
Abstract
Tuberculosis (TB) among hospitalized patients is underdiagnosed. This study assessed systematic TB-screening, followed by an enhanced TB-diagnostic package for hospitalized patients implemented by trained lay health workers in KwaZulu-Natal, South Africa. In this before-and-after study we included patients ≥ 18 years. The intervention consisted of systematic clinical screening for TB, HIV and diabetes mellitus by lay health workers and provision of an enhanced TB-diagnostic package including sputum Xpert MTB/Rif Ultra, urine lateral-flow lipoarabinomannan assay (LF-LAM), chest x-ray, and sputum culture. We compared TB case findings with people hospitalized one year preceding the intervention. In the pre-intervention phase, 5217 people were hospitalized. Among 4913 (94.2%) people not on TB treatment, 367 (7.5%) were diagnosed with TB. In the intervention phase, 4015 eligible people were hospitalized. Among 3734 (93.0%) people not on TB treatment, 560 (15.0%) were diagnosed with TB. The proportion of patients diagnosed with TB was higher in the intervention phase (15.0% vs. 7.5%, p < 0.001). Overall in-hospital mortality was lower in the intervention phase [166/3734(4.5%) vs. 336/4913(6.8%), p < 0.001]. Lay health worker-led implementation of systematic TB-screening, coupled with provision of an enhanced TB-diagnostic package significantly improved TB case detection and mortality among hospitalized adults.
Similar content being viewed by others
Background
Tuberculosis (TB) is a leading cause of global morbidity and mortality, with more than ten million people becoming sick with TB, of whom an estimated 1.3 million died in 20221. Studies show that even with newer TB diagnostic tools, up to one-third of people living with TB remain undiagnosed1,2. In hospitalized patients, TB diagnosis is often delayed, with as many as 50% of patients being “missed” despite being in a healthcare setting3,4.
Rapid improvement in TB case finding is necessary to achieve the global reduction targets in TB morbidity and mortality laid out in the endTB strategy5. Achieving these goals will require more effective screening tools and more sensitive and specific point-of-care diagnostic tests. There is also a need for more effective implementation strategies to deploy these tools6. Especially the role of lay health workers (LHW) may play an essential role in improving TB screening.
A LHW is defined as any health worker carrying out functions related to health care delivery, who is trained in the context of the intervention, but who does not have formal professional training/certification7. LHWs have a long history of providing TB care services, but they are largely based in the community and involved in adherence support or patient tracing. The limited number of studies assessing LHWs based in health facilities suggest that their activities can significantly improve TB case detection8. Given the well-documented shortages in professional health worker cadres9, LHWs may have a crucial role to play in TB diagnostic efforts, especially in improving TB screening.
In addition to screening, the impact of LHWs on TB diagnosis among hospitalized patients might be enhanced when combined with point-of-care TB tests that can be performed on easy to collect samples. One such existing test is the lateral-flow lipoarabinomannan assay (LF-LAM) recommended for all hospitalized people living with HIV (PLHIV)10. The test can be done at the bedside using a urine sample and could thus be done by trained LHWs. When point-of-care diagnostic tools, such as the Xpert MTB/Rif Ultra and LF-LAM are coupled, TB diagnosis among PLHIV increases by 17–25.9%; the addition of chest X-ray increases the diagnostic yield by an additional 10%11,12.
In 2018, South Africa issued guidelines recommending the use of LF-LAM for critically ill hospitalized patients with HIV, but there was limited implementation13.
In addition to TB, other illnesses, especially Diabetes Mellitus, play a major role in morbidity and mortality in people living with HIV in South Africa15. Multimorbidity has been increasing, with significant comorbidity between HIV, TB and non-communicable diseases (NCDs)14,15. According to the latest WHO data, NCDs were estimated to account for over 50% of all deaths in the country in 201616.
Systematic implementation of TB and NCD screening among hospitalized patients in high burden settings remains challenging. While there are a variety of reasons for this, one may be that existing facility staff are too overwhelmed to systematically screen all patients and to perform all available diagnostic TB tests among those who are eligible17. We explored an LHW-led intervention of systematic screening for TB, HIV and diabetes mellitus (DM), followed by the provision of an enhanced TB diagnostic package including urine LF-LAM, Xpert MTB/Rif Ultra, and chest X-ray for hospitalized patients in the high TB and HIV burden setting of KwaZulu-Natal, South Africa.
