
Abstract
Social isolation is common and associated with many adverse outcomes. The evidence regarding social isolation and mortality among middle-aged and older adults with arthritis was lacking. The study aimed to examine the association between social isolation and mortality in this population. This study used data from four prospective cohorts: National Health and Aging Trends Study (NHATS), English Longitudinal Study of Ageing (ELSA), China Health and Retirement Longitudinal Study (CHARLS), and Chinese Longitudinal Healthy Longevity Survey (CLHLS). Individuals with arthritis (including osteoarthritis and rheumatoid arthritis) in these cohorts were included. Social isolation was assessed using self-reported questionnaires. Cox proportional hazards regression models were conducted to evaluate these associations. At baseline, a total of 16,035 individuals with arthritis (3872 from NHATS, 3259 from ELSA, 5645 CHARLS, and 3259 from CLHLS) were included. Social isolation was associated with increased risk of mortality in meta-analysis (hazard ratio [HR] 1.42, 95% confidence interval [CI]: 1.26–1.59), and individual cohorts (NHATS: HR 1.53, 95% CI 1.19–1.97; ELSA: HR 1.31, 95% CI 1.02–1.67; CLHLS: HR 1.50, 95% CI 1.36–1.64) after being adjusted for confounder factors. Additionally, with increasing social isolation score, the risk of mortality also increased in meta-analysis (HR 1.19, 95% CI 1.15–1.24), as well as in individual cohorts (NHATS: HR 1.22, 95% CI 1.14–1.30; CLHLS: HR 1.19, 95% CI 1.13–1.26). Subgroups analysis results suggested that social isolation was independently associated with a higher likelihood of mortality in middle-aged and older adults with arthritis, regardless of gender, lifestyles, and chronic diseases.
Similar content being viewed by others

Introduction
Arthritis is a common condition characterized by inflammation, pain, stiffness, and reduced mobility of the joints. Previous studies have shown that psychopathological symptoms, personality traits, and environmental factors play a crucial role in the progression of arthritis1,2,3. Among these modifiable factors, social isolation stands out as a particularly noteworthy aspect. Social isolation, characterized by lack of sufficient social contact and interaction with others, may exacerbate the risk or progression of certain diseases by affecting individuals’ psychological states and lifestyle4,5. The global prevalence of social isolation was approximately 25% (95% confidence interval [CI]: 21.0–30.0) among community-dwelling older adults6. More importantly, several studies have demonstrated significant association between social isolation and increased risk of mortality in the general and disease-specific populations7,8,9. However, the evidence that whether social isolation is associated with mortality among individuals with arthritis is still lacking, no studies are conducted to investigate the potential association at present.
In this study, we hypothesized that social isolation may be associated with increased risk of mortality among individuals with arthritis. To test this hypothesis, we examined the potential association between social isolation and mortality among people with arthritis using data from four prospective population-based cohorts: the National Health and Aging Trends Study (NHATS), the English Longitudinal Study of Ageing (ELSA), the China Health and Retirement Longitudinal Study (CHARLS), and the Chinese Longitudinal Healthy Longevity Survey (CLHLS).
Methods
Study design and population
Four prospective cohort were used in this study, including the National Health and Aging Trends Study (NHATS), English Longitudinal Study of Ageing (ELSA), China Health and Retirement Longitudinal Study (CHARLS) and Chinese Longitudinal Healthy Longevity Survey (CLHLS).
NHATS is a longitudinal study focusing on the health and aging trends of older Americans10. It aims to provide comprehensive data on the health, functional status, and well-being of older adults in the United States. Data were collected annually from 2011 (Round 1). In this study, we used data from Round 1 (2011) to Round 8 (2018). At baseline (Round 1), a total of 8245 individuals were recruited. The diagnosis of arthritis was based on self-report at baseline (“Please tell me if a doctor ever told you that you had arthritis (including osteoarthritis or rheumatoid arthritis)”). The follow-up period ranged from 2011 to 2018. The median follow-up time is 5.34 ± 2.49 years. Among them, 4248 individuals were diagnosed as arthritis. Additionally, 376 individuals were excluded due to lacking data on social isolation. Finally, 3872 individuals with arthritis were included in this cohort.
