
Abstract
Hemophagocytic lymphohistiocytosis (HLH) is an excessive immune activation with cytokine storm und multi-organ dysfunction. It can occur secondarily, especially due to viral infections like COVID-19. Rapid treatment is crucial for favourable outcomes, but diagnosing HLH is challenging. The most common diagnostic instrument is the H-Score. However, the prognostic value of the H-score has not yet been assessed in detail in the spotlight of secondary HLH in severe COVID-19. COVID-19 patients treated between February 2020 and April 2021 at the intensive care unit (ICU) of the Department of Infectious Diseases and Tropical Medicine, Clinic Favoriten, Vienna, Austria, were included in this study. Data were assessed retrospectively by document review, and the follow-up period was at least 90 days. A total of 208 critically ill COVID-19 patients with an age of 61.8 ± 13.6 years were enrolled in this study. We found an average H-Score in the entire study collective of 94 ± 51 points, and 8.7% had a score ≥ 169 testing positive for HLH. A positive score was associated with increased mortality rates at 28 (66.7 vs. 26.3%, p < 0.001) and 90 days (72.2 vs. 27.9%, p < 0.001). In our cohort study, critically ill COVID-19 patients with an H-Score ≥ 169 during their ICU stay had increased mortality rates at 28 and 90 days. Thus, attention should be paid to individuals with rising or high scores. Therapeutic options and their impact on mortality for patients with COVID-19-associated secondary HLH should be evaluated in further studies.
Similar content being viewed by others

Introduction
Hemophagocytic lymphohistiocytosis (HLH; also known as hemophagocytic syndrome) is a life-threatening excessive immune activation with cytokine storm and multi-organ dysfunction. HLH can occur as a sporadic disorder or due to a genetic predisposition. Infection is a common trigger in both entities, especially when induced by human herpes virus (HHV), influenza virus, human immunodeficiency virus (HIV), Epstein-Barr virus (EBV), cytomegalovirus (CMV), or parvovirus or varicella-zoster virus (VZV) (1–7), but also COVID-19, caused by SARS-CoV-2, can be associated with HLH (8). So far, in a collective of 669 patients with severe COVID-19, Alam et al. have reported a rate of 2% with an H-Score ≥ 169 (9, 10), and Tang et al. have described a HLH prevalence of 7% in severe COVID-19 patients in a systematic review (8).
Rapid initiation of HLH treatment is crucial for a favourable outcome, but diagnosis of HLH is challenging due to the wide range of possible laboratory findings, the clinical gestalt, and the rarity of the syndrome. While the so-called HLH-94 protocol (11) or its updated version (HLH-2004) (12) have been widely used in the past, the H-Score (13, 14), which was first described in 2014, is nowadays commonly utilized for estimating an individual’s risk of having HLH. The score gives points for a known underlying immunosuppression, temperature/fever, organomegaly, number of cytopenias, levels of ferritin, triglycerides, fibrinogen and alanine aminotransferase (AST), as well as hemophagocytosis features on bone marrow aspirate. (13) As the score increases, so does the probability of HLH: ≤ 90 points confers a < 1% probability of HLH, whereas a score of ≥ 241 (up to a maximum of 337) corresponds to a > 99% probability. (13) There is no uniform cut-off in the literature, but a value around 169 (93% sensitivity, 86% specificity, accurate classification in 90% of patients (15)) is usually seen as diagnostic for HLH (9).
It is known that higher H-Scores seem to be associated with a higher risk of ICU admission, an extended hospitalization, and higher mortality rates in COVID-19 patients. (16) However, the prognostic value of the H-score has not yet been assessed in detail in the spotlight of secondary HLH in severe COVID-19.
Methods
Study population and design
In this retrospective cohort study, COVID-19 patients treated at the intensive care unit (ICU) of the Department of Infectious Diseases and Tropical Medicine, Clinic Favoriten, Vienna Healthcare Group, Vienna, Austria, were eligible for inclusion. Patients were consecutively enrolled between February 2020 and April 2021. Exclusion criteria were transfer to another intensive or intermediate care unit (due to lack of adequate follow-up), age < 18 years, and missing relevant data.
