
Abstract
The association between constipation and suicidal ideation remains inadequately explored. This study aims to investigate the potential correlation between constipation and suicidal ideation in US adults, while assessing the mediating role of depression.For this cross-sectional study, a total of 13,493 adults aged 20 years and older were included from the National Health and Nutrition Examination Survey 2005–2010. The definition of constipation was defined by considering the consistency or frequency of stool. The ninth item on the Patient Health Questionnaire-9 (PHQ-9) evaluated suicidal ideation, and depression was evaluated using the PHQ-8 score. Adjusted odds ratios (ORs) were calculated using multivariate logistic regression models. Sensitivity analysis was performed to ensure stable results. Furthermore, study employed mediation analysis to examine the effect of constipation on suicidal ideation through depression. The bootstrapping method was used to assess the significance of the mediation effect. After controlling for demographic factors, risk behaviors, comorbidities, dietary intake, and relevant medications, constipation was associated with an increased risk of suicidal ideation (OR 1.41, 95%CI 1.08–1.83, P = 0.011). Sensitivity analyses showed the stability of the results. Moreover, mediation analysis demonstrated a significant direct effect of constipation on suicidal ideation (P = 0.016), with depression playing a partial mediating role in this interaction (40.81%, P < 0.0001). In conclusion, this study demonstrated a significant association between constipation and suicidal ideation, with depression serving as a partial mediator in this relationship. Further prospective longitudinal studies are essential to establish a definitive causal relationship between these factors so as to guide the development and implementation of targeted intervention strategies.
Similar content being viewed by others

Introduction
Suicidal ideation is the desire for one’s life to end or thoughts of self-harm or suicide1,2, and is a significant indicator of potential suicide. Suicide is considered a major public health concern worldwide3. According to the World Health Organization’s (WHO) Global Suicide Report 2019, which was released in 2021, it was estimated that 703,000 individuals died by suicide worldwide in 2019, accounting for 1.3% of all annual deaths4. Nevertheless, these statistics are probably lower than the actual numbers because of inadequate recording of deaths and societal norms that discourage suicide5. Thus, it is crucial to investigate and identify the risk factors associated with suicidal ideation. The primary aim of the World Health Organization’s initiatives is to pinpoint populations at high risk in order to prevent and reduce suicide attempts6.
Recent studies have indicated a link between several gastrointestinal diseases and suicide7,8, including inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). Constipation, defined by persistent difficulty, incomplete evacuation, or infrequent bowel movements9, affects approximately 10.1% of the global adult population10. This condition results in a substantial decrease in quality of life and contributes to increased healthcare expenditures11. While extensive research has established a strong correlation between constipation and mental health issues like anxiety and depression12,13,14,15,16–known risk factors for suicidal ideation17,18,19– the direct association between constipation and suicidal ideation remains underexplored.
A study based on a US population found that individuals with constipation were significantly more prone to reporting suicidal ideation compared to those with regular bowel habits16. Similarly, a French study reported that individuals with more frequent constipation were at a higher risk of suicidal ideation20. In contrast, a study based on self-reported constipation found no link between constipation and suicidal ideation21. Consequently, the potential link between constipation and suicidal ideation is a topic of debate. Additionally, the influence of concurrent depression on constipated patients with suicidal ideation remains ambiguous.
There is an interaction between depression and gastrointestinal symptoms. For instance, IBS and IBD are both associated with significantly higher rates and severity of depression in the general population22,23,24. Similarly, patients with diagnosed depression report significantly more frequent gastrointestinal symptoms compared with individuals without depression25, with bowel-related symptoms highly associated with depression severity scores26. This interaction is likely mediated by mechanisms involving the gut-brain axis, gut microbiota dysbiosis, and chronic inflammation. This bidirectional relationship not only negatively impacts patients’ quality of life but also increases the healthcare burden. Therefore, clinicians should adopt a holistic approach when managing gastrointestinal symptoms, taking into account the emotional and psychological well-being of patients.
Further investigation into the correlation among constipation, depression and suicidal ideation will contribute to a deeper understanding of the psychological profiles of individuals with constipation, as well as timely identification of high-risk groups for suicidal ideation. This will provide clinicians with more comprehensive insights for treating patients with constipation and suicidal ideation. Owing to the paucity of evidence, we conducted a cross-sectional study utilizing a substantial sample from the National Health and Nutrition Examination Survey spanning 2005 to 2010 to investigate the potential association between suicidal ideation and constipation, as well as the impact of depression.
Materials and methods
Study population
The National Health and Nutrition Examination Survey (NHANES), administered by the National Center for Health Statistics (NCHS) under the auspices of the Centers for Disease Control and Prevention (CDC), is a cross-sectional survey targeting the non-institutional civilian population in the United States27. The research group, comprising a doctor, medical and healthcare specialists, as well as individuals conducting dietary and health interviews, journeyed throughout the nation. The Mobile Examination Center (MEC) was utilized to perform comprehensive physical examinations, interviews, and laboratory tests subsequent to demographic, socioeconomic, and medical health assessments conducted at participants’ residences. As this study utilized publicly available de-identified data from NHANES, informed consent was obtained by the original data collectors during primary data collection, and the study received approval from the NCHS Ethics Review Board.
