
Abstract
Treatment approaches are lacking for Fukuyama congenital muscular dystrophy (FCMD), the second most common type of pediatric muscular dystrophy after Duchenne muscular dystrophy (DMD) in the Japanese population. Recent studies demonstrating the involvement of prostaglandin (PG) D2 in DMD progression has led to the development of novel inhibitors targeting hematopoietic PGD2 synthase. This study aimed to determine the role of PGD2 in FCMD etiology in 42 patients with FCMD and 77 healthy age-matched individuals. Concentrations of tetranor-PGDM and tetranor-PGEM, the metabolites of PGD2 and PGE2, respectively, and creatinine were measured in spot urine samples. Mean tetranor-PGDM/creatinine and tetranor-PGEM/creatinine concentrations and tetranor-PGEM/tetranor-PGDM ratio were significantly higher in patients with FCMD than the healthy controls (5.3 ± 2.1 and 30.9 ± 52.3 ng/mg creatinine and 6.8 ± 2.0 vs. 3.4 ± 0.3 and 9.5 ± 0.9 ng/mg creatinine and 3.2 ± 0.3, respectively; p = 0.0011, p < 0.0001 and p < 0.0001, respectively). These metabolites were increased in patients with typical and severe FCMD phenotypes than in those with the mild FCMD phenotype, indicating their correlation with disease severity. These results implicate that PGD2 and PGE2 play important roles in FCMD pathogenesis and that novel hematopoietic PGD2 synthase inhibitors and steroids used in DMD may also have therapeutic utility in FCMD.
Similar content being viewed by others


Introduction
Fukuyama congenital muscular dystrophy (FCMD), the second most common type of childhood-onset muscular dystrophy in the Japanese population, is characterized by severe muscular dystrophy accompanied with ocular complications and central nervous system dysgenesis1, with approximately 90% of the patients never acquiring ambulation. Most patients become bedridden and develop complications, such as respiratory failure, heart failure, and dysphagia, after the age of 10 years and die around the age of 20 years2,3.
Patients with FCMD attain peak motor function between the ages of 5 and 10 years4 and can be classified based on their maximum motor development. The typical FCMD phenotype, which is characterized by the ability to sit without support or to slide on buttocks while sitting by extending and flexing the knees with hip rotation, accounts for 50% of the cases. Patients with the ability to crawl, stand, or walk, have the mild phenotype, which accounts for approximately 12% of the cases, whereas patients who lack head control or are not able to sit while having the ability of head control have the severe phenotype, which accounts for the remaining 38% of the cases5.
A 3-kb retrotransposal insertion into the 3’-untranslated region of FKTN is present in 87% of the patients with FCMD6. Aberrant mRNA splicing, induced by exon trapping, results in the truncation of fukutin encoded by FKTN, which underlies the pathogenic mechanism of FCMD7. Fukutin is a glycosyltransferase that transfers ribitol 5-phosphate from cytidine diphosphate-ribitol to the sugar chains of α-dystroglycan8, which is necessary for linking basal lamina with the cytoskeletal proteins in skeletal muscle and brain. In patients with FCMD, selective deficiency of α-dystroglycan as well as a secondary deficiency in laminin-211/merosin, which is specifically expressed in skeletal muscle, Schwann cells and thymocytes9, results in the disruption of a series of connections between the basement membrane and the cytoskeleton maintained via α-dystroglycan, leading to the development of muscular dystrophy.
