
Abstract
This retrospective study investigates the correlation between visual acuity changes and structural modifications observed through optical coherence tomography (OCT) in patients with central retinal artery occlusion (CRAO) treated with urokinase. Conducted at the Neuro-Ophthalmology Center of Xi’an People’s Hospital from January 2022 to May 2023, the study included 217 CRAO patients (217 eyes), comprising 157 males and 60 females, aged 18 to 83 years (mean age: 57.8 ± 13.3 years). Key data were collected on visual acuity, ocular motility, and various imaging techniques at admission and post-thrombolysis. Results showed a significant improvement in visual acuity from 2.4 ± 0.5 to 1.9 ± 0.7 (P < 0.001) after treatment. Notably, patients with severe retinal damage had poorer visual recovery compared to those with milder damage. OCT analysis revealed a decrease in macular foveal retinal thickness from 415.5 ± 107.7 μm to 362.1 ± 93.8 μm (P < 0.001). Correlation analysis confirmed an association between visual acuity and retinal thickness (P < 0.001). Inter-observer variability for OCT grading was assessed using Cohen’s Kappa, which yielded a Kappa value of 0.873 (P < 0.001). This study underscores the relationship between visual recovery and retinal structural changes in CRAO patients, emphasizing the efficacy of urokinase treatment, particularly in mild to moderate cases, and the need for personalized therapeutic strategies based on condition severity.
Similar content being viewed by others
Introduction
Central retinal artery occlusion (CRAO) is an ophthalmic emergency caused by acute retinal ischemia due to obstruction of the central retinal artery, potentially leading to catastrophic visual impairment or complete vision loss1. It is more commonly seen in the elderly, with an incidence of approximately 1 per 100,000 people per year2. Risk factors for CRAO include carotid artery disease, atrial fibrillation, arterial hypertension, valvular heart disease, diabetes, hypercholesterolemia, coronary artery disease, smoking, a history of transient ischemic attacks or cerebrovascular accidents, and a family history of any type of vascular disease2,3,4. CRAO can be classified into four clinical subtypes based on clinical presentation and etiology: non-arteritic permanent, arteritic, non-arteritic with cilioretinal artery sparing, and non-arteritic transient5. Patients typically present with sudden, painless, monocular vision loss, with approximately 61% of CRAO patients reporting visual acuity as poor as counting fingers or worse4. Moreover, research has established a strong correlation between the duration of CRAO and the visual acuity outcomes6. Consequently, early imaging assessment and prompt diagnosis of CRAO are critical for guiding treatment strategies and enhancing visual prognosis3.
Optical coherence tomography (OCT) serves as an indispensable tool for evaluating the extent of retinal ischemia, staging the disease, and predicting patient prognosis4. While fluorescein fundus angiography (FFA) is regarded as the gold standard for the diagnosis of CRAO and is an important metric for assessing improvements in visual function1,7, the correlation between FFA results and enhancements in visual function is frequently suboptimal, attributable to variations in etiology and disease progression among CRAO patients. OCT Angiography (OCTA) plays a crucial role in CRAO by non-invasively visualizing retinal and choroidal blood flow, facilitating the assessment of vascular changes and enabling early detection of ischemic damage and neovascularization. OCT, as a non-contact, non-invasive, high-resolution optical imaging modality, elucidates the layered architecture of the retina and facilitates the observation of in vivo pathological changes8. Current OCT investigations in CRAO predominantly concentrate on image analysis9. For instance, Kim et al.10 conducted an analysis of OCT images from 12 CRAO patients and determined that individuals with less macular damage tended to exhibit better visual prognoses.
Urokinase thrombolysis has shown promising outcomes in the treatment of CRAO, particularly for patients diagnosed at an early stage, as it significantly enhances the likelihood of visual recovery4,11. Previous studies have corroborated the safety and efficacy of urokinase thrombolysis in managing CRAO12. Nevertheless, the relationship between alterations in visual acuity and OCT imaging findings in CRAO patients warrants further investigation. Therefore, this study aims to explore the association between visual acuity and structural modifications observed in OCT images by analyzing visual changes before and after urokinase thrombolysis treatment in CRAO patients.
