetime; no: smoking < 100 cigarettes over the course of a lifetime) and drinking behavior (yes: >12 alcoholic drinks consumed over the last year; no: < 12 alcoholic drinks consumed over the course of a lifetime).
Co-morbidities included hypertension and diabetes mellitus (DM). Hypertension was diagnosed as a patient currently receiving antihypertensive medication, a diagnosis by a physician, or a mean systolic blood pressure ≥ 140 mmHg or mean diastolic blood pressure ≥ 90 mmHg30. Patients were classified as having diabetes mellitus if any of the following criteria were met: self-reported diabetes, a glycosylated hemoglobin of 6.5% or higher, the patient used glucose-lowering medication or insulin, or the patient had a random blood glucose or 2 h oral glucose tolerance test blood glucose of 11.1 mmol/L or higher, or a fasting blood glucose of 7.0 mmol/L or higher31.
Statistical analysis
In order to ensure that our results were representative, sampling weights were applied to the data collected from 2013 to 2020; this was performed with designated NHANES sampling weights (1/4 × wtint2 year) to address the complexities of the survey design. The baseline characteristics of participants who were classified as fertile or infertile were analyzed by weighted t-tests for continuous variables and weighted Chi-squared tests for categorical variables. Mean values are reported with standard errors (SEs) for continuous variables, while frequencies and percentages are presented for categorical variables. The association between BMI, WC, RFM and infertility was investigated using logistic regression models. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). RFM was also categorized into quartiles, as RFM quartiles (RFMQ) (Q1: < 36, Q2: 36–41.26, Q3: 41.26–45.97, Q4: ≥ 45.97), with Q1 serving as the reference category. Cut-offs were determined by ranking all RFM values in ascending order and dividing them into four equal groups based on the 25th, 50th and 75th percentiles. We employed three regression models in our analysis: a Crude Model with no adjustments; Model 1, which adjusted for age and race; and Model 2, which adjusted for a comprehensive set of covariates, including age, race, poverty income ratio, education, smoking status, alcohol consumption, hypertension and diabetes mellitus.
Subgroup analysis was performed to investigate the potential modifying effects of age group, race, smoking, drinking and hypertension. We adjusted for age, race, marital status, PIR, drinking, smoking, hypertension and DM, except for the stratification factor itself, on the association between RFM and infertility. Age was categorized into four groups (< 25, 25 ≤ Age < 30, 30 ≤ Age < 35, and ≥ 35 years). Three sensitivity analyses were conducted to ensure that our findings were robust. First, we performed unweighted analysis, in which logistic regression analyses were performed without applying sampling weights, or adjusting for all covariates. Second, participants over 40 years-of-age were excluded from the weighted logistic regression analyses as infertility rates and abdominal obesity both increase with age, potentially leading to higher RFM values and introducing bias into the association between RFM and infertility20. Thirdly, we addressed missing data using a combination of imputation methods. Missing continuous variables, including PIR (n = 497) and BMI (n = 3), were imputed using the median, while categorical variables, such as marital status (n = 555), education (n = 168), drinking (n = 269), hypertension (n = 2), and smoking (n = 2), were imputed using a missing indicator category. These imputations were followed by logistic regression analyses that adjusted for all covariates. Finally, restricted cubic spline (RCS) analysis was conducted to explore the potential non-linear relationship between RFM and infertility. Weighted data were used to account for the complex sampling design of the NHANES, thus ensuring population representativeness. Seven knots were placed at fixed percentiles of the RFM distribution (5th, 10th, 25th, 50th, 75th, 90th and 95th percentiles) based on minimization of the Akaike Information Criterion (AIC) for optimal model fit. All statistical analyses were conducted using R version 4.3.3. Statistical significance was determined by two-sided tests, and differences > 0.05 were considered statistically significant.