Inflammatory response in dystrophic muscles has been considered to play an important role in disease pathogenesis and progression in patients with Duchenne muscular dystrophy (DMD)10,11. Specifically, increased expression of hematopoietic prostaglandin D2 (PGD2) synthase (HPGDS) was reported in inflammatory cells and grouped necrotic fibers in patients with DMD. Importantly, HPGDS expression in skeletal muscles exhibiting early necrotic changes has been reported in patients with severe DMD but not in controls or in patients with other types of dystrophy including FCMD11. PGD2 and PGE2 are synthesized by action of phospholipase A2 and cyclooxygenase that convert phospholipids to arachidonic acid and PGH2, a common precursor of PGD2 and PGE2 (Fig. 1). The enzyme HPGDS catalyzes the isomerization of the 9-11-endoperoxide group of PGH2 to 9-hydroxy and 11-keto groups, producing PGD2 in the presence of a reduced form of glutathione and Mg2+. Subsequently, PGD2 and PGE2 are metabolized to 11,15-dioxo-9α-hydroxy-2,3,4,5-tetranorprostan-1,20-dioic acid (i.e., tetranor-PGDM) and 9,15-dioxo-11α-hydroxy-2,3,4,5- tetranorprostan-1,20-dioic acid (i.e., tetranor-PGEM), respectively (Fig. 1). The urinary concentrations of these metabolites were reported to be higher in patients with DMD than in healthy controls12. In one study, the urinary tetranor-PGDM concentrations remained approximately 1.5-fold higher in patients with DMD than in age-matched controls until 7 years of age but significantly increased after 8 years of age, indicating that tetranor-PGDM might reflect clinical disease progression13. On the other hand, PGE2, as well as PGF2α and PGI2, promotes muscle fiber regeneration in DMD14,15. Although urinary tetranor-PGEM has been reported to be elevated in patients with inflammatory diseases, cancer, and obesity16,17, there has been little discussion on trends in tetranor-PGEM or the tetranor-PGEM/tetranor-PGDM ratio in patients with DMD.

Biosynthesis and metabolism of PGD2 and PGE2 to tetranor-PGDM and tetranor-PGEM. Enzymes and their inhibitors and major substances in the PG cascade are shown, in which the inhibitors are circled and enzymes are indicated in bold letters. NSAIDs, non-steroid anti-inflammatory drugs; TXA2, thromboxane A2; LPGDS, lipocalin-type PGD2 synthase; PGES, PGE2 synthase.
The demonstration that the HPGDS-specific inhibitor HQL79, which suppresses PGD2 production18, could ameliorate muscle necrosis and improve muscle strength in mdx mice in a murine model of DMD10 has led to the development of novel potent HPGDS inhibitors, such as TAS20419 and TAS20520. Studies in mdx mice and beagle dogs with the canine form of DMD, CXMD, demonstrate that these HPGDS inhibitors efficiently prevent muscular necrosis and muscle atrophy21. Phase 1 (NCT02246478)22 and early phase 2 (NCT02752048)23 trials including patients with DMD treated with TAS205 have been recently completed. The phase 2 trial has demonstrated the favorable safety profile of the drug23, whereas one phase 3 trial (NCT04587908, jRCT2041200055) is currently ongoing.
The above mentioned study reporting the lack of HPGDS immunoreactivity in FCMD11 included a small number of infant patients and did not evaluate the urinary metabolite concentrations. We hypothesized that PGD2 would play a role in the etiology and progression of disease in patients with FCMD. In the present study, we measured the tetranor-PGDM, tetranor-PGEM and creatinine concentrations in spot urine from 42 patients with FCMD and 77 healthy controls, and compared their urinary tetranor-PGDM/creatinine and tetranor-PGEM/creatinine concentrations and tetranor-PGEM/tetranor-PGDM ratios. Herein, we report that the urinary concentrations of both metabolites were significantly higher in patients with FCMD than in healthy controls, raising the possibility that therapeutic interventions targeting PGD2 and PGE2 production may mitigate clinical and pathologic disease progression in these patients.
Results
The cohort characteristics
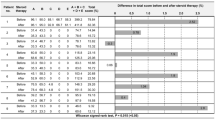
Table 1 summarizes cohort characteristics of healthy controls and patients with FCMD. The group of 42 Japanese patients with FCMD included 21 male and 21 female patients, with a mean age of 8.7 ± 1.0 (median, 6.5; range, 0–29) years (Table 1). Of these, 32 and 10 patients were homozygous and heterozygous founders harboring a 3-kb insertional mutation in FKTN and 4, 28, and 10 patients were classified as mild, typical, and severe phenotypes of FCMD, respectively. The healthy control group included 63 male and 14 female participants, with a mean age of 11.7 ± 0.5 (median, 13; range, 2–22) years.
Urinary tetranor-PGDM and tetranor-PGEM concentrations in healthy controls
Table 2 summarizes urinary tetranor-PGDM/creatinine and tetranor-PGEM/creatinine concentrations and tetranor-PGEM/tetranor-PGDM ratio in healthy controls, patients with FCMD, and their subpopulations. In the group of age-matched healthy controls, the urinary tetranor-PGDM concentration was 3.4 ± 0.3 (median 2.8, range 0.8–18.6) ng/mg creatinine (Fig. 2a) and the tetranor-PGEM concentration was 9.5 ± 0.9 (median 7.7, range 0.6–39.6) ng/mg creatinine (Fig. 2b). The mean tetranor-PGEM concentrations were 2.8-fold higher than the mean tetranor-PGDM concentrations in the same group. The tetranor-PGDM/tetranor-PGDM ratio was 3.2 ± 0.3 (median 2.5, range 0.4–18.3; Fig. 2c).