Methods
Setting
This study was conducted in two hospitals (Eshowe and Mbongolwane) in King Cetshwayo District, KwaZulu-Natal, South Africa. King Cetshwayo District has a high HIV prevalence, estimated at 26.4% of adults aged between 15 and 59 years in 201818. At the time the study started in 2018, the prevalence of TB was reported to be 717 per 100,000 people19. Médecins Sans Frontières (MSF) has run an HIV/TB project in this area since 2011 and supported both hospitals with HIV and TB care. Eshowe Hospital is a 460-bed district hospital located in a semi-urban area. Mbongolwane is a 196-bed hospital located in a rural area. The project area achieved the UNAIDS 90-90-90 targets in 201818.
Study design
This is a before-and-after study. The intervention included implementation of systematic screening for TB, HIV and diabetes mellitus (DM), and enhanced TB diagnostic package including urine LF-LAM, Xpert MTB/Rif Ultra, and chest X-ray. The intervention period, which was from March 2019 to March 2020 in Eshowe Hospital and from April 2019 to April 2020 in Mbongolwane Hospital, is referred to as the “intervention phase”. Pre-intervention period was defined as 12 months prior to the start of the intervention, i.e. from March 2018 to February 2019 for both hospital sites. Pre-intervention study component was a retrospective review of hospital admissions and discharge registers, and review of information collected in the South African electronic HIV and TB patient management system (TIER.Net).
Study population
The study was conducted among adult patients aged ≥ 18 years old who were admitted for acute care to the medical and infectious disease wards in Eshowe and Mbongolwane hospitals during the time periods defined above.
In the intervention phase, all consented patients ≥ 18 years old were eligible for inclusion, with the exception of persons who had been known to have active TB at the time of admission. Recruitment into the study was implemented 7 days a week. Written informed consent was sought from all eligible patients or from their next of kin if a patient had decreased consciousness due to a medical condition per attestation of their treating physician. If a person had more than one hospital admission during the 12 months of study period, consent was sought for each admission. Consent and participant information forms were available in English and isiZulu. Consented participants were followed prospectively from the date of hospital admission to date of hospital discharge or death if occurring whilst in hospital. Consented patients who were discharged from hospital before release of positive TB culture results were traced by phone and linked to care. Patients newly diagnosed with DM or HIV were also linked to care for their HIV and DM management.
In the pre-intervention phase, we included all ≥ 18 years old adults, with exclusion of patients who were known to have active TB at time of hospital admission. Eligible hospital admissions were identified through review of hospital registers and Tier.Net. For the pre-intervention component, patients’ consent was waived and approved by Ethics Review Boards.
Intervention and procedures
MSF recruited and trained six LHWs to provide systematic screening for TB, HIV and DM for patients in the intervention phase. LHWs were experienced lay workers who worked in communities with local NGOs. LHWs went through 1 day of theoretical training, followed by continuous clinical mentoring and hands-on bed-side training, done by the hospital nurses and physicians, assisted by the study coordinator. These LHWs were trained in TB screening and testing and worked in the hospitals’ inpatient wards. They were paid according to the South African community LHW wages.
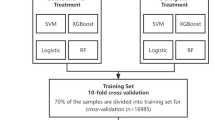
The screening and diagnostic algorithm is depicted in Fig. 1.

Diagnostic algorithm for TB screening among hospitalized patients in KwaZulu Natal, South Africa. TB tuberculosis, LHW lay health workers, PICT provider-initiated HIV counseling and testing, DM diabetes mellitus, RBS random blood sugar, HbA1C hemoglobin A1C, FBS fasting blood sugar, Xpert Xpert MTB/RIF Ultra, CXR chest X-ray, LF-LAM lateral flow urine lipoarabinomannan assay.
TB testing algorithm included systematic utilization of LF-LAM, Xpert MTB/Rif (Xpert), culture for Mycobacterium tuberculosis and drug susceptibility testing, and chest x-ray. TB testing protocol was aligned with South Africa guidelines13,20. In addition, this study intervention included the following components: (i) Xpert for all patients with HIV, DM or suspects of tuberculosis, (ii) Chest x-ray for all patients with HIV infection, DM, and suspected TB, and (iii) LF-LAM for all HIV positive patients irrespective of presence of advanced HIV disease.
