
Abstract
Anti-TNFα antibodies are effective in controlling intestinal inflammation caused by Crohn’s disease. However, many patients undergo surgery due to diminished efficacy of the antibodies during maintenance therapy. Currently, the decision between intensification of TNFα therapy and surgery is difficult to make. The purpose of this study was to determine the effect of preoperative treatment with anti-TNFα antibodies on postoperative recurrence of Crohn’s disease. One hundred and fourteen consecutive patients with Crohn’s disease who underwent bowel resection with anastomosis between 2009 and 2021 were retrospectively analyzed on the preoperative treatment history and perioperative information. Of the 74 patients who used anti-TNFα antibodies preoperatively, 43 underwent surgery after intensification of therapy following attenuation of anti-TNFα antibody efficacy. Time to postoperative endoscopic recurrence was significantly shorter in the group using anti-TNFα antibodies than in the group not using them (p = 0.0055). We found no difference in time to postoperative endoscopic recurrence between patients who underwent intensified therapy and those who underwent immediate surgery. Patients who received preoperative anti-TNFα antibody had a shorter time to postoperative endoscopic recurrence, but the presence or absence of intensified treatment after weakening of the anti-TNFα antibody effects did not affect the time to postoperative endoscopic recurrence.
Similar content being viewed by others

Introduction
Crohn’s disease (CD) is a chronic inflammatory bowel disease common among young people in their late teens and early 20 s. In recent years, the number of CD patients in Asia, including Japan, has increased1,2. As of 2014, the number of CD patients in Japan was estimated to be 70,7003. Although the etiology of CD is currently unknown, it is considered to be a multifactorial disease caused by a combination of environmental and genetic factors. Many patients require intestinal surgery during the course of CD. The cumulative operative rate within 10 years of CD diagnosis is approximately 44–50%4. The recurrence rate of CD is high even after surgery, and controlling intestinal inflammation with medical therapy is important5 to prevent repeat surgeries and improve patients’ prognosis.
Antibody preparations against the inflammatory cytokine tumor necrosis factor alpha (TNFα), drugs such as Infliximab and Adalimumab, can be used in patients with CD8,9. In addition, Ustekinumab, an anti-IL-12/23p40 monoclonal antibody; Janus kinase (JAK) inhibitor; and Vedolizumab, monoclonal antibodies targeting α4β7 integrin heterodimers have been used to induce or maintain remission of CD10,11.
In patients with CD who have undergone ileal resection and have no residual disease, 1 year of maintenance therapy with infliximab started within 4 weeks postoperatively significantly reduces endoscopic recurrence at 1 year12. In the POCER study, which examined the usefulness of endoscopy in evaluating postoperative recurrence and the efficacy of intensified treatment when early mucosal lesions are detected, adalimumab-treated patients had significantly fewer recurrences than patients treated with thiopurine13. Planned adalimumab maintenance therapy after surgery has also been shown to be beneficial in Japanese patients with CD14. Thus, postoperative administration of anti-TNFα antibodies may be effective in preventing postoperative recurrence of CD. However, the efficacy of intensified treatment in cases in which the therapeutic effect is attenuated during preoperative maintenance therapy, called loss of response (LOR), is unknown. Few studies have analyzed the relationship between preoperative anti-TNFα antibody treatment history and postoperative recurrence. The purpose of the present study was to examine this relationship.
Patients and methods
Patients
One hundred and fourteen consecutive patients with CD who underwent surgical bowel resection and anastomosis for CD related inflammatory indications of other than malignancy from 2009 to 2021 were included in this study. All patients underwent treatment and follow-up at Osaka University Hospital.
Assessment of clinical features
Gender, age at surgery, age at diagnosis, BMI, surgical history, lesion location, blood test results, and CD treatment history were collected retrospectively from the patients’ records. The dosage of infliximab approved by the Japanese regulatory authorities for the treatment of CD is 5 mg per kg of body weight as a single intravenous infusion, administered again 2 weeks, 6 weeks, and 8 weeks after the initial dose. For adalimumab, 160 mg is injected subcutaneously for the first dose, 80 mg 2 weeks later, and 40 mg every 2 weeks thereafter. For patients with a diminished response to infliximab, doubling the dose, shortening the dosing interval to every 4–7 weeks, or switching to adalimumab are acceptable alternatives. For patients with a diminished response to adalimumab, the dose can be doubled or the treatment switched to infliximab.