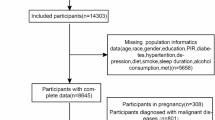
Since constipation data only existed in NHANES 2005−2010, the data in study were entirely from these three 2-years cycles, in which we extracted data from participants aged 20 years and older. Participants with incomplete data on suicidal ideation, stool frequency, and stool consistency were excluded from the analysis. Those who had missing data for other variables were not included in the analysis. Individuals diagnosed with colon and/or rectal cancer28,29 or currently pregnant28,29,30,31 were also excluded. Due to the substantial sample size, missing values for covariates were observed in less than 5%, thus we opted for direct deletion. In total, 13,493 participants were included in the analysis. The process of data selection is visually depicted in a flowchart, as shown in Fig. 1.

Flow diagram of the sample selection from the National Health and Nutrition Examination Survey (NHANES) 2005–2010.
Constipation
The definition of constipation was established by considering the consistency or frequency of stool, as previously suggested in publications utilizing the NHANES database32,33,34. This questionnaire was completed using a computer-assisted personal interview system in a mobile examination center interview room. Stool consistency was assessed using the Bristol Stool Form Scale (BSFS)35,36. Participants were shown a card with colored pictures and descriptions of the 7 BSFS types (Type 1–Type 7) and asked to “Please look at this card and tell me the number that corresponds with your usual or most common stool type.” Constipation is defined as BSFS type 1 (separate hard lumps, like nuts) or 2 (sausage-like, butlumpy), and normal function was defined as type 3 (like a sausage but with cracks in the surface), type 4 (like a sausage or snake, smooth and soft), type 5 (soft blobs with clear-cut edges), type 6 (fluffy pieces with ragged edges, a mushy stool) or type 7 (watery, no solid pieces)30,31,37,38. Stool frequency was assessed by asking participants how often they have a bowel movement in a week. Participants were asked "How many times per week do you usually have a bowel movement?" Participants reported a range of 1 to 80 bowel movements per week. According to NHANES data, those with less than 3 bowel movements per week were considered constipated, while those with 3 or more were considered non-constipated30,31,37,38.
Depression
The validated Patient Health Questionnaire-9 (PHQ-9) was utilized for the detection of depression in patients. In the general population, the PHQ-9 functions as a highly reliable and valid screening tool39. It is a validated 9-item public depression questionnaire40 that asks about symptoms of depression on a 4-point scale (0 = not at all; 1 = days; 2 = more than half the time; 3 = almost every day) with scores ranging from 0 to 27. These questions were asked by trained interviewers in Spanish or English using the Computer-Assisted Personal Interviewing (CAPI) system during the MEC private interview. Typically, patients with clinical depression were identified using a PHQ-9 score of 10 or above, which has an 88% sensitivity and specificity in detecting depression40,41. Depression was assessed in this research using the PHQ-8 scale, which has a potential score range of 0 to 24, by excluding the item related to thoughts of suicide from the PHQ-942. The presence or absence of depression was determined based on whether the PHQ-8 score was 10 or higher, indicated as “Yes” or “No” respectively43.
Suicidal ideation
A suicidal ideation assessment was conducted using item 9 of PHQ-943,44,45. Item 9 inquires, “Over the last two weeks, how often have you felt that you would be better off dead, or hurting yourself ?” Response options included “nearly every day”, “more than half the days”, “several days”, or “not at all”. Based on previous literature43,44,45, participants who responded "nearly every day," "more than half the days," and “several days” were considered to have suicidal ideation, while those who responded “none” were defined as not having suicidal ideation.
Covariates
Covariates included various factors that were theorized or previously demonstrated to have a connection with constipation or suicidal ideation16,43,44. The variables considered were sex (female and male), age, marital status, race/ethnicity, BMI (Body Mass Index), physical activity, level of education, smoking habits, alcohol consumption, use of SSRI (selective serotonin reuptake inhibitor) medications, reported health conditions, and dietary habits. Among these, age, BMI, physical activity, and dietary factors were directly examined as continuous variables. There were five groups used to categorize ethnicity/race: non-Hispanic White, non-Hispanic Black, other Hispanic, Mexican American, and other race groups. Marital status was categorized into six groups: married, widowed, divorced, separated, living with partner, and never married. The education level was divided into five categories: college graduate or higher, some college or associate’s degree, high school graduate/GED or equivalent, 9th–11th grade, and less than 9th grade. The level of physical activity was determined by considering the metabolic equivalent (MET) values associated with the type, frequency, and duration of activities performed each week. This was calculated by multiplying the MET value by the weekly frequency and the duration of each physical activity. MET values differ depending on the exercise type, and NHANES provides the suggested MET values for each specific physical activity46,47.
Alcohol consumption and smoking status are also risk factors associated with suicidal ideation3. Based on participants’ responses to the question "Do you smoke now?", smoking status was classified into three categories: never, former, and current smokers. Those categorized as “never smokers” were defined as individuals who had either never smoked or had consumed fewer than 100 cigarettes prior to the interview. The term “former smokers” included individuals who had previously smoked more than 100 cigarettes but had quit by the time of the interview. “Current smokers” referred to individuals with a history of smoking at least 100 cigarettes and were still actively smoking during the interview. Alcohol consumption was classified into three groups: never drinkers, former drinkers, and current drinkers. Individuals categorized as never drinkers had never consumed alcohol. Former drinkers were those who had previously imbibed but did not drink in the past year. Current drinkers referred to individuals who had consumed alcohol at least once and continue to do so.