For DM screening, LHWs were trained to measure random blood sugar (RBS) for all patients and assess for symptoms or history of DM. HbA1c or fasting blood sugar was done for those with RBS ≥ 11.1 mmol/L. HbA1c was measured for patients known to have DM before admission to determine their glycemic control. The Society for Endocrinology, Metabolism, and Diabetes of South Africa guidelines were followed for the diagnosis of DM21.
We systematically assessed the HIV status of the patients through clinical history and medical file review. LHW performed HIV testing for those with unknown status. South African national HIV counseling and testing policy guideline was followed for HIV testing22.
LHW provided TB health education, including an explanation of TB screening questions. They then screened for the presence of TB symptoms, including cough of any duration, fever of any duration, weight loss in the last one month, or night sweats. They showed a video on how to produce quality sputum samples for all patients with HIV, DM, or those patients who reported at least one TB symptom. They collected sputum for the Xpert test. All procedures were conducted by the LHWs in the wards where the patients were admitted, supervised by the DoH ward nurse. Sputum sample processing and quality assurance were performed according to the standards of the South African National Health Laboratory Service23.
Patients who had at least one TB symptom, HIV, or DM also had a posterior-anterior chest X-ray (CXR). The attending medical officers read the CXRs. If there was ambiguity about the CXR findings, telemedicine radiology support was provided by MSF.
Patients who were known or newly diagnosed HIV-positive underwent bedside urine LF-LAM testing irrespective of CD4 count or symptoms. LF-LAM diagnostic procedure was done by the LHW according to the manufacturer’s recommendation and South African guidelines13,24.
TB culture was done as described in Fig. 1. Genotypic testing for resistance to isoniazid, rifampicin, fluoroquinolones, and the injectable class of medications was done using line-probe assay testing in all persons found to have rifampicin resistant (RR)-TB on Xpert test.
Table 1 summarizes the screening and diagnostic tests done in the pre-intervention and intervention phases. In the pre-intervention phase, practice differed from the South African guidelines in that symptom-based screening was not systematically done, and LF-LAM wasn’t done despite the introduction of a policy to do LF-LAM for selected patients in 201813. Task-shifting to LHWs was done in the intervention phase, while pre-intervention, nurses were assigned these tasks.
TB diagnosis was determined, and treatment was started by the attending medical officers. TB was classified based on the method of diagnosis, site of TB, and rifampin sensitivity. For analysis, TB diagnosis was considered (i) microbiologically confirmed if patient had positive smear microscopy, culture or Xpert; (ii) LF LAM confirmed if the grade of the test was 1 or higher; (iii) radiologically confirmed if the CXR showed findings suggestive of TB. Patients were considered to be clinically diagnosed if they had clinical findings suggestive of TB and the treating physician decided to initiate TB treatment, and neither the Xpert, culture, CXR, nor LF-LAM were positive. TB treatment was provided based on the South African national guidelines20.
Outcomes
The outcomes of the study were the number of newly diagnosed TB cases, time from admission to TB treatment initiation, and all-cause in-hospital mortality during 12-months period. The primary outcomes during the intervention period were compared with pre-intervention period. The secondary outcomes were prevalence of DM, HIV infection, and TB, each as an individual condition and as comorbidities, among hospitalized patients during the 12 months intervention period.
Data collection and analysis
In the intervention phase, we prospectively recorded the patients’ demographic, clinical and laboratory tests data using standard pretested data form. If a patient had repeat admissions during the study period, data was collected for each eligible hospital admission.
For the pre-intervention phase, we retrospectively collected data on demographic characteristics, dates of admission and discharge, TB diagnosis, and discharge outcomes from hospital admission and discharge registers. For patients who had evidence of a diagnosis of TB in admission and discharge registers, additional information on the date of diagnosis, type of TB, TB site, methods of TB diagnosis, date of TB treatment initiation, HIV status, CD4 count, and DM status was collected from the South African electronic patient management system (TIER.Net) or patient files. Information on HIV status and DM was collected only for newly diagnosed TB patients in pre-intervention phase (i.e. not collected for all admitted patients).
Demographic characteristics of enrolled patients and outcomes were described and compared using descriptive statistical methods. Methods of TB diagnosis among new TB cases were compared between study’s phases and displayed using Venn diagrams. Categorical data were compared using Chi-square or Fisher’s exact tests, as appropriate, continuous variables were compared using Wilcoxon rank-sum test. In all statistical tests, p-values ≤ 0.05 were considered significant.
