
Abstract
The optimal management of perianal abscess ( PA) in infants remains controversial. This study aimed to compare incision and drainage (ID), incision and drainage with primary fistulotomy (IDF), and conservative management(CM)for the treatment of infants with PA (< 1 year). A retrospective cohort study was conducted for infants with PA between 2014 and 2020. Patients undergoing IDF were assigned to the IDF group, those undergoing ID were assigned to the ID group, and those whose parents declined surgery were assigned to the CM group. A total of 597 patients were identified (591 boys and 6 girls); 282 in the IDF group, 162 in the ID group, and 153 in the CM group. The median age at first visit was 43 days (range 30–90 days). The median follow-up was 5.8 years (range 3–9.4 years). The baseline characteristics of the three groups were similar (except for abscess size, length of stay, and inpatient costs). The cure rate in the IDF group (97.8%, 276/282) was higher than that in the ID group (82.1%, 133/162; p < 0.001), and the CM group (80.4%, 123/153; p < 0.001). No severe complications were found in the ID or CM groups. The IDF group had 3 cases of sepsis, including 1 with a concurrent central nervous system infection. No fecal incontinence was observed in any of the patients. PA in infants may be a self-limiting disease. CM should be the first-line approach in most cases of PA in infants.
Similar content being viewed by others

Introduction
A perianal abscess (PA) is a common infectious disease in infants that develops from infection in abnormally deep crypts of Morgagni1, with a strong male predominance2. The incidence was highest in the first 3 months of age, decreased gradually until 1 year of age3. Presently, the optimal management of PA in infant has not yet been established. The most common treatment methods include incision and drainage (ID)4,5,6,7,8,9,10,11,12,13,14,15, incision and drainage with primary fistulotomy (IDF)16,17,18,19,20,21,22,23,24,25,26,27, and conservative management (CM)2,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43. Among them, ID is currently the preferred treatment choice. IDF is also a prevalent treatment modality, exhibiting higher cure rates. Since 1998, PA in infants has been recognized as a self-limiting disease30, and CM has been proven to be effective. Due to a lack of large sample size and long-term follow-up data, there is currently no universally recognized optimal treatment method. Further research is needed to address these issues.
Our previous study compared the outcomes of ID versus IDF for PA in neonates. We found both to be safe and effective treatment modalities, with IDF demonstrating superior efficacy44. In our latest study, we found that CM resulted in a long-term cure rate of 90.8%3. In the last four years, our understanding of PA in infants has continuously deepened. What is the optimal management?
To the best of our knowledge, no study has directly compared the outcomes of ID, IDF, and CM for PA in infants. This study aimed to compare the efficacy and safety of ID, IDF, and CM for infants with PA.
Materials and methods
This study is a retrospective cohort study, with the study population consisting of infants with PA who were treated at our center from September 2014 to December 2020 (aged less than 1 year). Before 2023, the treatment for PA in infants was mainly surgical management at our hospital. Surgeons in different departments have different discretion for specific surgical procedure. Infants with PA can be treated either in the department of pediatric surgery (ID) or anorectal surgery (IDF). The decision of whether an infant visited the department of pediatric surgery or the colorectal surgery is determined by the parents’ awareness and preferences, rather than the severity of the infant’s condition. Infants who underwent IDF in the department of anorectal surgery were included in the IDF group, while those who underwent ID in the department of pediatric surgery were included in the ID group. Infants whose parents refused surgery and opted for conservative treatment were included in the CM group. The grouping in this cohort was not artificially intervened; rather, it was naturally formed. Patients in the ID and IDF groups received intravenous antibiotics routinely (Cefathiamidine in the ID group and Ceftazidime in the IDF group) for 3–5 days.
It’s important to note that our previous study3 shares the same patient population as the current study, with the sample of patients undergoing CM being identical. The difference lies in the criteria for treatment failure; in the previous study, treatment failure included new-onset abscesses, whereas in the current study, new-onset cases are discussed separately and not included in the statistics for treatment failure.
This study has received approval from the Affiliated Hospital of Jining Medical University Institutional Review Board. All methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all participants’ legal guardians.
Incision and drainage
Under local anesthesia, a small incision was carefully created at the apex of the abscess. Subsequently, the internal pockets within the cavity were meticulously disrupted through gentle probing using a hemostatic forcep.
