
Abstract
Previous studies found that frailty has a significant impact on the prognosis of hypertensive patients. However, most of the previous studies only focused on baseline frailty status. The association of changes in frailty with mortality in hypertensive patients is little known. Therefore, we aimed to investigate the association of frailty transitions with all-cause mortality and cardiovascular death in older adults with hypertension. A total of 1827 older hypertensive participants age ≥ 65 years from the Chinese Longitudinal Healthy Longevity Study were included. Frailty status was assessed by a 35-item frailty index (FI). Changes in frailty were evaluated by frailty at baseline (wave 2011) and the second survey (wave 2014), and four types of changes in frailty were identified: remaining non-frail, frail to non-frail, non-frail to frail, and remaining frail. The accelerated failure time model was used to evaluate the association of changes in frailty status with all-cause mortality and cardiovascular death. The dose–response relationship between annual changes in FI and mortality was analyzed using restricted cubic splines (RCS). During 6128.9 person-years of follow-up, a total of 623 all-cause mortality and 131 cardiovascular deaths were recorded. Compared to the remaining non-frail group, the fully adjusted time ratios (TRs) of all-cause mortality were 0.75 (95% CI 0.59–0.96, p = 0.025), 0.48 (95% CI 0.41–0.57, p < 0.001), and 0.45 (95% CI 0.37–0.55, p < 0.001) in the frail to non-frail group, non-frail to frail group, and remaining frail group, respectively. After adjusting for potential confounding variables, the adjusted TRs of cardiovascular death were 0.63 (95% CI 0.36–1.11, p = 0.108), 0.34 (95% CI 0.23–0.48, p < 0.001), and 0.34 (95% CI 0.22–0.53, p < 0.001) in the frail to non-frail group, non-frail to frail group, and remaining frail group, respectively. RCS analysis revealed a non-linear relationship between annual changes in FI and all-cause mortality and cardiovascular death (both p for non-linearity < 0.05). Stratified and sensitivity analysis showed similar results. Frailty is a dynamic process, and worsening in frailty status accelerated all-cause mortality and cardiovascular death in older adults with hypertension. In contrast, improvement in frailty status prolonged the survival time of patients.
Similar content being viewed by others

Introduction
Hypertension is one of the most common chronic diseases, the number of individuals with hypertension in the global has been estimated to increase from 1.13 billion in 2015 to 1.56 billion in 20251,2, and more than 60% of people aged > 60 years suffered from hypertension3. It is a leading risk factor for cardiovascular diseases and mortality4,5, accounting for 13% of deaths worldwide6, which brings a heavy burden to society and families.
Hypertension and frailty often coexist in older people7. Frailty is a complex age-related clinical condition characterized by a decline in the physiological reserves of multiple organ systems and an increased sensitivity to stressors, which increases the risk of adverse health outcomes for older adults8,9. Frailty is becoming an increasingly common condition with an increasing burden of global population aging. Previous studies demonstrated that the prevalence of frailty in different hypertensive populations ranged from 17.8% to 27.6%, and frailty increases the risk of falls, fractures, hospitalization, and mortality in hypertensive patients9,10,11,12. In addition, based on a national prospective cohort study, our team found that baseline frailty status is significantly associated with overall survival in older adults with hypertension aged ≥ 65 years. Compared with robust hypertensive patients, the survival time of patients with prefrailty and frailty is significantly shorter13. However, most of the previous studies only focused on baseline frailty status, not considering changes in frailty status during follow-up. Frailty is a dynamic process over time and it is partially reversible14,15, studying frailty transitions can reflect more comprehensive biological associations than a single assessment of frailty status at baseline. In recent years, the association of frailty transitions with health outcomes has attracted great attention. He et al.16 reported that changes in frailty status are associated with the risks of incident cardiovascular disease (CVD), recovery of frailty status decreases incident CVD risks, while the progression of frailty status increases incident CVD risks. Nari et al.17 evaluated the influence of frailty transitions on cognitive function in older adults, and the results showed that individuals who experienced frailty transitions (ameliorating or worsening) and those maintaining frail were more likely to have a lower cognitive function than those maintaining non-frail. Other studies also reported the association of changes in frailty status with health outcomes18,19,20. However, little is known about the association of frailty transitions with adverse outcomes in hypertensive patients.
To fill this research gap, in the present study, we used a prospective cohort study to evaluate the association of changes in frailty status with all-cause mortality and cardiovascular death among older adults with hypertension.