Ethics statement
Ethical approval for this study (EK 20–079-VK) was provided by the Ethical Committee of the City of Vienna. The study protocol complies with the Declaration of Helsinki, and data reporting was performed according to STROBE guidelines.
Collection of demographic and medical data
Data including patient characteristics, medical history, clinical information, laboratory parameters, and further ICU data were assessed retrospectively by document review and were then inserted into a predefined record abstraction form.
Statistical analysis
Categorial data are presented as absolute and relative frequencies and were compared among subgroups using χ2-test. Continuous variables are described using means ± standard deviations (SD) or medians and the respective interquartile ranges (IQR), and were compared via Mann-Whitney-U test. We used a cut-off of ≥ 169 for the diagnosis of HLH by using the H-Score (‘positive’ H-Score). (9, 13, 17) We assumed statistical significance through two-sided p-values of < 0.05, and performed calculations with the statistical software R (RStudio Version 1.2.5033, RStudio Inc., Boston, MA, U.S.A.).
Results
Between February 2020 and April 2021, we enrolled 254 COVID-19 patients (defined as new onset of symptoms and positive for SARS-CoV-2 by RT-PCR test (CT value < 30) from tracheal secretion, nasal or nasopharyngeal swab). After excluding 46 subjects, the data of 208 (81.9%) patients could be analyzed. Figure 1 gives an overview of the study participants and the classification in terms of H-Score.

Flow chart of study participants and classification in terms of H-Score. ICU = intensive care unit; IMCU = intermediate care unit.
Basic characteristics
The average age was 61.8 ± 13.6 years, around a quarter were women (28.4%), and more than half were obese (29.9 ± 6.3 kg/m2). There were no significant differences in the aforementioned parameters between the two groups H-Score ≥ 169 and H-Score < 169. The groups also hardy differed regarding known chronic diseases (only chronic kidney disease (CKD) was more frequent in the group with a H-Score ≥ 169). Table 1 gives a more detailed overview of the basic study population characteristics, known chronic diseases, and laboratory findings. During the inclusion period, the entire study cohort was unvaccinated.
Established ICU scores
Data regarding the patients’ APACHE II, SAPS II, and SAPS III scores at ICU admission can be found in Table 1. Only APACHE II showed significant differences between the two H-Score groups. In patients with a “negative” H-Score, the mortality rates fit to the mortality rates regarding the ICU scores. However, in patients with a H-Score of ≥ 169, the mortality rates were much higher. 28-day mortality: For H-Score < 169: 26.3% vs. APACHE II 16 (25%), SAPS II 34 (15.3%), and SAPS III 54 (23.9%); whereas for H-Score ≥ 169: 66.7% vs. APACHE II 19 (25%), SAPS II 38 (21.3%), and SAPS III 59 (33.5%).
(Predicted) mortality
With special regard to the then initial stage of pandemic and the lack of overall knowledge, especially regarding infectiousness and the according fears, autopsies were rarely carried out at this time. Based on the clinical presentation, however, we assume that sepsis and subsequently multiple organ failures were the main cause of death.
H-Score
The average H-score for the entire study population was 94 ± 51 points, despite the fact that no one received a bone marrow aspiration (up to 35 points) and several patients had no imaging documented (up to 38 points can be given for hepatosplenomegaly). The proportion of patients with an H-Score ≥ 169 was 8.7% (18 individuals) or 4.8% (10 individuals; all laboratory parameters included in the score from the same day), respectively. Table 2; Fig. 2 give an overview of the exact distribution.

Overview of the points achieved in the H-Score.
H-Score in detail
Almost all patients (93.3%) received points for an elevated aspartate aminotransferase (AST), 70.7% for high triglyceride levels, 55.3% had a temperature of > 38.4 °C, more than a quarter (27.9%) had ferritin levels ≥ 2,000 ng/mL, and 21.2% had at least two lines of cytopenia (Fig. 3; Table 3). Less than 5% were scored for immunosuppression and fibrinogen levels. No statement can be made about organomegaly or pathological bone marrow aspiration due to missing data.

