
Abstract
Tracheal, bronchial, and lung cancer (TBL) is among the most common malignancies worldwide, with persistently high incidence and mortality rates, posing a significant threat to public health. However, existing studies on TBL disease burden are often limited to specific regions or short-term trends, lacking systematic and predictive analyses. This study comprehensively evaluated the global, regional, and national burden of TBL across 204 countries and territories from 1990 to 2021, utilizing predictive models to estimate trends from 2022 to 2035. This study used data from the Global Burden of Disease (GBD) 2021 database to systematically analyze the prevalence (ASPR), incidence (ASIR), mortality (ASMR), and disability-adjusted life years (DALYs) associated with TBL. Age-standardized rates (ASR) were used to quantify disease burden. Historical trends were assessed using Joinpoint regression analysis, while ARIMA and Bayesian age-period-cohort (BAPC) models were employed to predict future trends. The study also incorporated the Sociodemographic Index (SDI) to investigate the impact of socioeconomic development on TBL burden. In 2021, the global ASPR, ASIR, ASMR, and DALYs for TBL were 37.28, 26.43, 23.50, and 638.60 per 100,000 population, respectively. From 1990 to 2021, ASPR increased slightly (0.09 per 100,000), while ASIR, ASMR, and DALYs declined by 0.07, 0.15, and 0.23 per 100,000, respectively. Regionally, the highest ASPR was observed in the high-income Asia-Pacific region (69.79 per 100,000), while East Asia recorded the highest ASIR (43.41 per 100,000) and ASMR (38.53 per 100,000). Sub-Saharan Africa had the lowest burden. Gender analysis showed that males had a significantly higher TBL burden than females, but their burden declined over the study period. In contrast, females, particularly in older age groups, experienced an increase in burden. Future predictions indicate that the overall TBL burden will decline between 2022 and 2035; however, the burden among females and older adults is projected to rise, with a marked increase in female ASPR. This study highlights the global and regional trends in TBL burden from 1990 to 2021 and provides predictions for future burden. Although the overall burden is declining, significant disparities exist across genders and regions, with East Asia and high-income North America warranting particular attention. Females and older adults are priority groups for future interventions. The findings underscore the importance of early screening, targeted interventions, and region-specific strategies to optimize public health policies, resource allocation, and tailored prevention efforts.
Similar content being viewed by others


Introduction
Lung cancer is one of the most prevalent types of cancer worldwide. According to global cancer data from 2022, lung cancer is the leading cause of cancer-related deaths, with a five-year survival rate of less than 15% among patients1. Tracheal, bronchial, and lung cancers (TBL) have long posed a significant threat to human health. In recent years, despite substantial advancements in early diagnosis and clinical treatment of TBL2, factors such as genetic predispositions and environmental influences play a crucial role in the occurrence, metastasis, and infiltration of TBL3,4. Additionally, the aging population and tobacco exposure have intensified the global burden of TBL. Furthermore, there are notable differences in the causes contributing to the rising burden of TBL across various countries and regions5,6,7. Given the limited global public health resources, a current understanding of the burden of TBL is essential for the rational allocation of resources and the effective prevention and diagnosis of this disease.
The Global Burden of Disease (GBD) database compiles data on 369 diseases from 204 countries and territories worldwide. It serves as a crucial tool for evaluating the incidence, mortality, prevalence, and disability-adjusted life years (DALYs) associated with tracheal, bronchial, and lung cancers. In a previous study, researchers utilized the GBD database to analyze global, regional, and national disease burden trends for TBL in 20198. However, the prevalence and global burden of TBL have evolved over time. Therefore, we systematically analyzed the global disease burden of TBL using the most recent GBD data (1990–2021) to more effectively address the health threats it presents. Based on existing research, we innovatively employed two predictive models for comparative analysis to enhance the accuracy of the predictions. Furthermore, we conducted a detailed examination of the relationship between all GBD regions and the Sociodemographic Index (SDI), as well as the Expected Annual Percentage Change (EAPC) in disease burden across 204 countries. This comprehensive approach aims to provide a deeper understanding of regional and national disparities in disease burden, thereby facilitating the development of targeted policies.
Methods
Data Acquisition and download
The latest GBD data and its standardized methodology systematically analyzed 369 diseases and 88 risk factors across 204 countries and territories9. The age-standardized incidence, prevalence, mortality, and DALYs, along with their 95% uncertainty intervals (95% UI), for this study were obtained from the GBD (2021 version) database (https://vizhub.healthdata.org/gbd-results/). Additionally, sociodemographic index (SDI) data were utilized for the analyses, accounting for variations in income, education level, and fertility across different regions10.
Socio-Demographic Index (SDI)
SDI was introduced by the Institute for Health Metrics and Evaluation (IHME) in 2015 to assess the relationship between social development and population health outcomes. In the most recent GBD data, 204 countries and territories worldwide were categorized into five SDI regions: low, medium-low, medium, medium-high, and high11.
Analysis of EAPC in 204 countries (1990–2021)
To gain a deeper understanding of the temporal trends in age-standardized rates (ASR) across 204 countries from 1990 to 2021, we introduced the EAPC. The EAPC is calculated using the formula:12
where β represents the slope of the log-linear regression model. An EAPC greater than 0 indicates an increasing trend, while an EAPC less than 0 reflects a declining trend. At the national level, if the 95% confidence interval (CI) of the EAPC does not include zero, the corresponding ASR is considered to have a statistically significant upward or downward trend. Conversely, if the 95% CI includes zero, the trend is deemed non-significant. This analysis provides critical insights into the dynamic changes in ASR over time, offering valuable information for evaluating national-level progress and disparities in disease burden reduction.
SDI correlation analysis
To investigate the correlation between the SDI and the ASRs of TBL, this study employed Locally Weighted Scatterplot Smoothing (Lowess) to fit smoothed curves for the relationship between SDI and age-standardized incidence rate (ASIR), age-standardized mortality rate (ASMR), and age-standardized disability-adjusted life years rate (AS-DALYs) across 21 GBD regions and 204 countries. Additionally, Spearman correlation analysis was conducted to calculate the correlation coefficients between ASR and SDI, along with their statistical significance (P < 0.05). This systematic methodological approach integrates trend analysis with socioeconomic development indicators to provide a comprehensive perspective on the dynamics of the global TBL burden and its underlying determinants.
