
Abstract
This study aimed to evaluate the long-term efficacy and clinical outcomes of catheter ablation performed with cryoballoon (CRYO) in comparison with robotic magnetic navigation (RMN) in patients with persistent atrial fibrillation (PersAF). A total of 200 patients with symptomatic PersAF were prospectively enrolled and non-randomly assigned (1:1) to the CRYO or RMN guided-ablation group undergoing pulmonary vein isolation (PVI) and additional linear ablation if necessary and then followed up over 5 years. The primary endpoint was freedom from atrial tachyarrhythmias (ATs) recurrence following a 3-month blanking period after the initial procedure. The secondary endpoints consisted of all-cause and cardiovascular rehospitalizations, rates of electrical cardioversion (EC) and re-do ablation, new-onset neurological event, major bleeding event and the difference in CHA2DS2-VASc score at 5-year compared with baseline. After a median follow-up period of 60 months, 184 patients (93 in RMN, 91 in CRYO) completed the follow-up. Freedom from recurrent ATs was achieved in 44 out of 93 patients in the RMN group and 37 out of 91 patients in the CRYO group (47.3% vs. 40.7%, P = 0.32). There were no significant differences in the risk of all-cause and cardiovascular rehospitalizations, rates of EC and re-do ablation, new-onset neurological event, and major bleeding event at 5 years. Anticoagulation (OAC) discontinuation was relatively common after ablation, since 48.4% of patients with a CHA2DS2-VASc score ≥ 2 were not on OAC therapy. CRYO is comparable to RMN-guided ablation with respect to long-term freedom from ATs in patients with PersAF. Discontinuation of OAC after ablation is not rare even in patients at risk of stroke for continued OAC therapy.
Similar content being viewed by others
Introduction
Atrial fibrillation (AF) is the most prevalent arrhythmia in clinical practice, and is associated with the increasing occurrence of thromboembolisms, heart failure (HF) and mortality1. Catheter ablation of AF has been demonstrated to be superior to antiarrhythmic drugs (AADs) in maintaining sinus rhythm on a mid- to long-term basis2,3. Both cryoballoon (CRYO) and radiofrequency (RF) ablation are in routine clinical use for not only paroxysmal AF (PAF) but also persistent AF (PersAF) worldwide4,5. A majority of studies have suggested that robotic magnetic navigation (RMN)-guided ablation for AF has similar success rate to that of the conventional manual technique, but with a reduced risk of major procedural complications6,7,8,9,10. Randomized controlled trials have shown that CRYO ablation is noninferior to manual RF ablation regarding efficacy and clinical outcomes for PAF11,12,13. Some studies have demonstrated a comparable efficacy between CRYO and RF ablation of PersAF with a relatively limited follow-up period14,15,16. However, based on the available data, little is known about the long-term efficacy of CRYO ablation on AF recurrence compared to that using RMN for the treatment of PersAF. Our previous study reported that CRYO is equivalent to RMN-guided ablation with regard to AF freedom in PersAF patients at mid-term follow-up17. Hence, the aim of this sequential study was to compare the long-term efficacy of CRYO with RMN-guided ablation in PersAF patients at 5 years follow-up, as well as the long-term clinical outcomes, including all-cause and cardiovascular rehospitalizations, new-onset neurological event, major bleeding event and the change in CHA2DS2-VASc score. Furthermore, we evaluated the patterns of anticoagulation (OAC) that have been used in patients after AF ablation.