Points awarded according to the H-Score in detail; light or dark blue depending on the number of points given. WBC = white blood cell; AST = aspartate aminotransferase.
H-Score and ICU data
On average, patients required intensive care from day eight after symptom onset. Two thirds needed support in the form of non-invasive ventilation, 45.7% even required invasive mechanical ventilation, with an average ventilation duration of 15 ± 8 days. About 5% needed continuous renal replacement therapy, and 4% ECMO treatment. Furthermore, superinfection was very common, with 100% of the patients who also had an H-Score of > 169.
H-Score and mortality
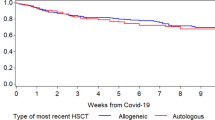
ICU survival was significantly lower in the higher H-score group (38.9% vs. 75.8%). The same trend was observed for 28-day (66.7 vs. 26.3%, p < 0.001, Figs. 4) and 90-day mortality (72.2 vs. 27.9%, p < 0.001). In particular, increased temperature and ferritin levels were associated with mortality, but there were also significant differences in cytopenia and triglyceride levels (Table 4).

H-Score and 28-day-mortality.
Patients with a ‘positive’ H-Score
Eighteen patients of the study cohort (8.7%) had a H-Score of ≥ 169 points and are shown in detail in Table 5. All of them got points due to increased temperature, for at least two lineages of cytopenia, and high ferritin, triglyceride, and AST levels. Patients who did not survive died at 22 [14–31] days after symptom onset.
Discussion
Our study assessed the rate of secondary HLH (sHLH) in critically ill COVID-19 patients as well as their mortality, and found an average H-Score of 94 ± 51 points; 8.7% had a score of ≥ 169, thus testing positive for sHLH. A positive score was associated with increased mortality rates.
Viral infections, sHLH, and mortality
Secondary HLH can occur associated with a variety of triggers, but the most important is viral infection. In 74%, sHLH is triggered by Epstein-Barr virus (EBV), which also has the poorest prognosis, followed by infections with Cytomegalovirus (CMV) and human herpes virus 8 (HHV-8) as main triggers. Regarding mortality, data are very heterogeneous: Ishii et al. reported a 5-year overall survival rate of over 80% for patients with EBV- or other infection-associated HLH in Japan (19); a recently published study reported an overall HLH mortality rate of 40% (20); and even higher mortality rates of around 57% (regardless of HLH aetiology or specific treatment) were reported in a large ICU cohort of patients diagnosed with HLH in France (10). Within this wide range lie the results of our study with a 28-day mortality of two-thirds of all patients with COVID-19 and a positive score.
(S)HLH and (severe) COVID-19
In contrast to other published studies, our patient population shows an average H-Score in the entire study collective of 94 ± 51 points, with 8.7% scoring ≥ 169 and thus testing positive for sHLH. In addition, we report significantly higher mortality rates (two-thirds of all patients). In hospitalized paediatric and adult patients with a proven diagnosis of COVID-19 (n = 193), Bordbar et at. described a median H-Score of 43.0 (IQR 0–63), and, in general, a higher score in those who need intensive care and died of COVID-19. (16) Data from 19 patients with COVID-19 requiring an ICU stay showed 2% with a H-Score ≥ 169, and 16% of all subjects in this study died. (9) The significantly higher mortality rates also suggest that the population analysed in our study was likely to have been much more severely affected by the underlying disease. High rates of invasive mechanical ventilation and bacterial superinfection also support this. Of note, when assessing established ICU scores such as APACHE II, SAPS II, and SAPS III, the respective mortality rates fit patients without HLH but not those with HLH (in whom mortality was much higher than predicted by the scores). Accordingly, the H-score could potentially be a better predictor of ICU mortality in severe COVID-19 than the mentioned ICU scores. This must be further investigated.