Joinpoint regression analysis
In this study, we employed the Joinpoint regression model to assess the trends in the prevalence and mortality of TBL over time. This model is commonly utilized in epidemiological studies13 and serves as a crucial tool for calculating the Annual Percentage Changes (APCs) and their 95% CI. These calculations enable the analysis of trends in prevalence, mortality, incidence, and DALYs over time. Conversely, the Average Annual Percentage Change (AAPC) was used to evaluate the long-term trend in APC. If the APC or AAPC, along with its 95% CI lower limit, is greater than zero, it indicates an upward trend over the specified time frame. Conversely, a downward trend is indicated if the 95% CI is close to zero, suggesting a more stable trend14.
ARIMA model predictions
ARIMA (p, d, q) model was developed to predict the trend of TBL disease burden from 2022 to 2035, utilizing data on prevalence, incidence, mortality, and DALYs for TBL from 1990 to 2021. In this context, the letters p, d, and q represent the autoregressive, differencing, and moving average components of the ARIMA model, respectively. Essentially, an ARIMA model is constructed from a set of data points that are regularly collected, recorded, or observed15,16.
Bayesian age-period-cohort model for TBL trend prediction
Bayesian age-period-cohort (BAPC) modeling, utilizing integrated nested Laplace approximations and assuming an inverse-gamma prior distribution of existing data, is a crucial method for predicting future trends in cancer17,18. Consequently, we developed a BAPC model using the ‘BAPC’ and ‘INLA’ packages along with GBD data from 1990 to 2021 to forecast the trend of TBL from 2022 to 2035.
Ethics approval
The ethics committee approved the ethical exemption for this study because it utilizes publicly available data that does not contain any confidential information or patient privacy concerns.
Statistical analyses
Age-standardized values for prevalence, incidence, mortality, and DALYs, along with their 95%UIs, are presented as predicted values per 100,000 population. All statistical analyses were conducted using R software (Version 4.4.0), while Joinpoint analyses were performed using Joinpoint software (Version 5.2.0). A p-value of less than 0.05 was considered statistically significant.
Results
Global level
In 2021, the global prevalence of TBL was 3,253,729 cases, with ASPR of 37.28 cases per 100,000 people. Between 1990 and 2021, the ASPR increased by 0.09 cases per 100,000 people (Table 1) (Fig. 1A). The global incidence of TBL was 2,280,688 cases, with an ASIR of 26.43 cases per 100,000 people. The ASIR exhibited a decreasing trend, with a rate of decline of 0.07 cases per 100,000 people during the period from 1990 to 2021 (Table 1) (Fig. 1B). The number of deaths attributed to TBL was 2,016,547 cases, with an ASMR of 23.50 deaths per 100,000 people. The ASMR showed a declining trend, with a decrease of 0.15 deaths per 100,000 people over the period from 1990 to 2021 (Table 1) (Fig. 1C). The global DALYs due to TBL in 2021 were 46,536,272 cases, and the AS-DALYs was 638.60 per 100,000 people. The AS-DALYs declined by 0.23 per 100,000 people between 1990 and 2021 (Table 1) (Fig. 1D). In summary, although the prevalence rates of TBL increased, the incidence rates, mortality rates, and DALY rates all exhibited a downward trend between 1990 and 2021. The 95%UI for all results data can be viewed in the corresponding tables.

Global disease burden of TBL, 1990–2021. (A) Prevalence numbers and ASPR. (B) Incidence numbers and ASIR. (C) Mortality numbers and ASMR. (D) DALYs numbers and AS-DALYs.
Regional level
In 2021, we conducted a systematic analysis of TBL disease status across various regions of the world. The results indicated that the ASPR for TBL was highest in regions with a high-SDI regions, reaching 64.26 cases per 100,000 people (Table 1). Geographically, the ASPR was highest in high-income regions of North America and the Asia-Pacific, with rates of 67.21 cases per 100,000 people and 69.79 cases per 100,000 people, respectively (Table 1; Fig. 2A). In contrast, Africa exhibited the lowest ASPR, with 3.68 cases per 100,000 people in the Western Sub-Saharan Africa region and 5.8 cases per 100,000 people in Eastern Sub-Saharan Africa. The overall ASPR for Saharan Africa was 5.8 cases per 100,000 people (Table 1; Fig. 2A).

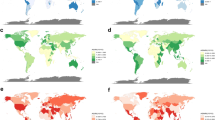
Global distribution of TBL disease burden in 2021. (A) Age-standardized prevalence rates. (B) Age-standardized incidence rates. (C) Age-standardized mortality rates. (D) Age-standardized DALYs rates.
Between 1990 and 2021, the global ASPR for TBL showed a slight upward trend of 0.09 cases per 100,000 people, with varying trends observed across different regions. Among the five SDI regions, only the low SDI region demonstrated a decreasing trend in ASPR, with a rate of 0.01 cases per 100,000 people. Geographically, East Asia experienced the most significant increase in ASPR for TBL, with a rate of 0.71 cases per 100,000 people, followed by the high-income Asia-Pacific region, which recorded an increase of 0.41 cases per 100,000 people. The regions exhibiting the most pronounced decreasing trends were Southern Latin America and high-income North America, with rates of decline of 0.27 cases per 100,000 people and 0.30 cases per 100,000 people, respectively (Table 1). The regions with the highest ASIR were East Asia (43.41 cases per 100,000 people, 95% UI: 35.14–52.35) and High-Income North America (37.21 cases per 100,000 people, 95% UI: 34.50-38.95). Among the five SDI regions, the ASIR was highest in the high SDI and medium-high SDI regions, with rates of 34.64 cases per 100,000 people and 36.41 cases per 100,000 people, respectively (Table 1; Fig. 2B).
In 2021, among different SDI regions, the ASMR for TBL was highest in high SDI regions, at 27.31 cases per 100,000 people. Conversely, the ASMR was lowest in low SDI regions, at 5.91 cases per 100,000 people. Regionally, the ASMR was highest in East Asia, at 38.53 cases per 100,000 people, followed by high-income North America, with 28.92 cases per 100,000 people (Table 1; Fig. 2C). Notably, the number of TBL deaths in East Asia has continued to rise from 1990 to 2021, at a rate of 0.12 cases per 100,000 people. The most significant increase occurred in Western Sub-Saharan Africa, with a rate of 0.18 cases per 100,000 people. In contrast, the most pronounced decline in ASMR during the same period was observed in the southern region of Latin America, with a rate of 0.32 deaths per 100,000 population (Table 1).
