
Abstract
Hepatitis delta virus (HDV) is the most aggressive form of chronic viral hepatitis, yet substantial knowledge gaps exist regarding its epidemiology and optimal diagnostic workflows. From February 2019 to March 2022, an HBV screening project was conducted across various healthcare settings in Valencia, Spain. This included twenty-six primary care centers, six sexual and reproductive health centers, three mental health centers, three addiction treatment centers, selected hospital departments, outpatient clinics, and a penitentiary center. A retrospective analysis of HDV diagnostic and prevalence (2007–2020) was followed by prospective HDV screening using reflex testing from April to October 2022. Of 31,995 patients screened, 141 were HBsAg-positive (0.44% seroprevalence). Previously unknown HBV infection prevalence was 0.36%. Among HBsAg-positive patients, 5.15% had HDV IgG/IgM antibodies, and 2% had HDV RNA. Reflex single-step HDV testing increased HDV diagnosis coverage from 24 to 99.4%. This study highlights the effectiveness of reflex HDV testing, which significantly increased diagnostic coverage and simplified the screening process. Reflex testing provides a cost-effective and efficient approach, particularly benefiting high-risk populations such as migrants, who accounted for 77.8% of HBsAg-positive cases. Its implementation is crucial for improving patient outcomes and addressing gaps in HDV diagnosis and management.
Similar content being viewed by others

Introduction
Hepatitis delta virus (HDV) is classified as the severest form of chronic viral hepatitis1. Approximately 52% of individuals with acute HDV infection develop a chronic infection, which can result in cirrhosis within five years, and hepatocellular carcinoma (HCC) within ten years2. It is estimated that 4.5–15% of patients testing positive for hepatitis B virus (HBV) surface antigen (HBsAg) present HDV co-infection3. Current evidence suggests that HDV infection significantly contributes to liver-related morbidity and mortality among individuals co-infected with HBV4. HDV accounts for approximately 18% of all cirrhosis cases and 20% of HCC cases among HBsAg-positive individuals, markedly elevating the risk of HCC beyond that of HBV mono-infection alone5. Furthermore, HDV replication has been documented in liver transplant patients who received HBsAg-containing immunoglobulins, with HDV antibodies remaining detectable for several weeks following transplantation6.
Despite the exacerbation of health issues caused by HDV co-infection in HBV patients, current evidence indicates that HDV screening among HBV carriers is not routinely performed. A retrospective study in the Andalusia region of Spain revealed that only 18.5% of HBsAg carriers were tested for HDV between 2018 and 20227. This situation may be attributed to the historical absence of uniform screening guidelines and effective treatment options. These elements correspond to two of the last ten principles outlined by the World Health Organization (WHO) for early detection of diseases that warrant routine screening: ‘There should be an accepted treatment for patients with recognized disease’ and ‘There should be an agreed policy on whom to treat as patients’8. Regarding the agreed policy, both the WHO and the European Association for the Study of the Liver (EASL) recommend HDV testing for patients with HBV9,10. Additionally, in 2023, EASL further strengthened this guidance by recommending one-step HDV screening for all HBsAg carriers, with additional retesting when clinically indicated, or annually for those at continued risk of infection11. Various strategies could be adopted to enhance screening for HDV. In this context, reflex testing has proven to be effective in enhancing HDV testing among individuals who test positive for HBsAg12.
HDV prevalence across many European nations, including Spain, has experienced a decline due to the implementation of mandatory HBV vaccination programs13. Nevertheless, recent trends indicate an uptick in chronic hepatitis D prevalence in some European countries, predominantly among immigrant groups originating from areas where the virus is endemic, such as Eastern Europe, Africa, and Turkey14. Assessing HDV prevalence and its impact on liver dysfunction across both general and specific demographic segments is crucial for informing screening strategies, prevention measures, clinical management, policy formulation, public health initiatives, and the innovation of novel treatments5.
The present study aimed to ascertain the prevalence of HDV diagnosis among people living with HBV in the largest health department of Valencia, Spain. Additionally, we sought to establish a reflex HDV diagnosis workflow.