Methods
Study design and population
This study was based on the Chinese Longitudinal Healthy Longevity Study (CLHLS), which is an ongoing, nationwide, prospective cohort study of community-dwelling Chinese older people. The CLHLS utilized a multistage, stratified cluster sampling method to recruit participants from half of the counties and cities of 23 provinces in China, covering approximately 85% of the Chinese population, and its primary aim was to investigate the factors influencing healthy aging and longevity among the elderly. It was initiated in 1998, and subsequent follow-up surveys were conducted every 2–4 years (waves 2000, 2002, 2005, 2008, 2011, 2014, and 2018). New participants of the same sex and similar age were enrolled in each follow-up wave to reduce the attrition due to death and loss to follow-up. Trained interviewers administered the surveys using a structured questionnaire at participants’ homes. A more detailed description of CLHLS can be found in previous studies21,22. This study was approved by the Medical Ethics Committee of Peking University (IRB00001052-13074), and all participants or their legal representatives provided written informed consent.
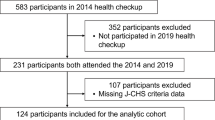
In the current study, wave 2011 was considered as the study baseline, wave 2014 was regarded as the second survey, and participants completing the frailty status assessment at baseline and the second survey were included. Subsequently, the participants were followed up until wave 2018. The detailed recruitment process for the participants and the study timeline and design are depicted in Fig. 1. Finally, 1827 hypertensive patients aged ≥ 65 years were included in the present analysis.

Study flow chart. Note: Except for the missing data, some potential abnormal blood pressure values were defined as missingness, including SBP < 80 or > 300 mm Hg, DBP < 40 or > 200 mm Hg, and SBP minus DBP < 10 or > 200 mm Hg. Abbreviations: SBP: systolic blood pressure; DBP: diastolic blood pressure.
Assessment of hypertension
The participants were asked to receive two BP measurements by trained researchers using a mercurial sphygmomanometer after resting for 5 min or longer. The systolic blood pressure (SBP) and diastolic blood pressure (DBP) for each participant were determined by calculating the average of the two measurements. In addition, participants’ hypertension history was evaluated by the question “Are you suffering from hypertension?”. According to the guideline23, hypertension was defined as (1) SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg or (2) a self-reported of history of physician-diagnosed hypertension.
Assessment of frailty status
Frailty status was defined by the frailty index (FI), a robust marker of biological age24,25. The standard procedure for creating FI was outlined by Searle et al.26, and it was recommended that at least 30 deficit items should be included. Based on the standard procedure for constructing FI, we appropriately modified the 38-item FI used in previous research27. The modified FI contains 35 items, encompassing multiple age-related health deficits. FI calculates a person’s cumulative health deficits, and each deficit is mapped onto the interval of 0 to 1; dichotomous items are scored as 0 (absence) or 1 (present), and polychotomous items are assigned different scores (e.g., always = 0, often = 0.25, sometimes = 0.5, seldom = 0.75, never = 1). Table S1 shows the items used to construct FI, and the items’ corresponding scores are defined in detail. The FI was calculated as the sum of the items’ scores divided by the number of items each participant owned. FI ranges from 0–1, and participants with a higher FI indicate a higher frailty status. In our study, participants who had items ≥ 30 were included. Referring to a previous study28, we classified frailty status into two categories: non-frail (FI ≤ 0.20) and frail (FI > 0.20). Changes in frailty were evaluated by frailty status at baseline and the second survey, and four types of change in frailty were identified: remaining non-frail, frail to non-frail, non-frail to frail, and remaining frail (Figure S1).
Covariates
Covariates include sociodemographic information, lifestyle-related factors, and chronic comorbidities. Sociodemographic information includes sex, age, marital status, residence, education, income, and living with family. Lifestyle-related factors include lifestyles (current smoking, current drinking, and current exercise) and regular intake of foods (vegetables, fruits, meats, fish, eggs, and beans). Chronic comorbidities include heart disease, diabetes, cerebrovascular disease, respiratory diseases, and cancer. Table S2 shows detailed information on these covariates.
Study outcomes
The participants were followed up until wave 2018, and the study outcomes were all-cause mortality and cardiovascular death. The International Classification of Diseases, Tenth Revision (ICD-10) was utilized to define the underlying causes of death, and cardiovascular death was identified by ICD-10 codes I00-I99. Participants’ survival status was ascertained as surviving, deceased, or lost to follow-up in each survey. The date and cause of death were collected based on the official death certificate if available, or from participants’ close relatives or residents committee. The quality of mortality data in the CLHLS is relatively reliable, with generally satisfactory results compared to other major aging studies21.