Patient information for both study phases was entered in a study database designed in Epi-InfoTM 7 (CDC, Atlanta). Data analysis was done using STATA version 15 (StataCorp, College Station, TX).
Ethics
The study was approved by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal, South Africa (BFC/109/18) and the MSF Ethics Review Board (Geneva, Switzerland) (ID: 1833).
Results
Study population
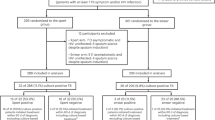
A total of 10,159 eligible patients were admitted to both hospitals during the study period (Fig. 2). In the pre-intervention phase, 5217 eligible patients were admitted, of whom 304 (5.8%) were excluded because they were already on TB treatment. A total of 4913 patients [median age 50 years (IQR 32–67); 56.6% females] were included. Out of these, 367 (7.5%) patients were diagnosed with TB. In the intervention phase, 4942 eligible patients were admitted, among whom 4015 (81.2%) provided consent; 281 (7.0%) were excluded because they were already on TB treatment; 3734 patients [median age 51 years (IQR 33–68); 62.0% females] were included. Out of these, 560 (15.0%) patients were diagnosed with TB. The age distribution of people included in the study was similar between the intervention and non-intervention phase (median age 50 years, IQR 32–67 vs. median age 51 years, IQR 33–68 respectively (p = 0.053), but the proportion of females included in the intervention phase was higher than the pre-intervention phase (62.0% vs. 56.6%, p < 0.001).

Cascade of TB screening by lay health workers among hospitalized patients in KwaZulu-Natal, South Africa. TB tuberculosis.
Newly diagnosed TB cases
560/3734 (15.0%) of patients in intervention phase and 367/4913 (7.8%) in pre-intervention were newly diagnosed with TB during hospital admission (p < 0.001). TB patients in intervention phase were older as compared to pre-intervention (median age 43 years old vs 40 years old, p = 0.004), (Table 2). Newly diagnosed TB patients in pre-intervention phase had higher proportion of those with unknown HIV or DM status (Table 2). Out of those whose status was known, the proportion of those with HIV infection or DM did not differ between two study phases (intervention vs pre-intervention: HIV, 73 vs 74%, p = 0.67; DM, 8.8 vs 5.6%, p = 0.11).
41% (230/560) of new TB cases in intervention phase were LF LAM positive. As compared to pre-intervention, newly diagnosed TB patient in the intervention phase had similar proportion of microbiologically confirmed disease [119 (21%) vs 87(24%), p = 0.29) and higher proportion of chest X-ray confirmation [422 (80%) vs 189 (51%), p < 0.001). Consequently, TB patients in intervention phase had fewer people diagnosed on clinical grounds alone [49 (8.8%) vs 94 (26%) p < 0.001] (Fig. 3). Out of those diagnosed clinically, 26/94 (27.7%) in the pre-intervention group and 38/49 (77.6%) in the intervention group were diagnosed with EPTB.

TB diagnosis by diagnostic tests among hospitalized patients in KwaZulu-Natal, n (%). (A) Pre-intervention (n = 367) and (B) intervention (n = 560). CXR chest X-ray, GXP gene-Xpert, LF-LAM lateral flow urine lipoarabinomannan assay.
Comorbidities
The overlap of TB, HIV, and DM in the intervention phase is depicted in Fig. 4. Out of the 3734 patients included in the intervention, 1346 (36.0%) were HIV-positive, 706 (18.9%) had diabetes, and 560 (15.0%) were newly diagnosed with TB during this admission. Among patients with TB, 402 (71.8%) were HIV-positive, and 49 (8.8%) had DM; among the HIV-positive, 402 (29.9%) were newly diagnosed with TB and 114 (8.5%) had DM; and among those with DM, 114 (16.1%) had HIV and 49 (6.9%) were diagnosed with TB.

Overlap of HIV, DM, and TB among patients in intervention phase among patients hospitalized in KwaZulu Natal, South Africa (total number = 3734), n (% total participants). DM diabetes mellitus, TB tuberculosis.
Outcomes
Among those diagnosed, 361 (98.4%) in the pre-intervention and 556 (99.3%) in the intervention group were initiated on TB treatment during hospitalization. The median time from admission to TB treatment initiation was two days (IQR: 0–5) in the pre-intervention phase and 2 days (IQR: 0–4) in the intervention phase. Most of the patients enrolled in the study started TB treatment within 30 days of admission [369 (99.2%) in the pre-intervention phase (min–max 0–44 days), and 557 (99.5%) in the intervention phase (min–max 0–62 days)].