Methods
Project design
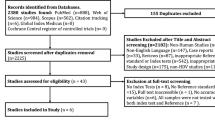
The study was performed following the TEST model16, which incorporates testing and linkage to care (LTC) into routine clinical workflows, electronic health record (EHR) modifications for patient eligibility and lab requests, systemic policy changes, and staff training with quality improvement feedback. The project was structured into two distinct stages: retrospective and prospective screening.
The prospective screening, implemented between February 2019 and October 2022, included two key phases. Phase 1 encompassed an initial opportunistic screening (February 2019–March 2022): this phase focused on integrating opportunistic HBV, HCV, and HIV screening across 26 primary care centers, six sexual and reproductive health centers, three mental health centers, three addiction treatment centers, selected hospital departments, outpatient clinics, and a penitentiary center15. Targeted individuals were ≥ 18 years old, had no prior test records, and could provide oral consent. In phase 2 (April–October 2022): Reflex testing for HDV was incorporated for HBsAg-positive patients undergoing diagnostic evaluations for hepatitis B. This approach streamlined the diagnostic process by automatically testing eligible patients for HDV in the same laboratory workflow.
The retrospective stage (phase 3) analyzed EHRs from HBsAg-positive patients receiving care between 2007 and 2020 in our department. Patients were included if they had previously undergone HDV IgG/IgM antibody testing. This analysis aimed to assess the prevalence of HDV diagnosis during this period. As a retrospective phase, the Ethics Committee for Drug Research of the General University Hospital Consortium waived the need for informed consent.
Testing technology
In this study, we used a range of diagnostic assays for HBV and HDV detection and quantification. The Alinity I® system (Abbott Laboratories) was employed for HBV detection, specifically the Alinity Anti-HBc II assay (#06P0660), Alinity i HBeAg assay (#G71188R04), Alinity HBe assay (#G71185R04), anti-HBs (#G72481R04) and HBV surface antigen (HBsAg, #G71228R03). For HDV antibody detection, we used the LIAISON® XL MUREX Anti-HDV assay (DiaSorin, # 311260), a reflex one-step immunoassay designed to identify both Immunoglobulin G (IgG) and Immunoglobulin M (IgM) antibodies, with a sensitivity of 100% and a specificity of 99.35%17. Quantification of HDV RNA was conducted using the RealStar® HDV RT-PCR Kit 1.0 (Altona Diagnostics, #401003). This real-time PCR assay has demonstrated sensitivity of 100% and specificity of 100% based on manufacturer data18.
Main outcomes and variables
Variables assessed across the study phases included sex, age (categorized into seven strata: < 25, 25–34, 35–44, 45–54, 55–64, 65–74, > 75), and country of origin (categorized into three groups: Spanish, non-Spanish, or unknown). The primary outcomes reported were the number of HBV and HDV tests conducted and the positive test results obtained. For phase 2, additional variables included the diagnosing hospital department, and the timing of HDV diagnosis. This parameter was divided into two groups (patients diagnosed between 2007–2017 and 2018–2020), corresponding to periods before and after the publication of the EASL guidelines advocating HDV screening11.
Statistical analysis
All data points were analyzed descriptively, with resulting statistics reported as percentages. To assess associations between categorical variables, Chi-square tests were utilized. Results from the Chi-square tests are presented wherever applicable. A p-value < 0.05 was considered statistically significant.
Ethical and legal aspects
The Ethics Committee of Hospital General Universitari de València (Valencia, Spain) approved this project on October 25, 2018 (code reference 10/2018). This research was conducted in accordance with the principles of the Helsinki Declaration and complied with the European Union’s General Data Protection Regulation (GDPR), guaranteeing the removal of all personal identifiers from the results.
Results
Phase 1: prospective opportunistic screening
As previously reported, a total of 31,995 individuals were tested for HBsAg19. HBsAg positivity was identified in 0.44% (n = 141) of the participants, with 82% (n = 115) of these individuals previously unaware of their infection status, indicating an unknown HBsAg prevalence of 0.36%. An elevated prevalence was noted in male participants relative to their female counterparts (Fig. 1A, 0.57% vs. 0.32%, p < 0.05). A statistically significantly higher prevalence of HBsAg was also observed among migrants compared to Spanish nationals (Fig. 1B), with rates of 1.27% and 0.30%, respectively (p < 0.0001). Additionally, a statistically significant variation was detected across different age groups, with a prevalence rate of 0.65% in the 45–64 age group (p = 0.0003).