In 2021, the AS-DALYs for TBL across various regions of the world exhibited an overall decreasing trend. Among the five SDI regions, the highest AS-DALYs were recorded in the middle and high SDI regions, with rates of 762.67 cases per 100,000 people. Conversely, the lowest AS-DALYs were observed in the low SDI regions, at 147.55 cases per 100,000 people. Within the regions, Central Europe reported the highest AS-DALYs at 896.35 cases per 100,000 people, while Western Sub-Saharan Africa had the lowest AS-DALYs at 98.80 cases per 100,000 people (Table 1; Fig. 2D). Overall, AS-DALYs for TBL demonstrated a declining trend in most regions of the world from 1990 to 2021, with the most significant reduction occurring in Southern Latin America, which saw a decrease of 0.38 cases per 100,000 people. However, the rate of DALYs increased in certain regions, such as Western Sub-Saharan Africa, which experienced an increase of 0.14 cases per 100,000 people (Table 1). The 95%UI for all results data can be viewed in the corresponding tables.
National level
In 2021, the global TBL ASPR was approximately 33 to 40 cases per 100,000 people. Notably, Monaco had the highest ASPR at 123.49 cases per 100,000 people, followed by France (89.26 cases per 100,000 people), Japan (71.23 cases per 100,000 people), Croatia (68.43 cases per 100,000 people), Iceland (67.65 cases per 100,000 people), and Canada (67.60 cases per 100,000 people) (Supplementary Table 1S1). In contrast, Nigeria (1.31 cases per 100,000 people), Malawi (2.40 cases per 100,000 people), The Gambia (2.95 cases per 100,000 people), Kenya (3.15 cases per 100,000 people), Côte d’Ivoire (3.71 cases per 100,000 people), and Niger (3.84 cases per 100,000 people) had the lowest ASPR (Supplementary Table 1S1). Additional TBL ASPR values for other countries can be found in Supplementary Table 1S1. Changes in ASPR between 1990 and 2021 varied significantly by country. Egypt (1.30 cases per 100,000 people) and the Republic of Korea (1.28 cases per 100,000 people) exhibited the most notable increases. The most significant decrease in ASPR was observed in Kazakhstan (0.63 cases per 100,000 people) and Uzbekistan (0.60 cases per 100,000 people) (Supplementary Table 1S2). The countries with the highest ASIR were Monaco (76.86 cases per 100,000 people) and Greenland (63.31 cases per 100,000 people). In contrast, the countries with the lowest ASIR were Nigeria (1.40 cases per 100,000 people) and Malawi (2.42 cases per 100,000 people) (Supplementary Table 1S3). The countries that experienced the most significant increase in ASIR between 1990 and 2021 were Egypt (1.46 cases per 100,000 people) and Lesotho (1.01 cases per 100,000 people). Conversely, Kazakhstan (0.63 cases per 100,000 people) and Kyrgyzstan (0.59 cases per 100,000 people) showed the most significant declines in ASIR (Supplementary Table 1S4).
In 2021, the global ASMR for TBL was 21–25 deaths per 100,000 people. Among the countries, Monaco reported an ASMR of 64.05 cases per 100,000 people, and Greenland had an ASMR of 63.94 cases per 100,000 people, both significantly exceeding the global average. In contrast, Nigeria recorded an ASMR of 1.52 cases per 100,000 people, and Malawi had an ASMR of 2.57 cases per 100,000 people, indicating lower rates (Supplementary Table 1S5). Over the period 1990–2021, Egypt (1.51 cases per100,000 people) had the most significant rise in ASMRs and Kazakhstan (0.63 cases per100,000 people) had the most significant decrease in ASMR (Supplementary Table 1S6). In terms of AS-DALYs, Greenland reported the highest rate at 1,525.23 cases per 100,000 people, while Nigeria had the lowest rate at 35.33 cases per 100,000 people (Supplementary Table 1S7). Additionally, Egypt experienced the most significant increase in AS-DALYs, with a rate of 1.21 cases per 100,000 people, whereas Kazakhstan recorded the most substantial decrease in AS-DALYs, with a rate of 0.66 cases per 100,000 people during the period from 1990 to 2021 (Supplementary Table 1S8). The 95%UI for all results data can be viewed in the corresponding tables.
EAPC Analysis for 204 countries from 1990 to 2021
The results of the EAPC analysis indicate that from 1990 to 2021, among 204 countries globally, Egypt exhibited the most significant increases in the EAPC for TBL’s ASPR, ASIR, ASMR, and AS-DALYs, with values of 3.68, 3.99, 4.09, and 3.54, respectively. In contrast, Kazakhstan showed the most pronounced decreases, with corresponding EAPC values of -3.23, -3.22, -3.23, and − 3.59. These findings align closely with the GBD-reported results for TBL, confirming the robustness and reliability of the EAPC estimates (Fig. 3A-D).

Estimated annual ASRs for TBL from 1990–2021, combining both sexs across 204 countries. (A) ASPR, (B) ASIR, (C) ASMR, (D) AS-DALYs. DALYs, disability-adjusted life–years.
Age and gender analysis
In 2021, the prevalence of TBL was primarily concentrated in the age group of 45 to 79 years, with the highest prevalence rate and number of cases observed in individuals aged 75 to 79 years. Among all age groups, the prevalence rate and the number of cases in males were higher than those in females (Fig. 4A). The incidence rate and the number of new cases of TBL gradually increased after the age of 30, showing a decline after the age of 79. Similarly, the incidence rate and the number of new cases remained higher in males than in females (Fig. 4B). In 2021, the mortality rate for TBL progressively increased from age 30 onwards, peaking for those aged 95 years and older, with the highest number of deaths occurring in the age group of 65 to 74 years. Overall, excluding individuals over 95 years of age, mortality rates were consistently higher in men than in women across all age groups (Fig. 4C). The overall trend in the rates and numbers of DALYs mirrored that of the incidence rates, and the gender distribution was generally consistent with both prevalence and incidence rates (Fig. 4D). Notably, the prevalence rate, incidence rate, mortality rate, and DALY rate were all at their highest levels for TBL in the 65 to 79 age group, and were higher in males than in females (Fig. 4A–D).