sHLH versus severe COVID-19
COVID-19 and sHLH (with cytokine release syndrome (CRS) or hyperinflammatory syndrome (HIS)) have parallels but are two different entities; sHLH may or may not be present in COVID-19. Moreover, the H-Score without directing it at evaluating HLH is likely not appropriate for detecting hyperinflammatory states in “pure” COVID-19 and also not suitable to make statements regarding outcome. (21–26) Temperature peaks of > 39 °C, leukopenia, very high levels of ferritin, hypertriglyceridaemia, and low levels of fibrinogen (all paramters from the H-Score) are, however, no typical clinical features of COVID-19: Common laboratory findings among hospitalized COVID-19 patients include lymphopenia (27) with a varying total WBC (28) and elevated inflammatory markers (e.g., ferritin). In a large study with 5700 hospitalized COVID-19 patients, only 31% had a temperature of > 38 °C at presentation, the ferritin was 798 (411–1515; reference range 15–400) ng/mL, and the WBC 7.0 (5.2–9.5) G/L (29). Other authors published ferritin levels of 139 (66–403) ng/mL, fibrinogen of 386 (129) mg/dL (= 3.86 g/L) (30), and median triglyceride concentrations between 0.96 and 1.94 mmol/L (= 85.0 or 171.7 mg/dL, respectively). (31–33)
Bone marrow aspiration and potential hemophagocytosis features
As in previous literature (16), no bone marrow punctures were performed in our study collective (see Limitations). However, the limited available data predict a very high rate of hemophagocytosis in patients with both HLH and severe COVID-19: Bichon et al. reported a bone marrow hemophagocytosis for 91% of patients in a general ICU-HLH collective (10), and haemophagocytes with erythrophagocytosis were detected in 67% of a collective of deceased individuals with severe COVID-19 (18). If we assume the same 2/3 rate in our subjects, we would have a rate of patients with an H-score ≥ 169 of 16.8% (N = 35). An adjustment of the score could be considered in the future, considering among other things that a puncture is time-consuming, can be associated with complications and is not very specific.
Clinical implications and future outlook
The findings support regular collection of the H-Score, especially for COVID-19 ICU patients. An automatic warning of an ICU IT solution when a certain limit value is exceeded could be considered to be mindful of potential worse outcomes and a potential trigger for specific therapeutic options. Automatic HLH screening could be conducted daily by artificial intelligence, for instance.
Of note, our findings should be validated in another COVID-19 cohort which is vaccinated against SARS-CoV-2-.
Limitations
The main limitation of this study was the lack of bone marrow aspiration and imaging data, as no one had a puncture, and some imaging was not documented. Therefore, up to 73 points (21.7% of a maximum of total score of 337) are missing in the score results. The lack of bone marrow analyses and knowledge about organomegaly was due to the beginning of the pandemic, where little was known about COVID-19, let alone respective sHLH, and these diagnostics were simply not performed routinely.
Furthermore, 37 patients had to be excluded because of transfers to other ICUs or IMCUs. These patients had a maximum H-Score of 126 at the time of transfer, which is significantly higher than the average of the collective examined in this study (94 ± 51 points). Also, the percentage with a positive score was higher (13.5 vs. 8.7%). A possible reason could be the lack of availability of veno-venous extracorporeal membrane oxygenation in the ICU of the study site, which is often the last therapeutic option in the most severe COVID-19 cases. In general, the single-centre nature of a study is always fraught with disadvantages.
Moreover, the timepoint of patients presenting to the emergency medical services, the emergency department, and the ICU naturally varied, depending on incubation time, clinical courses, and also the patients’ subjective feelings. Therefore, the H-score was determined at different stages of the disease.
With regard to mortality, there could also be confounding factors that were not taken into account and could therefore play a role. In particular, we did not have detailed information about the treatment, how much the patients had previously been affected in their lives, or the causes of mortality.
Conclusion
In our cohort study, critically ill COVID-19 patients with a H-Score ≥ 169 and thus testing positive for sHLH during their ICU stay had increased mortality rates at 28 and 90 days. Thus, specific attention should be paid to individuals with high H-Scores in ICUs. Therapeutic options and their impact on mortality for patients with COVID-19-associated sHLH should be evaluated in further studies.