Results
Participant characteristics
A total of 44,960 individuals participated in the study. After excluding participants below 18 and above 45 years of age, as well as those with missing information relating to infertility history, missing RFM, and missing covariate information, a final cohort of 3,915 individuals was included in the study (Fig. 1). The weighted baseline characteristics of participants who were fertile or infertile are presented in Table 1. Women with history of infertility were significantly older (35.04 ± 0.43 vs. 32.07 ± 0.19 years, p < 0.0001), had a significantly higher BMI (31.91 ± 0.61 vs. 29.07 ± 0.23 kg/m², p < 0.0001), and a significantly higher RFM (42.94 ± 0.40 vs. 40.47 ± 0.19, p < 0.0001) than those who were fertile. In addition, the PIR was slightly higher in women with history of infertility (2.93 ± 0.10 vs. 2.73 ± 0.06, p = 0.05), although this was not statistically significant (p = 0.05). Age group, marital status, smoking, hypertension and RFMQ all differed significantly between infertile and fertile women (p < 0.001).
The association between RFM and history of infertility
Analysis of the relationships between BMI, WC, RFM and a history of infertility are presented in Table 2. Models adjusted for all covariables (age, race, PIR, education, smoking, drinking, hypertension and DM) revealed that a higher BMI, WC, and RFM were all significantly associated with an increased risk of infertility. Specifically, each one standard deviation (SD) increase in BMI corresponded to a 3% increase in the risk of history of infertility (OR [odds ratio]: 1.03; 95% CI [confidence interval]: 1.02–1.05, p < 0.001), and each one SD increase in WC corresponded to a 2% increase in the risk of history of infertility (OR: 1.02; 95% CI: 1.01–1.03, p < 0.0001). Each one SD increase in RFM was associated with a 6% increase in the risk of history of infertility (OR: 1.06; 95% CI: 1.03–1.09, p < 0.0001). As a continuous variable, RFM demonstrated a stronger predictive association with a history of infertility risk when compared to BMI and WC, as evidenced by its higher odds ratio per standard deviation. The risk of a history of infertility increased progressively with a higher RFMQ. Compared to women in the lowest quartile (Q1), those in the second quartile (Q2) had an OR of 1.72 (95% CI: 1.11–2.67, p = 0.02), those in the third quartile (Q3) had an OR of 1.67 (95%: CI 1.11–2.50, p = 0.02), and those in the highest quartile (Q4) had an OR of 2.87 (95% CI: 1.85–4.44, p < 0.0001). A significant trend was observed with increasing RFM and the risk of infertility (p for trend < 0.0001), demonstrating a clear dose-response relationship.
To further explore this relationship, we conducted weighted RCS analysis, adjusted for all covariates (age, race, marital status, PIR, education, drinking, smoking, hypertension and DM). When we used four knots, similar to the four quartiles, we identified a linear relationship (p for non-linearity = 0.108), thus suggesting that the general trend between RFM and infertility risk followed a dose-response pattern. When we selected seven knots based on the lowest AIC, our analysis identified a significant non-linear relationship between RFM and a history of infertility (p for non-linearity = 0.009). This association exhibited a near W-shaped pattern, with multiple inflection points where both low and high RFM values corresponded to an elevated history of infertility risk. The lowest risk was observed in the moderate RFM range of 36–41.This indicates that although a dose-response relationship was evident overall, the association between RFM and infertility risk was not entirely linear in certain ranges, thus highlighting the complex interplay between body fat distribution and reproductive health (Fig. 2).

Adjusted RCS curve for the RFM index and infertility, Weighted.
Subgroup analyses
The results derived from subgroup analysis are shown in Table 3. After adjusting for covariates, subgroup analysis revealed that the association between RFM and a history of infertility was predominantly observed in women under the age of 35 years, with age being the only significant modifying factor (p for interaction = 0.02). Specifically, the risk of a history of infertility increased with a higher RFMQ in younger age groups: for women aged 18–24 years, the highest RFMQ (Q4) had an OR of 7.10 (95% CI: 1.68–29.91, p for trend = 0.003); for those aged 25–29 years, the OR was 4.51 (95% CI: 2.10–9.70, p for trend < 0.001); and for those aged 30–34 years, the OR was 4.45 (95% CI: 1.77–11.14, p for trend < 0.001). The association between RFM and a history of infertility was independent of other factors such as race, education, marital status, smoking, drinking, and hypertension, where no significant interactions were observed (all p for interaction > 0.05).