Methods
Study design
The trial was a single-center, prospective, non-randomized and concurrent controlled study that compared the long-term efficacy and clinical outcomes of CRYO to RMN-guided ablation in patients with PersAF at a 5-year follow-up. The study design and full inclusion/exclusion criteria have been described in detail in our previous study17. All participating patients provided written informed consent. This study was approved by Ruijin Hospital Ethics Committee, Shanghai Jiao Tong University School of Medicine, in accordance with the principles of the Declaration of Helsinki. In brief, eligible patients were enrolled from June 2016 through October 2019 and assigned 1:1 to RMN-guided or CRYO ablation groups to undergo AF catheter ablation. Patients assigned to the RMN group underwent circumferential pulmonary vein isolation (PVI) guided by a 3-D mapping system (CARTO 3, Biosense Webster, USA) and the RMN Niobe ES system (Stereotaxis Inc., USA) using an irrigated RF ablation catheter (Navistar RMT ThermoCool, Biosense Webster, USA). Circumferential ablation lesions were delivered around each of the pulmonary vein (PV) ostia until each vein was electrically isolated to achieve bidirectional conduction block in all PVs. Patients assigned to the CRYO group underwent PVI using a second-generation 23- or 28- mm cryoballoon (Medtronic, USA) guided by a 3-D mapping system (Ensite system, Abbott, USA). The balloon was placed at each PV until it was occluded, and then the tissue was cooled until conduction block was achieved. A single “bonus” freeze was delivered to each vein following the rewarming phase of the successful lesion. An electrical PVI and bidirectional block was confirmed with the Achieve catheter (Medtronic, USA). If AF organized into atrial tachycardia (AT) or atrial flutter (AFL), activation and entrainment mapping were performed to guide ablation as necessary with a Freezor Max (Medtronic, USA) or RF catheter in both groups. Cavotricuspid isthmus (CTI) ablation was performed in patients who had clinical or inducible CTI-dependent AFL. Electrical cardioversions (ECs) were administered to restore sinus rhythm in patients who remained in AF after ablation. All patients were followed for 5 years after the ablation procedure.
Primary and secondary endpoints
The primary endpoint of the study was the freedom from any documented atrial tachyarrhythmias (ATs), including AF, AFL, and AT lasting ≥ 30 s after a 3-month blanking period at 5 years after the initial ablation procedure. The key secondary endpoints were defined as all-cause and cardiovascular rehospitalizations, rates of ECs and re-do ablation, new-onset neurological event, major bleeding event and the difference in CHA2DS2-VASc score at 5-year compared with baseline.
Follow-up and data collection
After the index procedure, patients were discharged on AADs, together with OAC. OAC was continued for at least 3 months after ablation, then re-evaluated in the fourth month, and the continuation of OAC was decided based on their rhythm and CHA2DS2-VASc score according to current guidelines. Class I/III AADs (including propafenone, amiodarone and sotalol) were maintained for 3 months and thereafter withdrawn if free from arrhythmia-related symptoms. Patients were observed for routine follow-up at 1 and 3 months, and then every 3 to 6 months (or earlier, if symptoms occurred) during the first year after ablation. Then, clinical appointments were scheduled every 6 months. Study visits included a medical history, physical examination, 12-lead electrocardiogram, and 24-hour Holter recordings. Clinical events occurring during the follow-up were recorded and evaluated. In addition, ambulatory electrograms were recorded when the patient had any symptoms during the study period. The patients received EC if they suffered PersAF recurrences within a 90-day blanking period after ablation and received either re-do ablations or continuing Class I/III AADs outside the blanking period according to the patients’ willingness. Moreover, the status of OAC therapy was recorded at the 5-year follow-up.
Statistical analysis
Continuous variables were presented as the mean ± standard deviation for normally distributed data and analyzed with the Student’s t-test or Wilcoxon rank-sum test, as appropriate. Categorical variables were expressed as percentages and compared using a chi-square test or Fisher’s exact test. The Kaplan– Meier method was used to determine cumulative estimates of arrhythmia recurrence from the time of enrollment through subsequent follow-up according to the treatment group. The log-rank test was used to compare the cumulative event rates between CRYO and RMN groups. The Cox proportional hazards model was applied to test the consistency of the group effect, while accounting for patient age and gender. Left atrium volume (LAV) was measured by contrast computed tomography scan of the left atrium. Univariable and multivariable Cox regression models were performed to determine which variables were significant by themselves in predicting arrhythmia recurrence. Logistic regression analysis was performed to investigate the risk factors associated with stroke prevalence at baseline and new-onset stroke. All statistical tests were two-sided, and a p-value < 0.05 was considered to indicate statistical significance. Statistical analysis was performed using R (R version 4.3.2).
Results
Patient characteristics and completeness of follow-up
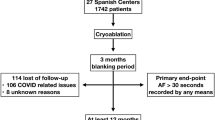
The primary analysis included 200 patients whose demographics and baseline characteristics have been previously published17. There were no significant differences in baseline characteristics between the two groups. Overall, 92% of patients (184/200) completed their follow-up at 5 years after a single AF ablation procedure, including 93 patients in the RMN group and 91 in the CRYO group. The median and maximum follow-up time were 60 months and 81 months, respectively. The patient flow diagram was shown in Fig. 1.

Flow chart of the study.