Methods
Study design and patients
This retrospective study encompassed patients diagnosed with CRAO who were hospitalized at the Neuro-ophthalmology Center of Xi’an People’s Hospital from January 2022 to May 2023. The study received approval from the Ethics Committee of Xi’an People’s Hospital (Approval No. 20220005). Given the retrospective nature of the investigation, the Ethics Committee of Xi’an People’s Hospital waived the necessity for individual informed consent.
The inclusion criteria for patient selection were as follows: (1) color fundus photography revealing grayish-white edema in the posterior pole, (2) FFA (Spectralis HRA, Heidelberg, Germany) indicating a delayed arm-retinal circulation time exceeding 15 s and/or an extended time of more than 2 s for fluorescein filling from the central retinal artery to its branches, potentially accompanied by retrograde filling, faint fluorescein flow, segmental filling patterns, and with or without fluorescein leakage3, (3) OCT (Spectralis OCT, Heidelberg, Germany) demonstrating retinal edema characterized by thickening, indistinct anatomical layers, and increased reflectivity, (4) logarithm of the minimum angle of resolution (LogMAR) visual acuity of ≥ 1.0, and (5) onset of symptoms occurring within 168 h.
Exclusion criteria included: (1) ocular ischemic syndrome (transient ocular ischemia), (2) inflammatory CRAO, (3) computed tomography (CT)-confirmed intracranial hemorrhage, (4) a history of intracranial hemorrhage, arteriovenous malformation, or intracranial aneurysm, (5) a history of intracranial surgery, head trauma, or stroke in the past 3 months, (6) active bleeding history in the gastrointestinal or urinary tract within the last 21 days, and (7) severe cardiovascular, pulmonary, renal, or hepatic disease.
During the study period, the routine standard treatment was performing arterial thrombolysis using a femoral artery approach, with both antegrade administration and retrograde infusion into the ocular artery with urokinase12.
I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Data collection and assessment criteria
The following data were collected from the patient’s medical records: visual acuity at admission and one week post-arterial thrombolysis, ocular motility, slit-lamp microscopy, fundus photography, OCT, FFA, and results from cranial magnetic resonance imaging or CT.
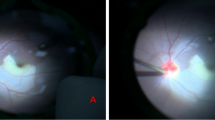
Best-corrected visual acuity was assessed utilizing the International Standard Visual Acuity Chart and subsequently converted to LogMAR for statistical analysis13,14. An enhancement of one level in visual acuity was regarded as an improvement in vision. OCT was performed immediately upon admission of the patient and again one week post-thrombolysis. The retinal thickness measured by OCT serves as an indicator of the extent of retinal edema, while structural alterations in retinal tissue may differ according to the severity depicted in OCT images, such as structural loss, blurriness, or decreased visibility. Based on the morphological characteristics observed in OCT images at admission, patients were classified into four categories: extremely severe (unable to analyze the retinal layered structure), severe (retinal layered structure is blurred and partially visible, with half or fewer of the retinal layers distinguishable), moderate (more than half of the retinal layers are visible), and mild (retinal layered structure is identifiable) (Fig. 1). All evaluations were independently conducted by two physicians possessing extensive clinical experience, and inter-observer variability for OCT grading was assessed.

Morphological classification of the retinal thickness and layered structures. (A) Extremely severe macular edema; unable to analyze the layered structure. (B) Severe; partially discernible retinal layered structure; able to differentiate one half of the retinal layers or less. (C) Moderate; able to differentiate more than half of the retinal layers. (D) Mild; clearly able to differentiate the retinal layers.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA), with continuous variables presented as mean ± standard deviation (± s). Paired t-tests were utilized to compare LogMAR visual acuity and retinal thickness measurements before and after treatment. Differences in age and gender distribution among groups were analyzed using the χ² test, while variations in LogMAR visual acuity and retinal thickness among groups were evaluated using one-way analysis of variance. The association among visual acuity, baseline OCT severity grading and macular retinal thickness was assessed using the non-parametric Spearman rank correlation test. Inter-observer variability for OCT grading was evaluated by calculating Cohen’s Kappa. A two-sided p-value of < 0.05 was considered statistically significant.