Data availability
The data underlying this article will be shared on reasonable request to the corresponding author.
References
1. Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet. 2014;383(9927):1503-16.
2. Mou SS, Nakagawa TA, Riemer EC, McLean TW, Hines MH, Shetty AK. Hemophagocytic lymphohistiocytosis complicating influenza A infection. Pediatrics. 2006;118(1):e216-9.
3. Harms PW, Schmidt LA, Smith LB, Newton DW, Pletneva MA, Walters LL, et al. Autopsy findings in eight patients with fatal H1N1 influenza. Am J Clin Pathol. 2010;134(1):27–35.
4. Chen TL, Wong WW, Chiou TJ. Hemophagocytic syndrome: an unusual manifestation of acute human immunodeficiency virus infection. Int J Hematol. 2003;78(5):450-2.
5. Fardet L, Blum L, Kerob D, Agbalika F, Galicier L, Dupuy A, et al. Human herpesvirus 8-associated hemophagocytic lymphohistiocytosis in human immunodeficiency virus-infected patients. Clin Infect Dis. 2003;37(2):285 − 91.
6. Grossman WJ, Radhi M, Schauer D, Gerday E, Grose C, Goldman FD. Development of hemophagocytic lymphohistiocytosis in triplets infected with HHV-8. Blood. 2005;106(4):1203-6.
7. Mostaza-Fernández JL, Guerra Laso J, Carriedo Ule D, Ruiz de Morales JM. Hemophagocytic lymphohistiocytosis associated with viral infections: Diagnostic challenges and therapeutic dilemmas. Rev Clin Esp (Barc). 2014;214(6):320-7.
8. Tang KT, Hsu BC, Chen DY. Autoimmune and Rheumatic Manifestations Associated With COVID-19 in Adults: An Updated Systematic Review. Front Immunol. 2021;12:645013.
9. Alam F, Becetti K, Alamlih L, Cackamvalli P, Veettil S, Awadh B, et al. Rate of secondary HLH and performance of H-score in patients with severe COVID-19. Qatar Med J. 2022;2022(2):11.
10. Bichon A, Bourenne J, Allardet-Servent J, Papazian L, Hraiech S, Guervilly C, et al. High Mortality of HLH in ICU Regardless Etiology or Treatment. Front Med (Lausanne). 2021;8:735796.
11. Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18(1):29–33.
12. Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124 − 31.
13. Fardet L, Galicier L, Lambotte O, Marzac C, Aumont C, Chahwan D, et al. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014;66(9):2613-20.
14. Debaugnies F, Mahadeb B, Ferster A, Meuleman N, Rozen L, Demulder A, et al. Performances of the H-Score for Diagnosis of Hemophagocytic Lymphohistiocytosis in Adult and Pediatric Patients. Am J Clin Pathol. 2016;145(6):862 − 70.
15. HScore for Reactive Hemophagocytic Syndrome [Available from: https://www.mdcalc.com/calc/10089/hscore-reactive-hemophagocytic-syndrome.
16. Bordbar M, Sanaei Dashti A, Amanati A, Shorafa E, Mansoori Y, Dehghani SJ, et al. Assessment of the HScore as a predictor of disease outcome in patients with COVID-19. BMC Pulmonary Medicine. 2021;21(1):338.
17. Meng M, Chen L, Zhang S, Dong X, Li W, Li R, et al. Risk factors for secondary hemophagocytic lymphohistiocytosis in severe coronavirus disease 2019 adult patients. BMC Infect Dis. 2021;21(1):398.
18. Swoboda J, Wittschieber D, Sanft J, Kleemann S, Elschner S, Ihle H, et al. Bone marrow haemophagocytosis indicates severe infection with severe acute respiratory syndrome coronavirus 2. Histopathology. 2021;78(5):727 − 37.
19. Ishii E, Ohga S, Imashuku S, Yasukawa M, Tsuda H, Miura I, et al. Nationwide survey of hemophagocytic lymphohistiocytosis in Japan. Int J Hematol. 2007;86(1):58–65.