Statistical analyses
Table S3 shows the distributions of baseline variables with missing data in the present study, and the missing values were no more than 1.06%. To ensure the authenticity and reliability of our analysis, we deleted the participants with missing baseline variables in the main analyses. We conducted the analyses with the following five steps: (1) comparisons of baseline data; (2) evaluating the association of changes in frailty status with all-cause mortality and cardiovascular death; (3) exploring the dose–response relationship between annual changes in FI and outcomes; (4) performing stratified analyses and sensitivity analyses to evaluate the robustness of the main findings; and (5) conducting additional analyses to expand the main results.
Participants were categorized into four groups based on the changes in frailty. When describing the baseline characteristics of these four groups, continuous variables were expressed as median (interquartile range, [IQR]), while categorical variables were expressed as number (percentage). The Kruskal–Wallis test was performed for continuous variables and the Chi-square test or Fisher’s exact test was conducted for categorical variables. The survival probability in each group was estimated using the Kaplan–Meier method, and the log-rank test was used for comparisons. Because Schoenfeld Residuals indicated a violation of the proportional hazards assumption in the Cox proportional hazards regression models, multivariable parametric accelerated failure time (AFT) models were used to assess the association of changes in frailty status with all-cause mortality and cardiovascular death. Three models were constructed, and potential confounding variables associated with frailty and mortality were adjusted. AFT models with different distributions (Weibull, logistic, log-logistic, log-normal, exponential, and Gaussian) were examined, and the Weibull distribution was selected in the present analysis based on the minimum Akaike Information Criterion (Table S4). The results of AFT models were expressed using the time ratio (TR). TR is called an acceleration factor, and it is usually used to reflect the impact of each variable on the survival. A TR < 1 indicates that the time to event was shorter than the reference group, whereas a TR > 1 indicates the time to event was prolonged29,30.
Restricted cubic splines (RCS) analysis was used to assess the dose–response relationship between annual changes in FI and all-cause mortality and cardiovascular death among individuals with hypertension, and the Likelihood ratio test was used to test nonlinearity. Stratified analyses were conducted to evaluate the association of changes in frailty status with outcomes in different subgroups, and interactions were examined using the likelihood ratio test. Additionally, several sensitivity analyses were conducted to test the robustness of the main findings: (1) to minimize potential reverse causation, we excluded the participants who died within the first year; (2) to clarify the role of participants lost to follow-up in the association of changes in frailty status and outcomes, we regarded these participants censored at two time points: median (3.70 years) and the end of follow-up time (5.19 years); (3) to mitigate potential bias caused by missing data of baseline covariates, multiple imputations were performed for these covariates, and 10 datasets were created using by chained equations, of which the resultant model estimates for each were combined using Rubin’s rules; (4) because the FI cut-off values for defining frailty status were controversial, we used another common FI cut-off value to define frailty: non-frail (FI < 0.25) and frail (FI ≥ 0.25)16; (5) because diabetes and heart disease are cardiovascular risk factors, we re-constructed the FI after excluding the two items from the original FI, and analysis the association of changes in frailty status with cardiovascular death; (6) we regarded participants with unknown causes of death as cardiovascular death, and then performed analysis to test the robustness of main findings.
Furthermore, to expand the main results, we classified baseline frailty status into three categories: robust (FI ≤ 0.10), prefrail (0.10 < FI ≤ 0.20), and frail (FI > 0.30)28, and then, 9 types of changes in frailty status were developed from baseline to the second survey. We performed exploratory analyses to examine the association of these changes in frailty with all-cause mortality and cardiovascular death. We regarded it as an exploratory analysis because the sample size for each group is relatively small.
All statistical analyses were performed using R software (version 4.1.3), and a two-sided p < 0.05 was considered statistically significant.
Results
Baseline characteristics of the study population
At baseline, there were 1555 (85.1%) non-frail participants and 272 (14.9%) frail participants. After a period of 2–3 years, the trajectories of frailty among participants changed: 1313 (71.9%) participants maintained non-frail, 115 (6.3%) changed from frail to non-frail, 242 (13.2%) changed from non-frail to frail, and 157 (8.6%) maintained frail. The baseline characteristics of the study population according to changes in frailty status were presented in Table 1. The median age of these participants was 80.0 (IQR: 73.0, 88.0) years, and 838 (45.9%) participants were men. Overall, results revealed statistically significant differences in most baseline characteristics across the four groups, including sex, age, marital status, education, income, lifestyles, regular intake of fruits, regular intake of vegetables, regular intake of meats, diabetes, heart disease, cerebrovascular diseases, and respiratory diseases.