Results
Characteristics of the patients
This study examined a group of 217 patients (217 eyes) diagnosed with CRAO, consisting of 157 males and 60 females. The mean age of the participants was 57.8 ± 13.3 years (range, 18–83 years). All cases presented with unilateral occlusion, affecting 111 right eyes and 106 left eyes. The duration from onset to presentation was 57.0 ± 61.5 h (range, 4–168 h), which is close to the time window for arterial thrombolysis. Urokinase thrombolysis was performed immediately after the emergency ocular and systemic examinations upon admission. The patients were categorized based on severity into mild, moderate, severe, and extremely severe groups. Statistical analysis indicated no significant differences among the groups with regard to age (P = 0.209), affected eye (P = 0.610), or onset interval (P = 0.547). However, a significant difference was observed in sex distribution among the groups (P = 0.015) (Table 1).
Changes in visual acuity after treatment
Prior to treatment, visual acuity declined concurrently with the advancement of the condition. One week post-thrombolysis, the mean visual acuity improved from 2.4 ± 0.5 before treatment to 1.9 ± 0.7 (t = 13.485, P < 0.001). Among the 217 patients diagnosed with CRAO, 160 (73.3%) exhibited an improvement in visual acuity. In the mild group, all 28 patients (100%) demonstrated an enhancement in vision. Within the moderate group of 101 patients, 81 exhibited improvement, representing 80.2%. In the severe group, 29 out of 41 patients experienced enhancement, resulting in an improvement rate of 70.7%. In the extremely severe group, 22 out of 47 patients showed improvement, yielding an improvement rate of 46.8% (Table 2).
Changes in retinal thickness after treatment
As the condition progressed, there was a notable increase in macular retinal edema, which resulted in an enhancement of retinal thickness and a reduction in the resolution of retinal morphology observed in OCT images (all P < 0.001). One week following urokinase thrombolysis, subsequent OCT assessments demonstrated a decrease in macular retinal thickness from 415.5 ± 107.7 μm prior to treatment to 362.1 ± 93.8 μm (t = 9.095, P < 0.001). When compared to pre-treatment measurements, retinal thickness exhibited significant reductions across all groups (all P < 0.05) (Table 3).
Correlation between visual acuity and retinal thickness
In this study, Spearman correlation analysis was employed to examine the relationship among LogMAR visual acuity, baseline OCT severity grading, and macular retinal thickness as observed in OCT images. Prior to treatment, the LogMAR visual acuity was in positive correlation with that of both baseline OCT severity grading (correlation coefficient of r = 0.679, P < 0.001) and macular retinal thickness (correlation coefficient of r = 0.328, P < 0.001). Following treatment, the positive correlation between LogMAR visual acuity and macular retinal thickness was found to strengthen, as indicated by reduced retinal edema and increased visual acuity, yielding a correlation coefficient of r = 0.420, P < 0.001 (Fig. 2).

Scatter diagram showing the relationship between visual acuity and macular retinal thickness in CRAO patients. (A) Pre-treatment visual acuity positively correlates with macular retinal thickness (r = 0.328, P < 0.001). (B) Post-treatment visual acuity positively correlates with macular retinal thickness (r = 0.420, P < 0.001).
Inter-observer variability for OCT grading
An evaluation of inter-observer variability was conducted using Cohen’s Kappa to quantify the agreement between the observers. The Kappa value of 0.873 (P < 0.001) indicates a high level of agreement between the two experienced physicians in their classification of the 217 samples into four categories, reflecting a robust and reliable framework for the OCT grading process.
Discussion
The findings of this study indicate a correlation between LogMAR visual acuity and macular foveal retinal thickness in patients with CRAO, a correlation that is enhanced following urokinase thrombolysis. This observation suggests a relationship between visual function and macular edema in this patient population. Furthermore, OCT images reveal that patients exhibiting severe retinal structural damage demonstrate a reduced visual recovery post-urokinase thrombolysis compared to those with less structural impairment.