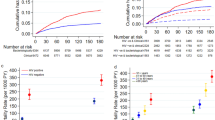
The overall in-hospital mortality of the patients included in the study was significantly lower in the intervention phase compared with the pre-intervention phase [166/3734(4.4%) vs. 336/4913(6.8%), p < 0.001].
Discussion
In this study, we demonstrate that enhanced TB screening and diagnostic package that relied on all available TB testing methods was associated with a significant two-fold increase in number of newly diagnosed TB cases among patients admitted for acute hospital care. The findings of this study support calls for increased access to point-of-care TB tests that rely on easy to collect samples in order to improve testing coverage and timely treatment initiation25. We demonstrated the access to TB testing could be improved through addressing shortage of nursing staff and tasks shifting to trained lay health workers. In our study, trained LHWs effectively administrated LF-LAM to hospitalized patients.
Our study adds to available evidence that adding LF LAM to initial TB diagnostic tests among HIV-positive patients could diagnose notable number of TB disease, who otherwise could be missed12,26. The improvement in TB diagnosis in our study is also consistent with the result of the STAMP trial in which the addition of LF-LAM to the TB diagnostic algorithm in HIV-positive patients in South Africa and Malawi improved TB case-finding27. However, our study differs from the STAMP trial in that our study is an implementation study and LHW administered LF-LAM and other screening tasks. Compared with the pre-intervention group, a lower proportion of patients in the intervention group were diagnosed on clinical grounds alone. Of note, most of the patients diagnosed clinically in the intervention group had EPTB. Similar results have also been reported in other studies in which the certainty of diagnosis of TB improved when the TB diagnostic algorithm included the use of urinary LF-LAM, particularly in sputum-scarce patients28,29. Increased certainty in TB diagnosis might have downstream positive effects for patients, as studies with other diseases show that the certainty of diagnosis may improve adherence30. Although this would need to be formally assessed in persons living with TB, it represents another compelling reason to increase access to improved TB tests.
Over half of hospital admissions had HIV, DM, TB, or a combination of the three diseases. Two-thirds of patients with TB were HIV-positive, which is consistent with previous reports from the province31 and one-third of those living with HIV were newly diagnosed with TB, highlighting the importance of providing integrated care. Prevalence of DM in our intervention cohort was 18.9% what was generally in agreement DM burden estimates ranging from 10 to 22% from other studies in the country32,33.
The important finding from our study is that the overall in-hospital mortality in the intervention phase was significantly lower than in the pre-intervention phase. Our intervention that included TB, HIV and DM diagnostics (Fig. 1) and rapid initiation of relevant treatment may have contributed to this observation. These findings are consistent with modelling studies which show that enhanced techniques of TB diagnosis that rely on active case finding and rapid molecular testing, can reduce TB mortality34,35. In pre-intervention phase we observed higher proportion of patients with unknown DM status which mirrors concerns of others regarding underdiagnosis and gaps in DM care in South Africa32,36. Contextual factors such as improved ART coverage in our area18 may have also contributed to the observed reduction in mortality seen in this study. Although our study design limits our ability to make causal inferences, the decreased in-hospital mortality suggests a notable benefit for patients that should be further assessed.
Our study utilized trained, supervised, and paid LHWs to deliver much of the screening and point-of-care testing in the intervention period. They also facilitated the sample collection and logistics for the other TB diagnostic tests, working in partnership with nurses and medical officers. The presence of this cadre of healthcare workers was likely an important part of the success of the overall intervention. Other studies have shown the effectiveness of LHWs in inpatient settings, but these are largely from the era before the use of LF-LAM and Xpert MTB/Rif Ultra37,38. Our study also expanded the role of LHWs beyond what is sometimes described in the literature as “cough officers” focused only on symptom screening or sample collection39. The range of activities LHWs can take on can include both HIV and TB testing40 and our findings support expanding their work to inpatient settings and NCD screening as part of disease programs integration and overall health systems strengthening.
Health system weaknesses in the diagnostic approach to TB, including shortages of physicians and nurses enhance the importance to task-shift work to LHWs41,42. The LHWs were a key part of this intervention, however, facility LHW are not existing cadres within the Department of Health system, so their positions were not maintained after the study. There is a need for professionalizing and formalizing this important cadre of healthcare paraprofessionals.