Incision and drainage with primary fistulotomy
Immediately following ID, a fistulotomy was routinely performed with the patient positioned in the left lateral decubitus position under conscious sedation and local anesthesia. The critical step was identifying the internal opening. A fine probe was carefully advanced from the abscess cavity to the affected anal crypt, after which the fistula tract was unroofed and opened using diathermy. If the internal opening could not be probed, the corresponding internal opening, located at the center of the abscess, was identified and laid open.
Conservative management
Before 2023, surgical intervention was the standard approach for managing PA in infants at our center. The patients were treated conservatively because their parents refused surgery. Conservative treatment consisted of sitz baths with traditional Chinese medicine, hygiene, erythromycin ointment, and mupirocin ointment, et al. Antibiotics (one course) were not routinely used. To fully observe the effects of CM, patients who underwent surgical management within 2 months of CM were excluded.
Diagnostic criteria
The diagnosis was made using the International Classification of Diseases (ICD) criteria. Diagnosis of PA and anal fistula is based on medical history and physical examination. Key points for diagnosing PA include redness, swelling, and pain around the anus, with palpable firm masses in the perianal area.
Definitions
Treatment Failure: This encompasses the anal fistula formation and recurrence.
Fistula Formation: The formation of a fistula opening in the perianal skin with a tract between the anal canal and rectum.
Recurrence: Refers to the reappearance of PA in the original location after the abscess was cured.
Cure: There is neither recurrence nor fistula formation.
New-onset abscess: Formation of a PA in a location outside the primary lesion site.
Inclusion criteria
The study population consists of infants with PA (aged less than 1 year) who were first diagnosed and treated at our outpatient department from August 2014 to December 2020.
Exclusion criteria
Infants with PA who received treatment at another hospital before visiting our outpatient department, infants treated conservatively for less than 2 months, infants with disease duration exceeding three months at the time of consultation resulting in the formation of an anal fistula, as well as patients lost to follow-up or with incomplete medical records, were excluded from the study. Infants with inflammatory bowel disease and systemic diseases were excluded from our study.
Follow-Up
Short-term follow-up was performed weekly using outpatient evaluations in the first three weeks, and monthly thereafter. Long-term follow-up data were predominantly acquired through telephone interviews or WeChat (a Chinese multi-purpose messaging, social media app developed by Tencent. It not only allows users to send text messages, pictures, and videos, but also to make voice and video calls).
Data collection
The collected data encompassed baseline characteristics, duration of follow-up, fistula formation, recurrence of abscesses, incidence of new-onset abscesses, cure time, and fecal incontinence. The abscess size was recorded as the longest abscess diameter, excluding the depth.
Statistical analysis
Quantitative variables were presented as medians accompanied by interquartile ranges (IQR). Categorical variables were expressed as frequency (percentages). As the quantitative variables did not meet the assumption of normal distribution, Kruskal–Wallis H-test or the Mann–Whitney U-test (length of stay, and inpatient costs) were utilized. Chi-square and Fisher’s exact tests were used for contingency table analysis. Bonferroni correction was applied to post hoc pairwise comparisons. A p-value of less than 0.05 was considered to indicate statistical significance. All statistical analyses were conducted using SPSS software, version 23.0.
Results
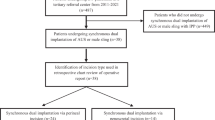
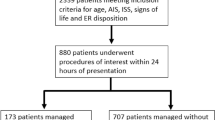
In total, 772 infants with PA (< 1 year) were identified from 2014 to 2020. 597 patients were included in the statistical analysis according to the inclusion and exclusion criteria. A flow chart showing patient screening is shown in Fig. 1.

The flowchart of patient inclusion. PA perianal abscess.
Table 1 summarizes the comparison of baseline characteristics including gender, age at presentation, number of abscesses, abscess size, location of abscessed, length of stay, inpatient costs, and follow-up among the three groups of patients. The median follow-up period was 5.8 years (range 3–9.4 years). There were no statistically significant differences among the three groups in terms of follow-up time. Except for abscess size, length of stay, and inpatient costs, the baseline characteristics of the three groups were similar, with no statistically significant differences observed (p > 0.05).