ELSA is a longitudinal study designed to explore various aspects of aging in England. It collects data on individuals aged 50 and over to understand the physical, mental, and social changes associated with aging11. The diagnosis of arthritis was based on self-report at baseline (“Have you been diagnosed with arthritis (including osteoarthritis, or rheumatism) by a doctor?”). The follow-up period ranged from 2002 to 2012. The median follow-up time is 7.64 ± 3.15 years. At baseline, 12,099 individuals from the database were included. We excluded participants who did not have arthritis or lacked data on arthritis (N = 8,289). In addition, participants who lacked data on social isolation (N = 526) and mortality (N = 25) were also excluded. Finally, 3259 individuals were included in the final sample.
CHARLS is a nationally representative longitudinal survey of Chinese residents aged 45 and older. It aims to collect data on health, economic status, social networks, and family structures of the middle-aged and elderly population in China12. The diagnosis of arthritis was based on self-report at baseline (“Have you been diagnosed with arthritis or rheumatism by a doctor?”). In the first stage, there were 17,596 participants from the database included in the screening process. The follow-up period ranged from 2011 to 2020. The median follow-up time is 8.22 ± 1.80 years. We excluded participants who did not have arthritis or lacked data on arthritis (N = 11823). In addition, participants who lacked data on social isolation (N = 115) and mortality (N = 13) were also excluded. The final sample had 5645 individuals with arthritis.
CLHLS is a longitudinal study of Chinese adults aged 65 and older, focused on healthy longevity, family dynamics, and living arrangements13. The diagnosis of arthritis was based on self-report at baseline (“Do you currently suffer from arthritis?”). There were 16,064 individuals were included at the first stage. The follow-up period ranged from 2002 to 2018. The median follow-up time is 5.34 ± 4.63 years. After exclusion of participants who did not have arthritis or lacked data on arthritis (N = 12,211). In addition, participants who lacked data on social isolation (N = 343) and mortality (N = 251) were also excluded. The final sample had 3259 individuals with arthritis.
Assessment of social isolation
In the NHATS, social isolation was assessed by four domains: living arrangement, core discussion network size, religious attendance, and social participation14. If any aspect is not met, a score of 1 point is given. Individuals who had a sum score of three or more were classified as social isolation, and those with less than three were classified as normal14. Based on previous research, the definition of social isolation in the ELSA, CHARLS and CLHLS was established15,16,17. Participants received 1 point for each of the following: unmarried (including separated, divorced, widowed, or never married), had less contact with their children per week (by phone, in person, or by email), and had not participated in any social activities in the past month (including interacting with friends, playing chess or cards, participating in sports, social, or other clubs). The social isolation index is scored on a scale of 0 to 3, with higher scores indicating higher levels of social isolation. Participants who scored ≥ 1 were assigned to the social isolation group.
Assessment of outcomes
The primary outcome for this study was mortality among individuals with arthritis. In NHATS and CLHLS, the time of death was determined based on the recorded date of death from the follow-up assessments. In ELSA and CHARLS, the time of death was based on the last follow-up date on which death was confirmed.
Assessment of covariates
The covariates included age, gender, marital status, smoking status, body mass index (BMI), education, vigorous exercise, depression status, and number of chronic diseases18,19,20. For consistency among the NHATS, ELSA, CHARLS, and CLHLS, gender was divided into man and woman, marital status was divided into two categories: married or partnered and single or widowed. Smoking status was categorized as never smokers and ever smokers. BMI was computed as kg/m2 based on self-reported height and weight in NHATS, ELSA, CHARLS and CLHLS. In CLHLS, height was estimated according to knee height (in cm) with a validated equation for participants as follows: body height for men = 2.01 × knee height + 67.78, body height for women = 1.81 × knee height + 74.0821. For NHATS, ELSA, and CHARLS, the educational levels were categorized as Less than High School (level 1), High School (level 2), and More than High School (level 3). For CLHLS, the educational level was designated as School Years, which is further classified into three levels: 0 years (level 1), 1 to 6 years (level 2), and more than 6 years (level 3). Vigorous exercise was divided into those engaging in vigorous exercise and those not. In ELSA and CHARLS, depressive symptoms are assessed using the Centre for Epidemiologic Studies Depression Scale (CES-D). In NHATS and CLHLS, depressive symptoms are determined using customized questionnaires. Chronic diseases in all cohorts included the following major diseases: heart disease, cerebrovascular disease, cancer, and diabetes.