The comorbid conditions comprised diabetes, hypertension, arthritis, hepatic disease, pulmonary disease (emphysema, asthma or chronic bronchitis), cardiovascular disease (including angina, myocardial infarction, chronic heart failure or coronary artery disease), and malignancy. The diagnostic criteria for diabetes mellitus comprised a physician’s diagnosis, glycohemoglobin (HbA1c) levels exceeding 6.5%, fasting glucose levels of ≥7.0 mmol/L, random or two-hour oral glucose tolerance test (OGTT) blood glucose levels of ≥11.1 mmol/L, or the utilization of diabetes medication/insulin. Comorbidities were determined through a series of 12 specific inquiries, such as: “Have you ever received a medical diagnosis for any of the following conditions: hypertension, arthritis, emphysema, asthma, chronic bronchitis, angina, liver disease, heart attack, congestive heart failure, coronary heart disease, or cancer?” The responses were classified as either affirmative or negative for each condition. Participants reported whether they used SSRI medications, categorizing their use as either “yes” or “no”. In the NHANES 24-hour dietary recall conducted in 2005−2010, information regarding dietary fiber, moisture, overall fat content, and caffeine was collected and examined as variables with continuous values.
Statistical analyses
A descriptive analysis was performed on the data obtained from all participants. Measures of central tendency and dispersion, such as means and standard deviations (SD) or medians and interquartile ranges (IQR), were used for continuous data, depending on the distributional characteristics. Categorical variables were represented in percentage form. The chi-square test was utilized to compare categorical variables, and t-tests were used for the analysis of continuous variables. Logistic regression models were employed to explore the relationship between constipation and suicidal thoughts. Both unadjusted and multivariate adjusted models were utilized for this investigation: Model I did not consider any covariates; Model II included age, sex, marital status, race/ethnicity, physical activity, level of education, BMI, alcohol consumption, and smoking; Model III was adjusted for the covariates in Model II as well as diabetes, hypertension, arthritis, heart disease, pulmonary disease, liver disease, cancer, and the use of SSRI; Model IV included adjustments for the variables in Model III along with dietary fiber, moisture, total fat, and caffeine. Finally, Model V accounted for covariates in model IV as well as depression (assessed by PHQ-8 score).
Subgroup analyses and interactions were conducted to assess the robustness of the association between constipation and suicidal ideation, with stratification by age, sex, education level, BMI, MET, hypertension, depression, SSRI use, diabetes, and dietary intake.
Additionally, two sensitivity analyses were performed to further evaluate the robustness of the results. Firstly, we incorporated the PHQ-8 score (obtained by subtracting item 9 from the PHQ-9 score) as a continuous variable in the analysis; secondly, we controlled for depression assessed by PHQ-9 as a covariate to confirm the consistency of the findings.
To assess the mediating role of depression in the relationship between constipation and suicidal ideation, causal mediation analyses were conducted. This involved: 1) examining the overall impact of constipation on suicidal ideation while controlling for all covariates, 2) analyzing the direct impact of constipation on suicidal ideation after adjusting for all covariates and depression, 3) assessing the indirect impact of constipation on suicidal ideation through depression while controlling for all covariates, and 4) determining the proportion of mediation by depression in the relationship between constipation and suicidal ideation (i.e., indirect effect/total effect). The results were identical to the usual LSEM method by Baron and Kenny48. The 95%CI for the mediated proportion was estimated through nonparametric bootstrapping with 1000 iterations.
Statistical significance was evaluated by comparing adjusted odds ratios (ORs) to 1.0 and presenting the 95% confidence intervals (95%CIs). The R software (http://www.R-project.org, The R Foundation) and Free Statistics software versions 1.9.2 were utilized for conducting the statistical analysis. A two-tailed test was conducted, and a significance level of P < 0.05 was adopted.
Results
Baseline characteristics
Table 1 presents a comparison of the characteristics of individuals in the constipated and non-constipated categories. Among these participants, 1376 reported experiencing constipation, resulting in a prevalence rate of 10.2%. Individuals with constipation were more likely to be younger, female, separated, widowed, divorced, never married, cohabiting with a partner, non-Hispanic black; have lower levels of education; engage in less physical activity; and have a lower BMI. Individuals experiencing constipation tend to have lower intake of dietary fiber, total fat, caffeine, and water in their diets. Constipation has been associated with increased risk of pulmonary disease and depression among patients with other health conditions. There were 528 cases of suicidal ideation reported, representing a prevalence rate of 3.9%. Individuals experiencing constipation had a notably higher prevalence of suicidal ideation (6.8%) compared to those who do not experience it (3.6%, P < 0.001), as shown in Table 1 and Fig. 2.

Suicidal ideation in non-constipated and constipated patients.