Sex- and age-structured analysis of TBL disease burden in 2021. (A) Prevalence rates and numbers. (B) Incidence rates and numbers. (C) Mortality rates and numbers. (D) DALYs rates and numbers.
Joinpoint regression analysis of TBL
Joinpoint regression analysis revealed a significant upward trend in the ASPR of TBL from 1990 to 2021 (AAPC = 0.27, 95% CI: 0.16–0.38, P < 0.001) (Supplementary Table 1S9), with the most pronounced increase occurring between 1998 and 2001 (APC = 2.33, 95% CI: 1.68–2.99, P < 0.001) (Fig. 5A and Supplementary Table 1S10). In contrast, the ASIR exhibited an overall decreasing trend (AAPC = -0.28, 95% CI: -0.36 to -0.17, P < 0.001) (Supplementary Table 1S11), with the most significant decline observed between 2011 and 2021 (AAPC = -0.82, 95% CI: -0.94 to -0.70, P < 0.001) (Fig. 5B and Supplementary Table 1S12). Similarly, the ASMR also demonstrated a general decreasing trend (AAPC = -0.26, 95% CI: -0.41 to -0.17, P < 0.001) (Fig. 5B and Supplementary Table 1S13), with the most substantial reduction occurring during the period from 2010 to 2021 (AAPC = -0.98, 95% CI: -1.08 to -0.87, P < 0.001) (Fig. 5C and Supplementary Table 1S14). The trend in AS-DALYs can reflect changes in mortality to some extent, and the results indicated that AS-DALYs generally exhibited a decreasing trend (AAPC = -0.86, 95% CI: -0.98 to -0.75, P < 0.001) during the period from 1990 to 2021 (Supplementary Table 1S15), with the most significant decrease occurring between 2004 and 2007 (AAPC = -1.49, 95% CI: -2.18 to -0.78, P < 0.001) (Fig. 5D and Supplementary Table 1S16). Further analysis by gender revealed that the ASPR, ASIR, and ASMR for females exhibited a decreasing trend throughout the remainder of the study period, with the exception of AS-DALYs, which showed an increasing trend until 2004 (Fig. 4A-C). In contrast, the ASPR for males continued to rise from 1998 to 2012, while their ASMR, ASIR, and AS-DALYs all demonstrated a downward trend (Fig. 5A-C). Males contributed more significantly to the deterioration of health outcomes in the context of TBL compared to females.

The Joinpoint regression analysis of the TBL disease burden temporal trends, 1990–2021. (A) Age-standardized prevalence rates. (B) Age-standardized incidence rates. (C) Age-standardized mortality rates. (D) Age-standardized DALYs rates.
We also conducted Joinpoint regression analyses of prevalence and mortality rates for the five regions with the highest ASPR. The results indicated that the prevalence rate was increasing in all four regions, except for High-Income North America, which exhibited a downward trend (AAPC = -0.99, 95% CI: -1.22 to -0.77, P < 0.001) (Supplementary Figure. S1A and Supplementary Table 2S1-S5). Among these regions, High-Income Australasia demonstrated the most significant upward trend between 1999 and 2002 (APC = 3.78, 95% CI: 1.26 to 6.36, P < 0.001) (Supplementary Figure. S1B and Supplementary Table 2S6). East Asia also showed a notable upward trend during the same period (APC = 3.38, 95% CI: 3.14 to 3.63, P < 0.001) (Supplementary Figure. S1C and Supplementary Table 2S7). Additionally, Western Europe experienced a significant increase in prevalence from 1998 to 2002 (APC = 3.62, 95% CI: 2.87 to 4.37, P < 0.001) (Supplementary Figure. S1D and Supplementary Table 2S8). High-Income Asia Pacific recorded the largest increase between 1998 and 2001 (APC = 5.30, 95% CI: 3.31 to 7.32, P < 0.001) (Supplementary Figure. S1E and Supplementary Table 2S9). Notably, the High-Income North America region, the only one among the five to show a downward trend, experienced the most pronounced decline between 2012 and 2019 (APC = -4.22, 95% CI: -4.55 to -3.88, P = 0.86) (Supplementary Figure. S1 A and Supplementary Table 2S10). Although the P-value is not significant, the trend remains informative.
Joinpoint regression analyses of ASMR in the five regions revealed that the mortality rate in East Asia exhibited a slow increasing trend (AAPC = 0.37, 95%Cl: 0.15 to 0.60, P = 0.001) during the period from 1990 to 2021 (Supplementary Figure. S2A and Supplementary Table 2S11). In contrast, the mortality rates in the remaining four regions demonstrated a decreasing trend (AAPC < 0) (Supplementary Figure. S2B and Supplementary Table 2S12-S15). Notably, there were interregional differences in the upward or downward trends in mortality rates across these regions. For instance, East Asia experienced the most significant increase in mortality rates between 2007 and 2011 (APC = 0.87, 95% CI: 0.16 to 1.59, P = 0.02) (Supplementary Figure. S2A and Supplementary Table 2S16). Among the regions with more pronounced downward trends in mortality rates, the High-income Australasia region exhibited the largest decline in mortality rates between 1990 and 2019 (APC = -1.30, 95% CI: -1.35 to -1.25, P < 0.001) (Supplementary Figure. S2B and Supplementary Table 2S17). Due to the lack of mortality data for 2019–2021 in the GBD database for this region, we can only analyze the change in mortality rates from 1990 to 2019. The high-income Asia Pacific region demonstrated a significant downward trend between 2012 and 2021 (APC = -1.47, 95% CI: -1.71 to -1.23, P < 0.001) and an increasing trend during the period from 1990 to 1998 (APC = 0.38, 95% CI: 0.22 to 0.55, P < 0.001) (Supplementary Figure. S2C and Supplementary Table 2S18). During the period from 2014 to 2019, the mortality rate in North America experienced the most significant decrease (APC = -3.79, 95% CI: -4.37 to -3.19, P < 0.001) (Supplementary Figure. S2D and Supplementary Table 2S19), while Western Europe saw the greatest decline between 2016 and 2021 (APC = -2.45, 95% CI: -2.94 to -1.96, P < 0.001) (Supplementary Figure. S2E and Supplementary Table 2S20). Overall, both prevalence and mortality rates exhibited distinct trends across the regions.