Urinary tetranor-PGDM/creatinine and tetranor-PGEM/creatinine concentrations and tetranor-PGEM/tetranor-PGDM ratios in healthy controls and patients with different FCMD phenotypes. (a) Urinary tetranor-PGDM/creatinine concentrations in healthy controls and in patients with specific FCMD phenotypes. (b) Urinary tetranor-PGEM/creatinine concentrations in healthy controls and in patients with specific FCMD phenotypes. (c) Urinary tetranor-PGEM/tetranor-PGDM ratio in healthy controls and in patients with specific FCMD phenotypes. +p < 0.05, ++p < 0.01 by Mann–Whitney U test; ##p < 0.01 by Tukey’s multiple comparisons test. (d) Dispersion graph of urinary tetranor-PGDM/creatinine and urinary tetranor-PGEM/creatinine concentrations. Symbols indicate healthy controls (〇) and patients with mild (△), typical (●), and severe (◇) FCMD phenotypes. Solid and dotted lines show linear regression lines for patients with FCMD (y = 2.68x + 16.9, r2 = 0.286) and healthy controls (y = 1.45x + 4.3, r2 = 0.145), respectively.
Among the healthy controls, the tetranor-PGDM concentrations were not significantly different between the healthy male and female controls (Table 2, p = 0.378). However, the tetranor-PGEM concentrations were significantly higher in healthy female controls than in healthy male controls (Table 2, p = 0.031 by Mann–Whitney U test). The mean values of tetranor-PGEM/tetranor-PGDM ratios were 2.1-fold higher in healthy female controls than in healthy male controls (Table 2, p < 0.0001 by Mann–Whitney U test).
The tetranor-PGDM concentrations of all or male healthy controls did not significantly change with age, whereas in female healthy controls, it decreased significantly with age (r = − 0.838; p = 0.003). The tetranor-PGEM concentrations of all healthy controls decreased significantly with age (r = − 0.237; p = 0.038); however, no age correlation was observed in the respective groups of males and females. The tetranor-PGEM/tetranor-PGDM ratio of all healthy controls was not correlated with age (p = 0.633), whereas in healthy female controls, it increased significantly with age (r = 0.540; p = 0.049).
Increased urinary tetranor-PGDM and tetranor-PGEM concentrations in patients with FCMD
The tetranor-PGDM concentrations in patients with FCMD were 5.3 ± 2.1 (median 4.1 and range 1.2–22.7), the mean value of which was 1.5-fold higher than that in healthy controls (p < 0.0001, Fig. 2a). The tetranor-PGEM concentrations in patients with FCMD were 30.9 ± 52.3 (median 24.1 and range 9.8–99.0, Fig. 2b), which were 5.8-fold higher than the tetranor-PGDM concentrations in patients with FCMD (Fig. 2a). Furthermore, the mean tetranor-PGEM concentrations were 3.2-fold higher in patients with FCMD than in healthy controls (p < 0.0001, Fig. 2b). The mean tetranor-PGEM/tetranor-PGDM ratios of the patients with FCMD (mean 6.8 ± 2.0, median 5.9, range 2.2–19.8) were 2.1-fold higher than those of the healthy controls (p < 0.0001, Fig. 2c).
The tetranor-PGDM and tetranor-PGEM concentrations and the tetranor-PGEM/tetranor-PGDM ratio did not differ between the male and female patients with FCMD and between the patients with homozygous and heterozygous 3-kb insertional mutations (Table 2).
The tetranor-PGDM and tetranor-PGEM concentrations and the tetranor-PGEM/tetranor-PGDM ratio did not significantly change with age in patients with FCMD (Table 2).