Outcomes of the three groups are shown in Table 2. The cure rate in the IDF group was 97.8% (276/282), significantly higher than that in the ID group (82.1%, 133/162; p < 0.001) and the CM group (80.4%, 123/153; p < 0.001). Moreover, there was no significant statistical difference in cure rates between the ID group and the CM group. Pairwise comparisons with Bonferroni correction are shown in Table 3.
In the ID group, of the 29 treatment failures, 22 were cured by surgery and 7 by CM alone. Among the 6 treatment failures in the IDF group, 5 were cured with conservative treatment and 1 underwent surgery. In the CM group, out of 30 treatment failures, 10 underwent surgery and 20 continued with CM; 17 were cured and 3 remained uncured.
During the treatment process, new abscess formation occurred in all three groups of patients. Statistical analysis showed a significant difference in the rate of new-onset abscesses across the three groups. However, post hoc pairwise comparisons with Bonferroni correction did not reveal any significant differences between any two groups (see Table 3). The age range of patients with newly developed abscesses is from 15 to 281 days. The time from the initial onset of symptoms to the development of the new abscess ranges from 3 to 8 years, with the majority occurring within 2 months. Among the 11 new cases in the ID group, 8 cases underwent surgery, and 3 cases opted for conservative treatment. In the IDF group, out of the 6 cases of new abscess formation, 5 cases opted for conservative treatment, and 1 case underwent surgery. In the CM group, out of the 10 new cases, 4 cases underwent surgery, and 6 cases opted for conservative treatment. All the mentioned patients achieved cure.
No severe complications were found in the ID or CM groups. The IDF group had 3 cases of sepsis, including 1 with a concurrent central nervous system infection. The preoperative white blood cell counts for the three patients were 15.1, 21.3, and 35.6 × 109/L, respectively. No fecal incontinence was observed in any of the patients.
Discussion
Our study investigated the efficacy of different treatment strategies for pediatric PA in infants under 1 year of age. We observed a total of 772 infants with PA in the outpatient setting over a period of 6 years, ultimately enrolling 597 patients in our study after exclusions and losses to follow-up. We achieved a high follow-up rate of 87.3%, with a median follow-up period of 5.8 years.
In our study, all three treatment methods were safe and effective. However, the efficacy of conservative treatment exceeded our expectations, with a cure rate of 80.4% (123/153) 2 months after initial diagnosis and a cure rate of 91.5% (140/153) at the long-term follow-up. This suggests that PA in infants may be a self-limiting condition, which is consistent with previous studies30,36,41. A study indicates that the cure rates for abscesses that naturally rupture and drain are the same as those for surgically drained abscesses32. For patients whose abscesses had already ruptured at the time of consultation, further ID did not provide additional benefits, making CM a better choice. If there is no significant progression during the treatment process, extending the duration of CM can improve the cure rate.
In the ID and IDF groups, a total of 59 patients experienced surgical treatment failure, of which 29 (50%) were cured with CM. This demonstrates that CM can be used not only for first-time PA, but also for patients who have failed surgical treatment, potentially reducing the trauma caused by secondary surgeries and anesthesia.
The cure rate in the IDF group was 97.8% (276/282), significantly higher than that in the ID group and the CM group. We believe that excising the fistula, incising the internal opening, or removing the corresponding anal crypt ensures more adequate drainage and mitigates factors that contribute to recurrence and the formation of fistulas, thereby enhancing the cure rate. This is fully consistent with previous literature, which showed no recurrences19,21 or a recurrence rate of less than 15%17,23 in patients who underwent fistulotomy at the time of initial drainage. Based on these findings, we recommended that ID and simultaneous laying open of any coexisting fistulous tract should be performed for PA in neonates44.
It is worth noting that this was our perspective in 2022 (advocating IDF), which is inappropriate. Patients who underwent IDF require anesthesia, are subjected to surgical trauma, and face a potential risk of postoperative complications. Therefore, in spite of a significant cure rate, IDF has ceased to be the mainstream treatment approach at our hospital in 2023.