Primary endpoint
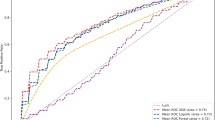
Following an initial AF ablation procedure, off Class I/III AADs, the long-term success rates at 5 years were 47.3% in the RMN group and 40.7% in the CRYO group, respectively. ATs free survival curves were shown in Fig. 2A. There was no significant difference in freedom from ATs between the two groups (47.3% vs. 40.7%, P = 0.32). Furthermore, we performed a pairwise subgroup analysis to determine the interaction between the two ablation techniques and clinical or demographic factors (Fig. 2B). The results suggested that RMN-guided ablation might be a better choice for patients presenting with a larger LAV (when LAV ≥ 143 ml, P = 0.04).

(A) Kaplan-Meier curves showed the cumulative freedom from recurrence of ATs after CRYO and RMN-guided ablation at 5 years. There was no significant difference in freedom from recurrence of AF between the two groups when compared by the log-rank test (P = 0.32). (B) Hazard ratios for AF recurrence in patients in the RMN and CRYO groups, in accordance with six clinical and demographic factors. Each rectangle indicated the estimated treatment effect, and the horizontal lines represent the 95% CI. * P Value from the interaction term in Cox regression model. BMI, body mass index; CI: confidence interval; CRYO: cryoballoon; HR: Hazard ratio; LAV, left atrium volume; RMN: robotic magnetic navigation.
Predictors of AF recurrence
Among those patients (103) with recurrence, 50 (50/103) patients suffered from PAF and/or AFL, and 53 (53/103) were still in PersAF. The proportion of PersAF was slightly higher in the CRYO group compared with the RMN group, but without statistical difference (29% vs. 24%, P = 0.423). Additionally, there were 27 patients (14 in CRYO and 13 in RMN) who experienced AF recurrence and continued with class I/III AADs. The Cox regression analysis was used to identify risk factors correlated with AF recurrence (Table 1). In the univariable analysis, LAV was found to be significantly predictive of AF recurrence (hazard ratio (HR), 1.006 [95% confidence interval (CI), 1.000-1.011], P = 0.037). Moreover, the multivariable analysis also demonstrated that LAV significantly increased the risk of AF recurrence (HR, 1.006 [95% CI, 1.000-1.012], P = 0.041).
Secondary endpoints
The results of secondary endpoints were summarized in Table 2. 54 all-cause rehospitalizations occurred in 43 patients (43/91; 47.3%) in the CRYO group when compared with 56 all-cause rehospitalizations that occurred in 46 patients (46/93; 49.5%) in the RMN group. No statistically significant difference was observed (P = 0.764). When examining cardiovascular rehospitalizations, it demonstrated that 39 cardiovascular rehospitalizations occurred in 31 subjects (31/91; 34.1%) of the CRYO group, whereas 36 cardiovascular rehospitalizations occurred in 28 subjects (28/93; 30.1%) of the RMN group. Also, no significant difference was found in the risk of cardiovascular rehospitalizations between the two groups (P = 0.565).
15 ECs were administered during follow-up to 13 subjects (13/91; 14.3%) in the CRYO group, whereas 9 ECs were given to 9 subjects (9/93; 9.7%) in the RMN group. The frequency of ECs did not differ between the two groups, although there was a trend for a lower rate in the RMN group than that of the CRYO group (P = 0.335). 13 re-do ablations were conducted in 12 subjects (12/91; 13.2%) in the CRYO group and 12 re-do ablations were conducted in 12 subjects (12/93; 12.9%) in the RMN group. Likewise, there was no significant difference in the rate of re-do ablations between the two groups (P = 0.954).
The cumulative 5-year incidence of new-onset stroke was 2.2% (4/184) and there was no major bleeding event occurring during follow-up. Compared with baseline, there was no difference in the change of CHA2DS2-VASC score at 5 years between the two groups. Among 184 patients, CHA2DS2-VASc score remained the same as baseline in 113 (61.4%) patients. There were 71 (38.6%) patients whose differences of CHA2DS2-VASc score increased by ≥ 1 at 5 years compared with baseline. A total of △CHA2DS2-VASc score was 79 shown by pie chart (Fig. 3). There were five risk factors contributing to the differences of CHA2DS2-VASc score, mainly due to the increase in age (68.4%), neurological events (10.1%), and new-onset cardiovascular events, including hypertension (12.7%), diabetes mellitus (3.8%), and HF (5.1%).

The differences of CHA2DS2-VASc at 5-year.