Disease severity-dependent changes in tetranor-PGDM and tetranor-PGEM concentrations
The analyses in patients categorized according to the clinical phenotype revealed that the tetranor-PGDM concentrations in those with the mild phenotype (mean 2.3 ± 0.4, median 2.4, range 1.2–3.4) were comparable to those of the healthy controls (p = 0.175). The mean tetranor-PGDM concentrations in patients with the typical phenotype (mean 5.3 ± 2.8, median 4.2, range 2.3–22.7) were 1.6-fold higher than those of the healthy controls (p = 0.007) and 2.3-fold higher than those of the patients with the mild phenotype (p = 0.002; Fig. 2a). The mean tetranor-PGDM concentrations in patients with the severe phenotype (mean 6.2 ± 3.9, median 5.0, range 2.0–11.5) were 1.9-fold higher than those of the healthy controls (p = 0.024) and 2.7-fold higher than those of the patients with the mild phenotype (p = 0.004) but were not significantly different than those of the patients with the typical phenotype (p = 0.523; Fig. 2a).
In patients with the mild phenotype, the mean tetranor-PGEM concentrations (mean 13.6 ± 8.6, median 13.3, range 9.8–16.2) were 5.5-fold higher than the tetranor-PGDM concentrations. Conversely, the tetranor-PGEM concentrations in these patients were 1.4-fold higher than those of the healthy controls, albeit without statistical significance (p = 0.099; Fig. 2b).
In patients with the typical phenotype, the tetranor-PGEM concentrations (mean 34.2 ± 75.9, median 26.3, range 11.3–99.0) were 6.3-fold higher than the tetranor-PGDM concentrations. The mean tetranor-PGEM concentrations were also 2.0-fold higher in patients with the typical phenotype than in those with the mild phenotype (p = 0.002).
In patients with the severe phenotype, the mean tetranor-PGEM concentrations (mean 28.6 ± 52.8, median 23.7, range 20.0–55.5) were 4.6-fold higher than the tetranor-PGDM concentrations. Additionally, the mean tetranor-PGEM concentrations of the patients with the severe phenotype were 3.9-fold higher than those of the healthy controls (p < 0.0001) and 1.8-fold higher than those of the patients with the mild phenotype (p = 0.0020). However, the tetranor-PGEM concentrations did not significantly differ between the patients with the severe and typical phenotypes (p = 0.328; Fig. 2b).
The mean values of tetranor-PGEM/tetranor-PGDM ratio of the patients with the mild phenotype (mean 6.2 ± 1.2, median 5.9, range 4.8–8.2) was 2.0-fold higher than that of the healthy controls (p = 0.003, Fig. 2c). The mean values of tetranor-PGEM/tetranor-PGDM ratio of the patients with the typical phenotype (mean 7.2 ± 2.6, median 6.3, range 2.9–19.8) was 2.0-fold higher than that of the healthy controls (p < 0.0001, Fig. 2c) but not significantly different than that of the patients with the mild phenotype (p = 0.383). Albeit not significant, the mean values of tetranor-PGEM/tetranor-PGDM ratio of the patients with the severe phenotype (mean 5.9 ± 4.9, median 4.9, range 2.2–13.9) was 1.8-fold higher than that of the healthy controls (p = 0.050) and 0.95- and 0.82-fold lower than that of the patients with the mild and typical phenotypes, respectively, (p = 0.855 and 0.407, respectively).
Figure 3d shows the dispersion graph of tetranor-PGDM and tetranor-PGEM concentrations among all patients with FCMD and healthy controls. Briefly, the values in the healthy controls distributed within an area much smaller than that of the patients with FCMD. In both the FCMD and control groups, the tetranor-PGEM concentrations exhibited a linear increase in a tetranor-PGDM concentration-dependent manner, creating a linear regression line with a slope of 2.68 for the group of all 42 patients with FCMD and a slope of 1.45 for the healthy control group; this finding was consistent with the fact that both PGD2 and PGE2 are produced in the same pathway (Fig. 1). The analysis of specific FCMD phenotypes revealed that the slope of the regression line decreased from the mild phenotype (y = 3.67x + 5.04, r2 = 0.700) to the typical (y = 2.98x + 18.3, r2 = 0.328) and severe (y = 0.90x + 23.0, r2 = 0.060) phenotypes in a disease severity-dependent manner, suggesting that PGD2 contributes to the disease pathology relatively more than PGE2 and the contribution of PGD2 production is more evident in the severe phenotype compared with the mild and typical phenotypes.
No significant association between disease severity and genotypes (homozygous vs. heterozygous), sex, or age of the patients with FCMD was observed (data not shown).