Number of patients screened for HBV in phase 1 (February 2019 to March 2022) and HBsAg seroprevalence according to (A) sex and (B) nationality. Adapted from19.
Phase 2: impact of reflex testing on HDV diagnosis
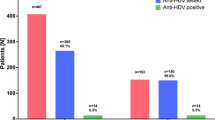
In this phase, analysis of 15,541 individuals for HBsAg, HDV antibodies, and HDV RNA was conducted prospectively. An HBsAg prevalence of 2.3% (n = 351), which included both newly identified and previously known infections, was noted. Among the HBsAg-positive individuals, 99.4% (n = 349) underwent further HDV testing, revealing an HDV IgG/IgM antibody prevalence of 5.15%. Among the individuals positive for HDV IgG/IgM antibodies (n = 18), 38.8% (n = 7) were identified as viremic, indicative of active HDV infection (Table 1). Patients with HDV antibodies had a mean age of 48.2 years and 61.1% (n = 11) were male. Regarding the country of origin, 22.2% (n = 4) were Spanish and 77.8% (n = 14) were migrants: 38.9% (n = 7) from Eastern Europe, 27.8% (n = 5) from Africa, 5.5% (n = 1) Latin-American, and 5.5% (n = 1) Asian. Of particular note is an atypical patient from Mali who had negative HDV viremia with very high HBV viremia (Table 1). Of the 7 HDV viremic patients, 4 were from Eastern Europe (fibrosis stage: one F0, two F3 and one F4), 2 Spanish (one F2 and one F4) and 1 African (F3). One patient, accounting for 5.5% (n = 1/18), was co-infected with HCV and HIV and at least 22.2% of the patients also had a recorded history of alcohol or drug abuse.
Phase 3: retrospective analysis of HDV
A total of 3663 patient records, positive for HBsAg, were evaluated for subsequent HDV testing (Table 2). Regarding the analysis of HDV antibody penetration, we found that HDV antibody testing was performed in about one third (28.4%, n = 1041) of HBsAg positive samples. This percentage remains low between the two analyzed periods: 708/2,286 patients (31.0%) between 2007 and 2017 and 333/1,377 (24.2%) between 2018 and 2020 (p < 0.0001). Overall, HDV antibody prevalence was 11.6%, with higher rates of 14.8% (n = 105) from 2007 to 2017 compared to 4.8% (n = 16) from 2018 to 2020. Data on HDV RNA testing could not be obtained. Information on the diagnosing hospital department was accessible for 79% (n = 2,596) of the patients.
Discussion
Understanding the prevalence of HDV infection, HBV co-infection, and its association with the increased risk of progressive liver disease is critical for informing viral hepatitis prevention and clinical management strategies. This study assesses the prevalence of HDV infection within the largest health department in Valencia, Spain, while establishing a workflow for reflex HDV diagnosis.
A previous seroprevalence study conducted in Spain during 2017–2018 reported an overall weighted prevalence of active HBV infection (HBsAg positive) in the population aged 20 to 80 years of 0.2%20. Our current data revealed a higher prevalence of HBsAg-positive cases, with 0.4% in Phase 1 and 2.3% in Phase 2. This discrepancy can be attributed to the inclusion of high-risk individuals, such as migrants and patients already flagged for HBV-related conditions, in Phase 2. In fact, detailed analysis confirmed that migrants constituted 77.8% of the HBsAg-positive cohort in phase 2. This aligns with previous reports showing elevated HBV and HDV prevalence among migrants due to lower vaccination rates and limited public health infrastructure in their countries of origin21,22. Our observation that the prevalence of serum HBsAg + was fourfold greater in foreigners than native Spaniards has been highlighted in prior studies assessing the rate of HDV in Spain23. These findings underscore the importance of targeted screening initiatives for high-risk groups, particularly migrants, as a critical component of public health interventions.