The status of OAC therapy at 5-year
All of the patients were on OAC for at least for 3 months following the initial procedure. The status and types of OAC therapy at 5 years were depicted in Fig. 4. Among 184 patients, 58 (31.5%, 29 in RMN and 29 in CRYO) continued OAC use whose mean CHA2DS2-VASc score was 2.0 ± 1.2, including those who were always on OAC and those who retook it after an occurrence. However, the remaining 126 (68.5%, 64 in RMN and 62 in CRYO) patients stopped OAC whose mean CHA2DS2-VASc score was 1.7 ± 1.4 according to the doctor’s prescription or on their own decision. Among the 126 patients who discontinued OAC, 61 (48.4%, 35 in RMN and 26 in CRYO) at risk of stroke with a CHA2DS2-VASc score of ≥ 2 stopped OAC use.

The status and types of OAC therapy.
New-onset stroke in association with OAC discontinuation
There were 9 (9/200) patients suffering from stroke events before the procedure. No clinical or demographic factors were found to be significantly predictive of stroke prevalence (Table 3). New-onset stroke occurred in 4 (2.2%, 1 in RMN and 3 in CRYO) patients at the 5-year follow-up. Nevertheless, they all experienced AF recurrences, with a mean CHA2DS2-VASc score of 2, however, they were on OAC use before the new-onset stroke. Further, we performed the logistic regression analysis, which did not show any risk factors related to these new-onset stroke events, including the status of OAC therapy (Table 4).
Discussion
To the best of our knowledge, this is the first prospective, observational and controlled trial that directly compares the long-term efficacy and clinical outcomes after catheter ablation using RMN or CRYO in patients with PersAF. Moreover, this is one of the longest follow-ups available for an RMN study regarding either PAF or PersAF ablation. Our main findings are as follows: First, there is no significant difference in the freedom from ATs at 5 years between the two groups. Cox regression analysis demonstrates that LAV is an important prognostic factor, significantly correlated with the risk of AF recurrence. Second, there are no significant differences in the risk of all-cause and cardiovascular rehospitalizations, rates of EC and re-do ablation, incidences of new-onset neurological event and major bleeding event, as well as the change in CHA2DS2-VASc score at the 5-year follow-up. Finally, despite guideline recommendations advocating for continued OAC use in patients at risk of stroke, OAC discontinuation after ablation is common, 48.4% of patients with a CHA2DS2 VASc score ≥ 2 stopping OAC after ablation. However, the cumulative 5-year incidence of stroke is extremely low (2.2%), with an annual rate of 0.4%, despite the high rate of OAC withdrawal.
Long-term efficacy and clinical predictors for AF recurrence
In the present study, we demonstrated a comparable long-term efficacy in terms of freedom from ATs by directly comparing the two different ablation techniques in patients with PersAF. The 5-year event-free rate after an initial procedure off Class I/III AADs was 40.7% in the CRYO group, which was in line with that of other investigations. They reported a single-procedure 5-year clinical success rates of 46.9%18 and 41.4%19 respectively following a second-generation CRYO ablation for treatment of PersAF. However, the long-term success rate of RMN-guided ablation in this trial was 47.3%, which seemed higher than that from earlier studies. Notably, our study demonstrated the longest mean follow-up of RMN-guided ablation for PersAF with a medium number of patient cohort. The freedom rate of AF was only 13% after a mean follow-up of 2.3 ± 2.3 years20. Likewise, another trial reported that AF-free rates was 42% at 3.5 years post ablation21. There might be some explanations for the difference in long-term efficacy by using RMN. Firstly, previous studies used earlier generations of the RMN system, non-irrigated or first generation irrigated-tip ablation catheters. Secondly, the patients enrolled in our study were younger with a mean age of 59.1 years and smaller mean LA diameter (43.1 mm), which might significantly improve the ablation effect. Although no difference in overall ATs recurrence was observed between the two groups, the proportion of AF recurrence in persistent form was higher in the CRYO group. The lesion size, depth, durability, and even lesions covering the posterior wall of the LA created by CRYO might differ from RMN-guided ablation and lead to different presenting patterns of AF22. These issues demanded further investigation.