Statistical analysis
First, we described the data by the mean with standard deviation (SD) or frequency (%) based on continuous and categorical variables, respectively. Second, we utilized Cox proportional hazard models to estimate the HR of mortality associated with social isolation and score. Two models were conducted: Model 1 was unadjusted; Model 2 was adjusted for age, gender, BMI (excluded ELSA), educational level, smoking status, vigorous exercise, depression status and number of chronic diseases. Meta-analysis was conducted using random-effects models to estimate the association between mortality and social isolation, as well as a specific score. Missing data for covariates were managed using median imputation techniques. The normal group (non-social isolation) was as reference. Third, a sensitivity analysis was conducted by excluding individuals who died within the first year to address potential reverse causation. Finally, re-analyses were conducted to examine the association of social isolation with mortality in stratified subgroups. The subgroups included gender (male vs. female), smoking status (never vs. ever), vigorous exercise (yes vs. no), number of chronic disease (0–1 vs. 2–3 vs. >3). The heterogeneity between subgroups was assessed based on meta-regression analysis. All results were considered significant at a P-value < 0.05 (2-tailed). All analyses were conducted using R statistical software (version 4.2.1; www.r-project.org).
Results
Baseline characteristics of the study
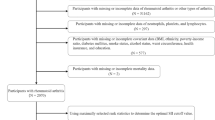
Figure 1 showed the selection process of the study population. In this study, a total of 16035 individuals with arthritis were included. Of them, 3872 participants were from NHATS (male: 34.35%, mean age: 77.74 years), 3259 from ELSA (male: 34.83%, mean age: 66.94 years), 5645 CHARLS (male: 42.09%, mean age: 59.96 years), and 3259 from CLHLS (male: 40.17%, mean age: 85.29 years) were included. At baseline, 3429 individuals from NHATS, 2127 from ELSA, 3400 from CHARLS, and 2029 from CLHLS were defined as social isolation, respectively. The detail characteristics of participants from the four cohorts were presented in Table 1.

Selection process of the study population. NHATS, National Health and Aging Trends Study; ELSA, English Longitudinal Study of Ageing; CHARLS, China Health and Retirement Longitudinal Study; CLHLS, Study Chinese Longitudinal Healthy Longevity Survey.
Association between social isolation and the risk of mortality
Figure 2 showed the association between social isolation and the risk of mortality. Compared with normal individuals, those with social isolation had higher risk of mortality in meta-analysis (HR 1.42, 95% CI 1.26–1.59) and the individual cohorts, including NHATS (HR 1.53, 95% CI 1.19–1.97), ELSA (HR 1.31, 95% CI 1.02–1.67), and CLHLS (HR 1.50, 95% CI 1.36–1.64) after adjusted age, gender, BMI (excluded ELSA), educational level, smoking status, vigorous exercise, depression status, and number of chronic diseases. With increasing social isolation sFig. (Fig. 3), the risk of mortality also increased in meta-analysis (HR 1.19, 95% CI 1.15–1.24), as well as in individual cohorts, including NHATS (HR 1.22, 95% CI 1.14–1.30) and CLHLS (HR 1.19, 95% CI 1.13–1.26). Additionally, those with highest social isolation score (≥ 3) had higher risk of mortality (Table 2) in NHATS (HR 1.87, 95% CI 1.43–2.44), CHARLS (HR 1.99, 95% CI 1.05–3.78), CLHLS (HR 1.44, 95% CI 1.18–1.75), but not in ELSA (HR 1.32, 95% CI 0.79–2.20).

Meta-analyses for the association between social isolation and the risk of mortality in individuals with arthritis. Model 1, unadjusted; Model 2, all databases were adjusted for age, gender, BMI (excluded ELSA), educational level, smoking status, vigorous exercise, depression status, and number of chronic diseases.

Meta-analyses for association between social isolation score and the risk of mortality in individuals with arthritis. Model 1, unadjusted; Model 2, all databases were adjusted for age, gender, BMI (excluded ELSA), educational level, smoking status, vigorous exercise, depression status and number of chronic diseases.