Discussion
In the present study, we found that urinary tetranor-PGDM and tetranor-PGEM concentrations were higher in patients with FCMD than in age-matched healthy individuals. We also found that the tetranor-PGDM and tetranor-PGEM concentrations were increased in parallel with disease severity, with higher values observed in patients without ambulatory function, such as those with severe and typical FCMD, compared to those with the ambulatory mild FCMD phenotype. These results suggest that PGD2 and PGE2 are involved in the pathogenesis of FCMD and that steroids or HPGDS inhibitors used in patients with DMD may, at least in part, also be useful for the treatment of patients with FCMD.
The tetranor-PGDM (3.4 ± 0.3 ng/mg creatinine) and tetranor-PGEM (9.5 ± 0.9 ng/mg creatinine) concentrations and the tetranor-PGEM/tetranor-PGDM ratio (3.2 ± 0.3) measured in the healthy controls included in the present study (Table 2; Fig. 2) are consistent with the reported values so far in a previous study (3.7 and 10.8 ng/mg creatinine and 2.92, respectively12). In the present study, the tetranor-PGDM concentrations of the patients with FCMD (5.3 ± 2.1 and 5.9 ± 1.0 ng/mg creatinine for all and male patients, respectively; Table 2) were lower than those reported in patients with DMD of all male (6.913 and 9.7 ng/mg creatinine12) whereas the tetranor-PGEM concentrations (30.9 ± 52.3 and 31.1 ± 3.5 ng/mg creatinine for all and male patients, respectively) and the tetranor-PGEM/tetranor-PGDM ratio (6.8 ± 2.0 and 6.6 ± 0.8 for all and male patients, respectively) of the patients with FCMD (Table 2) were higher than those reported in patients with DMD (20.5 ng/mg creatinine and 2.11, respectively12). The mean tetranor-PGEM concentration in male patients with FCMD, age-matched to ones with DMD in a previous study12, was 29.5 ± 5.1 ng/mg creatinine, which is significantly higher than that of patients with DMD. These results indicate that the contribution of PGD2 and PGE2 to disease pathophysiology is different between FCMD and DMD and that PGD2 production is lower whereas PGE2 production is higher in FCMD than in DMD.
Although the pathophysiologic functions of PGD2 and PGE2 in FCMD remain unclear, certain predictions can be made based on previous studies on other muscular dystrophies including DMD11,24. PGD2 production in DMD is involved in the expansion of muscular necrosis caused by muscular inflammation based on the observation that the administration of HPGDS inhibitors, including HQL79, TAS204, and TAS205, ameliorates muscular atrophy by decreasing urinary tetranor-PGDM concentrations in animal models10,19,20,21 and in patients with DMD22,23. Therefore, the HPGDS inhibitor TAS20520,21,22,23, which is currently evaluated in a phase 3 clinical trial for DMD (NCT04587908, jRCT2041200055) may also be useful for patients with FCMD. A recent study reported that transient receptor potential cation channel subfamily V member 2 (TRPV2) inhibitors, especially a widely used anti-allergic drug known as Tranilast, ameliorated cardiac function in muscular dystrophy including DMD, Becker muscular dystrophy, and limb-girdle muscular dystrophy with decreasing urinary tetranor-PGDM and increasing PGE324. In patients with DMD, steroids are commonly used to suppress the production of all PGs, including PGD2 and PGE2, by inhibiting phospholipase A2 (Fig. 1).
The finding that tetranor-PGEM concentrations are higher in FCMD than in DMD suggests that PGE2 is more actively involved in the pathogenesis of FCMD than DMD. PGE2, along with PGF2α and PGI2, promotes muscle fiber regeneration in DMD14,15. However, active muscle regeneration is more pronounced in young DMD patients, but quite poor in FCMD patients, at least at the ages studied here. FCMD patients exhibit more severe muscle involvement than those with DMD. Therefore, normal muscle regeneration appears to be less active in FCMD than in DMD. Although few studies have explored the role of PGE2 in FCMD pathogenesis, it may be involved in maintaining immature, small-diameter myofibers or promoting excessive fibrosis from an early stage, as seen in patients with FCMD.