Recent studies and meta-analyses have highlighted that an increase in LAV is associated with an increase in therapeutic ineffectiveness in both CRYO and RF ablation for AF23,24,25. We also identified LAV as a risk factor remarkably predicting AF recurrence, which was consistent with previous findings. Regarding the probability of recurrence in a given patient, the LAV should therefore be considered one of the most important factors in this prediction. In addition, Ikenouchi26 et al. first reported the impact of LA size on selection of catheter ablation methods for AF. The results showed that the efficacy was comparable between the two methods without LA enlargement, but CRYO was inferior to RF ablation in patients with LA enlargement. Likewise, we found that RMN-guided ablation might favor patients presenting with a larger LAV (when LAV ≥ 143 ml) by performing a pairwise subgroup analysis.
Long-term clinical outcomes and the change in CHA2DS2-VASc score
In the present trial, the cumulative all-cause rehospitalizations were nearly 50% and the cumulative cardiovascular rehospitalizations rates were more than 30% following AF ablation, with 12% readmission due to early AF recurrences requiring ECs within a 90-day blanking period, 13% underwent re-do ablations and 15% resuming Class I/III AADs outside the blanking period. However, very similar rates were found across the entire study for all-cause rehospitalizations, cardiovascular rehospitalizations, rates of ECs and re-do ablations over 5 years, suggesting the two different ablation techniques were comparable in PersAF patients. FIRE AND ICE trial have shown that all-cause rehospitalizations rate is 32.6% (CYRO) and 41.5% (RF) respectively throughout the 30 months of follow-up. Moreover, there were significant differences in favor of CRYO ablation with regard to fewer reinterventions, lower all-cause and cardiovascular rehospitalization rates27. In contrast, the CIRCA-DOSE study demonstrated the incidence of rehospitalizations within 1 year was 14.5%. Additionally, no difference between CRYO and RF is observed on health care utilization (emergency department visits, rehospitalizations, ECs, AADs use, and re-do ablations)28,29. By comparison, the rate of all-cause and cardiovascular rehospitalizations were lower compared with previous studies mainly due to younger age, lower rates of concomitant diseases and CHA2DS2-VASC score in our trial, hence, they might be healthier and have lower incidences of hospital readmissions. Moreover, the lower incidence of re-do ablations might relate to the patients’ unwillingness to receive second procedures considering economic costs.
Moreover, our study revealed a trend towards low incidences of new-onset neurological event and major bleeding event during follow-up. Additionally, there were 38.6% of patients whose differences of CHA2DS2-VASc score increased by ≥ 1 at 5 years compared with baseline. We found five risk factors contributing to the differences in CHA2DS2-VASc scores, mainly due to increasing age, new-onset cardiovascular and neurological events.
The status of OAC therapy after ablation in real-world
In the present observational study, the rate of discontinuation of OAC after AF procedure was 68.5% at 5 years, probably according to doctor’s prescription or on their own decision, thus reflecting real clinical practice. Among those stopping OAC, 48.4% of patients were at risk of stroke with a CHA2DS2-VASc score ≥ 2. The high rate of OAC withdrawal led to no major bleeding event. However, at the same time, the cumulative 5-year incidence of stroke was 2.2%, with annual rate of 0.4%. Similarly, Kawaji30 et al. reported 10-year clinical outcomes after AF ablation, in which they showed the incidence of ischemic stroke was also extremely low (4.2%) with an annual incidence of only 0.3%. A previous study has revealed that the risk of ischemic stroke on the assumption of no-OAC population was estimated about 2.0% per year based on the mean CHA2DS2-VASc score of 2.031. Thus, the rate of stroke in our study was low considering the high rate of OAC discontinuation. On the other hand, in our study, all the patients who experienced new-onset ischemic stroke suffered from AF recurrences, though they remained on OAC before stroke. Catheter ablation of AF could be useful not only to relieve patients’ symptoms but also to prevent cardiogenic stroke by maintaining sinus rhythm32. Hence, we postulated that the risk of stroke was highly relevant to arrhythmia recurrence despite OAC use. Therefore, our findings have shown that recommendations are commonly not being followed in clinical practice, reflecting a lack of randomized trial data to guide practice and equipoise with regards to the appropriate stroke prevention strategy after AF procedure. This suggests a critical need to further evaluate the association between OAC discontinuation after AF ablation and subsequent outcomes.