Multivariate logistic regression analysis
In the examination of the association between constipation and suicidal ideation as depicted in Fig. 3, Model I (unadjusted) revealed an increased likelihood of constipation in patients with suicidal ideation (OR: 1.95, 95%CI 1.54–2.45, P < 0.001). Upon adjusting for age, sex, marital status, race/ethnicity, physical activity, level of education, BMI, alcohol consumption, and smoking (Model II), constipation continued to exhibit an association with depression (OR: 1.75, 95%CI 1.38–2.23, P < 0.001). After accounting for covariates related to caffeine, moisture, total fat, and dietary fiber intake in addition to those included in Model II (Model III), the findings remained largely unchanged (OR: 1.74, 95%CI 1.37–2.21, P < 0.001). Furthermore, further adjustments were made by including covariates related to diabetes, hypertension, arthritis, heart disease, pulmonary disease, liver disease, cancer, and the use of SSRI on top of those from Model III (Model IV), resulting in consistent outcomes (OR: 1.72, 95%CI 1.35–2.20, P < 0.001). Finally, inclusion of depression as a covariate alongside those from Model IV (Model V) resulted in a persistent positive relationship between constipation and suicidal ideation (OR: 1.41, 95%CI 1.08–1.83, P < 0.001).

Multivariate regression analysis of the association between constipation and suicidal ideation. Notes aModel I: no adjusted. bModel II: adjusted for age + sex + race/ethnicity + marital status + education level + BMI + physical activity + smoking status + alcohol consumption. cModel III: Model II+ dietary fiber + moisture + total fat + caffeine. dModel IV: Model III + diabetes + hypertension + arthritis + heart disease + pulmonary disease + liver disease + cancer + SSRI use. eModel V: Model IV + depression(assessed by PHQ-8 score).
Subgroup analysis
Figure 4 and Supplementary figure 1 presents subgroup analyses that investigated the association between suicidal ideation and constipation. No statistically significant interactions were observed in subgroup analyses (P > 0.05). The link between constipation and suicidal ideation remained consistent across all subgroups.

Subgroup analysis and interaction of the association between constipation and suicidal ideation. Notes aSSRI: selective serotonin reuptake inhibitor. Adjusted for age, sex, race/ethnicity, marital status, education level, physical activity, BMI, smoking status, alcohol intake, dietary fiber intake, moisture intake, total fat intake, caffeine intake, SSRI use, diabetes, liver disease, heart disease, pulmonary disease, hypertension, arthritis, cancer and depression.
Sensitivity analysis
In the initial analysis of sensitivity, model V was adjusted by incorporating the PHQ-8 score (excluding item 9 of the PHQ-9 score) as a continuous variable. The results remained consistent (OR: 1.35, 95%CI 1.03–1.78, P = 0.031), as illustrated in Supplementary Table 1. In the subsequent sensitivity analysis, depression evaluated by PHQ-9 (including item 9) was included as an adjusting covariate in the final model, and once again produced reliable outcomes (OR: 1.33, 95%CI 1.02–1.74, P = 0.037), as indicated in Supplementary Table 2.
Mediation analysis
A mediation analysis was conducted to explore the role of depression in the relationship between constipation and suicidal ideation (Fig. 5, Table 2 and Supplementary Table 3). We used Model IV to conduct the mediation analysis. The total effect on the suicidal ideation was 0.0026 (95% CI 0.0011–0.0046, P < 0.0001), of which the direct effect of depression was 0.0015 (95%CI 0.0002–0.0031, P = 0.016), and the indirect effect of constipation was 0.0011 (95%CI 0.0007–0.0018, P < 0.0001). It suggests that depression partially mediated the association between constipation and suicidal ideation, accounting for approximately 40.81% (95%CI 27.20–85.70%) of the total effect.

Effect of the depression (mediators) on the relationship between constipation (exposure) and suicidal ideation (outcome). *** P-value < .001.
Discussion
This study conducted with a sample representing the entire nation revealed a strong correlation between constipation and suicidal ideation, regardless of other factors such as baseline characteristics, risk factors, diet, and other medical conditions. Co-existing depression partially mediates the association between constipation and suicidal ideation.
There have been limited studies investigating the link between suicidal ideation and constipation. A study conducted in France on 1469 outpatients found that individuals with more frequent constipation were more likely to have suicidal ideation compared to those without constipation, even after accounting for factors such as age, gender, BMI, psychological scores, and clinical scales (P < 0.001)20. However, our investigation is based on a larger sample of the American population, and after adjusting for more covariates associated with suicidal ideation or constipation, we confirmed the reliability of the significant correlation between constipation and suicidal ideation. According to NHANES data, another study also found that individuals with constipation were significantly more prone to reporting suicidal ideation compared to those with regular bowel habits (P = 0.036)16. Nevertheless, this research only conducted a preliminary analysis of the correlation and did not independently quantify the findings. In addition, this study only defined constipation based on BSFS, but did not consider defecation frequency, which is also an important method to assess constipation. Our study added bowel frequency as a measure of constipation, independently quantified the association between constipation and suicidal ideation using multivariate regression analysis, and validated the robustness of the findings through subgroup analysis and interaction assessment. Furthermore, neither of the above studies investigated the role of depression in the association between constipation and suicidal ideation. Our study, however, found that depression partially mediated the association between constipation and suicidal ideation.