Ahn et al.15 reported an association between the degree of retinal edema and decreased visual acuity in CRAO patients, which aligns with our findings. Additionally, a previous study demonstrated that the presence of cilioretinal arteries, which are found in 7–50% of the population16, contributes to the treatment of ischemic damage and the reduction of edema17, thereby facilitating visual recovery. This further supports the hypothesis that urokinase thrombolytic therapy can ameliorate retinal edema, thus enhancing visual outcomes. Fouad et al.18 suggested that retinal edema in CRAO should be differentiated from that in diabetic retinopathy and should be conceptualized as retinal swelling rather than edema. Moreover, a small study involving 11 patients conducted by Chen et al.19 indicated that macular thickening is associated with edema and visual decline; however, a significant reduction in thickness one week post-CRAO suggests more severe damage, which also correlates with a decline in LogMAR visual acuity. The pathological manifestations of varying retinal nerve fiber thickness across different fundus regions reflect their differential tolerance to ischemic stress, resulting in varying degrees of edema and structural damage20. In OCT images, CRAO is characterized by thickening and edema of retinal layers in the macular and posterior pole regions, increased reflectivity, and widening of photoreceptor dark zones21. Post-treatment thinning of the macular fovea can enhance retinal function, thereby increasing the likelihood of visual recovery; however, excessive thinning may indicate retinal damage19. Studies suggest that anatomical and functional recovery of the macular region significantly affects short-term visual acuity, particularly in acute CRAO patients4. Consequently, the correlation between LogMAR visual acuity and retinal thickness is notably strengthened immediately after treatment. Furthermore, a higher correlation coefficient post-thrombolysis may indicate a better potential for visual recovery as macular foveal retinal thickness normalizes. Nevertheless, the relationship between retinal thickness and visual acuity post-CRAO necessitates further investigation. This study classified the severity of CRAO into extremely severe, severe, moderate, and mild categories. Results indicated significant differences in visual acuity based on the degree of structural damage caused by retinal edema. Visual acuity in the extremely severe and severe groups ranged from no light perception to counting fingers, corresponding to LogMAR scores of 2.3 to 3.0. Conversely, the moderate and mild groups exhibited visual acuity ranging from 0.01 to 1.0, corresponding to LogMAR scores of 1.0 to 1.8. Furashova et al.9 demonstrated that with increasing CRAO severity, the thickness of the inner and middle retinal layers increased, with no observable differences in the outer layer, although they did not investigate visual acuity. Nonetheless, based on the aforementioned results, we can hypothesize that greater retinal thickening is associated with poorer visual outcomes, thus supporting the conclusions drawn from this study.
There was no statistically significant difference in the arterial thrombolysis time window between the groups; however, there were statistically significant differences in visual acuity and retinal thickness. These results may be attributable to individual patient variability. Specifically, some patients experienced a brief onset time, yet tissue edema can escalate rapidly, resulting in considerable structural and functional impairment. In such instances, even with prompt thrombolysis, visual improvement may be limited. Conversely, severe edema may also arise from a prolonged, slow-progressing course, and these patients may exhibit a more favorable response to treatment. Unfortunately, the sample size was insufficient to perform a subgroup analysis based on onset time, which warrants further investigation in future studies. Nevertheless, patients with superior pre-treatment vision demonstrated significant enhancement in visual acuity following arterial thrombolysis, aligning with existing literature4,11. This finding emphasizes the crucial importance of early intervention and the timing of treatment in the recovery of visual function. For patients with early CRAO, effective thrombolytic therapy can optimize vision restoration while maintaining retinal function.
Considering the small caliber of the retinal artery and the inherent fragility of the retina, mechanical endovascular treatment is not a viable option for CRAO. In comparison to other contemporary treatments for CRAO, urokinase thrombolysis has emerged as a safe and effective intervention, offering substantial benefits to patients11. Prompt intervention has the potential to markedly enhance visual prognosis, particularly for patients with early-stage CRAO whose retinal ganglion cells have not yet undergone significant degeneration22,23. Among a cohort of 217 CRAO patients, 160 (73.7%) exhibited improvements in visual acuity. This outcome is consistent with existing literature, which underscores the potential of arterial thrombolysis to facilitate visual recovery and improve overall visual function in cases of CRAO4. The high success rate of thrombolysis may be attributable to thorough pre-treatment evaluations and meticulous patient selection, as well as the accurate administration of thrombolysis via catheter-based interventions and imaging guidance. Timely, localized thrombolytic therapy can rapidly and effectively dissolve obstructive thrombi, restore retinal blood flow, enhance retinal ganglion cell functionality, and significantly elevate the rate of visual recovery.