After 2022, through a retrospective study3, we discovered that infant PA may be a self-limiting condition. CM is effective and safe for PA in infants, achieving a cure rate of over 80% while incurring minimal treatment costs (without severe adverse effects). Since the majority of patients achieved cure with CM, avoiding the risks of anesthesia and surgical trauma, we now recommend CM as the first-line approach for infant PA. Starting in 2023, we initiated a prospective clinical study (ChiCTR2300077406) to evaluate the efficacy and safety of CM for PA in infants. To date, we have enrolled 30 patients, and the preliminary results of our study provide initial evidence supporting the effectiveness of CM.
In the IDF group, three severe complications occurred, including two cases of sepsis and one case of sepsis with a concurrent central nervous system infection. All three patients had multiple abscesses larger than 2 cm and suffered from severe diarrhea and watery stools. In fact, the sepsis did not necessarily result from surgery. We hypothesize that sepsis may be associated with leukocytosis, extensive infection, transient intraoperative entry of purulent fluid into the bloodstream, and postoperative absorption of watery stool through the open wound. Fortunately, after intensive treatment, all three patients recovered well.
In the IDF group, 6 patients (2.2%, 6/282) failed surgery; 5 were cured with conservative treatment and 1 underwent surgery. CM was the main treatment for those who failed IDF. This is mainly because secondary surgeries can potentially lead to medical disputes. In most cases, unless the abscess is too large, the symptoms of anal fistula recur frequently, or the patient’s parents strongly insist on surgery, we prefer to adopt a conservative approach. In fact, out study showed that CM is effective in patients who experience failure following IDF surgery.
ID remains the most common treatment approach for pediatric abscesses, although the recurrence rate and the likelihood of fistula formation vary according to the literature. In our study, the cure rate in the ID group was 82.0% (133/162), consistent with our previous data44 on neonatal PA. Given the similar effectiveness of ID and CM, we prefer CM for initial abscess incidents in infants. Since 2023, we have prioritized conservative treatment as the primary approach (not only due to parental refusal for surgery), moving away from the previously preferred IDF method. Only a minority of patients are suitable for surgical resection.
Determining the appropriate timing for surgical intervention remains a challenge with no universally accepted standard. Based on our clinical experience, we suggest that surgery should be considered under the following circumstances: The patient exhibits abnormal irritability or inconsolable crying; Signs of sepsis are present; The patient has a fever exceeding 38.5 °C; The abscess cavity measures larger than 3 cm in diameter; There are more than three abscesses; The patient does not achieve complete cure despite undergoing several months of CM; The parents of the patient strongly request surgical intervention.
The decision to proceed with surgery should also take into account the preferences of the patient’s parents, as this is a shared decision-making process. Effective communication is essential, especially since CM is not guaranteed to be fully effective. Providing comprehensive information can help mitigate potential conflicts between healthcare providers and patients’ families.
An interesting and unique finding in our study is the asymmetrical occurrence of PA among the 597 pediatric patients; right-sided abscesses (at the 9 o’clock position) occurred at a higher rate of 53.9% (322/597) compared to the left side (at the 3 o’clock position) at 36.3% (217/597) (P < 0.05), with bilateral occurrences at 7.2% (43/597) and other locations at 2.5% (15/597). This is the first time such a phenomenon has been observed and has not been previously reported. We speculate that this may be related to anatomical differences in the anal glands, but the reason for this finding is not yet understood and requires further study.
Our data show that among the 48 patients who developed fistulas, the rate of new abscess formation was 18.7% (9/48), which is higher than the overall new abscess rate of 4.5% (27/597, p < 0.001). It is also significantly higher than the new abscess rate of 3.3% (18/549, p < 0.001) in patients who did not develop fistulas. The reasons for this correlation are not yet understood and may be related to the longer disease course, repeated purulent discharges irritating the anal skin, or other unclear factors. Therefore, in patients with fistulas who continued with CM, attention should be paid to new abscess formation.
In the CM group, out of the 10 new cases, 6 cases opted for conservative treatment. Some patients developed new abscesses during the course of CM, yet their parents continued to reject surgical intervention. Through follow-up, we found that CM was also effective for managing newly developed abscesses. Among the three groups of patients, a total of 27 cases of new abscess formation occurred. Of these, 17 patients chose surgery and 10 opted for CM as their parents refused surgery. Ultimately, all 27 patients with new abscesses were cured. This may be because that PA in infants may be a self-limiting condition, suggesting that CM is effective, with surgery being best avoided whenever possible.