Sensitivity analyses
The findings of our sensitivity analysis are shown in Table 4. These results confirmed the robustness of the association between RFM and infertility. Unweighted logistic regression analysis showed that women in the highest RFMQ (Q4) had an OR of 2.38 (95% CI: 1.76–3.23, p for trend < 0.001) compared to the lowest quartile (Q1). When excluding participants over 40 years-of-age, the OR increased to 3.66 (95% CI: 2.18–6.15, p for trend < 0.001). This adjustment reduced biases associated with age-related infertility risks and elevated RFM, as older women are more likely to develop abdominal obesity. This provided a clearer view of the direct relationship between RFM and infertility in younger women. Following the imputation of missing values, the OR was 2.41 (95% CI: 1.63–3.58, p for trend < 0.001).
Discussion
In this population-based study, we analyzed NHANES data and identified a strong and independent association between a higher RFM and an increased risk of a history of infertility in women aged 18 to 45 years. Notably, younger women (< 35 years-of-age) with an elevated RFM had a significantly higher risk of a history of infertility. These findings were consistent across various sensitivity analyses, underscoring the utility of RFM as an important metric for the evaluation of reproductive health. This is the first study to explore the relationship between the RFM tool for body fat distribution and infertility, offering some preliminary insights that could inform future approaches to the prevention and management of infertility.
Currently, there are limited tools available to evaluate the distribution of body fat, and few studies have examined their utility in infertility research. Our study fills this gap by identifying RFM as a novel and precise predictor of infertility. Unlike traditional metrics, such as BMI and WC, RFM directly estimates fat percentage and distribution, offering unique insights into the role of adiposity in reproductive health32. Previous studies have demonstrated that RFM is a superior predictor of metabolic syndrome and dyslipidemia when compared to BMI33, with stronger correlations to adverse metabolic outcomes. This highlights the relevance of RFM to reproductive health, given that metabolic factors, such as insulin resistance, hormonal imbalances, and chronic inflammation, play a key role in infertility. These associations are consistent with findings from other studies that connect adiposity to infertility, highlighting the mechanisms by which excess body fat affects reproductive health34,35. The ability of RFM to directly estimate the distribution of body fat offers a more accurate and clinically relevant measure when compared to BMI and WC, which have traditionally been used in research addressing obesity and reproductive health. This precision allows RFM to better identify individuals at higher risk of infertility10. Our findings suggest that the incorporation of RFM into clinical evaluations and public health strategies could effectively address reproductive risks associated with obesity.
RFM was strongly associated with the history of infertility in younger women may be related to age-related changes in fat distribution and the physiological effects linked to these changes. In younger individuals, an increase in RFM typically corresponds to a increase in waist WC and total body fat proportion, with fat predominantly accumulating in the visceral area, especially abdominal visceral fat27. Visceral fat has a profound impact on reproductive health, as this represents a major source of estrogen. Excess fat accumulation can lead to elevated estrogen levels, which may inhibit follicular development and disrupt the normal menstrual cycle36. Moreover, visceral fat promotes insulin resistance, leading to a hyper-insulinemic state that encourages androgen secretion, further inhibiting ovulation37. In addition, visceral fat secretes a variety of pro-inflammatory cytokines (e.g., TNF-α, IL-6), thus inducing systemic inflammation that can interfere with ovulatory function38. In contrast, as women age, fat distribution tends to shift toward subcutaneous fat, primarily in the thighs and hips27. This pattern of fat distribution has a lower impact on hormonal levels, insulin resistance, and inflammation, which may explain the weaker association between RFM and infertility risk in older women.