Analysis based on severity classification indicated a 100% improvement rate within the mild group. This outcome may be attributed to the relatively undamaged state of retinal ganglion cells in this group, which enhances their likelihood of benefiting from prompt restoration of blood flow. The moderate obstruction group exhibited an improvement rate of 80.2%, suggesting that even moderate obstructions can yield significant improvements with early intervention. In contrast, the severe and extremely severe groups demonstrated lower improvement rates of 70.7% and 46.8%, respectively, indicating that the progression of the disease may diminish treatment responsiveness due to the extent of retinal damage. Previous studies corroborate that when retinal structural integrity is severely compromised, the potential for vision recovery becomes constrained3,11. These findings suggest that urokinase thrombolysis may alleviate retinal edema irrespective of the initial severity of CRAO. Notably, in the mild and moderate groups, where retinal structure was not severely compromised, the reduction in retinal thickness was more pronounced. Conversely, while the severe and extremely severe groups also exhibited thinning, they encountered greater functional impairment. Urokinase thrombolysis has been shown to reduce macular foveal retinal thickness in patients with CRAO and markedly promotes improvements in retinal structure. However, further validation, including the incorporation of a control group in future studies, is necessary to establish a more robust cause-effect relationship. It is important to note that retinal layer atrophy naturally occurs after CRAO, and spontaneous improvement in visual acuity can also take place in untreated patients. Future research should prioritize the investigation of the impact of this treatment strategy on retinal cell function, long-term prognosis, and its synergistic effects when combined with other therapeutic modalities, thereby contributing to a more comprehensive approach to the management of CRAO.
This study has several limitations. First, the patient population was derived from a single hospital, and the small sample size may have introduced biases associated with local practices and policies. Furthermore, the sample size was insufficient to conduct subgroup analyses (e.g., based on time to onset). The study employed a retrospective design, with data restricted to what was documented in the medical records. Given the relatively small sample size, limited clinical data, and unequal group distributions, only correlation analyses were feasible, precluding the implementation of reliable multivariate analyses. Finally, this study protocol did not include perfusion analysis via FFA or OCTA. Consequently, the observed visual acuity improvement was attributed to urokinase thrombolysis treatment, without considering adaptive macular mechanisms, such as collateral perfusion. Further research is necessary, preferably involving large-scale, multicenter studies with longer-term follow-up, to assess visual outcomes, complications, and recurrence rates over extended periods, as well as to conduct perfusion analyses that can elucidate these adaptive macular mechanisms.
In conclusion, the findings of this study provide evidence of a correlation between visual recovery and structural changes observed in OCT images of patients with CRAO. Furthermore, the research demonstrates that visual acuity can improve in CRAO patients, particularly those presenting with mild to moderate conditions, following urokinase treatment. Importantly, the correlation between visual acuity and retinal thickness becomes more pronounced after urokinase thrombolysis. In patients with severe and extremely severe conditions, while some improvement was noted, the potential for visual recovery appears to be constrained by the duration of the occlusion and the extent of retinal damage. These findings indicate that clinical decisions regarding urokinase thrombolysis should take into account the severity of the condition and its associated prognosis in order to facilitate the implementation of individualized treatment plans. Ultimately, these results and conclusions necessitate further clinical trials for validation.
Data availability
All data generated or analysed during this study are included in this published article.
References
Liu, W., Bai, D. & Kou, L. Progress in central retinal artery occlusion: A narrative review. J. Int. Med. Res. 51, 3000605231198388 (2023).
Scott, I. U., Campochiaro, P. A., Newman, N. J. & Biousse V. Retinal vascular occlusions. Lancet 396, 1927–1940 (2020).
Mac Grory, B. et al. Management of central retinal artery occlusion: A scientific statement from the American Heart Association. Stroke 52, e282–e294 (2021).
Chen, C., Singh, G., Madike, R. & Cugati, S. Central retinal artery occlusion: A stroke of the eye. Eye 38, 2319–2326 (2024).
Hayreh, S. S. & Zimmerman, M. B. Central retinal artery occlusion: Visual outcome. Am. J. Ophthalmol. 140, 376–391 (2005).
Kim, H., Kim, H. K., Yang, J. Y. & Kim, S. S. Optical coherence tomography measurement and visual outcome in acute central retinal artery occlusion. Korean J. Ophthalmol. 32, 303–311 (2018).