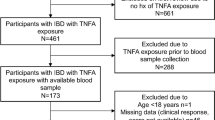
The patients were divided into two groups to determine the relationship between preoperative use of anti-TNFα antibodies and postoperative recurrence. The TNFα Group was defined as patients who used anti-TNFα antibodies preoperatively, and the Non-TNFα Group was defined as patients who did not use anti-TNFα antibodies preoperatively. In addition, the TNFα Group was divided into two groups to evaluate the association between intensified treatment for preoperative anti-TNFα antibody attenuation and postoperative recurrence. The LOR Group consisted of patients who received double doses of anti-TNFα antibody, a shortened dosing regimen, or drug modification after weakening of the anti-TNFα antibody efficacy, whereas the Non-LOR Group consisted of patients who received a standard dose of anti-TNFα antibody before surgery (Fig. 1). In the introduction of biologics, anti-TNFα antibody were introduced first in all cases, and Ustekinumab, Vedolizumab and JAK inhibitors were not used prior to anti-TNFα antibody. The LOR for biologics is defined as a deviation from the state of remission after the introduction of biologics, i.e. IOIBD 0 or 1 and a state where both the erythrocyte sedimentation rate and CRP are within the institutional reference range, or when the attending physician judges that there has been a relapse based on endoscopic examination. Our department’s postoperative medical treatment policy was to not administer prophylactic anti-TNFα antibodies to the Non-TNFα Group and to resume the dose of anti-TNFα antibodies from before surgery in both the LOR and Non-LOR Groups, with treatment intensified according to the results of the first postoperative endoscopic examination.

Patient selection. Anti-TNFα, anti-tumor necrosis factor α; LOR, loss of response.
Postoperative follow-up and diagnosis of recurrence
After surgery, patients were followed up as outpatients once every 1–3 months. As a rule, lower endoscopy, ileal endoscopy, and double-balloon endoscopy were performed 6–12 months after surgery, even in the absence of symptoms. Thereafter, endoscopy was performed every 1–2 years. The Crohn’s Disease Activity Index (CDAI) was used to assess symptomatic recurrence, defined as CDAI ≥ 220. The Rutgeerts score (RS) was used to assess endoscopic recurrence, defined as RS ≥ i215,16.
Statistical analysis
Categorical data were compared using chi-squared or the Wilcoxon rank sum test. The Kaplan–Meier method and log rank test were used to compare endoscopic and symptomatic recurrence in the two groups and to calculate significant differences. P < 0.05 was considered significant. All statistical analyses were performed in JMP statistical software, package 14.0 (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
The characteristics of the 114 patients with CD who underwent surgical bowel resection and anastomosis for CD related inflammatory indications other than malignancy are provided in Table 1. The patients were mainly those who underwent initial surgery, and all patients who received biologics preoperatively were first treated with TNF agents; of those who received intensified biologic therapy before surgery after the TNF agents had diminished their efficacy, 11 patients switched to Ustekinumab and 2 patient switched to Vedolizumab. There were no cases of preoperative use of JAK inhibitors.
Clinical features of the TNF groups
Anti-TNFα antibodies were used preoperatively in 74 patients. We found no differences between the TNFα and Non-TNFα Groups with respect to age at surgery, gender, BMI, preoperative CRP levels, preoperative CDAI, or corticosteroid use. However, there were significantly more cases of repeated surgery and preoperative albumin levels were significantly lower in the TNFα Group. Also, the number of patients using immunomodulatory drugs was significantly higher in the TNFα Group (Table 2).
Clinical features of the LOR groups
Of the 74 patients who used preoperative anti-TNFα antibodies, 43 received intensified treatment for decreased efficacy of the antibodies. We found no difference between the LOR and Non-LOR Groups in terms of age at surgery, gender, BMI, surgical history, preoperative albumin level, preoperative CRP level, preoperative CDAI, presence of immunomodulatory drugs or corticosteroid use (Table 3).
Endoscopic and symptomatic relapse and recurrence
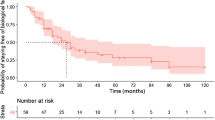
The median follow-up period was 84 months. Figure 2 shows the endoscopic and symptomatic recurrence-free periods and the time elapsed without requiring reoperation for 111 patients.

Postoperative endoscopic and symptomatic relapse-free duration and operation-free duration. RS, Rutgeerts score; CDAI, Crohn’s disease activity index.
The time to postoperative endoscopic recurrence was significantly shorter in the TNFα Group than the Non-TNFα Group (p = 0.0055; Fig. 3a). The time to postoperative symptomatic recurrence was not significantly different between the two groups (Fig. 3b). In addition, we found no predominant difference in time to postoperative endoscopic recurrence-free or time to symptomatic recurrence between the LOR and Non-LOR Groups (Fig. 4).

Endoscopic and symptomatic relapse-free duration based on preoperative anti-TNFα agent use. Anti-TNFα, anti-tumor necrosis factor α.