Overall temporal trends in gender and age structures
To better understand the impact of gender and age on the burden of TBL, we conducted a comprehensive analysis of the prevalence and mortality rates of TBL in males and females across all age groups from 1990 to 2021. Overall, the prevalence and mortality rates of TBL in all age groups exhibited an increasing trend during this period and were consistently higher in males than in females (Fig. 6A-B and Supplementary Table 1S17-S18). Similarly, both the prevalence rate and DALYs rate for TBL showed varying degrees of increase. Notably, although the DALYs rate for males exhibited a slower upward trend, it remained higher than that of females overall (Fig. 6C-D and Supplementary Table 1S19-S20). In addition, we systematically analysed Prevalence, Incidence, Mortality and DALYs as well as gender for each age group starting from the age of 15 years when Prevalence of TBL appeared and comparing the gender subgroups to analyse the trend over the period of 1990–2021 in an age interval of every 5 years. The results showed that TBL and Prevalence rates continued to decline in the 15–60 age group, with a greater decline in males than in females, with the most significant decline in the 15–19 age group, and the most pronounced upward trend in those aged 80 years and older (Fig. 7A-B and Supplementary Table 1S21-S22). Changes in Prevalence rates in other age groups can be found in Supplementary Figure. S3 and Supplementary Table 3S1-12. With the increase in global public health investment, there has been a general downward trend in Mortality rates for TBL in people under 80 years of age, except for a significant increase in Mortality rates for females in the 75–79 age group, however, the Mortality rates for TBL in people over 80 years of age continued to increase from 1990 to 2021 (Fig. 7C-D and Supplementary Table 1S23-S24). Changes in Mortality rates for other age groups can be found in Supplementary Figure. S4 and Supplementary Table 3S13-24.

Global temporal trends in TBL disease burden, 1990–2021. (A) Prevalence rates in all age groups. (B) Mortality rates in all age groups. (C) Incidence rates in all age groups. (D) DALYs rates in all age groups.

Trends in age-group-specific prevalence and mortality rates for TBL, 1990–2021. (A) 15–19 years. (B) 80 + years. (C) 75–79 years. (D) 80 + years.
Correlation analysis between SDI and ASR
The correlation analysis between the SDI and ASRs revealed a significant positive association for TBL from 1990 to 2021. Specifically, the correlation coefficients were as follows: ASPR (R = 0.87, P < 0.01), ASIR (R = 0.83, P < 0.01), ASMR (R = 0.80, P < 0.01), and AS-DALYs (R = 0.77, P < 0.01) (Fig. 8A-D). Notably, regions such as High-income North America, East Asia, and Central Europe exhibited values significantly exceeding the global average. A detailed correlation analysis of TBL burden and SDI across 204 countries is provided in Supplementary Figure. S5.

Trends and correlation of ASRs with SDI from 1990–2021. (A) Trends and correlation of ASPR with SDI across 22 regions. (B) Trends and correlation of ASIR with SDI across 22 regions. (C) Trends and correlation of ASMR with SDI across 22 regions. (D) Trends and correlation of AS-DALYs with SDI across 22 regions.
TBL Disease Burden projections
We employed two forecasting models, ARIMA and BAPC, to predict trends in TBL from 2022 to 2035 and to cross-validate the accuracy of these models. The results of both analyses indicated that the overall ASPR of TBL is projected to exhibit a gradual decline between 2022 and 2035 (Fig. 9A, E; Supplementary Table 4S1-S2); the results of the projections for the ASIR of TBL during the same period revealed a significant and continuous decrease in the total ASIR (Fig. 9B, F; Supplementary Table 4S3-S4). Similarly, the total ASMR for TBL is expected to show a consistent decline from 2022 to 2035 (Fig. 9C, G; Supplementary Table 4S5-S6). Furthermore, the predictions for AS-DALYs indicated a significant and continuous reduction in total AS-DALYs throughout the 2022–2035 period (Fig. 9D, H; Supplementary Table 4S7-S8). Our findings suggest that the future trends of TBL disease follow a similar trajectory in both prediction models, which supports the validity of the forecasting models used and demonstrates the reliability of the predictions regarding TBL’s future disease trends.

Projected global burden of TBL from 2022 to 2050. (A–D) Age-standardized prevalence, incidence, mortality and DALYs rates of ARIMA model. (E–H) Age-standardized prevalence, incidence, mortality and DALYs rates of BAPC model.
Predictions of the burden of disease in different age groups
To better understand the future disease burden of TBL across different age groups, we analyzed the ASPR and ASMR in each age group using the BAPC model. The results indicated that the ASPR of TBL varied significantly among the different age groups from 2022 to 2035. Specifically, the ASPR exhibited a decreasing trend until the age of 75, with the most pronounced decline observed in the 70–74 age group. Conversely, the age group over 75 years demonstrated an increasing trend; however, the 75–79 age group showed a decrease after 2027, while the remaining age groups consistently exhibited an upward trend (Fig. 10 and Supplementary Table 4S9). Furthermore, the analysis of future trends in ASMR across various age groups revealed a decreasing trend in nearly all age groups, with the exception of the 95 + age group, which experienced a brief upward trend between 2022 and 2025 (Fig. 11 and Supplementary Table 4S10).

Predictions of future trends of TBL ASPR in different age groups, 2022–2035.

Predictions of future trends of TBL ASMR in different age groups, 2022–2035.
Discussion
It is well known that cancer poses one of the most significant threats to public health worldwide. According to statistics, lung cancer accounts for 13% of all cancer cases and is responsible for 23% of cancer-related deaths. TBL represent a major category of cancer with considerable morbidity and mortality19. The high rates of morbidity and mortality associated with TBL cancer have emerged as a critical global public health challenge. The present study spans three decades and encompasses the entire globe, including all continents, 204 countries, and 16 age groups. It systematically details the burden of TBL disease across various regions, countries, and age groups from 1990 to 2021. More importantly, for the first time, we have innovatively assessed the timing of the TBL disease burden and projected future trends up to 2035. More importantly, for the first time, we innovatively applied two distinct predictive models to enhance the robustness of the prediction results. Additionally, we utilized SDI correlation analysis and EAPC analysis to elucidate the differences and trends in the disease burden of TBL across all GBD regions and 204 countries. Beyond this, we evaluated the temporal trends in TBL disease burden and identified pivotal years of change, providing critical insights for understanding the current global epidemiology of TBL and laying a solid foundation for precision prevention efforts.