20. La Marle S, Richard-Colmant G, Fauvernier M, Ghesquières H, Hot A, Sève P, et al. Mortality and Associated Causes in Hemophagocytic Lymphohistiocytosis: A Multiple-Cause-of-Death Analysis in France. J Clin Med. 2023;12(4).
21. Leverenz DL, Tarrant TK. Is the HScore useful in COVID-19? Lancet. 2020;395(10236):e83.
22. Lorenz G, Moog P, Bachmann Q, La Rosée P, Schneider H, Schlegl M, et al. Title: Cytokine release syndrome is not usually caused by secondary hemophagocytic lymphohistiocytosis in a cohort of 19 critically ill COVID-19 patients. Sci Rep. 2020;10(1):18277.
23. Wood H, Jones JR, Hui K, Mare T, Pirani T, Galloway J, et al. Secondary HLH is uncommon in severe COVID-19. Br J Haematol. 2020;190(5):e283-e5.
24. Yadav G, Malhotra H, Mehta P, Sachu R, Rizvi I, Bharti VR, et al. Severe COVID-19-associated hyperinflammatory syndrome versus classic hemophagocytic lymphohistiocytosis: similarities, differences, and the way forward. J Investig Med. 2023;71(3):244 − 53.
25. Alfaro-Murillo A, Lazo-Paéz G. [Secondary hemophagocytic lymphohistiocytosis and cytokine release syndrome in COVID-19, the same or different entities?]. Rev Chilena Infectol. 2021;38(2):271-8.
26. Clark KEN, Nevin WD, Mahungu T, Lachmann H, Singh A. Assessment of the Hemophagocytic Lymphohistiocytosis HScore in Patients With Coronavirus Disease 2019. Clin Infect Dis. 2021;73(9):e3110-e2.
27. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. Jama. 2020;323(11):1061-9.
28. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507 − 13.
29. Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. Jama. 2020;323(20):2052-9.
30. Kornblith LZ, Sadhanandhan B, Arun S, Long R, Johnson AJ, Noll J, et al. γ’ fibrinogen levels as a biomarker of COVID-19 respiratory disease severity. Blood Cells Mol Dis. 2023;101:102746.
31. Wei X, Zeng W, Su J, Wan H, Yu X, Cao X, et al. Hypolipidemia is associated with the severity of COVID-19. J Clin Lipidol. 2020;14(3):297–304.
32. Cao WJ, Wang TT, Gao YF, Wang YQ, Bao T, Zou GZ. Serum Lipid Metabolic Derangement is Associated with Disease Progression During Chronic HBV Infection. Clin Lab. 2019;65(12).
33. Madsen CM, Varbo A, Tybjærg-Hansen A, Frikke-Schmidt R, Nordestgaard BG. U-shaped relationship of HDL and risk of infectious disease: two prospective population-based cohort studies. Eur Heart J. 2018;39(14):1181-90.
Acknowledgements
We would like to thank all those involved in the collection of the study data and all the clinical staff who cared for the patients described.
Funding
None.
Author information
Authors and Affiliations
Contributions
JO, TCS, AK, FE, RB, MN, AO, CV, and SS contributed to data acquisition and study design. JO, TCS, and SS crafted the manuscript and executed data analyses. TCS and SS supervised the study process. CW, AP, DT, RS, and HA contributed to study design and amended the manuscript. All authors critically revised and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval (N°20-079-VK) was provided by the Ethics Committee of the City of Vienna. Due to the retrospective nature of the study, the Ethics Committee of the City of Vienna waived the need of obtaining informed consent. The study complies with the Declaration of Helsinki and STROBE guidelines.
Consent for publication
Informed consent (and therefore also consent for publication) was waived by the Ethics Committee.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Oppenauer, J., Clodi-Seitz, T., Kornfehl, A. et al. Secondary Hemophagocytic Lymphohistiocytosis in severe COVID-19 - a retrospective cohort study. Sci Rep 15, 6137 (2025). https://doi.org/10.1038/s41598-025-90766-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-90766-x
Keywords
This article is cited by
-
Cytokine storm
Nature Reviews Disease Primers (2026)