Endoscopic and symptomatic relapse-free duration based on the loss of response (LOR) after preoperative anti-TNFα with intensified treatment.
Discussion
The outcome of CD has improved dramatically with advances in medical therapy, especially biologic agents17. However, the emergence of a LOR to anti-TNFα antibodies has been problematic, with an attenuated therapeutic response reported to occur in approximately 37% of cases18. LOR is typically seen in 20% to 30% of patients, but approximately 10% of cases each year and nearly half of cases in 5 years have been reported to experience LOR19. The primary mechanism of LOR is thought to be a decrease in blood and tissue levels of anti-TNFα antibody. Anti-infliximab and anti-adalimumab antibodies have been reported as a possible cause20,21. As the main cause of LOR is a decrease in blood levels, the ACCENT I study increased the dose in 40 patients who initially responded but had lost efficacy by week 54. To avoid a decrease in efficacy during maintenance therapy, 5 mg/kg infliximab was increased to 10 mg/kg, which restored efficacy in 36 patients (90%)22.
In addition to evaluating clinical symptoms, endoscopic evaluation of postoperative recurrence is important23. After resection of the ileum, only 20% of CD patients are symptomatic 1 year postoperatively, but endoscopically recurrent lesions in the anastomotic ileum have been reported in 73% of cases24. Regarding recurrence after ileal resection and anastomosis, small aphthous ulcers appear on the ileal side of the anastomosis within the first postoperative year, and serpiginous ulcers and nodular thickening appear 1 to 3 years postoperatively. Anastomotic stenosis has been shown to occur within 3 to 10 years postoperatively25. The RS is used to evaluate postoperative endoscopy based on these observations. Symptomatic recurrence rates are low for i0 and i1 cases, but high for i2 to i4 cases.
In this study, we examined the preoperative anti-TNFα antibody treatment history and postoperative recurrence. As previously reported, endoscopic recurrence preceded symptomatic recurrence.
Preoperative serum albumin levels were significantly lower in the TNFα-treated group than the untreated group. Lower serum albumin levels are significantly correlated with increased clearance of infliximab, leading to a shorter half-life26. Low serum albumin levels also correlate with postoperative endoscopic recurrence in patients receiving preoperative anti-TNFα antibody therapy27, consistent with a significantly higher incidence of endoscopic recurrence in the TNFα Group than in the Non-TNFα Group. In addition to low serum albumin levels, male sex and high BMI are known factors that increase the clearance of anti-TNFα antibodies28.
One of the main causes of LOR is the appearance of antibodies to biological agents. Patients who develop LOR during preoperative anti-TNFα antibody therapy are considered to have emerging antibodies to anti-TNFα antibodies and are likely to relapse even with postoperative anti-TNFα antibody therapy.
This study has several limitations. First, it is a retrospective study conducted at a single institution with a small number of patients. Second, the timing of postoperative endoscopy in this study varied from patient to patient. Finally, this study did not measure antibody levels to biologics, a possible cause of LOR. Many new anti-TNFα antibodies have emerged to replace infliximab and adalimumab, as well as antibodies targeting cytokines and chemokines other than TNFα. Postoperative follow-up should consider the history of preoperative antibody therapy.
In conclusion, patients who received preoperative anti-TNFα antibody therapy had a shorter time to endoscopic recurrence than those who did not receive the therapy.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to consent from participants but are available from the corresponding author on reasonable request.
References
Ooi, C. J. et al. Best practices on immunomodulators and biologic agents for ulcerative colitis and Crohn’s disease in Asia. Intest. Res. 17, 285–310 (2019).
Ogino, T., Mizushima, T., Matsuda, C., Mori, M. & Doki, Y. Essential updates 2018/2019: Colorectal (benign): Recent updates (2018–2019) in the surgical treatment of benign colorectal diseases. Ann. Gatroenterol. Surg. 4, 30–38 (2019).
Murakami, Y. et al. Estimated prevalence of ulcerative colitis and Crohn’s disease in Japan in 2014: an analysis of a nationwide survey. J. Gastroenterol. 54, 1070–1077 (2019).
Peyrin-Biroulet, L., Loftus, E. V. Jr., Colombel, J. F. & Sandborn, W. J. The natural history of adult Crohn’s disease in populationbased cohorts. Am. J. Gastroenterol. 105, 289–297 (2010).
Pariente, B. et al. Development of the Crohn’s disease digestive damage score, the Lémann score. Inflamm. Bowel Dis. 17, 1415–1422 (2011).
Alexander-Williams, J. & Haynes, I. G. Up-to-date management of small-bowel Crohn’s disease. Adv. Surg. 20, 245–264 (1987).
Watanabe, Y. et al. Cumulative inflammation could be a risk factor for intestinal failure in Crohn’s disease. Dig. Dis. Sci. 64, 2280–2285 (2019).