In regard to HDV detection, we observed a 5.15% seroprevalence rate of HDV-positive patients in the HBsAg-positive population. Among these individuals with HDV antibodies, 38.8% presented viremia, signaling active HDV infection. These findings align with the only other study we are aware of concerning HCV prevalence in Spain, which reported HDV Ab and RNA prevalence rates among HBsAg carriers 6.2%, with 39.9% of these individuals being viremic respectively24. HIV coinfection has a deleterious impact on patients with HDV25. We detected one patient coinfected with HIV (5.5%), which is comparable to the 6.5% reported in another study23.
Our rates are also consistent with European studies, where HDV antibody prevalence ranges from 5.1 to 16.7% (Supplementary Table 1)26,27,28,29,30,31. However, our RNA positivity rate is at the lower end of the European spectrum, which ranges from 38.1 to 80.5%12,26,27,28,29,30,31. These differences likely reflect variations in population characteristics, healthcare access, and diagnostic methodologies. For instance, Italy reports notably higher HDV Ab and RNA rates (10.7–16.7% and 5.7–10.8%, respectively), possibly due to distinct population risk profiles and broader screening efforts26,27. Future comprehensive analyses across European regions are needed to clarify these variations. In our study, 38.8% were migrants from Eastern Europe and 27.7% were Africans. The higher frequency of genotypes other than 1 in the latter could explain atypical virological patterns such as our patient from Mali with suppressed HDV viremia and very high HBV29. Fortunately, we also found that not all patients with active HDV viremia had advanced fibrosis, which is consistent with a recent review that shows that even over 50% of HDV patients may not present advanced fibrosis32. In our cohort of patients, 28.5% had F0-2 fibrosis and the rest F3-4.
Economic considerations are central to the implementation of HBV and HDV screening. A study in the UK demonstrated that HBV screening is cost-effective at a prevalence threshold of 0.25% or higher33. With a seroprevalence of 0.44% in Phase 1, our findings confirm that HBV screening in our population meets this threshold, justifying its implementation as a cost-effective public health measure. Additionally, opportunistic HBV testing during routine venipuncture further reduces costs, as illustrated by the modest incremental expense of €1.31 per test in our study. Reflex testing for HDV represents a natural extension of these efforts, offering significant advantages over traditional multi-step protocols27. By eliminating the need for additional blood draws34, reflex testing increased diagnostic rate from 28.4% in phase 3 to 99.4% in Phase 234. This approach is not only practical but also cost-effective, enabling efficient integration into existing workflows with minimal financial impact. Although single-step testing benefits are well known35, substantial barriers to the implementation of HDV reflex testing remain, as evidenced by a survey indicating that only 63% and 28% of Spanish hospitals are equipped to test for HDV antibodies and RNA, respectively36. In contrast, while 99% of these facilities conduct reflex testing for HCV, a mere 44% apply a similar approach to transitioning from HBV to HDV screening36. Thus, while reflex testing methodology has already proven effective in enhancing diagnostic coverage for other infections, such as HCV, its application to HDV represents a natural progression in optimizing viral hepatitis diagnostics.
The findings also highlight the need for routine reflex testing for HDV antibodies and RNA in all HBsAg-positive patients, regardless of clinical symptoms. Reflex testing simplifies the diagnostic process, making it particularly beneficial in resource-limited settings. It should prioritize high-risk groups, such as individuals over 50 and migrants from high-prevalence regions, and can mitigate stigma while improving access to preventive care. In the absence of mandatory HDV reporting, reflex testing addresses critical gaps in data collection and public health awareness, supporting its adoption as standard practice. This is particularly important in view of the novel therapeutic opportunities for patients with hepatitis delta, which have been postulated to contribute to HDV elimination in the future37.
Despite the promising outcomes of reflex testing, adherence to established guidelines, such as the 2017 EASL recommendations for systematic HDV testing among HBV carriers, remains inconsistent10. In our study, HDV testing rates varied significantly across hospital departments, with higher rates in infectious disease and hepatology units (54% and 44%, respectively) compared to primary care (10%). Other European studies have reported a broad range of diagnostic rate for HDV Ab, varying from 16.4 to 100%26,27,28,29,30,31. This variability highlights the need for standardized diagnostic protocols and increased clinician education to ensure consistent guideline implementation across all healthcare settings.