Association of changes in frailty status with all-cause mortality and cardiovascular death
During 6128.9 person-years of follow-up, 623 all-cause mortality were recorded, with 131 deaths attributed to cardiovascular disease. Table S5 shows the detailed information about the causes of death. The all-cause mortality rates were 6.9 (95% CI 6.2–7.6), 13.7 (95% CI 10.2–17.2), 19.9 (95% CI 16.9–22.9), and 29.7 (95% CI 25.1–34.3) per 100 person-years in the group of remaining non-frail, frail to non-frail, non-frail to frail, and remaining frail, respectively; and the cardiovascular mortality rates across the four groups were 1.3 (95% CI 0.9–1.6), 2.7 (95% CI 1.1–4.4), 5.5 (95% CI 3.8–7.2), and 6.5 (95% CI 4.0–9.0) per 100 person-years, respectively (Table 2). Kaplan–Meier analysis also showed a significant decrease in the survival probability from the remaining non-frail group to the remaining frail group in all-cause mortality and cardiovascular death (both log-rank p < 0.001) (Fig. 2). In the AFT models, compared to the remaining non-frail group, the fully adjusted TRs of all-cause mortality were 0.75 (95% CI 0.59–0.96, p = 0.025), 0.48 (95% CI 0.41–0.57, p < 0.001), and 0.45 (95% CI 0.37–0.55, p < 0.001) in the frail to non-frail group, non-frail to frail group, and remaining frail group, respectively. After adjusting for potential confounding variables, the adjusted TRs of cardiovascular death were 0.63 (95% CI 0.36–1.11, p = 0.108), 0.34 (95% CI 0.23–0.48, p < 0.001), and 0.34 (95% CI 0.22–0.53, p < 0.001) in the frail to non-frail group, non-frail to frail group, and remaining frail group, respectively (Table 2). The results indicated that compared with remaining non-frail participants, the time to occur all-cause mortality was accelerated by 25%, 52%, and 55% for those who transitioned from frail to non-frail, non-frail to frail, and remaining frail, respectively. Similarly, the time to occur cardiovascular death was accelerated by 66% for those who transitioned from non-frail to frail and remaining frail.

Kaplan–Meier curves of the survival rate of older adults with hypertension by changes in frailty status. Note: (A) All-cause mortality; (B) Cardiovascular death.
RCS analyses
Considering the influence of interval time of frailty assessment, we explored the dose–response relationship between annual changes in FI and all-cause mortality and cardiovascular death, and two nonlinear relationships were observed (both p for non-linearity < 0.05) (Fig. 3). The inflection points for both all-cause mortality and cardiovascular death were 0. When the annual change in FI was < 0, there was no association with all-cause mortality [TRper SD (standard deviation) = 1.03, 95% CI 0.95–1.13] and cardiovascular death (TRper SD = 1.07, 95% CI 0.87–1.31); When the annual change in FI > 0, the adjusted TR for all-cause mortality and cardiovascular death were 0.78 (95% CI 0.72–0.83) and 0.64 (95% CI 0.55–0.74) with per SD increase in annual changes in FI, which means when the annual change in FI > 0, the time to occur all-cause mortality and cardiovascular death was accelerated by 22% and 36% with per SD increase in annual changes in FI. In addition, RCS analysis revealed a linear relationship between baseline FI and all-cause mortality (p for non-linearity = 0.078) and cardiovascular death (p for non-linearity = 0.874) (Figure S2). The adjusted TR for all-cause mortality and cardiovascular death were 0.81 (95% CI 0.76–0.86) and 0.79 (95% CI 0.69–0.91) with per SD increase in baseline FI.

Dose–response relationship between annual changes in FI and mortality in older adults with hypertension. Note: (A) all-cause mortality, (B) cardiovascular death. Annual changes in FI = (FI at the second survey – FI at the baseline)/interval time between the two waves (years). The number of RCS nodes was determined based on the lowest value of the Akaike information criterion. TR and 95% CI were derived from the AFT model with adjustment for sex, age, marital status, residence, living with family, education, income, lifestyles (current smoking, drinking, and regular exercise), intake of foods (fruits, vegetables, meats, fish, eggs, and beans), systolic BP, and diastolic BP. Abbreviations: FI: frailty index; TR: time ratio; CI: confidence interval; SD: standard deviation; RCS: restricted cubic spline; BP: blood pressure.