Targan, S. R. et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn’s disease. Crohn’s disease cA2 study group. N. Engl. J. Med. 337, 1029–1035 (1997).
Colombel, J. F. et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial. Gastroenterology 132, 52–65 (2007).
Sandborn, W. J. et al. Ustekinumab induction and maintenance therapy in refractory Crohn’s disease. N. Engl. J. Med. 367, 1519–1528 (2012).
Vermeire, S. et al. Clinical remission in patients with moderate-to-severe Crohn’s disease treated with filgotinib (the FITZROY study): Results from a phase 2, double-blind, randomised, placebo-controlled trial. Lancet 389, 266–275 (2017).
Regueiro, M. et al. Infliximab prevents Crohn’s disease recurrence after ileal resection. Gastroenterology 136, 441–450 (2009).
De Cruz, P. et al. Crohn’s disease management after intestinal resection: A randomised trial. Lancet 385, 1406–1417 (2015).
Asada, T. et al. Postoperative adalimumab maintenance therapy for Japanese patients with Crohn’s disease: A single-center, single-arm phase II trial (CCOG-1107 study). Surg. Today 48, 609–617 (2018).
Ohara, N. et al. Adherence to an elemental diet for preventing postoperative recurrence of Crohn’s disease. Surg. Today 47, 1519–1525 (2017).
Ikeda, A. et al. A novel predictive nomogram for early endoscopic recurrence after intestinal resection for Crohn’s disease. Digestion 100, 269–276 (2019).
Grevenitis, P., Thomas, A. & Lodhia, N. Medical therapy for inflammatory bowel disease. Surg. Clin. North Am. 95, 1159–1182 (2015).
Gisbert, J. P. & Panés, J. Loss of response and requirement of infliximab dose intensification in Crohn’s disease: A review. Am. J. Gastroenterol. 104, 760–767 (2009).
Schnitzler, F. et al. Long-term outcome of treatment with infliximab in 614 patients with Crohn’s disease: results from a single-centre cohort. Gut 58, 492–500 (2009).
Nanda, K. S., Cheifetz, A. S. & Moss, A. C. Impact of antibodies to infliximab on clinical outcomes and serum infliximab levels in patients with inflammatory bowel disease (IBD): A meta-analysis. Am. J. Gastroenterol. 108, 40–47 (2013).
Karmiris, K. et al. Influence of trough serum levels and immunogenicity on long-term outcome of adalimumab therapy in Crohn’s disease. Gastroenterology 137, 1628–1640 (2009).
Rutgeerts, P. et al. Comparison of scheduled and episodic treatment strategies of infliximab in Crohn’s disease. Gastroenterology 126, 402–413 (2004).
Gionchetti, P. et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: Part 2: Surgical management and special situations. J. Crohns Colitis. 11, 135–149 (2017).
Rutgeerts, P. et al. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 99, 956–963 (1990).
Rutgeerts, P. et al. Natural history of recurrent Crohn’s disease at the ileocolonic anastomosis after curative surgery. Gut 25, 665–672 (1984).
Dotan, I. et al. Patient factors that increase infliximab clearance and shorten half-life in inflammatory bowel disease: A population pharmacokinetic study. Inflamm. Bowel Dis. 20, 2247–2259 (2014).
Hiraoka, S. et al. Efficacy of restarting anti-tumor necrosis factor α agents after surgery in patients with Crohn’s disease. Intest. Res. 16, 75–82 (2018).
Ordás, I., Mould, D. R., Feagan, B. G. & Sandborn, W. J. Anti-TNF monoclonal antibodies in inflammatory bowel disease: Pharmacokinetics-based dosing paradigms. Clin. Pharmacol. Ther. 91, 635–646 (2012).
Acknowledgements
We would like to thank San Francisco Edit (www.sfedit.net) for English language editing.
Funding
We did not receive any specific funding for this study.
Author information
Authors and Affiliations
Contributions
Y.S., T.O., and T.M. designed the study and wrote the manuscript. T.T., M.T., T.H., A.H., H.T., N.M., and M.U. performed data collection and analysis. Y.D. and H.E. approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
The Osaka University Clinical Research Review Committee approved this study (approval number: 15028-2). All patients provided written informed consent. If the patient was under 18 years of age, informed consent was obtained from the parent. All methods were performed in accordance with the relevant guidelines and regulations.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sekido, Y., Ogino, T., Takeda, T. et al. Influence of preoperative anti TNF alpha antibody therapy on postoperative recurrence of Crohn’s disease. Sci Rep 15, 11573 (2025). https://doi.org/10.1038/s41598-025-89834-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89834-z