In the present study, we used spot urine samples to evaluate PGD2 and PGE2 production in patients with FCMD. Given that muscle atrophy is associated with reduced serum and urinary creatinine concentrations in patients with FCMD compared to healthy controls25, tetranor-PGDM and tetranor-PGEM concentrations normalized to serum creatinine are better indicators of PGD2 and PGE2 production in the muscle tissue of patients with FCMD. Decreased muscle mass with disease progression, leading to a low creatinine concentration, may be partially associated with the higher tetranor-PGDM and tetranor-PGEM concentrations observed in patients with the typical and severe FCMD phenotypes compared to those with the mild FCMD phenotype. Future studies in patients with FCMD should investigate net changes in PGD2 and PGE2 production throughout the entire body using 24-hour urine collection. It is also important to evaluate the correlation between the level of each metabolite and the serum creatine kinase level of each patient with FCMD. As serum creatine kinase activity was negatively correlated with age and disease severity in patients with FCMD in our study (KI, TS, TM, and SN; unpublished results), both tetranor-PGDM and tetranor-PGEM concentrations are considered to be negatively correlated with serum creatine kinase activity.
FCMD is uniquely common in the Japanese population and is the second most common pediatric muscular dystrophy after DMD. Most patients are unable to walk for the rest of their lives, and many die around the age of 20 years. The efficacy of antisense nucleic acid therapy7 is being evaluated in an ongoing phase 1 clinical trial (NCT02246478). However, notably fewer treatment options are currently available for FCMD than for DMD. The HPGDS inhibitor TAS205 has been developed for DMD treatment22,23 based on the demonstrated role of PGD2, which is produced by HPGDS, in muscle fiber necrosis underlying DMD10,19,20,21. Based on one study, which used immunohistochemistry to demonstrate the increased expression of HPGDS in the necrotic muscle fibers of patients with DMD and polymyositis but not in those of the small number of patients with FCMD11, HPGDS inhibitors have not been considered as therapeutic options in patients with FCMD. However, several studies reported that steroid therapy suppressed disease progression in patients with FCMD or limb-girdle muscular dystrophy, also caused by FKTN mutations, as well as in patients with DMD26,27, potentially through the inhibition of PGD2 and PGE2 production (Fig. 1).
It is necessary to identify the subtypes of synthases and receptors for PGD2 and PGE2 and their cellular localization in the affected muscles of patients with FCMD to elucidate the pathologic function of PGD2 and PGE228. The isozyme and receptor subtypes can be identified with gene expression analyses of patient muscle samples, and their cellular localization can be determined with immunohistochemical staining, although muscle biopsies are rarely performed following the implementation of genetic testing for the definitive diagnosis of FCMD. Future studies are warranted to identify the isozyme and receptor subtypes and their cellular localization to understand the pathologic function of PGD2 and PGE2 in patients with FCMD and identify new therapeutic targets for FCMD.
Thus, we concluded that in patients with FCMD, urinary PGD2 and PGE2 metabolite concentrations were increased in parallel with the severity of the disease phenotype, indicating that PGD2 and PGE2 may be involved in the progression of FCMD as well as DMD. These results suggest that the novel HPGDS inhibitor TAS205 and steroids should be also considered for their utility as therapeutic agents for FCMD.
Methods
Patients
Of the 53 patients with FCMD who had attended Tokyo Women’s Medical University and agreed to participate in the study, 9 patients were excluded as they were unable to visit the hospital for evaluation, 1 had unclear genetic testing, and 1 was an infant with an unclear clinical form (Fig. 3). The present study included 42 patients with genetically confirmed diagnosis of FCMD. The clinical disease history and background characteristics of the patients, including age, sex, genotype, and clinical phenotype determined by the presence of complications such as epilepsy, respiratory failure, and cardiac failure, were retrospectively evaluated.

Study flow chart illustrating the inclusion and exclusion processes of patients with FCMD. Of the 53 patients with FCMD who agreed to participate in the study, 9 were excluded as they were unable to visit the hospital for evaluation, 1 had unclear genetic testing, and 1 was an infant with an unclear clinical form.
Healthy control samples were collected from volunteers who had consented to urinary prostaglandin metabolites study at Kobe Pharmaceutical University and 77 age-matched samples were selected according to the age of patients with FCMD.
The characteristics of all participants are summarized in Table 1. Since the first morning urine showed the lowest daytime concentration of tetranor-PGDM13, first morning urine samples were collected from the patients and healthy controls and stored at − 20 °C until further analysis.