Fecal incontinence can be a potential risk associated with fistulotomy due to the damage of the sphincter. In fact, fistulotomy is not associated with the risk of fecal incontinence, as the fistulae in infants are almost always sphincteric17,19,23,26,27,45. Only two patients have been reported to have developed fecal incontinence following surgery21. Thus, the risk of fecal incontinence following the IDF procedure is extremely low, making it a negligible concern in clinical practice.
Our study’s large sample size and long-term follow-up add reliability, but it is important to note that our study is a single-center retrospective study, and its conclusions are somewhat limited. What’s more, the abscess size was different between the three groups. It should be noted that the 153 patients in the CM group were treated conservatively because their parents refused surgical intervention, rather than due to the small size of the abscesses. In fact, 67 patients (43.8%) had abscesses larger than or equal to 1 cm. We must acknowledge that the selection of patients for CM may be subject to bias; however, the impact of this bias is likely minimal. Furthermore, we are currently conducting a prospective cohort study on CM for infants with PA, which will help to significantly reduce this bias.
Conclusions
Our data suggest that PA in infancy is likely a self-limiting disease, with most patients responding well to extended CM. For patients who develop fistulas following failed surgical treatment, CM is also recommended. Early surgical management should be avoided as the first choice for PA in infants.
Data availability
Te datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Shafer, A. D., McGlone, T. P. & Flanagan, R. A. Abnormal crypts of morgagni: the cause of perianal abscess and fistula-in-ano. J. Pediatr. Surg. 22, 203–204. https://doi.org/10.1016/S0022-3468(87)80327-5 (1987).
Gong, Z. et al. Treatment of first-time perianal abscess in childhood, balance recurrence and fistula formation rate with medical intervention. Eur. J. Pediatr. Surg. 28, 373–377. https://doi.org/10.1055/s-0037-1603092 (2018).
Yin, W. et al. Natural course of perianal abscess in infants: a real-world study. Sci. Rep. 13, 18416. https://doi.org/10.1038/s41598-023-45751-7 (2023).
Brook, I. & Martin, W. J. Aerobic and anaerobic bacteriology of perirectal abscess in children. Pediatrics 66, 282–284 (1980).
Boenicke, L. et al. Efficacy of conservative treatment of perianal abscesses in children and predictors for therapeutic failure. Clin. Exp. Pediatr. 63, 272–277. https://doi.org/10.3345/cep.2019.00969 (2020).
Niyogi, A., Agarwal, T., Broadhurst, J. & Abel, R. M. Management of perianal abscess and Fistula-in-ano in children. Eur. J. Pediatr. Surg. 20, 35–39. https://doi.org/10.1055/s-0029-1241878 (2010).
al-Salem, A. H., Qaisaruddin, S. & Qureshi, S. S. Perianal abscess and fistula in ano in infancy and childhood: a clinicopathological study. Pediatr. Pathol. Lab. Med. 16, 755–764 (1996).
Afşarlar, Ç. E. et al. Perianal abscess and fistula-in-ano in children: clinical characteristic, management and outcome. Pediatr. Surg. Int. 27, 1063–1068. https://doi.org/10.1007/s00383-011-2956-7 (2011).
Abercrombie, J. F. & George, B. D. Perianal abscess in children. Ann. R Coll. Surg. Engl. 74, 385–386 (1992).
Nix, P. & Stringer, M. D. Perianal sepsis in children: Perianal sepsis in children. Br. J. Surg. 84, 819–821. https://doi.org/10.1046/j.1365-2168.1997.02699.x (1997).
Enberg, R. N. Perirectal abscess in children. Arch. Pediatr. Adolesc. Med. 128, 360. https://doi.org/10.1001/archpedi.1974.02110280090011 (1974).
Arditi, M. & Yogev, R. Perirectal abscess in infants and children: report of 52 cases and review of literature. Pediatr. Infect. Dis. J. 9, 411–415. https://doi.org/10.1097/00006454-199006000-00009 (1990).
Charalampopoulos, A. et al. Surgical treatment of perianal abscess and fistula-in-ano in childhood, with emphasis in children older than 2 years. J. Pediatr. Surg. 47, 2096–2100. https://doi.org/10.1016/j.jpedsurg.2012.06.032 (2012).