This study has several strengths. First, we used the NHANES database; this ensured that we focused upon a nationally representative sample; this means that our findings are generalizable. Second, we used RFM to provide a more precise measure of body fat distribution, thus overcoming the limitations of both BMI and WC. Third, our findings are robust because we performed specific statistical analyses with multiple logistic regression models and sensitivity analyses. Finally, this study is the first to investigate RFM and infertility in a representative population of US subjects, predominantly focusing on younger women (< 35 years-of-age). However, there are some limitations to our study that need to be considered. First, the cross-sectional design of this study limits our ability to establish a causal relationship between RFM and infertility. In addition, RFM was measured only at baseline, while the history of infertility may have occurred years or even decades earlier. This temporal mismatch introduces potential limitations when interpreting our findings, as it is unclear whether the observed RFM levels directly contributed to the risk of infertility at the time of occurrence or are reflective of subsequent changes in body composition. Therefore, the association observed in this study reflects a potential link between RFM and infertility risk, rather than a direct causal relationship. To address this limitation, future research should prioritize longitudinal cohort studies that track RFM over time relative to infertility outcomes. Such studies would clarify whether changes in RFM precede or follow infertility and help establish temporal precedence. Furthermore, randomized controlled trials are now needed to assess whether targeted interventions to reduce RFM can effectively reduce the risk of infertility. These approaches will provide stronger evidence of causality and help elucidate the underlying biological mechanisms linking RFM with infertility. Second, reliance on self-reported infertility data may introduce recall bias and misclassification. Specifically, classifying all women who answered ‘no’ to RHQ074, or RHQ076 as ‘fertile’, may have introduced non-differential misclassification bias, potentially attenuating the observed associations. This approach did not account for women who may have experienced undiagnosed infertility or subfertility but did not report these conditions. Although we adjusted for multiple covariates, residual confounding cannot be ruled out. Future studies should consider the incorporation of clinically validated infertility diagnoses, such as those based on medical records or objective reproductive assessments, to improve accuracy and minimize bias. Third, while significant associations were observed in younger age groups, particularly among those under 35 years, the sample size in certain subgroups, especially the 18 ≤ age < 25 group, may have limited the statistical power of our analyses. The proportion of infertile women in these subgroups was relatively small; this could have further affected the power to detect meaningful differences. Future studies should prioritize larger sample sizes in these specific groups and conduct post-hoc power analyses to confirm the robustness and reliability of the findings. Fourth, while we adjusted for several potential confounders, residual confounding may still have occured due to variables such as physical activity, diet, and stress levels. Although these variables are included in the NHANES dataset, much of this data were missing, and certain years within the study period lacked this data entirely. The inclusion of this incomplete data could have introduced bias or reduced the reliability of our findings. Future studies should aim to incorporate more complete and consistent confounding factors to enhance the robustness of the analysis and provide a clearer understanding of their impact on reproductive health. Finally, the sample size of 3,915 women aged between 18 and 45 years limited the generalizability of our findings to other populations and age groups.
The findings of our study highlight the strong association between RFM and a history of infertility, emphasizing its value for the assessment of reproductive health. RFM can precisely estimate body fat and its distribution to support the early identification of high-risk individuals and targeted interventions, such as weight management programs, to improve fertility outcomes. On a broader level, integrating RFM into public health strategies and national guidelines could standardize assessments of obesity-related infertility risks, promote healthy lifestyles, and enhance reproductive health outcomes at both individual and population levels.
Conclusion
In this study, we identified a significant association between a high RFM and an increased risk of infertility in women aged 18 to 45 years. Analysis of data from the NHANES survey revealed that respondents with a high RFM were more likely to report a history of infertility than those in the bottom quartile. While an overall dose-response relationship was observed, non-linear patterns in certain RFM ranges highlight the complexity of this association. Given the limitations of this study, our findings suggest an association between RFM and infertility but cannot establish causality. Future longitudinal studies and randomized trials are now needed to validate these results and investigate the underlying mechanisms. Our findings emphasize the potential clinical value of RFM as a tool for assessing infertility risk. Nevertheless, its application should be approached cautiously until stronger evidence of causality is established.
Data availability
The NHANES dataset is publicly available online, accessible at https://www.cdc.gov/nchs/nhanes/.