This study has several limitations. Improvements in care over the study period might have contributed to improvement in TB diagnosis and mortality as we used a historical comparison group. Data in the pre-intervention phase was collected retrospectively. TB, HIV and DM screening were not done systematically and as such, screening information was often missing in the pre-intervention phase, which might have introduced biases. In the intervention phase, 12.8% of the patients were not able to give consent, and 6% declined to participate. One of the reasons was a notable number of patients with psychiatric conditions admitted to the medical wards who were not able to provide consent. It may be that these groups of patients were fundamentally different from those included, and they could have had both higher or lower rates of TB, or different outcomes. Furthermore, this study’s intervention was a complex intervention and it is difficult to determine which component(s) of the intervention might have been more effective in improving TB case detection.
Conclusion
The implementation of LHW-supported, systematic screening for TB, HIV, and DM with the provision of an enhanced package of diagnostic tests, including LF-LAM, Xpert, CXR, and/or TB culture for patients with TB symptoms, DM, or HIV, improved TB case finding among hospitalized patients. Task shifting of a major part of the screening and testing package to LHWs sets this intervention apart and turns the implementation of an enhanced TB diagnostic package into a success without overburdening medical staff, offering a potential solution to improve widespread implementation of enhanced TB screening.
Data availability
Data are available on request in accordance with MSFs data sharing policy. Requests for access to data should be made to data.sharing@msf.org. For more information please see: 1/ MSFs data sharing policy: https://www.msf.org/sites/msf.org/files/msf_data_sharing_policycontact_infoannexes_final.pdf 2/ MSFs data sharing policy PLOS Medicine article:https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1001562.
Abbreviations
- ART:
-
Anti-retroviral therapy
- CXR:
-
Chest X-ray
- DM:
-
Diabetes mellitus
- DoH:
-
Department of Health
- DSTB:
-
Drug sensitive tuberculosis
- EPTB:
-
Extrapulmonary tuberculosis
- FBS:
-
Fasting blood sugar
- HBA1C:
-
Glycated haemoglobin
- IQR:
-
Interquartile range
- LF-LAM:
-
Lateral flow urine lipoarabinomannan assay
- LHW:
-
Lay health worker
- MO:
-
Medical officer
- MSF:
-
Médecins sans Frontières
- NCD:
-
Non-communicable disease
- PLHIV:
-
People living with HIV
- PTB:
-
Pulmonary tuberculosis
- RBS:
-
Random blood sugar
- RR-TB:
-
Rifampicin-resistant tuberculosis
- TB:
-
Tuberculosis
- WHO:
-
World Health Organization
- Xpert ultra:
-
Xpert MTB/RIF Ultra
References
WHO. Global tuberculosis report 2023. World Health Organization. (2023).
Walzl, G. et al. Tuberculosis: advances and challenges in development of new diagnostics and biomarkers. Lancet Infect. Dis. 18, e199–e210. https://doi.org/10.1016/S1473-3099(18)30111-7 (2018).
Cohen, T. et al. The prevalence and drug sensitivity of tuberculosis among patients dying in hospital in KwaZulu-Natal, South Africa: a postmortem study. PLoS Med. 7, e1000296. https://doi.org/10.1371/journal.pmed.1000296 (2010).
Wong, E. B. et al. Causes of death on antiretroviral therapy: a post-mortem study from South Africa. PLoS One 7, e47542. https://doi.org/10.1371/journal.pone.0047542 (2012).
WHO. Implementing the End TB Strategy: The Essentials 2022. World Health Organization. (2022). https://www.who.int/publications/i/item/9789240065093 (accessed 20/02/2025).
Vesga, J. F. et al. Assessing tuberculosis control priorities in high-burden settings: a modelling approach. Lancet Glob. Health 7, e585–e595. https://doi.org/10.1016/S2214-109X(19)30037-3 (2019).
Lewin, S. A. et al. Lay health workers in primary and community health care. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD004015.pub2 (2005).
Jose, B. et al. Using community health workers for facility and community based TB case finding: An evaluation in central Mozambique. PLoS One 15, e0236262. https://doi.org/10.1371/journal.pone.0236262 (2020).
Human Resources for Health strategy. Investing in the Health Workforce for Universal Health Coverage (National Department of Health, 2020).