Sensitivity analysis by excluding individuals who died within the first year
A sensitivity analysis by excluding individuals who died within the first year after the baseline measurement. Supplementary Fig. S1 showed that compared with individuals without social isolation, those with social isolation had higher risk of mortality in meta-analysis (HR 1.30, 95% CI 1.16–1.45) after being adjusted for age, gender, BMI (excluded ELSA), educational level, smoking status, vigorous exercise, depression status, and number of chronic diseases. Additionally, as the social isolation score increased, the risk of mortality also increased in meta-analysis (HR 1.16, 95% CI 1.09–1.23) (Supplementary Fig. S2).
Subgroups analyses for the association of social isolation with the risk of mortality
We also conducted stratified analyses across various strata defined by gender, smoking vigorous exercise, and number of chronic diseases (Fig. 4). We found significant associations of social isolation with risk of mortality in each stratum in the four cohorts, and the interaction tests comparing the HRs across the strata were not significant (P-value > 0.05), suggesting that arthritis individuals with social isolation had significantly higher risks of mortality than those normal individuals, regardless of gender, lifestyles, and chronic diseases.

Association of social isolation with the risk of mortality in subgroups. All databases were adjusted for age, gender, BMI (excluded ELSA), educational level, smoking status, vigorous exercise, depression status, and number of chronic diseases. P-int represents the heterogeneity between subgroups based on the meta-regression analysis.
Discussion
In this study, we examined the association between social isolation and the risk of mortality among individuals with arthritis using data from four prospective cohort studies. We found that social isolation was associated with increased risks of mortality among individuals with arthritis, independent of socioeconomic status, lifestyles, and chronic diseases. It is the first large-scale, multi-cohort study to specifically investigate this relationship in arthritis patients. By systematically analyzing data from these population-based cohorts, we have provided new insights into the impact of social isolation on the prognosis of arthritis.
Although our study was first to examine the relationship between social isolation and mortality in individuals with arthritis, recent studies have investigated the association among in the general and other disease-specific populations7,8,9. For example, Wang et al. conducted a systematic review and meta-analysis of 90 cohort studies involving 2,205,199 individuals7. They found that social isolation and loneliness were significantly associated with an increased risk of all-cause mortality (HR 1.32, 95% CI 1.26–1.39), and cancer mortality (HR 1.24, 95% CI 1.19–1.28). Social isolation also increased the risk of cardiovascular mortality (HR 1.34, 95% CI 1.25–1.44). There was an increased risk of all-cause mortality in socially isolated individuals with cardiovascular (HR 1.28, 95% CI 1.10–1.48) or breast cancer (HR 1.51, 95% CI 1.34–1.70)7. In our study, we further provided evidence that social isolation was associated with mortality in individuals with arthritis using data from four prospective population-based cohorts.
The potential explanations by which social isolation increases the risk of mortality in arthritis patients may be multifaceted. Arthritis is characterized by chronic inflammation, and previous studies have shown that social isolation is associated with elevated levels of systemic inflammation22,23,24, exacerbating the inflammatory response and deteriorating arthritis patients’ health, and then lead to mortality in arthritis25,26,27. Social isolation is linked to unhealthy behaviors, such as irregular eating habits and lack of physical activity, which further increase mortality risk28,29,30. Additionally, social isolation was associated with increased risk of severe major diseases, such as stroke, coronary heart disease, and dementia31,32,33. As we known, these diseases were all the leading causes of mortality34. In summary, social isolation would increase mortality risk in individuals with arthritis through additive inflammation levels, unhealthy behaviors and major diseases.
This study has several strengths. It is the first to use data from four large population-based cohorts from different countries, enhancing the credibility of the findings. The diversity of data sources and the wide coverage increase the generalizability and applicability of our conclusions. However, our study also has some limitations. First, while the population in the CLHLS cohort may overlap with that of the CHARLS cohort, we did not have explicit individual-level data to identify and eliminate any overlap, which could lead to duplication and falsely increase the precision of the analysis. Besides, as an observational study, we cannot establish causal relationships but can only observe associations between social isolation and mortality risk. Several large-scale studies, including those based on the NHANES dataset, have demonstrated the feasibility and reliability of self-reported RA diagnoses in epidemiological research35,36. However, recall bias may exist since data collection relied on self-reports from participants. Furthermore, our analysis was based only on baseline data and did not account for changes over time, which may affect the accuracy of the results. Future research should consider longitudinal data to better understand the dynamic process of how social isolation impacts the health of arthritis patients.