Study limitations
There are several limitations in the present study. Firstly, our study is a prospective, observational design, but not a randomized control trial. Patients are assigned to groups based on their own preferences. However, consecutive patients are enrolled and clinical features are similar in both groups. All baseline characteristics between the two groups are revealed not to affect the endpoints. Secondly, AF recurrence rate and asymptomatic episodes might have been underestimated since no continuous or long-duration monitoring for detecting arrhythmia recurrence was systematically used. Thirdly, our study further strengthens that the two different ablation techniques are comparable in PersAF patients; however, with a limited size in a single center. These findings still show the real outcomes of daily ablation practice and confirm the results of previous trials. Large-scale randomized clinical trials are demanded to further confirm the conclusions of this study.
Conclusions
Our findings show that CRYO is comparable to RMN-guided ablation with respect to long-term freedom from ATs in patients with PersAF. In addition, there are no significant differences in the risk of all-cause or cardiovascular rehospitalizations, rates of EC and re-do ablation, and incidences of new-onset neurological event and major bleeding event during subsequent follow-up. Notably, OAC discontinuation after ablation remains relatively common, despite guideline recommendations for continued OAC therapy in patients at risk of stroke with a CHA2DS2-VASc score ≥ 2. However, the cumulative 5-year incidence of stroke is extremely low.
Data availability
The data presented in this study will be shared on reasonable request to the corresponding author. The data are not publicly available due to ethical requirements.
References
Vinter, N. et al. Trends in excess mortality associated with atrial fibrillation over 45 years (Framingham Heart Study): Community based cohort study. Bmj 370 (370), m2724 (2020).
Wilber, D. J. et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: A randomized controlled trial. Jama 303 (4), 333–340 (2010).
Packer, D. L. et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The CABANA randomized clinical trial. Jama 321 (13), 1261–1274 (2019).
Wazni, O. M. et al. Cryoballoon ablation as initial therapy for atrial fibrillation. N Engl. J. Med. 384 (4), 316–324 (2021).
Verma, A. et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl. J. Med. 372 (19), 1812–1822 (2015).
Virk, S. A. & Kumar, S. Remote magnetic versus manual catheter navigation for atrial fibrillation ablation: A meta-analysis. Circ. Arrhythm. Electrophysiol. 12 (10), e007517 (2019).
Koutalas, E. et al. Efficacy and safety of remote magnetic catheter navigation vs. manual steerable sheath-guided ablation for catheter ablation of atrial fibrillation: A case-control study. Europace 17 (2), 232–238 (2015).
Adragão, P. P. et al. Safety and long-term outcomes of catheter ablation of atrial fibrillation using magnetic navigation versus manual conventional ablation: A propensity-score analysis. J. Cardiovasc. Electrophysiol. 27 (Suppl 1(1), S11–16 (2016).
Weiss, J. P. et al. A comparison of remote magnetic irrigated tip ablation versus manual catheter irrigated tip catheter ablation with and without force sensing feedback. J. Cardiovasc. Electrophysiol. 27 (Suppl 1(1), S5–S10 (2016).
Jez, J. et al. Comparison of atrial fibrillation ablation efficacy using remote magnetic navigation vs. manual navigation with contact-force control. Biomed. Pap Med. Fac. Univ. Palacky Olomouc Czech Repub. 164 (4), 387–393 (2020).
Kuck, K. H. et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl. J. Med. 374 (23), 2235–2245 (2016).
Andrade, J. G. et al. Cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: A randomized clinical trial. Circulation 140 (22), 1779–1788 (2019).
Sørensen, S. K., Johannessen, A., Worck, R., Hansen, M. L. & Hansen, J. Radiofrequency versus cryoballoon catheter ablation for paroxysmal atrial fibrillation: Durability of pulmonary vein isolation and effect on atrial fibrillation burden: The RACE-AF randomized controlled trial. Circ. Arrhythm. Electrophysiol. 14 (5), e009573 (2021).
Akkaya, E. et al. Ice or fire? Comparison of second-generation cryoballoon ablation and radiofrequency ablation in patients with symptomatic persistent atrial fibrillation and an enlarged left atrium. J. Cardiovasc. Electrophysiol. 29 (3), 375–384 (2018).
Hoffmann, E. et al. Outcomes of cryoballoon or radiofrequency ablation in symptomatic paroxysmal or persistent atrial fibrillation. Europace 21 (9), 1313–1324 (2019).
Kobori, A. et al. Comparison of cryoballoon and contact force-sensing radiofrequency ablation for persistent atrial fibrillation in clinical practice. Circ. J. 86 (2), 290–298 (2022).
Li, X. et al. Comparison of the mid-term outcomes of robotic magnetic navigation-guided radiofrequency ablation versus cryoballoon ablation for persistent atrial fibrillation. J. Cardiovasc. Dev. Dis. ;9(3). (2022).