This study was conducted according to the principles of the Declaration of Helsinki, and was approved by the Medical Ethics Committee of Tokyo Women’s Medical University (No.3818). Written informed consent was obtained from all the participants. The research volunteers were given explanations and gave consent in advance regarding the purpose, method, safety considerations, and risks of the experiment.
Measurement of urinary tetranor-PGDM and tetranor-PGEM concentrations
Urinary concentrations of tetranor-PGDM and tetranor-PGEM were measured by liquid chromatography with tandem mass spectrometry (API3000 system; Applied Biosystems, Foster City, CA), as previously reported12, and d6-tetranor-PGDM and d6-tetranor-PGEM (Cayman Chemical, Ann Arbor, MI) were used as internal standards. Urinary creatinine concentrations were determined with a creatinine measurement kit (L-Type Creatinine M, FUJIFILM Wako Pure Chemical Corp, Tokyo, Japan) to normalize tetranor-PGDM and tetranor-PGEM concentrations in spot urine samples.
Statistical analyses
The tetranor-PGDM/creatinine and tetranor-PGEM/creatinine concentrations were used for analyses with GraphPad Prism 8 (8.4.3) for Windows (GraphPad Software, La Jolla, CA). Data were summarized using descriptive statistics, including means, standard errors, frequencies, and percentages. The differences between two variables were assessed with the Mann–Whitney U test. Tukey’s multiple comparison test was used to analyze four variables among different groups. We performed a paired t-test (Wilcoxon signed-rank sum test) for two variables (tetranor-PGDM and tetranor-PGEM concentrations) in the same group. The relationship between two variables was assessed by Spearman’s rank correlation coefficient test. Statistical significance was set at p < 0.05.
Data availability
Raw data were generated at Tokyo Women’s Medical University and Kobe Pharmaceutical University. Derived data supporting the findings of this study are available from the corresponding author [KI] on request. Some data are not publicly available because of containing information that could compromise the privacy of research participants.
References
Fukuyama, Y., Kawazura, M. & Hamura, H. A peculiar form of congenital muscular dystrophy. Report of fifteen cases. Paediatr. Univ. Tokyo. 4, 5–8 (1960).
Osawa, M. et al. Fukuyama type congenital muscular dystrophy in Congenital Muscular Dystrophies (eds Fukuyama, Y., Osawa, M. & Saito, K.), 31–68 (Elsevier Science, 1997).
Ishigaki, K. Fukuyama congenital muscular dystrophy: clinical aspects in Translational Research in Muscular Dystrophy (eds Takeda, S., Miyagoe-Suzuki, Y. & Mori-Yoshimura, M.), 1–19 (Springer, 2015).
Sato, T. et al. The gross motor function measure is valid for Fukuyama congenital muscular dystrophy. Neuromuscul. Disord. 27, 45–49 (2017).
Ishigaki, K. et al. National registry of patients with Fukuyama congenital muscular dystrophy in Japan. Neuromuscul. Disord. 28, 885–893 (2018).
Kobayashi, K. et al. An ancient retrotransposal insertion causes Fukuyama-type congenital muscular dystrophy. Nature 394, 388–392 (1998).
Taniguchi-Ikeda, M. et al. Pathogenic exon-trapping by SVA retrotransposon and rescue in Fukuyama muscular dystrophy. Nature 478, 127–131 (2011).
Kanagawa, M. et al. Identification of a post-translational modification with ribitol-phosphate and its defect in muscular dystrophy. Cell. Rep. 14, 2209–2223 (2016).
Holmberg, J. & Durbeej, M. Laminin-211 in skeletal muscle function. Cell. Adh Migr. 7, 111–121 (2013).
Mohri, I. et al. Inhibition of prostaglandin D synthase suppresses muscular necrosis. Am. J. Pathol. 174, 1735–1744 (2009).
Okinaga, T. et al. Induction of hematopoietic prostaglandin D synthase in hyalinated necrotic muscle fibers: its implication in grouped necrosis. Acta Neuropathol. 104, 377–384 (2002).
Takeshita, E. et al. Urinary prostaglandin metabolites as Duchenne muscular dystrophy progression markers. Brain Dev. 40, 918–925 (2018).
Nakagawa, T. et al. A prostaglandin D2 metabolite is elevated in the urine of Duchenne muscular dystrophy patients and increases further from 8 years old. Clin. Chim. Acta. 423, 10–14 (2013).