The findings of this study should be interpreted in the context of its limitations. First, Phase 1 encompassed a period that may have been impacted by the sanitary restrictions imposed during the COVID-19 pandemic38. This also implies that the loss of viral hepatitis follow-up during this time frame would reinforce the need to carry out projects to recapture lost patients39. Secondly, despite its breadth, the comprehensive prospective screening conducted in Phase 2 was limited by its short duration, potentially not reflecting the long-term effectiveness of the strategies deployed. Additionally, the reliance on retrospective data in Phase 3, which may introduce biases related to incomplete documentation. Furthermore, the absence of HDV RNA testing data in this phase likely led to underestimation of the actual prevalence of active HDV infections during that timeframe, because anti-HDV antibody testing alone cannot confirm viremia or differentiate between past exposure and active infection. Without RNA testing, antibody-positive but RNA-negative cases were excluded, potentially underreporting the true prevalence of HDV viremia. Moreover, we did not collect data regarding risk factors for hepatitis D in HBsAg-positive cases, thus difficulting the analysis of whether HDV testing was mainly requested in high-risk groups. Finally, because the study was performed exclusively in a health department in Valencia, Spain, the applicability of our findings may be limited across different demographics and healthcare infrastructures, reducing their generalizability.
In conclusion, this study supports reflex testing as an essential tool for HDV diagnosis, capable of overcoming the limitations of traditional multi-step protocols. Its widespread implementation, alongside targeted screening strategies, is pivotal for reducing the burden of HDV-related liver disease and improving outcomes for high-risk populations. Future initiatives should focus on expanding reflex testing capabilities, addressing systemic barriers, and fostering a unified approach to HDV management across healthcare settings.
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
References
Hughes SA, Wedemeyer H, Harrison PM. Hepatitis delta virus. Lancet. 2011; 378(9785):73–85. Epub 20110420. https://doi.org/10.1016/S0140-6736(10)61931-9.
Miao, Z. et al. Estimating the global prevalence, disease progression, and clinical outcome of hepatitis delta virus infection. J. Infect. Dis. 221(10), 1677–1687. https://doi.org/10.1093/infdis/jiz633 (2020).
Abbas, Z. & Abbas, M. An insight into the factors affecting the prevalence and natural history of hepatitis D. Cureus. 15(8), e43362. https://doi.org/10.7759/cureus.43362 (2023).
Gish, R. G. et al. Association of hepatitis delta virus with liver morbidity and mortality: A systematic literature review and meta-analysis. Hepatology. 79(5), 1129–1140. https://doi.org/10.1097/HEP.0000000000000642 (2024).
Stockdale, A. J. et al. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J. Hepatol. 73(3), 523–532. https://doi.org/10.1016/j.jhep.2020.04.008 (2020).
Chauhan, R. et al. Reactivation of hepatitis B after liver transplantation: Current knowledge, molecular mechanisms and implications in management. World J. Hepatol. 10(3), 352–370. https://doi.org/10.4254/wjh.v10.i3.352 (2018).
Casado, M. et al. Current status of hepatitis delta in Andalusia: multicenter study. J. Hepatol. 78, S1126. https://doi.org/10.1016/s0168-8278(23)03249-x (2023).
Wilson, J. M. & Jungner, Y. G. Principles and practice of mass screening for disease. Bol Oficina Sanit Panam. 65(4), 281–393 (1968).
World Health Organization. Guidelines for the prevention, diagnosis, care and treatment for people with chronic hepatitis B infection: web annex B: evidence-to-decision making tables and GRADE tables. [Internet] 2024; (accessed on 07-05-2024). Available from: https://www.who.int/publications/i/item/9789240090903.
European Association for the Study of the L. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 67(2), 370–398. https://doi.org/10.1016/j.jhep.2017.03.021 (2017).
European Association for the Study of the L. EASL Clinical Practice Guidelines on hepatitis delta virus. J. Hepatol. 79(2), 433–60. https://doi.org/10.1016/j.jhep.2023.05.001 (2023).