Our study found an overall stabilization of ASIR over the period from 1990 to 2021, while ASMR and annual AS-DALYs exhibited a consistent decreasing trend. Notably, the trends in ASIR and ASMR were divergent for males and females, with males demonstrating a decreasing trend and females showing an increasing trend in TBL. This finding aligns with previous research and suggests that the conclusions of our study are robust8. Although men represent the primary demographic affected by TBL, the rising trend of TBL burden among women cannot be overlooked20. It is reasonable to assert that men, as the predominant group exposed to tobacco globally, bear the most significant TBL burden. However, in East Asia, where fewer women smoke, the prevalence rate of TBL continues to rise, potentially linked to factors such as air pollution, cooking practices, and other environmental influences21.
Our study also identified an overall declining trend in AS-DALYs globally from 1990 to 2021. Notably, certain regions experienced the most significant declines, potentially linked to local prevention and treatment measures or a reduction in cancer-causing factors. Conversely, some regions exhibited less pronounced declines, which may be attributed to issues such as the unequal distribution of public health resources. The study revealed that Western Europe, high-income regions of North America, East Asia, Oceania, and high-income Asia-Pacific regions had the highest ASPR for TBL globally. East Asia, North America, and Western Europe, which have a long history of smoking and substantial population bases, may contribute to the elevated TBL burden in these areas. Furthermore, global regions and the five SDI regions displayed significant differences in TBL burden, which can be explained by disparities in healthcare resources resulting from uneven economic development. Although high SDI regions account for the majority of the global TBL burden, their AS-DALYs demonstrated the greatest decline, likely due to advanced prevention and healthcare systems22,23.
Our Burden of Disease study, which examined all global regions and the 5 SDI regions found that Western Europe, high-income North America, East Asia, Oceania, and high-income Asia-Pacific had the highest ASPR for TBL among all global regions. The study revealed that the high-income regions of East Asia, Western Europe, and North America are where smoking first emerged and have substantial population bases. The significant burden of TBL in these regions may be influenced by the historical prevalence of smoking, as well as the widespread use of tobacco and the size of the population24. Additionally, we observed varying ASPR, ASMR, and other metrics for TBL across the five different SDI regions. This variation is logical, given the disparities in healthcare resources resulting from uneven regional development25,26. Although high SDI regions bear the majority of the disease burden associated with TBL, they also experience the most significant decline in AS-DALYs. This decline may be attributed to the advanced prevention and healthcare systems present in high SDI regions27,28.
Analyses of the burden of disease for TBL across countries globally indicate that the highest ASPRs are concentrated in developed nations, with Monaco and France being the most prominent examples. This trend may be attributed to advanced case-counting systems in these countries, as well as higher levels of tobacco dependence. In 2021, Greenland and Monaco had much higher ASIRs and ASMRs than the Western European region, whereas Malawi’s ASRs were at the lowest level. The high ASIR in Greenland TBL may be related to its extreme natural environment29,30. The highest AS-DALYs in Greenland due to high ASPR as well as ASIR is understandable, while the lowest AS-DALYs were in Nigeria, but its 95% uncertainty interval suggests that we should be cautious about the AS-DALYs in Nigeria. and in our study, gender differences varied in TBL ASRs across regions and between years. In our study, we observed that gender differences in tobacco-related adverse health outcomes (ASRs) varied across regions and years. Previous research has demonstrated that female smokers face a significantly higher risk of lung cancer compared to their male counterparts31,32.
During the period from 1990 to 2021, the ASMR, ASIR, and AS-DALYs all exhibited a decreasing trend, despite the rise in the global ASPR. This suggests an improvement in the prevention and treatment of TBL worldwide. Among the five SDI regions, high SDI regions demonstrated the most significant declines in ASMR and AS-DALYs, likely due to their advanced healthcare systems. In contrast, the opposite trend observed in low and middle SDI regions may be attributed to disparities in governmental investment in health across different countries33. For example, in the high-income region of North America, ASMR, ASPR, ASIR, and AS-DALYs all declined significantly between 1990 and 2021, which may be attributed to its high accessibility to healthcare resources and high level of health care34. The most significant rise in ASPR was observed in East Asia, reaching 0.71 cases/100,000 people (95% UI: 0.30 to 1.21), which may be related to the large population base in the region as well as the continuous increase in tobacco consumption35.
In 2021, the ASPR of TBL was lowest among the 20–29 age groups, with incidence rates nearly identical for the 20–24 and 25–29 groups. Younger populations exhibit a lower probability of developing cancer, and the underlying causative factors remain unclear, potentially linked to genetic mutations36,37. Conversely, the ASPR, ASIR, ASMR and AS-DALYs were significantly higher in the 55–79 years age group. Research indicates that more than half of lung cancer cases occur in the elderly population38. Furthermore, the ASPR, ASIR, ASMR, and AS-DALYs for TBL across all age groups demonstrated significant gender disparities from 1990 to 2021, with males consistently exhibiting higher rates than females, despite an increasing burden of TBL among women. This trend is largely attributed to the higher prevalence of tobacco consumption among men. Therefore, regular screening for TBL is essential for the male population that overconsumes tobacco.
The SDI correlation analysis indicated that the global burden of TBL increases with higher SDI levels. This trend is primarily attributed to improved economic conditions, which enable increased healthcare expenditures, leading to significantly enhanced detection rates and diagnostic accuracy for TBL. Regions such as High-income North America, East Asia, and Central Europe were identified as areas with the highest TBL burden globally. However, over time, and with rising SDI levels, TBL mortality rates have shown a declining trend. This reduction is largely attributed to advancements in treatment modalities and improvements in lifestyle factors. These findings underscore the critical role of socioeconomic development in influencing both the detection and management of TBL39,40.