Heeger, C. H. et al. Second-generation cryoballoon-based pulmonary vein isolation: Lessons from a five-year follow-up. Int. J. Cardiol. 312, 73–80 (2020).
Nekić, A. et al. Treatment of atrial fibrillation with second-generation cryoballoon followed by contact-sensing radiofrequency catheter ablation for arrhythmia recurrences-results of a 5-year follow-up. J. Interv Card Electrophysiol. 23 (10), 024–01752 (2024).
Schlögl, S. et al. Remote magnetic navigation versus manual catheter ablation of atrial fibrillation: A single center long-term comparison. Pacing Clin. Electrophysiol. 45 (1), 14–22 (2022).
Yuan, S. et al. Long-term outcomes of the current remote magnetic catheter navigation technique for ablation of atrial fibrillation. Scand. Cardiovasc. J. 51 (6), 308–315 (2017).
Shi, L. B. et al. Cryoballoon vs. radiofrequency catheter ablation: insights from NOrwegian randomized study of PERSistent Atrial Fibrillation (NO-PERSAF study). Europace 24 (2), 226–233 (2022).
Njoku, A. et al. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: A meta-analysis. Europace 20 (1), 33–42 (2018).
Park, J. H., Yang, D. H., Kim, J. H. & Kim, Y. R. Left atrium volume measured with multislice computed tomography as a prognostic predictor for atrial fibrillation catheter ablation outcomes. J. Clin. Med. ;13(7). (2024).
Bavishi, A. A. et al. Patient characteristics as predictors of recurrence of atrial fibrillation following cryoballoon ablation. Pacing Clin. Electrophysiol. 42 (6), 694–704 (2019).
Ikenouchi, T. et al. The impact of left atrium size on selection of the pulmonary vein isolation method for atrial fibrillation: Cryoballoon or radiofrequency catheter ablation. Am. Heart J. 231, 82–92 (2021).
Kuck, K. H. et al. Cryoballoon or radiofrequency ablation for symptomatic paroxysmal atrial fibrillation: reintervention, rehospitalization, and quality-of-life outcomes in the FIRE AND ICE trial. Eur. Heart J. 37 (38), 2858–2865 (2016).
Andrade, J. G. et al. Quality of life and health care utilization in the CIRCA-DOSE study. JACC Clin. Electrophysiol. 6 (8), 935–944 (2020).
Andrade, J. G. et al. Healthcare utilization and quality of life for atrial fibrillation burden: The CIRCA-DOSE study. Eur. Heart J. 44 (9), 765–776 (2023).
Kawaji, T. et al. Very long-term clinical outcomes after radiofrequency catheter ablation for atrial fibrillation: A large single-center experience. Int. J. Cardiol. 249, 204–213 (2017).
Lip, G. Y., Nieuwlaat, R., Pisters, R., Lane, D. A. & Crijns, H. J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 137 (2), 263–272 (2010).
Friberg, L., Tabrizi, F. & Englund, A. Catheter ablation for atrial fibrillation is associated with lower incidence of stroke and death: data from Swedish health registries. Eur. Heart J. 37 (31), 2478–2487 (2016).
Acknowledgements
None.
Funding
This research was funded by Shanghai Municipal Education Commission-Gaofeng Clinical Medicine, grant number 20161404 and Clinical Research Plan for Shanghai Hospital Development Center, grant number SHD2020CR4096.
Author information
Authors and Affiliations
Contributions
Conceptualization, Q.L. and X.L.; methodology, Y.X., Y.B., Y.W., C.L., Z.L., N.Z., T.L., K.C., W.P., L.W. and Q.J.; software, Q.L. and X.L.; validation, Q.L. and X.L.; formal analysis, Q.L. and X.L.; investigation, Q.L. and X.L.; resources, Q.L. and X.L.; data curation, Q.L. and X.L.; writing—original draft preparation, Q.L.; writing—review and editing, X.L.; supervision, Q.J.; project administration, L.W. and Q.J.; funding acquisition, L.W. and Q.J. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Luo, Q., Li, X., Xie, Y. et al. Long-term outcomes of cryoballoon versus robotic magnetic navigation guided radiofrequency ablation in patients with persistent atrial fibrillation. Sci Rep 15, 6181 (2025). https://doi.org/10.1038/s41598-025-90920-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-90920-5