Zhu, Y. & Xu, F. The pathogens and curative effects analysis of perianal abscess of infants under 3 months. Turk. J. Pediatr. 61, 40. https://doi.org/10.24953/turkjped.2019.01.007 (2019).
Macdonald, A., Wilson-Storey, D. & Munro, F. Treatment of perianal abscess and fistula- in-ano in children. Br. J. Surg. 90, 220–221. https://doi.org/10.1002/bjs.4017 (2003).
Longo, W. E., Touloukian, R. J. & Seashore, J. N. Fistula in ano in infants and children: implications and management. Pediatrics 87, 737–739 (1991).
Juth Karlsson, A., Salö, M. & Stenström, P. Outcomes of various interventions for first-time perianal abscesses in children. BioMed. Res. Int. 2016, 1–6. https://doi.org/10.1155/2016/9712854 (2016).
Piazza, D. J. & Radhakrishnan, J. Perianal abscess and fistula-in-ano in children. Dis. Colon Rectum. 33, 1014–1016. https://doi.org/10.1007/BF02139215 (1990).
Bałaż, K. et al. Perianal abscess and fistula-in-ano in children—evaluation of treatment’s efficacy. Are we able to avoid the recurrence? Pol. J. Surg. 92, 1–5. https://doi.org/10.5604/01.3001.0013.8158 (2020).
Ezer, S. S., Oğuzkurt, P., Ince, E. & Hiçsönmez, A. Perianal abscess and fistula-in-ano in children: aetiology, management and outcome. J. Paediatr. Child. Health. 46, 92–95. https://doi.org/10.1111/j.1440-1754.2009.01644.x (2010).
Festen, C. & van Harten, H. Perianal abscess and fistula-in-ano in infants. J. Pediatr. Surg. 33, 711–713. https://doi.org/10.1016/s0022-3468(98)90193-2 (1998).
Murthi, G. et al. Perianal abscess in childhood. Pediatr. Surg. Int. 18, 689–691. https://doi.org/10.1007/s00383-002-0761-z (2002).
Buddicom, E., Jamieson, A., Beasley, S. & King, S. Perianal abscess in children: aiming for optimal management: Perianal abscess in children. ANZ J. Surg. 82, 60–62. https://doi.org/10.1111/j.1445-2197.2011.05941.x (2012).
Krieger, R. W. Perirectal Abscess in Childhood: a review of 29 cases. Am. J. Dis. Child. 133, 411. https://doi.org/10.1001/archpedi.1979.02130040065014 (1979).
Doerner, J. et al. Risk factors for therapy failure after surgery for perianal abscess in children. Front. Surg. 9, 1065466. https://doi.org/10.3389/fsurg.2022.1065466 (2022).
King, S. K. Should we seek a fistula-in-ano when draining a perianal abscess? Perianal abscess and fistula-in-ano. J. Paediatr. Child. Health. 46, 273–274. https://doi.org/10.1111/j.1440-1754.2009.01694.x (2010).
Tan Tanny, S. P. et al. Surgical management of perianal abscess in neonates and infants. ANZ J. Surg. 90, 1034–1036. https://doi.org/10.1111/ans.15801 (2020).
Chang, H. K., Ryu, J. G. & Oh, J-T. Clinical characteristics and treatment of perianal abscess and fistula-in-ano in infants. J. Pediatr. Surg. 45, 1832–1836. https://doi.org/10.1016/j.jpedsurg.2010.03.021 (2010).
Sueyoshi, R. et al. Combination therapy with traditional medicines for perianal abscess in children. Pediatr. Int. 61, 1025–1029. https://doi.org/10.1111/ped.13988 (2019).
Watanabe, Y. Conservative Management of Fistula in ano in Infants (Pediatr Surg Int, 1998).
Hanada, M. et al. Evaluation of the efficacy of incision and drainage versus hainosankyuto treatment for perianal abscess in infants: a multicenter study. Surg. Today. 45, 1385–1389. https://doi.org/10.1007/s00595-014-1058-2 (2015).
Kang, C. et al. Intermediate-term evaluation of initial non-surgical management of Pediatric Perianal Abscess and Fistula-In-Ano. Surg. Infect. 23, 465–469. https://doi.org/10.1089/sur.2021.351 (2022).