A different study found no link between constipation and suicidal ideation, with an OR of 1.36 and a 95%CI of 0.78–2.3721. In this study, the constipation data was self-reported. Participants responded to the question, "How often have you been constipated during the past 12 months?" Respondents who selected “most of the time” or “always” were categorized as experiencing constipation, whereas those who chose “never”, “rarely”, or “sometimes”, were not classified as such. First, this is really different from the way we evaluate constipation. The methods used to define constipation in this study focused on the participants’ own feelings, while the methods used in our study focused more on objective indicators, such as the consistency and frequency of stool. Further research is needed to investigate whether different definitions of constipation lead to different conclusions. Second, our sample size was relatively large, three times larger than the sample size of the cited studies. While the cited literature did not show a statistically significant variance in results, there was a noticeable trend indicating a potential association based on the effect size and 95%CI. If the sample size can be expanded, it is possible to obtain statistically significant results21. In general, the p value is related to sample size and significance49. It is possible to obtain small p values in large datasets with weak associations or large p values in small datasets with strong associations50. After all, for an outcome as serious as suicidal ideation, even a small probability is worth paying attention to.
Mental health conditions such as anxiety and depression have been demonstrated to significantly increase the likelihood of suicidal ideation in various medical contexts and within the general population17,18,19. Depression was found to have a strong correlation with constipation according to studies12,13,14,15,16. Nevertheless, it remains uncertain whether depression, as a significant covariate, has any impact on the significance of the association between constipation and suicidal ideation. Our research found that the link between constipation and suicidal ideation stayed strong even when accounting for depression (Model V) (OR 1.41, 95%CI 1.08–1.83, P < 0.001). The correlation, however, weakened significantly after accounting for depression compared to before (Model IV) (OR 1.72, 95%CI 1.35–2.20, P < 0.001), suggesting that although depression weakened the strength of the association between constipation and suicidal ideation, it did not affect the independent association between them. To further explore the role of depression in the relationship between constipation and suicidal ideation, a mediating analysis was also performed. The results revealed that depression partially mediated the association between constipation and suicidal ideation, accounting for approximately 40.81% of the total effect.
The association between constipation, depression and suicidal ideation may be related to a significant interaction between the central nervous system (CNS) and the gastrointestinal tract, also known as the brain-gut axis. First, constipation is associated with dysbiosis of the gut microbiota51. The gut microbiota can influence the synthesis and release of short-chain fatty acids (SCFAs) and neurotransmitters, such as such as 5-hydroxytryptamine (5-HT), which may contribute to mood disorders like depression and anxiety52,53,54. These mood disorders are significantly correlated with suicidal ideation55,56. Furthermore, the vagus nerve is a critical component of the gut-brain axis, facilitating bidirectional communication between the enteric nervous system (ENS) and the CNS57. Studies have shown that when the CNS is stimulated by mental disorders such as depression, it can reduce the vagal tone, leading to the occurrence or aggravation of many gastrointestinal diseases, including constipation58. Additionally, constipation patients often report a decline in quality of life, including reduced social engagement and increased feelings of loneliness59, which are strongly linked to suicidal ideation60.
This study also examined the demographic characteristics, dietary habits, and lifestyle factors associated with constipation and suicidal ideation (Fig. 4 and Supplementary figure 1). First, we explored the potential effects of age and gender on the association between constipation and suicidal ideation. Subgroup analysis showed that there was no significant difference in age between ≥ 50 years and < 50 years, nor between males and females (all P for interaction > 0.05). Although older adults could theoretically be at higher risk for depression due to chronic illness and social isolation61,62,63,64,65 and for suicidal ideation higher in women than in men66, our findings suggest that the association between constipation and suicidal ideation does not differ significantly in these subgroups. Future studies with larger samples are needed to confirm these exploratory observations. Second, the association between constipation and suicidal ideation was stronger in people with higher education level, BMI, and exercise metabolic equivalent. At present, there is a lack of previous relevant literature. We infer that this may be due to the fact that this segment of the population may be more sensitive to health problems, pay more attention to symptoms, and thus be more likely to report psychological distress. This remains to be further explored. Finally, the association between constipation and suicidal ideation was more pronounced among persons with lower water intake, which is consistent with previous studies67. Understanding the factors associated with constipation and suicidal ideation helps to optimize resource allocation and ensure that medical resources are directed to high-risk populations.
In light of these findings, it is important to examine the potential association between constipation and depression or suicidal ideation. Although this study suggests a possible link, further longitudinal research is necessary to establish causal relationships. Healthcare providers should consider integrating brief depression screening tools, such as the PHQ-268,69, into consultations with patients experiencing constipation. However, it is important to acknowledge that these findings require additional investigation before widespread clinical recommendations can be implemented. Moreover, future studies should investigate whether addressing constipation directly could improve both psychological and physical health outcomes.
The current research has numerous advantages. Our primary strength lies in the extensive, nationally representative sample of American individuals at our disposal, enabling us to meticulously investigate the correlation between constipation and suicidal ideation. Second, we adjusted for as many covariates as possible, such as BMI, risky behaviors, dietary intake, comorbidities, and associated medications, which made our results more robust. Thirdly, we bolstered the validation of our findings through subgroup analyses based on age, sex, education level, BMI, MET, hypertension, depression, SSRI use, diabetes, and dietary intake. Lastly, we delved deeper into investigating the potential influence of depression on the relationship between constipation and suicidal ideation—a facet that remained ambiguous in prior studies.