Palom, A. et al. Implementation of anti-HDV reflex testing among HBsAg-positive individuals increases testing for hepatitis D. JHEP Rep. 4(10), 100547. https://doi.org/10.1016/j.jhepr.2022.100547 (2022).
Rizzetto, M. & Stroffolini, T. Forty-five years after the discovery of the hepatitis D virus: Where do we stand?. Viruses. 13(4), 1. https://doi.org/10.3390/v13040555 (2021).
Demirel, A. et al. Epidemiology of hepatitis D virus infection in Europe: Is it vanishing?. J. Viral. Hepat. 31(2), 120–128. https://doi.org/10.1111/jvh.13899 (2024).
Ortega-Gonzalez, E. et al. HIV screening and linkage to care in a health department in Valencia, Spain: Lessons learned from a healthcare quality improvement project. Medicine (Baltimore). 101(41), e30400. https://doi.org/10.1097/MD.0000000000030400 (2022).
Sanchez, T. H. et al. A novel approach to realizing routine HIV screening and enhancing linkage to care in the United States: Protocol of the FOCUS program and early results. JMIR Res. Protoc. 3(3), e39. https://doi.org/10.2196/resprot.3378 (2014).
DiaSorin. LIAISON® XL Anti-HDV. Total automation for an accurate, easy and fast HDV diagnosis. (2020). Available from: https://hdv.diasorin.com/ese%20antiHDV%204330-A%2008-2018%20low.pdf.
Altona Diagnostics. Instructions for Use RealStar® HDV RT-PCR Kit 1.0(2018 November 27th 2024). Available from: https://altona-diagnostics.com/wp-content/uploads/2023/12/RealStar-HDV-RT-PCR-Kit-1.0_WEB_RUO_EN-S01.pdf.
Ortega Gonzalez, E. et al. Opportunistic population screening as a hepatitis elimination strategy: the CRIVALVIR-FOCUS program. Int. J. Infect. Dis. 146, 107131. https://doi.org/10.1016/j.ijid.2024.107131 (2024).
Limia Sanchez, A., & Olmedo Luceron, C. [2(nd) Seroprevalence Study in Spain, 2017–2018]. Rev Esp Salud Publica. 95. Epub 20210318 (2021).
Tout, I., Loureiro, D. & Asselah, T. The Changing Demographics of Hepatitis B Virus Infection. Clin Liver Dis. 25(4), 673–687. https://doi.org/10.1016/j.cld.2021.06.001 (2021).
Wedemeyer, H. The burden of hepatitis D - defogging the epidemiological horizon. J. Hepatol. 73(3), 493–495. https://doi.org/10.1016/j.jhep.2020.06.037 (2020).
Aguilera, A. et al. Prevalence and incidence of hepatitis delta in patients with chronic hepatitis B in Spain. Eur. J. Gastroenterol. Hepatol. 30(9), 1060–1062. https://doi.org/10.1097/MEG.0000000000001163 (2018).
Rodriguez-Tajes, S. et al. Characterizing chronic hepatitis delta in Spain and the gaps in its management. J. Hepatol. 78, S1098. https://doi.org/10.1016/s0168-8278(23)03208-7 (2023).
Yen, D. W., Soriano, V., Barreiro, P. & Sherman, K. E. Triple threat: HDV, HBV, HIV coinfection. Clin. Liver Dis. 27(4), 955–972. https://doi.org/10.1016/j.cld.2023.05.010 (2023).
Piermatteo, L. et al. Stable temporal trend of HDV seroprevalence in central Italy across the last two decades with the circulation of HDV sub-genotypes 1 inducing different inflammatory stimuli. J. Hepatol. 78, S1122–S1123. https://doi.org/10.1016/s0168-8278(23)03244-0 (2023).
Cossiga, V. et al. Implementation of anti-HDV reflex testing among HBsAg-positive in a tertiary center in South Italy. J. Hepatol. 78, S903 (2023).
Herta, T. et al. Hepatitis D screening in HBsAg positive individuals in Germany: insufficient implementation results in a large number of undiagnosed cases. J. Hepatol. 78, S1090–S1091. https://doi.org/10.1016/s0168-8278(23)03198-7 (2023).
Cardoso, M. et al. Predominance of genotype 5 hepatitis delta virus infection in a Portuguese centre. J. Hepatol. 78, S1111 (2023).