WHO. The use of lateral flow urine lipoarabinomannan assay (LF-LAM) for the diagnosis and screening of active tuberculosis in people living with HIV: policy guidance. World Health Organization. (2015).
Broger, T. et al. Diagnostic yield of urine lipoarabinomannan and sputum tuberculosis tests in people living with HIV: a systematic review and meta-analysis of individual participant data. Lancet Glob. Health 11, e903–e916. https://doi.org/10.1016/S2214-109X(23)00135-3 (2023).
Huerga, H. et al. Incremental yield of including determine-TB LAM assay in diagnostic algorithms for hospitalized and ambulatory HIV-positive patients in Kenya. PLoS One 12, e0170976. https://doi.org/10.1371/journal.pone.0170976 (2017).
Guidance on the use of Lateral Flow Urine Lipoarabinomannan (LF-LAM) assay for the diagnosis of tuberculosis in people living with HIV. National Department of Health, Republic of South Africa. (2018). https://knowledgehub.health.gov.za/elibrary/guidance-use-lateral-flow-urine-lipoarabinomannan-assay-lf-lam-diagnosis-and-management (accessed 20/02/2025).
Weimann, A., Dai, D. & Oni, T. A cross-sectional and spatial analysis of the prevalence of multimorbidity and its association with socioeconomic disadvantage in South Africa: A comparison between 2008 and 2012. Soc. Sci. Med. 163, 144–156. https://doi.org/10.1016/j.socscimed.2016.06.055 (2016).
Roomaney, R. A., van Wyk, B., Turawa, E. B. & Pillay-van Wyk, V. Multimorbidity in South Africa: a systematic review of prevalence studies. BMJ Open 11, e048676. https://doi.org/10.1136/bmjopen-2021-048676 (2021).
Mortality and causes of death in South Africa: Findings from death notification. Department Statistics South Africa, Statistical Release P0309.3. (2019). https://www.statssa.gov.za/publications/P03093/P030932020.pdf (accessed 20/02/2025).
Salifu, R. S. & Hlongwana, K. W. Barriers and facilitators to bidirectional screening of TB-DM in Ghana: Healthcare workers’ perspectives. PLoS One 15, e0235914. https://doi.org/10.1371/journal.pone.0235914 (2020).
Conan, N. et al. Increase in HIV viral suppression in KwaZulu-Natal, South Africa: Community-based cross sectional surveys 2018 and 2013. What remains to be done?. PLoS One 17, e0265488. https://doi.org/10.1371/journal.pone.0265488 (2022).
Conan, N. et al. Prevalence of TB and health-seeking behaviour. Int. J. Tuberc. Lung Dis. 26, 463–465. https://doi.org/10.5588/ijtld.22.0001 (2022).
National Tuberculosis Management Guidelines. National Department of Health, Republic of South Africa. (2014).
SEMDSA. SEMDSA 2017 guidelines for the management of type 2 diabetes mellitus. J. Endocrinol. Metab. Diabetes S. Afr. 22, S1–S196 (2017).
National HIV counselling and testing policy guidelines. National Department of Health, Republic of South Africa. (2015). https://www.nicd.ac.za/assets/files/HCT-Guidelines-2015.pdf (accessed 20/02/2025).
Primary Healthcare Laboratory Handbook, a Step-by-Step Guide. National Department of Health, Republic of South Africa. (2018).
Abbot. Alere DetermineTM TB LAM Ag Product Information. alere.com/en/home/product‐details/determine‐tb‐lam.html. (Accessed 24 Nov 2024). (2017).
Pai, M., Dewan, P. K. & Swaminathan, S. Transforming tuberculosis diagnosis. Nat. Microbiol. 8, 756–759. https://doi.org/10.1038/s41564-023-01365-3 (2023).
Talbot, E. et al. Test characteristics of urinary lipoarabinomannan and predictors of mortality among hospitalized HIV-infected tuberculosis suspects in Tanzania. PLoS One 7, e32876. https://doi.org/10.1371/journal.pone.0032876 (2012).
Gupta-Wright, A. et al. Rapid urine-based screening for tuberculosis in HIV-positive patients admitted to hospital in Africa (STAMP): a pragmatic, multicentre, parallel-group, double-blind, randomised controlled trial. Lancet 392, 292–301. https://doi.org/10.1016/S0140-6736(18)31267-4 (2018).