There is an overall declining trend in the burden of TBL from 2022 to 2035. In the case of a gradual increase in ASPR, we observed that the ASMR and ASIR of TBL, conversely, appear to be decreasing. We speculate that this may be related to increased investment in cancer research and public healthcare, as well as the implementation of various cancer-related legislation41,42,43. Currently, many countries are placing greater emphasis on changes in DALYs as a key indicator of disease burden44. According to our findings, there is expected to be a continuous decline in AS-DALYs for TBL in the future, which presents a promising outlook for the current critical global public health situation. This trend reflects significant progress in the global prevention and control of TBL, as well as advancements in treatment research has made great progress. However, it is worth noting that the disease burden of TBL in the female population is slowly increasing in the future, with the most significant rise in ASPR. Some studies have shown that women with a history of tobacco dependence have worse lung health than men45. Therefore, we advocate that early screening for TBL targeting with women should be implemented in a timely manner, especially in the group of women with a history of tobacco dependence. And according to the prediction results of each age group, the elderly population remains the main group with high Prevalence and Mortality of TBL. Unlike young people, the gradual weakening of various physiological functions in the elderly is a major reduction in the body’s ability to resist cancer cells, which is the main reason for high Prevalence and Mortality. Therefore, we suggest that intensive screening and special cancer care for the elderly is necessary.
Although this study provides a comprehensive and systematic analysis of the ASPR, ASIR, ASMR, and AS-DALYs of TBL globally, regionally, and across 204 countries. from 1990 to 2021, it shares certain limitations inherent to most GBD studies.
First, variations in economic and healthcare levels among countries may lead to biases in the accuracy and reliability of GBD data. Detailed mapping and analysis are essential to better represent the disease burden in individual countries46,47. Second, the long study period might overlook significant variations in disease burden within specific countries during particular years, limiting the ability to capture short-term changes. Third, the GBD database lacks detailed pathological classifications of lung cancer, such as non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). As a result, the specific contributions of different lung cancer types to the overall TBL burden could not be analyzed. Finally, the impact of COVID-19 on lung cancer burden cannot be ignored. However, in GBD 2021, COVID-19 is categorized as a separate disease and not considered a risk factor for TBL. Consequently, the potential influence of COVID-19 on TBL burden has been omitted. Further research is urgently needed to determine the precise impact of COVID-19 on TBL.
Conclusion
This study, based on GBD 2021 data, analyzed the burden of TBL globally, regionally, and across 204 countries from 1990 to 2021. The results indicated that the burden of TBL was predominantly concentrated in high-SDI regions and areas with large population bases, with High-income North America and East Asia being the most affected. Among countries, Egypt showed the most significant increase in the EAPC, while Kazakhstan exhibited the most notable decline. From 1990 to 2021, the overall global burden of TBL decreased slightly; however, the burden among females has consistently risen, a trend projected to persist until 2035. These findings provide critical epidemiological evidence of gender disparities in TBL burden. The study underscores the importance of early screening, accurate diagnosis, and timely treatment in the prevention and control of TBL. It also calls on nations to formulate and implement targeted policies to address this significant global public health challenge.
Data availability
The data from this study can be accessed openly through the GBD 2021 online database (https://www.healthdata.org/research-analysis/gbd).
References
Xia, C. et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin. Med. J. 135, 584–590 (2022).
Hirsch, F. R. et al. Lung cancer: current therapies and new targeted treatments. Lancet (Lond. Engl.) 389, 299–311 (2017).
McKay, J. D. et al. Large-scale association analysis identifies new lung cancer susceptibility loci and heterogeneity in genetic susceptibility across histological subtypes. Nat. Genet. 49, 1126–1132 (2017).
Lorenzo-González, M. et al. Lung cancer risk and do-it-yourself activities. A neglected risk factor for lung cancer. Environ. Res. 179, 108812 (2019).
Jemal, A. et al. Higher lung cancer incidence in young women than young men in the United States. N. Engl. J. Med. 378, 1999–2009 (2018).
Barnett, R. Lung cancer. Lancet (Lond. Engl.) 390, 928 (2017).
Haiman, C. A. et al. Ethnic and racial differences in the smoking-related risk of lung cancer. N. Engl. J. Med. 354, 333–342 (2006).
Deng, Y. et al. Epidemiological trends of tracheal, bronchus, and lung cancer at the global, regional, and national levels: a population-based study. J. Hematol. Oncol. 13, 98 (2020).
Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet (Lond. Engl.) 396, 1204–1222. (2020).
Tuo, Y. et al. Global, regional, and national burden of Thalassemia, 1990–2021: a systematic analysis for the global burden of disease study 2021. EClinicalMedicine 72, 102619 (2024).
Global incidence. Prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet (Lond. Engl.) 403, 2133–2161 (2024).
Hankey, B. F. et al. Partitioning linear trends in age-adjusted rates. Cancer Causes Control: CCC 11, 31–35 (2000).
Kim, H. J., Fay, M. P., Feuer, E. J. & Midthune, D. N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 19, 335–351 (2000).
Global National disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet (Lond. Engl.) 388, 1603–1658 (2016).
Ghazy, R. M., Al Awaidy, S. & Taha, S. H. N. Trends of HIV indicators in Egypt from 1990 to 2021: time-series analysis and forecast toward UNAIDS 90-90-90 targets. BMC Public. Health 23, 625 (2023).
Schaffer, A. L., Dobbins, T. A. & Pearson, S. A. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: a guide for evaluating large-scale health interventions. BMC Med. Res. Methodol. 21, 58 (2021).
Riebler, A. & Held, L. Projecting the future burden of cancer: bayesian age-period-cohort analysis with integrated nested laplace approximations. Biom. J. 59, 531–549 (2017).
Jürgens, V., Ess, S., Cerny, T. & Vounatsou, P. A bayesian generalized age-period-cohort power model for cancer projections. Stat. Med. 33, 4627–4636 (2014).
Siegel, R., Ward, E., Brawley, O. & Jemal, A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. Cancer J. Clin. 61, 212–236 (2011).
Torre, L. A., Siegel, R. L. & Jemal, A. Lung cancer statistics. Adv. Exp. Med. Biol. 893, 1–19 (2016).
Household use of solid fuels and high-temperature frying. IARC Monogr. Eval. Carcinog. Risks Hum. 95, 1–430 (2010).
Tsao, A. S. et al. Scientific advances in lung cancer 2015. J. Thorac. Oncol. Official Public. Int. Assoc. Study Lung Cancer 11, 613–638 (2016).