The clinical implication of this study underscores the role of social isolation as a significant risk factor for increased mortality in arthritis patients, suggesting that healthcare providers incorporate social support assessments and interventions into treatment to improve patient outcomes and quality of life. From a research perspective, the study highlights the need for further exploration into how social isolation influences arthritis progression through mechanisms like immune system dysfunction and chronic inflammation. Longitudinal studies will help clarify causal relationships. From the perspective of community health, addressing arthritis and social isolation is crucial for reducing chronic disease burdens and improving community well-being. Arthritis affects mobility and quality of life, while social isolation worsens its impact, leading to poorer health outcomes. By enhancing arthritis management and reducing isolation, communities can lower healthcare costs, improve mental and physical health, and foster social cohesion. These efforts support targeted health interventions and policies, ensuring better resource allocation and promoting long-term population health.
Conclusions
Overall, this study systematically reveals, for the first time, the association between social isolation and increased risk of mortality in individuals with arthritis. This finding underscores the importance of social isolation in chronic disease management, particularly for arthritis patients. Further study should explore the causal relationship between social isolation and arthritis prognosis and consider temporal changes to better understand and intervene in this risk factor.
Data availability
The datasets analyzed in NHATS are publicly available after registration at https://www.nhats.org/researcher. ELSA datasets analyzed are publicly available after registration at https://www.elsa-project.ac.uk/. CHARLS datasets analyzed are publicly available after registration at http://charls.pku.edu.cn/. CLHLS datasets analyzed are publicly available after registration at https://opendata.pku.edu.cn/dataset.xhtml? persistentId=doi:10.18170/DVN/WBO7LK&version=2.0.
Abbreviations
- NHATS:
-
National Health and Aging Trends Study
- ELSA:
-
English Longitudinal Study of Ageing
- CHARLS:
-
China Health and Retirement Longitudinal Study
- CLHLS:
-
Chinese Longitudinal Healthy Longevity Survey
- BMI:
-
Body mass index
- SD:
-
Standard deviation
- HR:
-
Hazard ratio
- CI:
-
Confidence interval.
References
Li, C., Liu, T., Sun, W., Wu, L. & Zou, Z. Y. Prevalence and risk factors of arthritis in a middle-aged and older Chinese population: The China health and retirement longitudinal study. Rheumatol. (Oxford England) 54, 697–706. https://doi.org/10.1093/rheumatology/keu391 (2015).
Cao, Z., Li, Q., Li, Y. & Wu, J. Causal association of leisure sedentary behavior with arthritis: A Mendelian randomization analysis. Semin. Arthritis Rheum. 59, 152171. https://doi.org/10.1016/j.semarthrit.2023.152171 (2023).
Deng, Y. et al. Indoor solid fuel use and incident arthritis among middle-aged and older adults in rural China: A nationwide population-based cohort study. Sci. Total Environ. 772, 145395. https://doi.org/10.1016/j.scitotenv.2021.145395 (2021).
Umberson, D. & Montez, J. K. Social relationships and health: A flashpoint for health policy. J. Health Soc. Behav. 51 Suppl, 54–66. https://doi.org/10.1177/0022146510383501 (2010).
Social Networks, H., Resistance & mortality A nine-year follow-up study of Alameda County residents. Am. J. Epidemiol. 185, 1070–1088. https://doi.org/10.1093/aje/kwx103 (2017).
Teo, R. H., Cheng, W. H., Cheng, L. J., Lau, Y. & Lau, S. T. Global prevalence of social isolation among community-dwelling older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 107, 104904. https://doi.org/10.1016/j.archger.2022.104904 (2023).
Wang, F. et al. A systematic review and meta-analysis of 90 cohort studies of social isolation, loneliness and mortality. Nat. Hum. Behav. 7, 1307–1319. https://doi.org/10.1038/s41562-023-01617-6 (2023).
Long, R. M. et al. Social isolation, and living alone associations with mortality risk in individuals living with cardiovascular disease: A systematic review, Meta-Analysis, and Meta-Regression. Psychosom. Med. 85, 8–17. https://doi.org/10.1097/psy.0000000000001151 (2023). Loneliness.