Littlewood, R., Mollan, S. P., Pepper, I. M. & Hickman, S. J. The utility of fundus fluorescein angiography in neuro-ophthalmology. Neuroophthalmology 43, 217–234 (2019).
Zeppieri, M. et al. Optical coherence tomography (OCT): A brief look at the uses and technological evolution of ophthalmology. Medicina 59 (2023).
Furashova, O. & Matthe, E. Retinal changes in different grades of retinal artery occlusion: An optical coherence tomography study. Invest. Ophthalmol. Vis. Sci. 58, 5209–5216 (2017).
Kim, Y. H., Park, K. H. & Woo, S. J. Clinical manifestations and visual prognosis of cilioretinal artery sparing central retinal artery occlusion. Korean J. Ophthalmol. 34, 27–34 (2020).
Mac Grory, B., Lavin, P., Kirshner, H. & Schrag, M. Thrombolytic therapy for acute central retinal artery occlusion. Stroke 51, 687–695 (2020).
Wang, R. et al. Evaluation of ophthalmic artery branch retrograde intervention in the treatment of central retinal artery occlusion (CRAO). Med. Sci. Monit. 23, 114–120 (2017).
Lambert, S. R. et al. Long-term effect of intraocular Lens vs contact Lens correction on visual acuity after cataract surgery during infancy: A randomized clinical trial. JAMA Ophthalmol. 138, 365–372 (2020).
Chen, H., Xia, H., Qiu, Z., Chen, W. & Chen, X. Correlation of optical intensity on optical coherence tomography and visual outcome in central retinal artery occlusion. Retina 36, 1964–1970 (2016).
Ahn, S. J. et al. Retinal and choroidal changes and visual outcome in central retinal artery occlusion: An optical coherence tomography study. Am. J. Ophthalmol. 159, 667–676 (2015).
Schneider, M. et al. Prevalence of cilioretinal arteries: A systematic review and a prospective cross-sectional observational study. Acta Ophthalmol. 99, e310–e318 (2021).
Brown, G. C. & Shields, J. A. Cilioretinal arteries and retinal arterial occlusion. Arch. Ophthalmol. 97, 84–92 (1979).
Fouad, Y. A., Hamza, M. N. & Wessam, M. M. Prevalence and distribution of macular fluid with central retinal artery occlusion and anterior ischemic optic neuropathy. Clin. Ophthalmol. 18, 887–893 (2024).
Chen, S. N., Hwang, J. F. & Chen, Y. T. Macular thickness measurements in central retinal artery occlusion by optical coherence tomography. Retina 31, 730–737 (2011).
Sood, G., Samanta, R., Kumawat, D., Agrawal, A. & Singh, A. Clinical profile and retinal nerve fibre layer thickness of optic disc oedema patients at a tertiary care Institute in North India. Ther. Adv. Ophthalmol. 14, 25158414211072634 (2022).
Mangla, R. et al. Retinal OCT findings in acute central retinal artery occlusion of varying severity at different disease stages—a retrospective, observational study. Int. J. Retina Vitreous 9, 37 (2023).
Li, X. et al. Improved visual outcomes of central retinal artery occlusion with local intra-arterial fibrinolysis beyond the conventional time window. J. Thromb. Thrombolysis 57, 503–511 (2024).
Donaldson, L., Nicholson, P. & Margolin, E. Visual recovery in 2 cases of central retinal artery occlusion treated with prompt Intra-ophthalmic artery fibrinolysis. J. Neuroophthalmol. 43, 383–386 (2023).
Funding
This work was supported by the Shaanxi Science and Technology Project under Grant No. 2021SF-154, and Xi’an Science and Technology Project under Grant No. 21YXYJ0043. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
W.W. drafted and critically revised the manuscript. T.L. and R.W. participated in collecting and analyzing data. B.Z., X.W., and T.M. contributed to acquisition and interpretation of data. R.W. critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Xi’an People’s Hospital (Xi’an Fourth Hospital) (No.20220005). Given the retrospective nature of the investigation, the committee waived the necessity for individual informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, W., Lei, T., Wang, R. et al. Correlation of visual acuity changes and optical coherence tomography imaging in patients with central retinal artery occlusion post-arterial thrombolysis. Sci Rep 15, 7962 (2025). https://doi.org/10.1038/s41598-025-92890-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92890-0