Nevertheless, it is important to acknowledge some constraints in our research. First of all, because the study is cross-sectional, it is not possible to make causal inferences about constipation and suicidal ideation, and reverse causality cannot be ruled out. Additionally, given the cross-sectional design of this study, the inability to establish temporal relationships between variables restricts causal interpretation, and also limits the validity of mediation analysis. Longitudinal studies are essential to monitor and analyze the temporal changes in gastrointestinal health and mental well-being. Furthermore, constipation was determined based on stool consistency or frequency of bowel movements according to previous research, yet it was unclear if participants met the Roman criteria for constipation. Finally, despite adjusting for possible confounders, observational studies still face the risk of residual confounding.
Conclusion
In conclusion, this study demonstrated a significant association between constipation and suicidal ideation, with depression serving as a partial mediator in this relationship. Therefore, it is necessary to conduct systematic screening and evaluation of depression and suicidal ideation in patients with constipation. Future research should adopt longitudinal designs with multiple assessment time points to systematically investigate the evolution of these relationships, thereby providing stronger evidence for developing intervention strategies.
Data availability
The data utilized in this study, which is both publicly accessible and de-identified, is located in the NHANES database of the CDC National Center for Health Statistics, accessible at https //wwwn.cdc.gov/nchs/nhanes/Default.aspx.
References
Nock, M. K. et al. Suicide and suicidal behavior. Epidemiol. Rev. 30 (1), 133–154 (2008).
Mann, J. J., Waternaux, C., Haas, G. L. & Malone, K. M. Toward a clinical model of suicidal behavior in psychiatric patients. Am. J. Psychiatry. 156 (2), 181–189 (1999).
Hawton, K. & van Heeringen, K. Suicide Lancet 373 (9672), 1372–1381 (2009).
WHO (World Health Organization). Suicide Worldwide in 2019: Global Health Estimates (World Health Organziation, 2021).
Michael, H., Merson, R. E. B. & Anne, J. Mills. Global Health (Jones & Bartlett Learning, 2012).
World Health Organization. World Report on Violence and Health (WHO, 2002).
Triantafillidis, J. K., Hyphantis, T., Cheracakis, P., Antoniou, A. & Sklavaina, M. Suicide as an outcome in patients with inflammatory bowel disease. Am. J. Gastroenterol. 97 (4), 1066–1068 (2002).
Miller, V., Hopkins, L. & Whorwell, P. J. Suicidal ideation in patients with irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2 (12), 1064–1068 (2004).
Vriesman, M. H., Koppen, I. J. N., Camilleri, M., Di Lorenzo, C. & Benninga, M. A. Management of functional constipation in children and adults. Nat. Rev. Gastroenterol. Hepatol. 17 (1), 21–39 (2020).
Barberio, B., Judge, C., Savarino, E. V. & Ford, A. C. Global prevalence of functional constipation according to the Rome criteria: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 6 (8), 638–648 (2021).
Nag, A. et al. The humanistic and economic burden of chronic idiopathic constipation in the USA: A systematic literature review. Clin. Exp. Gastroenterol. 13, 255–265 (2020).
Kim, J. Y. & Lim, M. H. Psychological factors to predict chronic diarrhea and constipation in Korean high school students. Med. (Baltim). 100 (27), e26442 (2021).
Rajindrajith, S. et al. Behavioral and emotional problems in adolescents with constipation and their association with quality of life. PLoS One. 15 (10), e0239092 (2020).
Adibi, P. et al. Relationship between depression and constipation: Results from a large Cross-sectional study in adults. Korean J. Gastroenterol. 80 (2), 77–84 (2022).
Andy, U. U. et al. Shared risk factors for constipation, fecal incontinence, and combined symptoms in older U.S. Adults. J. Am. Geriatr. Soc. 64 (11), e183–e188 (2016).
Ballou, S. et al. Chronic diarrhea and constipation are more common in depressed individuals. Clin. Gastroenterol. Hepatol. 17 (13), 2696–2703 (2019).
Nock, M. K., Hwang, I., Sampson, N. A. & Kessler, R. C. Mental disorders, comorbidity and suicidal behavior: Results from the National comorbidity survey replication. Mol. Psychiatry. 15 (8), 868–876 (2010).
Hintikka, J. et al. Are factors associated with suicidal ideation true risk factors? A 3-year prospective follow-up study in a general population. Soc. Psychiatry Psychiatr Epidemiol. 44 (1), 29–33 (2009).
Cavanagh, J. T., Carson, A. J., Sharpe, M. & Lawrie, S. M. Psychological autopsy studies of suicide: A systematic review. Psychol. Med. 33 (3), 395–405 (2003).
Deutsch, D. et al. Functional Gastrointestinal disorders as predictors of suicidal ideation. An observational study. Eur. J. Gastroenterol. Hepatol. 33 (1S Suppl 1), e758–e765 (2021).
Wang, Y., Shen, X. & Wang, P. Constipation is associated with depression of any severity, but not with suicidal ideation: Insights from a large cross-sectional study. Int. J. Colorectal Dis. 38 (1), 231 (2023).