References
Carson, S. A. & Kallen, A. N. Diagnosis and management of infertility: a review. JAMA 326, 65–76 (2021).
Zegers-Hochschild, F. et al. The International Glossary on Infertility and Fertility Care, 2017. Hum. Reprod. 32 (9), 1786–1801 (2017).
Mascarenhas, M. N., Flaxman, S. R., Boerma, T., Vanderpoel, S. & Stevens, G. A. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLoS Med. 9, e1001356 (2012).
Vander Borght, M. & Wyns, C. Fertility and infertility: definition and epidemiology. Clin. Biochem. 62, 2–10 (2018).
Langley-Evans, S. C., Pearce, J. & Ellis, S. Overweight, obesity and excessive weight gain in pregnancy as risk factors for adverse pregnancy outcomes: a narrative review. J. Hum. Nutr. Diet. 35, 250–264 (2022).
Devlieger, R. et al. Maternal obesity in Europe: where do we stand and how to move forward? A scientific paper commissioned by the European Board and College of Obstetrics and Gynaecology (EBCOG). Eur. J. Obstet. Gynecol. Reprod. Biol. 201, 203–208 (2016).
NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 387 (10026), 1377–1396 (2016).
Broughton, D. E. & Moley, K. H. Obesity and female infertility: potential mediators of obesity’s impact. Fertil. Steril. 107, 840–847 (2017).
Song, X., Wang, C., Wang, T., Zhang, S. & Qin, J. Obesity and risk of gestational diabetes mellitus: a two-sample mendelian randomization study. Diabetes Res. Clin. Pract. 197, 110561 (2023).
Venkatesh, S. S. et al. Obesity and risk of female reproductive conditions: a mendelian randomisation study. PLoS Med. 19 (2), e1003679 (2022).
Silvestris, E., de Pergola, G., Rosania, R. & Loverro, G. Obesity as disruptor of the female fertility. Reprod. Biol. Endocrinol. RBE. 16, 22 (2018).
Karchynskaya, V. et al. Is BMI a Valid Indicator of overweight and obesity for adolescents? Int. J. Environ. Res. Public. Health. 17, 4815 (2020).
Lee, S., Kim, Y. & Han, M. Influence of Waist Circumference Measurement Site on Visceral Fat and metabolic risk in Youth. J. Obes. Metab. Syndr. 31, 296–302 (2022).
Zhu, X. et al. The relationship between depression and relative fat mass (RFM): a population-based study. J. Affect. Disord. 356, 323–328 (2024).
Woolcott, O. O. & Bergman, R. N. Relative fat mass (RFM) as a new estimator of whole-body fat percentage a cross-sectional study in American adult individuals. Sci. Rep. 8, 10980 (2018).
Efe, S. Ç. et al. Relative Fat Mass Index can be solution for obesity paradox in coronary artery disease severity prediction calculated by SYNTAX score. Postgrad. Med. J. 97, 434–441 (2021).
Suthahar, N. et al. Associations of relative fat mass, a new index of adiposity, with type-2 diabetes in the general population. Eur. J. Intern. Med. 109, 73–78 (2023).
Moltrer, M. et al. Body mass index (BMI), waist circumference (WC), waist-to-height ratio (WHtR) e waist body mass index (wBMI): which is better? Endocrine 76 (3), 578–583 (2022).
Ennab, F. & Atiomo, W. Obesity and female infertility. Best Pract. Res. Clin. Obstet. Gynaecol. 89, 102336 (2023).
Wen, Z. & Li, X. Association between weight-adjusted-waist index and female infertility: a population-based study. Front. Endocrinol. (Lausanne). 14, 1175394 (2023).
Wise, L. A. et al. An internet-based prospective study of body size and time-to-pregnancy. Hum. Reprod. Oxf. Engl. 25, 253–264 (2010).
Ramlau-Hansen, C. H. et al. Subfecundity in overweight and obese couples. Hum. Reprod. Oxf. Engl. 22, 1634–1637 (2007).
Gesink Law, D. C., Maclehose, R. F. & Longnecker, M. P. Obesity and time to pregnancy. Hum. Reprod. Oxf. Engl. 22, 414–420 (2007).