Zhou, J. et al. Improvement of social isolation and loneliness and excess mortality risk in people with obesity. JAMA Netw. Open. 7 (e2352824). https://doi.org/10.1001/jamanetworkopen.2023.52824 (2024).
Freedman, V. A. & Kasper, J. D. Cohort profile: The National health and aging trends study (NHATS). Int. J. Epidemiol. 48, 1044–1045g. https://doi.org/10.1093/ije/dyz109 (2019).
Steptoe, A., Breeze, E., Banks, J. & Nazroo, J. Cohort profile: The english longitudinal study of ageing. Int. J. Epidemiol. 42, 1640–1648. https://doi.org/10.1093/ije/dys168 (2013).
Zhao, Y., Hu, Y., Smith, J. P., Strauss, J. & Yang, G. Cohort profile: The China health and retirement longitudinal study (CHARLS). Int. J. Epidemiol. 43, 61–68. https://doi.org/10.1093/ije/dys203 (2014).
Zeng, Y. Towards deeper research and better policy for healthy aging --Using the unique data of Chinese longitudinal healthy longevity survey. China Economic J. 5, 131–149. https://doi.org/10.1080/17538963.2013.764677 (2012).
Cudjoe, T. K. M. et al. The epidemiology of social isolation: National health and aging trends study. J. Gerontol. B 75, 107–113. https://doi.org/10.1093/geronb/gby037 (2020).
Song, Y. et al. Social isolation, loneliness, and incident type 2 diabetes mellitus: Results from two large prospective cohorts in Europe and East Asia and Mendelian randomization. EClinicalMedicine 64, 102236. https://doi.org/10.1016/j.eclinm.2023.102236 (2023).
Ikeda, T. et al. Association between social isolation and smoking in Japan and England. J. Epidemiol. 31, 523–529. https://doi.org/10.2188/jea.JE20200138 (2021).
Pan, C. & Cao, N. Patterns of social isolation and low social support and frailty trajectories among Chinese older adults. J. Appl. Gerontol. 42, 2325–2334. https://doi.org/10.1177/07334648231194508 (2023).
Chen, Z. et al. Dietary protein intake and all-cause and cause-specific mortality: Results from the Rotterdam study and a meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 35, 411–429. https://doi.org/10.1007/s10654-020-00607-6 (2020).
Zhang, X. et al. Body Roundness Index and All-Cause Mortality Among US Adults. JAMA Netw. Open 7, e2415051 (2024). https://doi.org/10.1001/jamanetworkopen.2024.15051
Svensson, T. et al. Association of sleep duration with All- and Major-Cause mortality among adults in Japan, China, Singapore, and Korea. JAMA Netw. Open. 4, e2122837. https://doi.org/10.1001/jamanetworkopen.2021.22837 (2021).
Zhang, H., Hsu-Hage, B. H. & Wahlqvist, M. L. The use of knee height to estimate maximum stature in elderly Chinese. J. Nutr. Health Aging 2, 84–87 (1998).
Koh-Bell, A., Chan, J., Mann, A. K. & Kapp, D. S. Social isolation, inflammation, and cancer mortality from the National health and nutrition examination Survey - a study of 3,360 women. BMC Public. Health 21, 1289. https://doi.org/10.1186/s12889-021-11352-0 (2021).
Matthews, T. et al. Social isolation, loneliness, and inflammation: A multi-cohort investigation in early and mid-adulthood. Brain Behav. Immun. 115, 727–736. https://doi.org/10.1016/j.bbi.2023.11.022 (2024).
Cudjoe, T. K. M. et al. Getting under the skin: Social isolation and biological markers in the National health and aging trends study. J. Am. Geriatr. Soc. 70, 408–414. https://doi.org/10.1111/jgs.17518 (2022).
Videm, V., Liff, M. H. & Hoff, M. Relative importance of inflammation and cardiorespiratory fitness for all-cause mortality risk in persons with rheumatoid arthritis: The population-based Trøndelag Health Study. RMD open 9 (2023). https://doi.org/10.1136/rmdopen-2023-003194
Videm, V., Houge, I. S., Liff, M. H. & Hoff, M. Inflammation mediates approximately one quarter of excess relative all-cause mortality in persons with rheumatoid arthritis: The Trøndelag health study. Sci. Rep. 12, 18599. https://doi.org/10.1038/s41598-022-21977-9 (2022).