Stratified analysis
Stratified analyses were conducted to evaluate the association of changes in frailty status with outcomes, based on sex, age, marital status, residence, living with family, education, income, lifestyles, comorbidities, SBP, and DBP. Changes in frailty status exerted a more pronounced impact on all-cause mortality in older hypertensive participants with DBP ≥ 90 mm Hg (p for interaction = 0.035), no significant interaction was detected in other subgroups (Figure S3). Regarding cardiovascular death, no significant difference was observed in all subgroup analyses (all p interactions ≥ 0.05) (Figure S4). Overall, the results of stratified analyses were consistent with the main findings.
Sensitivity analysis
Sensitivity analyses from different perspectives were performed to examine the stability of the main analysis. The results were consistent with the main analyses after excluding deaths within the first year of follow-up (Table S6). When treating participants lost to follow-up as censored at the median or the end of follow-up, the association of changes in frailty with all-cause mortality and cardiovascular death was also preserved (Table S7 and Table S8). Similar results were also observed after multiple imputations for missing values of baseline covariates (Table S9). Moreover, after using another cut-off value of FI to define frailty, the results remained unchanged (Table S10). In addition, the association of changes in frailty status with cardiovascular death did not find substantial changes when considering the death of unknown reasons as cardiovascular death (Table S11), or using the 33-item FI after excluding two items of diabetes and heart disease (Table S12). Overall, the results of a series of sensitivity analyses confirmed the stability of the main analysis.
Exploratory analysis
To expand the main results, we classified baseline frailty status into three categories, and 9 types of changes in frailty status were developed from baseline to the second survey. Then, we performed exploratory analyses to examine the associations of changes in frailty status with outcomes for baseline robust, prefrail, and frail participants, respectively. For baseline robust participants, compared to those in the remaining robust group, the fully adjusted TRs of all-cause mortality were 0.73 (95% CI 0.57–0.95, p = 0.019) and 0.55 (95% CI 0.38–0.80, p = 0.002) in robust to prefrail group and robust to frail group, respectively; the fully adjusted TRs of cardiovascular death were 0.63 (95% CI 0.35–1.15, p = 0.136) and 0.38 (95% CI 0.17–0.86, p = 0.020) in robust to prefrail group and robust to frail group, respectively (Table S13). For baseline prefrail participants, compared to those in the remaining prefrail group, the fully adjusted TRs of all-cause mortality were 1.45 (95% CI 1.08–1.93, p = 0.012) and 0.54 (95% CI 0.43–0.67, p < 0.001) in prefrail to robust group and prefrail to frail group, respectively; the fully adjusted TRs of cardiovascular death were 1.09 (95% CI 0.50–2.37, p = 0.830) and 0.25 (95% CI 0.13–0.46, p < 0.001) in prefrail to robust group and prefrail to frail group, respectively (Table S14). For baseline frail participants, compared to those in the remaining frail group, the multivariate-adjusted TRs of all-cause mortality were 1.60 (95% CI 1.22–2.08, p = 0.001) and 2.67 (95% CI 1.25–5.67, p = 0.011) in frail to prefrail group and frail to robust group, respectively; the multivariate-adjusted TRs of cardiovascular death was 1.60 (95% CI 1.03–2.48, p = 0.037) in frail to prefrail group (Table S15). Overall, improvement in frailty status significantly prolonged the time of occurring adverse outcomes, in contrast, worsening in frailty status accelerated all-cause mortality and cardiovascular death.
Discussion
Based on a prospective cohort study, we investigated the association of changes in frailty status with all-cause mortality and cardiovascular death among older adults with hypertension. The results of our research revealed that changes in frailty are significantly associated with adverse outcomes in aged hypertensive patients. Worsening in frailty status accelerated all-cause mortality and cardiovascular death, in contrast, improvement in frailty status prolonged the survival time of patients. Stratified analyses in different subgroups, a series of sensitivity analyses, and exploratory analyses confirmed the robustness of the results.