Lawn, S. D. et al. Diagnostic accuracy, incremental yield and prognostic value of Determine TB-LAM for routine diagnostic testing for tuberculosis in HIV-infected patients requiring acute hospital admission in South Africa: a prospective cohort. BMC Med. 15, 67. https://doi.org/10.1186/s12916-017-0822-8 (2017).
Sabur, N. F., Esmail, A., Brar, M. S. & Dheda, K. Diagnosing tuberculosis in hospitalized HIV-infected individuals who cannot produce sputum: is urine lipoarabinomannan testing the answer?. BMC Infect. Dis. 17, 803. https://doi.org/10.1186/s12879-017-2914-7 (2017).
Backer, V., Stensen, L., Sverrild, A., Wedge, E. & Porsbjerg, C. Objective confirmation of asthma diagnosis improves medication adherence. J. Asthma 55, 1262–1268. https://doi.org/10.1080/02770903.2017.1410830 (2018).
Strategic Plan 2015–2019. National Department of Health, Republic of South Africa. (2015).
Grundlingh, N., Zewotir, T. T., Roberts, D. J. & Manda, S. Assessment of prevalence and risk factors of diabetes and pre-diabetes in South Africa. J. Health Popul. Nutr. 41, 7. https://doi.org/10.1186/s41043-022-00281-2 (2022).
Sifunda, S. et al. Prevalence and psychosocial correlates of diabetes mellitus in South Africa: Results from the South African National Health and Nutrition Examination Survey (SANHANES-1). Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph20105798 (2023).
Dowdy, D. W., Chaisson, R. E., Moulton, L. H. & Dorman, S. E. The potential impact of enhanced diagnostic techniques for tuberculosis driven by HIV: a mathematical model. AIDS 20, 751–762. https://doi.org/10.1097/01.aids.0000216376.07185.cc (2006).
Kubjane, M., Osman, M., Boulle, A. & Johnson, L. F. The impact of HIV and tuberculosis interventions on South African adult tuberculosis trends, 1990–2019: a mathematical modeling analysis. Int. J. Infect. Dis. 122, 811–819. https://doi.org/10.1016/j.ijid.2022.07.047 (2022).
Brennan, A. T. et al. Gaps in the type 2 diabetes care cascade: a national perspective using South Africa’s National Health Laboratory Service (NHLS) database. BMC Health Serv. Res. 23, 1452. https://doi.org/10.1186/s12913-023-10318-9 (2023).
Cardarelli, R. et al. Reducing 30-day readmission rates in a high-risk population using a lay-health worker model in Appalachia Kentucky. Health Educ. Res. 33, 73–80. https://doi.org/10.1093/her/cyx064 (2018).
Basnight, R. et al. Evaluation of lay health workers on quality of care in the inpatient setting. PLoS One 18, e0293068. https://doi.org/10.1371/journal.pone.0293068 (2023).
Lin, C. H. et al. “Cough officer screening” improves detection of pulmonary tuberculosis in hospital in-patients. BMC Public Health 10, 238. https://doi.org/10.1186/1471-2458-10-238 (2010).
Ndlovu, Z. & Ellman, T. Lay testing cadres and point-of-care diagnostic tests for HIV and other diseases: An essential combination in health service delivery. PLoS Med 18, e1003867. https://doi.org/10.1371/journal.pmed.1003867 (2021).
WHO. Systematic Screening for Active Tuberculosis: Principles and Recommendations. World Health Organization. (2013).
Ahmad Khan, F. et al. Performance of symptom-based tuberculosis screening among people living with HIV: not as great as hoped. AIDS 28, 1463–1472. https://doi.org/10.1097/QAD.0000000000000278 (2014).
Author information
Authors and Affiliations
Contributions
Conceived the study and wrote the protocol: AS, GVC, SJS, CL, JF, PI, LO Collected the data: ABB, Performed the analysis: ABB, AYD, AS, CL Wrote the main manuscript: ABB, JF, PI, LO reviewed the manuscript: ABB, AYD, AS, GVC, SJS, MSB, MM, CL, JF, PI, LO.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bulti, A.B., Dumicho, A.Y., Shigayeva, A. et al. Enhancing tuberculosis (TB) case detection among hospitalized patients through lay health worker led screening: a before-and-after study in KwaZulu-Natal, South Africa. Sci Rep 15, 14140 (2025). https://doi.org/10.1038/s41598-025-90497-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-90497-z