Mykletun, A. et al. Prevalence of mood and anxiety disorder in self reported irritable bowel syndrome (IBS). An epidemiological population based study of women. BMC Gastroenterol. 10, 88 (2010).
Fuller-Thomson, E. & Sulman, J. Depression and inflammatory bowel disease: Findings from two nationally representative Canadian surveys. Inflamm. Bowel Dis. 12 (8), 697–707 (2006).
Bhandari, S., Larson, M. E., Kumar, N. & Stein, D. Association of inflammatory bowel disease (IBD) with depressive symptoms in the united States population and independent predictors of depressive symptoms in an IBD population: A NHANES study. Gut Liver. 11 (4), 512–519 (2017).
Hillilä, M. T., Hämäläinen, J., Heikkinen, M. E. & Färkkilä, M. A. Gastrointestinal complaints among subjects with depressive symptoms in the general population. Aliment. Pharmacol. Ther. 28 (5), 648–654 (2008).
Dipnall, J. F. et al. Into the bowels of depression: Unravelling medical symptoms associated with depression by applying Machine-Learning techniques to a community based population sample. PLoS One. 11 (12), e0167055 (2016).
CDC. Centers for Disease Control and Preventions National Health and Nutrition Examination Survey: Questionnaires, datasets, and related documentation. (2009).
Wang, C., Zhang, L. & Li, L. Association between selenium intake with chronic constipation and chronic diarrhea in adults: Findings from the National health and nutrition examination survey. Biol. Trace Elem. Res. 199 (9), 3205–3212 (2021).
Wang, P. et al. Association between constipation and major depression in adult AmericansEevidence from NHANES 2005–2010. Front. Psychiatry. 14, 1152435 (2023).
Shen, L. et al. Lower dietary fibre intake, but not total water consumption, is associated with constipation: A population-based analysis. J. Hum. Nutr. Diet. 32 (4), 422–431 (2019).
Wilson, P. B. Associations between physical activity and constipation in adult Americans: results from the National health and nutrition examination survey. Neurogastroenterol. Motil. 32 (5), e13789 (2020).
Liu, Q., Kang, Y. & Yan, J. Association between overall dietary quality and constipation in American adults: a cross-sectional study. BMC Public. Health. 22 (1), 1971 (2022).
Kang, Y. & Yan, J. Exploring the connection between caffeine intake and constipation: A cross-sectional study using National health and nutrition examination survey data. BMC Public. Health. 24 (1), 3 (2024).
Zhao, X., Wang, L. & Quan, L. Association between dietary phosphorus intake and chronic constipation in adults: Evidence from the National health and nutrition examination survey. BMC Gastroenterol. 23 (1), 24 (2023).
Yang, S. et al. Association of dietary energy intake with constipation among men and women: Results from the National health and nutrition examination survey. Front. Nutr. 9, 856138 (2022).
Yang, S. et al. Association of sleep duration with chronic constipation among adult men and women: Findings from the National health and nutrition examination survey (2005–2010). Front. Neurol. 13, 903273 (2022).
Li, Y., Tong, W. D. & Qian, Y. Effect of physical activity on the association between dietary fiber and constipation: Evidence from the National health and nutrition examination survey 2005–2010. J. Neurogastroenterol Motil. 27 (1), 97–107 (2021).
Zhang, L., Du, Z., Li, Z., Yu, F. & Li, L. Association of dietary magnesium intake with chronic constipation among US adults: Evidence from the National health and nutrition examination survey. Food Sci. Nutr. 9 (12), 6634–6641 (2021).
Martin, A., Rief, W., Klaiberg, A. & Braehler, E. Validity of the brief patient health questionnaire mood scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry. 28 (1), 71–77 (2006).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16 (9), 606–613 (2001).
Kroenke, K. Enhancing the clinical utility of depression screening. CMAJ 184 (3), 281–282 (2012).
Kroenke, K. et al. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 114 (1–3), 163–173 (2009).
Tektonidou, M. G., Dasgupta, A. & Ward, M. M. Suicidal ideation among adults with arthritis: Prevalence and subgroups at highest risk. Data from the 2007–2008 National health and nutrition examination survey. Arthritis Care Res. (Hoboken). 63 (9), 1322–1333 (2011).
Moazzami, K., Dolmatova, E. V. & Feurdean, M. Suicidal ideation among adults with cardiovascular disease: The National health and nutrition examination survey. Gen. Hosp. Psychiatry. 51, 5–9 (2018).
Simon, G. E. et al. Does response on the PHQ-9 depression questionnaire predict subsequent suicide attempt or suicide death? Psychiatr Serv. 64 (12), 1195–1202 (2013).
Liang, J. et al. Association between joint physical activity and dietary quality and lower risk of depression symptoms in US adults: Cross-sectional NHANES study. JMIR Public. Health Surveill. 9, e45776 (2023).
Chen, L. et al. Risk/benefit tradeoff of habitual physical activity and air pollution on chronic pulmonary obstructive disease: Findings from a large prospective cohort study. BMC Med. 20 (1), 70 (2022).