Van der Steeg, J. W. et al. Obesity affects spontaneous pregnancy chances in subfertile, ovulatory women. Hum. Reprod. Oxf. Engl. 23, 324–328 (2008).
Sermondade, N. et al. Female obesity is negatively associated with live birth rate following IVF: a systematic review and meta-analysis. Hum. Reprod. Update. 25, 439–451 (2019).
Yin, Y. H. et al. Higher waist circumference is associated with increased likelihood of female infertility: NHANES 2017–2020 results. Front. Endocrinol. 14, 1216413 (2023).
Wang, X., Zhu, R., Han, H. & Jin, J. Body Fat distribution and female infertility: a cross-sectional analysis among US women. Reprod. Sci. 30 (11), 3243–3252 (2023).
Flegal, K. M. et al. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 89, 500–508 (2009).
Ma, W. et al. Dose-Response Association of Waist-to-Height ratio plus BMI and risk of Depression: evidence from the NHANES 05–16. Int. J. Gen. Med. 14, 1283–1291 (2021).
Unger, T. et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 75, 1334–1357 (2020).
American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 33, S62–S69 (2010)
Shen, W. et al. Associations of Relative Fat Mass, a Novel Adiposity Indicator, with Non-Alcoholic Fatty Liver Disease and Cardiovascular Disease: Data from SPECT-China. Diabetes Metab. Syndr. Obes. Targets Ther. 16, 2377–2387 (2023).
Kobo, O., Leiba, R., Avizohar, O. & Karban, A. Relative fat mass is a better predictor of dyslipidemia and metabolic syndrome than body mass index. Cardiovasc. Endocrinol. Metab. 8, 77–81 (2019).
Deng, P., Yu, Q., Tang, H., Lu, Y. & He, Y. Age at Menarche Mediating visceral adipose tissue’s influence on pre-eclampsia: a mendelian randomization study. J. Clin. Endocrinol. Metab. 108 (2), 405–413 (2023).
Gao, Y., Zhou, M., Xu, X., Ma, J. Y. & Qin, M. F. Body composition and risk of gestational diabetes mellitus: a univariable and multivariable mendelian randomization study. J. Diabetes Investig. 15, 346–354 (2024).
Kurowska, P. et al. Adipokines change the balance of proliferation/apoptosis in the ovarian cells of human and domestic animals: a comparative review. Anim. Reprod. Sci. 228, 106737 (2021).
Hayón-Ponce, M. et al. Lower trabecular bone score in type 2 diabetes mellitus: a role for fat mass and insulin resistance beyond hyperglycaemia. Diabetes Metab. 47, 101276 (2021).
Goldsammler, M., Merhi, Z. & Buyuk, E. Role of hormonal and inflammatory alterations in obesity-related reproductive dysfunction at the level of the hypothalamic-pituitary-ovarian axis. Reprod. Biol. Endocrinol. 16 (1), 45 (2018).
Acknowledgements
We are grateful for the information provided by the National Health and Nutrition Examination Survey of the United States.
Funding
This study was supported by Key Research and Development Support Program of the Chengdu Municipal Bureau of Science and Technology, Sichuan Province (2024-YF05-00254-SN) and Key R&D Plan of the Sichuan Provincial Department of Science and Technology (No. 2023YFS0072).
Author information
Authors and Affiliations
Contributions
Kunyan Zhou designed the study. Kunyan Zhou and Dong Liu collected and analyzed the data and wrote the manuscript. Xiaoyan Luo provided suggestions and revised the manuscript. All authors contributed to the manuscript and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This research, which featured human participants were reviewed and approved by the National Health and Nutrition Examination Survey (https://www.cdc.gov/nchs/nhanes/irba98.htm). The patients/participants provided their written informed consent to participate in this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, D., Luo, X. & Zhou, K. Association between current relative fat mass and history of female infertility based on the NHANES survey. Sci Rep 15, 6294 (2025). https://doi.org/10.1038/s41598-025-89417-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89417-y