Sha, S., Gwenzi, T., Chen, L. J., Brenner, H. & Schöttker, B. About the associations of vitamin D deficiency and biomarkers of systemic inflammatory response with all-cause and cause-specific mortality in a general population sample of almost 400,000 UK biobank participants. Eur. J. Epidemiol. 38, 957–971. https://doi.org/10.1007/s10654-023-01023-2 (2023).
Luo, J. & Hendryx, M. Mediation analysis of social isolation and mortality by health behaviors. Prev. Med. 154, 106881. https://doi.org/10.1016/j.ypmed.2021.106881 (2022).
Delerue Matos, A., Barbosa, F., Cunha, C., Voss, G. & Correia, F. Social isolation, physical inactivity and inadequate diet among European middle-aged and older adults. BMC Public. Health 21, 924. https://doi.org/10.1186/s12889-021-10956-w (2021).
Zhang, Y. B. et al. Combined lifestyle factors, all-cause mortality and cardiovascular disease: A systematic review and meta-analysis of prospective cohort studies. J. Epidemiol. Commun. Health 75, 92–99. https://doi.org/10.1136/jech-2020-214050 (2021).
Smith, R. W. et al. Social isolation and risk of heart disease and stroke: analysis of two large UK prospective studies. The Lancet. Public health 6, e232-e239 (2021). https://doi.org/10.1016/s2468-2667(20)30291-7
Liang, Y. Y. et al. Association of social isolation and loneliness with incident heart failure in a population-based cohort study. JACC Heart Fail. 11, 334–344. https://doi.org/10.1016/j.jchf.2022.11.028 (2023).
Shen, C. et al. Associations of social isolation and loneliness with later dementia. Neurology 99, e164–e175. https://doi.org/10.1212/wnl.0000000000200583 (2022).
Global burden of 288 causes of death and life expectancy decomposition. In 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet (London England). 403, 2100–2132. https://doi.org/10.1016/s0140-6736(24)00367-2 (2024).
Chen, L. et al. Associations between biological ageing and the risk of, genetic susceptibility to, and life expectancy associated with rheumatoid arthritis: A secondary analysis of two observational studies. Lancet Healthy Longev. 5, e45–e55. https://doi.org/10.1016/S2666-7568(23)00220-9 (2024).
Kadier, K. et al. Rheumatoid arthritis increases the risk of heart failure: Results from the cross-sectional study in the US population and Mendelian randomization analysis in the European population. Front. Immunol. 15, 1377432. https://doi.org/10.3389/fimmu.2024.1377432 (2024).
Acknowledgements
The data and samples used for this research were obtained from the NHATS, ELSA, CHARLS and CLHLS. We would like to thank the workers, researchers, and participants involved in the NHATS, ELSA, CHARLS and CLHLS.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 82102199, 82303562), the Pudong New Area Clinical Plateau Discipline Project (No. PWYgy2021-03), the general program of Shanghai Municipal Commission of Health and Family Planning (No. 202040479), Shanghai Municipal Commission of Science and Technology (No. 23YF1458200), and Hubei Provincial Natural Science Foundation of China (No. 2023AFB759).
Author information
Authors and Affiliations
Contributions
C.M. wrote the draft of manuscript and prepared Fig. 1. S.H. and H.Z. conducted the analyses and prepared Figs. 2, 3 and 4. J.L., W. X., Z.Z., H.Z. verified the underlying data and conducted a technical review. All authors contributed to the interpretation of the results and revision of the manuscript and accepted responsibility to submit for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The NHATS project was approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board, the ELSA project by the National Research and Ethics Committee of the UK National Health Service, the CHARLS project by the Biomedical Ethics Review Committee at Peking University, and the CHILIS project by the Research Ethics Committees of Duke University and Peking University. Participants in all projects provided written informed consent for the use of their data in research.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ma, C., He, S., Luo, J. et al. Social isolation and risk of mortality in middle-aged and older adults with arthritis: a prospective cohort study of four cohorts. Sci Rep 15, 8073 (2025). https://doi.org/10.1038/s41598-025-93030-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-93030-4