Tingley, D., Yamamoto, T., Hirose, K., Keele, L. & Imai, K. Mediation: R package for causal mediation analysis. J. Stat. Soft. 59 (5), 1–38 (2014).
Kühberger, A., Fritz, A., Lermer, E. & Scherndl, T. The significance fallacy in Inferential statistics. BMC Res. Notes. 8, 84 (2015).
Kang, D., Choi, J., Kim, Y. & Kwon, D. An analysis of the dynamic Spatial spread of COVID-19 across South Korea. Sci. Rep. 12 (1), 9364 (2022).
Ohkusa, T., Koido, S., Nishikawa, Y. & Sato, N. Gut microbiota and chronic constipation: A review and update. Front. Med. (Lausanne). 6, 19 (2019).
Silva, Y. P., Bernardi, A. & Frozza, R. L. The role of Short-Chain fatty acids from gut microbiota in gut-Brain communication. Front. Endocrinol. (Lausanne). 11, 25 (2020).
Yano, J. M. et al. Indigenous bacteria from the gut microbiota regulate host serotonin biosynthesis. Cell 161 (2), 264–276 (2015).
Kelly, J. R. et al. Transferring the blues: Depression-associated gut microbiota induces neurobehavioural changes in the rat. J. Psychiatr Res. 82, 109–118 (2016).
Hawton, K., Casañas, I., Comabella, C., Haw, C. & Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 147 (1–3), 17–28 (2013).
Thibodeau, M. A., Welch, P. G., Sareen, J. & Asmundson, G. J. Anxiety disorders are independently associated with suicide ideation and attempts: Propensity score matching in two epidemiological samples. Depress. Anxiety. 30 (10), 947–954 (2013).
Bonaz, B., Bazin, T. & Pellissier, S. The vagus nerve at the interface of the Microbiota-Gut-Brain axis. Front. Neurosci. 12, 49 (2018).
Ranasinghe, N., Devanarayana, N. M., Benninga, M. A., van Dijk, M. & Rajindrajith, S. Psychological maladjustment and quality of life in adolescents with constipation. Arch. Dis. Child. 102 (3), 268–273 (2017).
Johanson, J. F. & Kralstein, J. Chronic constipation: A survey of the patient perspective. Aliment. Pharmacol. Ther. 25 (5), 599–608 (2007).
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T. & Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 10 (2), 227–237 (2015).
Grover, S. & Malhotra, N. Depression in elderly: A review of Indian research. J. Geriatr. Ment Heal. 2, 4–15 (2015).
Seo, J., Choi, B., Kim, S., Lee, H. & Oh, D. The relationship between multiple chronic diseases and depressive symptoms among middle-aged and elderly populations: Results of a 2009 Korean community health survey of 156,747 participants. BMC Public. Health. 17, 844 (2017).
Grover, S., Avasthi, A. & Sahoo, S. Relationship of loneliness and social connectedness with depression in elderly: A multicentric study under the aegis of Indian association for geriatric mental health. J. Geriatr. Ment Heal. 5, 99–106 (2017).
Minayo, M. C. & Cavalcante, F. G. Suicide in elderly people: A literature review. Rev. Saude Publica. 44, 750–757 (2010).
Negin Joel, M., et al. Prevalence of HIV and chronic comorbidities among older adults. AIDS 26, S55–S63 (2012).
Schernhammer, E. S. & Colditz, G. A. Suicide rates among physicians: A quantitative and gender assessment (meta-analysis). Am. J. Psychiatry. 161, 2295–2302 (2004).
Lee, J. W. & Kim, Y. Association of plain water intake with self-reported depression and suicidality among Korean adolescents. Epidemiol. Health. 46, e2024019 (2024).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The patient health Questionnaire-2: Validity of a two-item depression screener. Med. Care. 41 (11), 1284–1292 (2003).
Löwe, B., Kroenke, K. & Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 58 (2), 163–171 (2005).
Acknowledgements
We thank Dr. Liu Jie (People’s Liberation Army of China General Hospital, Beijing, China) and Dr. Yang Qilin (The Second Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, China) for their help with this revision.
Funding
This work was supported by Yan Xiaohua Nationally Famous Traditional Chinese Medicine Expert Inheritance Studio (2022-06), project for the construction of flagship hospitals for the collaboration of traditional Chinese and Western medicine.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows—P.W., Y.W., H.L., F.G., Y.J. and X.Y. contributed to study planning, data analyses and drafting of the manuscript; P.W., Y.Y., Y.W. and Y.J. contributed to study planning and manuscript development; P.W., H.L., X.H., F.G. and X.Y. contributed to study planning and data analyses; All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Informed consent
All individuals provided written consent.
Human Ethics and Consent to Participate
The Centers for Disease Control and Prevention ‘s Institutional Review Board for Research Ethics has given approval for the protocol of the National Health and Nutrition Examination Survey. The National Center for Health Statistics Ethics Review Board approved the protocol with the informed consent of all participants. All methods were carried out in accordance with relevant guidelines and regulations (declaration of Helsinki).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, P., Wang, Y., Li, H. et al. Association of constipation with suicidal ideation among US adults and the partial mediating role of depression. Sci Rep 15, 10936 (2025). https://doi.org/10.1038/s41598-025-95252-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-95252-y