Jackson, M. J., Brooke, M. H., Kaiser, K. & Edwards, R. H. Creatine kinase and prostaglandin E2 release from isolated Duchenne muscle. Neurology 41, 101–104 (1991).
McArdle, A., Foxley, A., Edwards, R. H. & Jackson, M. J. Prostaglandin metabolism in dystrophin-deficient MDX mouse muscle. Biochem. Soc. Trans. 19, 177S (1991).
Dong, L. M. et al. Urinary prostaglandin E2 metabolite and gastric cancer risk in the Shanghai women’s health study. Cancer Epidemiol. Biomarkers Prev. 18, 3075–3078 (2009).
Wen, W. et al. Association of urinary prostaglandin E2 metabolite and mortality among adults. Sci. Rep. 12, 8905 (2022).
Aritake, K. et al. Structural and functional characterization of HQL-79, an orally selective inhibitor of human hematopoietic prostaglandin D synthase. J. Biol. Chem. 281, 15277–15286 (2006).
Urade, Y. Benzoimidazole compound capable of inhibiting prostaglandin d synthetase, WO/2007/007778 (A1) (2007).
Urade, Y. Piperazine compound capable of inhibiting prostaglandin d synthase, WO/2010/104024 (A1) (2010).
Urade, Y. Orphan drug development for Duchenne muscular dystrophy by protein crystallization in space. IAC-16-B.3.3.6. In Proc. of 67th International Astronautical Congress (IAC) (2016).
Takeshita, E. et al. A phase I study of TAS-205 in patients with Duchenne muscular dystrophy. Ann. Clin. Transl Neurol. 5, 1338–1349 (2018).
Komaki, H. et al. Early phase 2 trial of TAS-205 in patients with Duchenne muscular dystrophy. Ann. Clin. Transl Neurol. 7, 181–190 (2020).
Takahashi, C. et al. Impact of the TRPV2 inhibitor on advanced heart failure in patients with muscular dystrophy: exploratory study of biomarkers related to the efficacy of Tranilast. Int. J. Mol. Sci. 24, 2167 (2023).
Ishigaki, K. et al. Renal dysfunction is rare in Fukuyama congenital muscular dystrophy. Brain Dev. 41, 43–49 (2019).
Murakami, T. et al. Efficacy of steroid therapy for Fukuyama congenital muscular dystrophy. Sci. Rep. 11, 24229 (2021).
Godfrey, C. et al. Fukutin gene mutations in steroid-responsive limb girdle muscular dystrophy. Ann. Neurol. 60, 603–610 (2006).
Smith, W. L., Urade, Y. & Jakobsson, P. J. Enzymes of the cyclooxygenase pathways of prostanoid biosynthesis. Chem. Rev. 111, 5821–5865 (2011).
Acknowledgements
This work was supported by Grant-in-Aid for Scientific Research (C) MEXT KAKENHI Grant Number JP 16K10001 (to KI), Grant No. 23K21430 (to IK and TIM), Japan Agency for Medical Research and Development (AMED) (grant no. 24ek0109611h0003 to KI), and SHISEIKAI Scientific Award (to KI). The authors would like to thank Enago (www.enago.jp) for the English language review and Dr.Hisateru Tachimori for his advices on statistical analysis.
Author information
Authors and Affiliations
Contributions
KI drafted the manuscript, conceived the study; participated in study design and performed data acquisition, data analysis and interpretation, and statistical analyses. AT participated in study design and measured prostaglandin metabolites in the urine samples of controls and patients. MTI participated in study design and performed data analysis and interpretation. TM, TS, MS, KI, and YK participated in study design, and collected the urine samples. NS drafted the manuscript. YU participated in study design, performed data acquisition, data analysis and interpretation, statistical analyses, and supervised the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
Keiko Ishigaki has received research grants from Sarepta Therapeutics, Inc. (clinical trial), Taiho Pharmaceutical Company, Ltd. (clinical trial), and Nippon Shinyaku Co. Ltd. (clinical trial).The other authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ishigaki, K., Takeuchi, A., Taniguchi-Ikeda, M. et al. Urinary prostaglandin D2 and E2 metabolites are elevated with disease severity in patients with Fukuyama congenital muscular dystrophy. Sci Rep 15, 6873 (2025). https://doi.org/10.1038/s41598-025-91539-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91539-2