Ohya, T. et al. Management for fistula-in-ano with ginseng and Tang-Kuei ten combination. Pediatr. Int. 46, 72–76. https://doi.org/10.1111/j.1442-200X.2004.x (2004).
Kawahara, H., Nakai, H., Yoneda, A. & Kubota, A. Management of perianal abscess with hainosankyuto in neonates and young infants: Perianal abscess and hainosankyuto. Pediatr. Int. 53, 892–896. https://doi.org/10.1111/j.1442-200X.2011.03395.x (2011).
Stokes, R., Wanaguru, D., Saadi, A. & Adams, S. Management of perianal abscesses in infants without general anaesthesia: a systematic review of the literature. Pediatr. Surg. Int. 36, 1317–1325. https://doi.org/10.1007/s00383-020-04728-7 (2020).
Christison-Lagay, E. R. et al. Nonoperative management of perianal abscess in infants is associated with decreased risk for fistula formation. Pediatrics 120, e548–e552. https://doi.org/10.1542/peds.2006-3092 (2007).
Serour, F., Somekh, E. & Gorenstein, A. Perianal abscess and Fistula-In-Ano in infants: a different entity? Dis. Colon Rectum. 48, 359–364. https://doi.org/10.1007/s10350-004-0844-0 (2005).
Samuk, I. et al. Perianal abscess in infants: amenable to conservative treatment in selected cases. Pediatr. Int. 61, 1146–1150. https://doi.org/10.1111/ped.13996 (2019).
Gosemann, J-H. & Lacher, M. Perianal abscesses and fistulas in infants and children. Eur. J. Pediatr. Surg. 30, 386–390. https://doi.org/10.1055/s-0040-1716726 (2020).
Abbott, M. B. Surgeons say no to surgery for Perianal abscesses in infants. Pediatrics 120, 646–646. https://doi.org/10.1542/peds.2007-1295 (2007).
Rosen, N. G. et al. The nonoperative management of fistula-in-ano. J. Pediatr. Surg. 35, 938–939. https://doi.org/10.1053/jpsu.2000.6931 (2000).
Ding, W., Sun, Y-R. & Wu, Z-J. Treatment of Perianal Abscess and Fistula in infants and Young children: from Basic etiology to clinical features. Am. Surg. 87, 927–932. https://doi.org/10.1177/0003134820954829 (2021).
Kubota, M., Hirayama, Y. & Okuyama, N. Usefulness of bFGF spray in the treatment of perianal abscess and fistula-in-ano. Pediatr. Surg. Int. 26, 1037–1040. https://doi.org/10.1007/s00383-010-2664-8 (2010).
Yin, W., Li, L., Su, L. & Wang, S. Incision and drainage with primary fistulotomy of Perianal Abscess is safe and effective in neonates: a long-term Follow-Up study. Front. Pediatr. 10, 862317. https://doi.org/10.3389/fped.2022.862317 (2022).
Poenaru, D. & Yazbeck, S. Anal fistula in infants: etiology, features, management. J. Pediatr. Surg. 28, 1194–1195. https://doi.org/10.1016/0022-3468(93)90163-F (1993).
Funding
This work was supported by the Talent Development Program of Affiliated Hospital of Jining Medical University [2023-yxyc-004], the Key Research and Development Program of Jining [2024YXNS241], and Nursery Fund of Affiliated Hospital of Jining Medical University [No. MP-ZD-2023–03 to zongke wang].
Author information
Authors and Affiliations
Contributions
S.W. conceptualized and designed the study, contributed to follow-up, drafted the initial manuscript, and critically reviewed and revised the manuscript. P.W., L.L., and Z.W. conceptualized and designed the study, contributed to follow-up, and critically reviewed and revised the manuscript. L.X., and Z.S. contributed to follow-up, collected data, carried out the initial analyses, and critically reviewed and revised the manuscript. J.X., and M.S. collected data, contributed to follow-up and interpretation of results, and critically reviewed and revised the manuscript. W.Y. and Y.W. conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, S., Wang, P., Liu, L. et al. Comparison of different treatment modalities for perianal abscess in infants: a retrospective cohort study. Sci Rep 15, 6382 (2025). https://doi.org/10.1038/s41598-025-89921-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89921-1