Truchi, R., De Monte, A., Tran, A., Giordanengo, V. & Ollier, L. Positive impact of reflex testing in performing hepatitis delta serology in HBsAg+ patients. J. Hepatol. 78, S1158–S1159 (2023).
Carey, I. et al. Hepatitis D infection in a HBsAg cohorts referred from specialist liver clinics vs. reflex community referred patients in South East London. J. Hepatol. 78, S905–S906 (2023).
Negro, F. & Lok, A. S. Hepatitis D: A review. JAMA. 330(24), 2376–2387. https://doi.org/10.1001/jama.2023.23242 (2023).
Williams, J. et al. An economic evaluation of the cost-effectiveness of opt-out hepatitis B and hepatitis C testing in an emergency department setting in the United Kingdom. Value Health. 23(8), 1003–1011. https://doi.org/10.1016/j.jval.2020.03.014 (2020).
Terrault, N. A. & Ghany, M. G. Enhanced screening for hepatitis D in the USA: Overcoming the delta blues. Dig. Dis. Sci. 66(8), 2483–2485. https://doi.org/10.1007/s10620-020-06584-w (2021).
Buti, M. et al. Impact of the anti-HDV reflex testing on the reduction of hepatitis D burden in Spain. J. Hepatol. 78, S896 (2023).
Cabezas, J., Aguilera, A., Berenguer, M., Buti, M., Forns, X., et al. Survey to evaluate the implementation of the recommendations on the comprehensive diagnosis of viral hepatitis in a single extraction: where are we? Vienna (Austria), EASL Congress [Internet] 2023; (accessed on 03-02-2025). Available from: https://www.postersessiononline.eu/173580348_eu/congresos/ILC2023/aula/-FRI_188_ILC2023.pdf.
Soriano, V., Moreno-Torres, V., Trevino, A., Corral, O. & de Mendoza, C. Bulevirtide in the treatment of hepatitis delta: Drug discovery, clinical development and place in therapy. Drug. Des. Dev. Ther. 17, 155–166. https://doi.org/10.2147/DDDT.S379964 (2023).
Ramos-Rincon, J. M. et al. Impact of the COVID-19 pandemic on hospital admissions due to viral hepatitis in Spain. J. Clin. Virol. 167, 105553. https://doi.org/10.1016/j.jcv.2023.105553 (2023).
Parada Vazquez, P. et al. Artificial intelligence-assisted identification and retrieval of chronic hepatitis C patients lost to follow-up in the health area of Pontevedra and O Salnes (Spain). Gastroenterol Hepatol. 48(1), 502226. https://doi.org/10.1016/j.gastrohep.2024.502226 (2025).
Acknowledgements
The authors thank the staff of HGUV for their contribution to this work. We also thank Ánchel González Barriga, from Medical Science Consulting (Spain), for providing editorial support, in the form of medical writing and assembling tables based on the authors’ detailed directions, collating author comments, copyediting, fact-checking, and referencing.
Funding
We acknowledge funding from Gilead Sciences’ FOCUS program to support viral hepatitis screening and linkage to the first medical appointment after diagnosis. FOCUS funding does not support activities beyond the first medical appointment and is agnostic to how organizations handle subsequent patient care and treatment.
Author information
Authors and Affiliations
Contributions
EOG, MDOM, AC, JLG-S and MGD contributed to the conception of the study and the work design; MM-R, CGC, NGM, MDM and MPT performed the acquisition and analysis of the data; EOG, MDOM, AC, JLG-S and MGD have drafted the work or substantively revised it; All authors contributed to the interpretation of the data and approved the submitted version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
AC and JLG-S own stock and are employees of Gilead Sciences. The remaining authors declare no conflicts of interest concerning the research, authorship, and publication of this article. Data collection and management were conducted independently, with additional oversight of independent data monitoring agencies.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ortega González, E., Ocete Mochón, M.D., Martínez-Roma, M. et al. Current prevalence of hepatitis delta diagnosis in Valencia, Spain. Sci Rep 15, 7584 (2025). https://doi.org/10.1038/s41598-025-91765-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91765-8