Frailty is a dynamic process over time. A meta-analysis revealed that among 42,775 community-dwelling older adults, 56.5% of participants maintained the baseline frailty status, and 42.8% of participants had frailty status changed (29.1% worsened, and 13.7% improved) during a mean follow-up of 3.9 years15. Roberto et al. prospectively included 119 patients with stable chronic obstructive pulmonary disease (COPD), and they reported that 70.5% of patients had maintained the same frailty status, 11.7% had worsened, and 17.6% had improved after 2 years of follow-up19. Other studies also reported dynamic changes in frailty status18,31,32. Our study confirmed the previous findings on the dynamic nature of frailty status. After a mean of 2.6 years of follow-up, we observed that 71.9% of participants maintained non-frail, 6.3% changed from frail to non-frail, 13.2% changed from non-frail to frail, and 8.6% maintained frail. Given that frailty is a dynamic process over time, and it has an important influence on adverse health outcomes, it is necessary to take appropriate measures to improve, prevent, or delay the progression of frailty. Physical activity, healthy lifestyles, management of multimorbidity and chronic diseases, psychosocial support, well management of weight, and protein intake could improve frailty transitions7,14,31,32.
The association of frailty transitions with health outcomes has attracted increasing attention in recent years. Based on three prospective cohorts, He et al.16 found that frailty transitions are associated with risks of incident CVD. Compared with stable robust participants, those who progressed to prefrail or frail had increased risks of incident CVD; while the risks of incident CVD decreased for those who recovered to robust or prefrail when compared with stable frail participants. Wang et al.33 conducted a prospective cohort study in 921 older community-based adults aged 65–99 years, the result demonstrated that compared with remaining robust participants, the risks of all-cause mortality increased by 2.76 folds, 3.87 folds, and 4.08 folds for those robust to frail, frail to robust, and frail to frail participants, respectively. A prospective study conducted by Roberto et al.19 demonstrated that transitions in frailty status are associated with significant changes in clinical outcomes in patients with stable COPD. In addition, Wang et al.34 found that remaining robust or improved frailty status is significantly associated with a lower risk of all-cause and cardiovascular mortality in community-dwelling older adults. In the present study, we examined the association of changes in frailty status with mortality in aged Chinese hypertensive patients. The results indicated that compared with remaining non-frail participants, the time to occur all-cause mortality was accelerated by 25%, 52%, and 55% for those who transitioned from frail to non-frail, non-frail to frail, and remaining frail, respectively. Similarly, compared with remaining non-frail participants, the time to occur cardiovascular death was accelerated by 66% for those who transitioned from non-frail to frail and remaining frail. More importantly, in stratified analyses, we found that worsening in frailty status is more likely to accelerate all-cause mortality in older hypertensive participants with DBP ≥ 90 mm Hg. Most previous studies have focused on SBP management in frail elderly adults7, our finding highlighted that we also need to strengthen the management of DBP in frail elderly patients with hypertension. However, no other relevant studies have been reported at present, and the underlying mechanisms are unclear, therefore, more studies are needed to verify the stability of the result and explore the underlying mechanisms.
Based on 4 longitudinal studies of aging, Erwin et al.35 found an increase in annual FI growth by 0.01 was associated with an increased all-cause mortality risk. In the present study, we found when annual changes in FI > 0, all-cause mortality and cardiovascular death of hypertensive patients were accelerated by 22%, and 36%, respectively, with per SD increase in annual changes in FI. In addition, we observed that there was a linear relationship between baseline FI and mortality in older hypertensive patients, which further corroborated previous findings13.
Our study has important clinical and public health implications. First, this study provides crucial evidence for the interventions on frailty in clinical practice. Frailty changes dynamically and it is partially reversible, periodically frailty assessment should be taken into routine clinical practice for older hypertensive patients, and effective prevention strategies should be taken to improve frailty status or delay the progression of frailty to reduce adverse health outcomes. Second, blood pressure should be closely monitored for older hypertensive patients, attention should be paid not only to SBP management but also to DBP management, especially for those with DBP ≥ 90 mm Hg. Third, in the context of global aging, healthcare systems should proactively allocate resources for frailty assessment, prevention, management, and research.
There are some limitations in this study. First, the sample size included in the study was relatively small, which may affect the generality of the results. In addition, this study only included hypertensive patients aged ≥ 65 years, the findings cannot be generalized to other populations. Second, frailty status was assessed only at baseline and after 2–3 years, which may not be adequate to capture the changes timely, especially for older adults with faster health deterioration. In addition, more times of evaluations may be more precise in determining changes in frailty status. Third, some of the data may exist recall bias as information was collected using a standard questionnaire. Fourth, although multiple confounders were adjusted, some residual and unmeasured confounders may still exist, such as genetic susceptibility (e.g., family history of hypertension or cardiovascular disease) and social determinants (e.g., socioeconomic status, or access to healthcare), which could influence both the progression of frailty and mortality in older adults with hypertension. This is a point that future research may need to pay attention to. Fifth, the AFT model assumes that the effect of covariates is multiplicative on the survival time, which, while suitable for our data given the violation of proportional hazards, may not capture more complex relationships. Additionally, the AFT model’s reliance on parametric assumptions (e.g., Weibull distribution) may limit its flexibility compared to the Cox model.