Wu, L., Leng, D., Cun, D., Foged, C. & Yang, M. Advances in combination therapy of lung cancer: Rationales, delivery technologies and dosage regimens. J. Control. Rel. Off. J. Control. Release Soc. 260, 78–91 (2017).
Thun, M., Peto, R., Boreham, J. & Lopez, A. D. Stages of the cigarette epidemic on entering its second century. Tob. Control 21, 96–101 (2012).
Dickman, S. L., Himmelstein, D. U. & Woolhandler, S. Inequality and the health-care system in the USA. Lancet (Lond. Engl.) 389, 1431–1441 (2017).
Baum, N., Kum, Y., Shalit, H. & Tal, M. Inequalities in a national health care system from the perspective of social workers in Israel. Qual. Health Res. 27, 855–865 (2017).
Barry, D. T., Glenn, C. P., Hoff, R. A. & Potenza, M. N. Group differences in pain interference, psychiatric disorders, and general medical conditions among hispanics and whites in the U.S. general population. Psychiatr. Res. 258, 337–343 (2017).
Spann, S. J. Interspeciality differences in medical resource utilization. J. Fam. Pract. 49, 18–19 (2000).
Gelvan, A., Risum, S. & Langer, S. W. Incidence and survival from lung cancer in Greenland is comparable to survival in the nordic countries. Dan. Med. J. 62, A5033 (2015).
Bjerregaard, P., Mulvad, G. & Olsen, J. Studying health in Greenland: obligations and challenges. Int. J. Circumpolar. Health 62, 5–16 (2003).
Papadopoulos, A. et al. Heavy smoking and lung cancer: are women at higher risk? Result of the ICARE study. Br. J. Cancer 110, 1385–1391 (2014).
Powell, H. A., Iyen-Omofoman, B., Hubbard, R. B., Baldwin, D. R. & Tata, L. J. The association between smoking quantity and lung cancer in men and women. Chest 143, 123–129 (2013).
Nwagbara, U. I., Ginindza, T. G. & Hlongwana, K. W. Lung cancer awareness and palliative care interventions implemented in low-and middle-income countries: a scoping review. BMC Public. Health 20, 1466 (2020).
Measuring performance on the healthcare access and quality index. For 195 countries and territories and selected subnational locations: a systematic analysis from the global burden of disease study 2016. Lancet (Lond. Engl.) 391, 2236–2271 (2018).
Sun, H. et al. Burden of lung cancer in China, 1990–2019: findings from the global burden of disease study 2019. Cancer Control J. Moffitt Cancer Cent. 30, 10732748231198749 (2023).
Liu, B. et al. Lung cancer in young adults aged 35 years or younger: a full-scale analysis and review. J. Cancer 10, 3553–3559 (2019).
Oliveira, I., Mota, P. & Almodovar, T. Lung cancer in young patients: natural history, biology and prognosis. Pulmonology 28, 80–81 (2022).
Frasca, M. et al. Serious health-related suffering impairs treatments and survival in older patients with cancer. J. Pain Sympt. Manag. (2024).
Sandström, N., Johansson, M., Jekunen, A. & Andersén, H. Socioeconomic status and lifestyle patterns in the most common cancer types-community-based research. BMC Public. Health 23, 1722 (2023).
Stewart, D. W. et al. Lower health literacy predicts smoking relapse among racially/ethnically diverse smokers with low socioeconomic status. BMC Public. Health 14, 716 (2014).
Agrawal, S. & Vagha, S. A. Comprehensive review of artificial intelligence in prostate cancer care: state-of-the-art diagnostic tools and future outlook. Cureus 16, e66225 (2024).
Siegel, R. L. et al. An assessment of progress in cancer control. Cancer J. Clin. 68, 329–339 (2018).
Lawler, M. et al. The European cancer patient’s bill of rights, update and implementation 2016. ESMO Open 1, e000127 (2016).
Shi, J. et al. Burden of cancer in China: data on disability-adjusted life years. Chin. J. Prev. Med. 49, 365–369 (2015).
Menson, K. E. & Coleman, S. R. M. Reprint of: Smoking and pulmonary health in women: a narrative review and behavioral health perspective. Prev. Med. 108113 (2024).
Colah, R. et al. Epidemiology of beta-thalassaemia in Western India: mapping the frequencies and mutations in sub-regions of Maharashtra and Gujarat. Br. J. Haematol. 149, 739–747 (2010).
Weatherall, D. J. The challenge of haemoglobinopathies in resource-poor countries. Br. J. Haematol. 154, 736–744 (2011).
Acknowledgements
We would like to thank those who participated in the GBD data survey and the IHME organization for submitting the complete GBD data. We are grateful for the financial support from the General Project of the Joint Special Project of Local Universities in Yunnan Province (202001BA070001-064, 202101BA070001-102), Dali University Doctoral Research Start-up Fund Project (KYBS2018012), Open Project of Yunnan Provincial Key Laboratory of Entomological Biopharmaceutical R&D (AG2024002), Clinical Medicine Discipline Team Building Project of the First Affiliated Hospital of Dali University (DFYYB2024026), and Open Project of Key Laboratory of Screening and Research of Resistant Plant Resources in West Yunnan, Yunnan Province (APKL2101). The study funders did not participate in the design of the study, data collection, analysis, interpretation, or report writing.
Author information
Authors and Affiliations
Contributions
Yuzhe Zhang designed the study. Xin Zhang conceived the protocol and wrote the first draft. Jing Zou analysed the GBD data. Jinghua Ning and Yanhong Zhao contributed to the statistical analysis and interpretation of data. Run Qu, Congcong Lv and Yi Liang participated in the first draft revision. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The ethics committee approved the ethical exemption for this study because it utilizes publicly available data that does not contain any confidential information or patient privacy concerns.
Consent for publication
All participants in this study consented to publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, X., Zou, J., Ning, J. et al. Disease burden of trachea, bronchus and lung cancer 1990–2021 and global trends projected to 2035. Sci Rep 15, 6264 (2025). https://doi.org/10.1038/s41598-025-90537-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-90537-8
Keywords
This article is cited by
-
Global, regional, national burden, trends and health inequality of neglected tropical diseases and malaria from 1990 to 2021
BMC Infectious Diseases (2025)