Conclusions
Changes in frailty status are significantly associated with adverse outcomes in older hypertensive patients. Worsening in frailty status accelerated all-cause mortality and cardiovascular death; in contrast, improvement in frailty status prolonged the survival time of patients. These findings highlight that we should assess frailty status periodically in older hypertensive patients, and develop effective prevention strategies to improve frailty status or delay the progression of frailty.
Data availability
The data used for analyses are available in the National Archive of Computerized Data on Aging (NACDA) repository, persistent web link: https://www.icpsr.umich.edu/icpsrweb/NACDA/series/487.
Abbreviations
- FI:
-
Frailty index
- TR:
-
Time ratio
- CI:
-
Confidence interval
- CLHLS:
-
Chinese Longitudinal Healthy Longevity Survey
- BP:
-
Blood pressure
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- IQR:
-
Interquartile range
- AFT:
-
Accelerated failure time
- RCS:
-
Restricted cubic spline
- SD:
-
Standard deviation
- HR:
-
Hazard ratio
References
Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet. 389, 37–55 (2017).
Kearney, P. M. et al. Global burden of hypertension: Analysis of worldwide data. Lancet 365, 217–223 (2005).
Williams, B. et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur. Heart J. 39, 3021–3104 (2018).
Aune, D., Huang, W., Nie, J. & Wang, Y. Hypertension and the risk of all-cause and cause-specific mortality: An outcome-wide association study of 67 causes of death in the national health interview survey. Biomed. Res. Int. 2021, 9376134 (2021).
Lawes, C. M. M., Vander, H. S. & Rodgers, A. Global burden of blood-pressure-related disease, 2001. Lancet 371, 1513–1518 (2008).
Ezzati, M., Lopez, A. D., Rodgers, A., Vander, H. S. & Murray, C. J. L. Selected major risk factors and global and regional burden of disease. Lancet 360, 1347–1360 (2002).
Li, L. et al. Hypertension in frail older adults: Current perspectives. Peer J. 12, e17760 (2024).
Ensrud, K. E. et al. Frailty and risk of falls, fracture, and mortality in older women: The study of osteoporotic fractures. J. Gerontol. A Biol. Sci. Med. Sci. 62, 744–751 (2007).
Ma, L., Zhang, L., Sun, F., Li, Y. & Tang, Z. Frailty in Chinese older adults with hypertension: Prevalence, associated factors, and prediction for long-term mortality. J. Clin. Hypertens. (Greenwich). 20, 1595–1602 (2018).
Li, L. et al. Frailty in hypertensive population and its association with all-cause mortality: Data from the National Health and Nutrition Examination Survey. Front. Cardiovasc. Med. 10, 945468 (2023).
Pajewski, N. M. et al. Characterizing frailty status in the systolic blood pressure intervention trial. J. Gerontol. A Biol. Sci. Med. Sci. 71, 649–655 (2016).
Hu, K. et al. Association between frailty and mortality, falls, and hospitalization among patients with hypertension: A systematic review and meta-analysis. Biomed. Res. Int. 2021, 2690296 (2021).
Li, L. et al. Association of frailty status with overall survival in elderly hypertensive patients: Based on the Chinese Longitudinal Healthy Longevity Survey. BMC Public Health 24, 1468 (2024).
Hoogendijk, E. O. et al. Frailty: Implications for clinical practice and public health. Lancet 394, 1365–1375 (2019).
Kojima, G., Taniguchi, Y., Iliffe, S., Jivraj, S. & Walters, K. Transitions between frailty states among community-dwelling older people: A systematic review and meta-analysis. Ageing Res. Rev. 50, 81–88 (2019).
He, D. et al. Changes in frailty and incident cardiovascular disease in three prospective cohorts. Eur. Heart J. 45, 1058–1068 (2024).
Nari, F. et al. Frailty transitions and cognitive function among South Korean older adults. Sci. Rep. 11, 10658 (2021).
Liu, Z. Y. et al. Frailty transitions and types of death in Chinese older adults: A population-based cohort study. Clin. Interv. Aging. 13, 947–956 (2018).
Bernabeu, M. R. et al. Frailty transitions and associated clinical outcomes in patients with stable COPD: A longitudinal study. PLoS ONE 15, e0230116 (2020).
Li, C. M. et al. Frailty status changes are associated with healthcare utilization and subsequent mortality in the elderly population. BMC Public Health 21, 645 (2021).
Zeng, Y. Towards deeper research and better policy for healthy aging —Using the unique data of Chinese Longitudinal Healthy Longevity Survey. China Econ. J. 5, 131–149 (2012).
Zeng, Y., Feng, Q., Hesketh, T., Christensen, K. & Vaupel, J. W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 389, 1619–1629 (2017).
Bakris, G., Ali, W. & Parati, G. ACC/AHA Versus ESC/ESH on hypertension guidelines: JACC guideline comparison. J. Am. Coll. Cardiol. 73, 3018–3026 (2019).
Goggins, W. B., Woo, J., Sham, A. & Ho, S. C. Frailty index as a measure of biological age in a Chinese population. J. Gerontol. A Biol. Sci. Med. Sci. 60, 1046–1051 (2005).
Jazwinski, S. M. & Kim, S. Examination of the dimensions of biological age. Front. Genet. 10, 263 (2019).
Searle, S. D., Mitnitski, A., Gahbauer, E. A., Gill, T. M. & Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 8, 24 (2008).
Zhang, J., Wang, Q., Hao, W. & Zhu, D. Long-term food variety and dietary patterns are associated with frailty among Chinese older adults: A cohort study based on CLHLS from 2014 to 2018. Nutrients 14, 4279 (2022).
Shrauner, W. et al. Frailty and cardiovascular mortality in more than 3 million US Veterans. Eur. Heart J. 43, 818–826 (2022).
Iraji, Z., Jafari, K. T., Dolatkhah, R. & Asghari, J. M. Parametric survival model to identify the predictors of breast cancer mortality: An accelerated failure time approach. J. Res. Med. Sci. 25, 38 (2020).
Jankowski, J. A. Z. et al. Esomeprazole and aspirin in Barrett’s oesophagus (AspECT): A randomised factorial trial. Lancet 39, 400–408 (2018).
Trevisan, C. et al. Factors influencing transitions between frailty states in elderly adults: The progetto veneto anziani longitudinal study. J. Am. Geriatr. Soc. 65, 179–184 (2017).
Pollack, L. R. et al. Patterns and predictors of frailty transitions in older men: The osteoporotic fractures in men study. J. Am. Geriatr. Soc. 65, 2473–2479 (2017).
Wang, M. C. et al. Frailty, transition in frailty status and all-cause mortality in older adults of a Taichung community-based population. BMC Geriatr. 19, 26 (2019).
Wang, Z., Ruan, H., Li, L., Song, N. & He, S. Association of changes in frailty status with the risk of all-cause mortality and cardiovascular death in older people: Results from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). BMC Geriatr. 24, 96 (2024).
Stolz, E., Hoogendijk, E. O., Mayerl, H. & Freidl, W. Frailty changes predict mortality in 4 longitudinal studies of aging. J. Gerontol. A Biol. Sci. Med. Sci. 76, 1619–1626 (2021).
Acknowledgements
The authors thank the staff and the participants of the CLHLS study for their valuable contributions.
Funding
This study was supported by Sichuan Science and Technology Program, China (Grant No. 2022YFS0186), the Key Technology Research and Device Development Project for Innovative Diagnosis and Treatment of Structural Heart Disease in the Southwest Plateau Region (Grant No. 202302AA310045), and Research and Application of Epidemiology, Pathogenesis, Diagnosis and Treatment of Cardiovascular Diseases in High Altitude of Yunnan Province Project (Grant No. 202103AC100004).
Author information
Authors and Affiliations
Contributions
L.L. and L.D. analyzed the data and wrote the manuscript. B.W. and K.W. analyzed the data. G.N., S.H., and J.T. reviewed and revised the manuscript. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The CLHLS study was approved by the Research Ethics Committee of Peking University (IRB00001052-13074). All methods and research processes for this study were performed in accordance with the Declaration of Helsinki guidelines and regulations. All participants or their proxy respondents provided written informed consent.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, L., Duan, L., Wang, B. et al. Association of changes in frailty with mortality in the aged with hypertension. Sci Rep 15, 12422 (2025). https://doi.org/10.1038/s41598-025-95904-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-95904-z
