
Abstract
Katakori, or neck and shoulder stiffness, is a common issue in Japan but also affects people globally. Recently, the Katakori Disability Index (KDI) was developed to measure the disability caused by Katakori, but its cross-cultural validity was unconfirmed. This study examined the KDI’s validity across Japan, the US, and Singapore through cross-sectional surveys of individuals aged 20–69 experiencing Katakori. Using multigroup confirmatory factor analysis (MGCFA), cross-cultural validity was deemed to exist if no statistically significant difference was found after changing to the partial metric invariance. Further, internal consistency was evaluated using Cronbach’s alpha, and KDI scores across the three countries were compared. MGCFA established cross-cultural validity by achieving partial metric invariance in 26 of 55 item combinations. Prevalence was 61.8% (420/680 participants) in the US and 75.1% (417/555 participants) in Singapore. Singaporeans (n = 162) reported the highest % KDI scores, followed by the US (n = 149), with the lowest scores being observed in Japan (n = 515). Internal consistency was strong across all countries (95% CI of alpha > 0.9). In conclusion, the KDI is valid for measuring Katakori disability across Japan, the US, and Singapore. This study underscores the need for global research on Katakori.
Similar content being viewed by others

Introduction
Katakori—stiff neck/shoulder in English—is a Japanese term for nonspecific symptoms such as discomfort or dull pain due to muscle stiffness around the occiput, cervical spine, acromion, and scapular area1. Katakori is diagnosed solely on subjective symptoms, and standardized diagnostic criteria have not been obtained2. Katakori can be primary, in which the underlying disease is unknown; or secondary, in which the underlying disease is obvious, such as orthopedic, medical, or neurological disease2. In the Japanese census, Katakori was identified as the most common symptom in women (12.5%) and the second most common symptom in men (6.0%)3. Katakori results in substantial loss of work productivity (the 2nd leading symptom of work productivity loss, at $414 per person per year) in Japan4. The latest Japanese clinical practice guideline for chronic pain5 identified Katakori as one of the most important clinical issues, but could not identify effective management due to a lack of valid outcomes6.
Since then, a series of studies has been initiated to develop a valid and reliable patient-reported outcome measures (PROM) for disability due to Katakori through investigations of the following three orders of importance according to the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) guidelines: (1) content validity, (2) internal structure assessments (i.e., construct validity, internal consistency, and cross-cultural validity), (3) others, including reliability, measurement error, criterion validity, hypotheses testing for construct validity and responsiveness. In 2024, a unidimensional PROM with 11 question items, the Katakori Disability Index (KDI), was developed through the content validity investigations7,8, assessments of construct validity and internal consistency in the Japanese population9. Among the internal structure to be assessed, investigation of the cross-cultural validity of the KDI is required to use the KDI globally.
Experience of Katakori would not be a uniquely Japanese complaint. In a comparative study with the US, Ishida10 reported that the same experience of Katakori as by Japanese is also observed among Americans. In Japanese, KATA in Katakori means shoulder, and KORI means stiffness. The meaning of “KATA” in Japanese Kanji characters denotes authority, power, mental strain, or tension11, and similar meanings are found in Chinese and Korean languages. Thus, while the experience of Katakori may be universal, it is possible that the internal structure measured by the KDI is different between people in Asian countries and between people in the Asia and the West, indicating the lack of cross-cultural validity of the KDI. Currently, cross-cultural validation is possible only among Japan, English-speaking countries with a Western background (e.g., US), and English-speaking countries with an Asian background (e.g., Singapore) because the only non-Japanese version of the KDI is the English one that was translated by its developer9.
The latest Japanese clinical practice guideline for chronic pain5 suggested more studies to identify effective strategies for management and prevention of Katakori. These verifications will thus accelerate and produce a major medical revolution if cross-cultural validity of the KDI is confirmed and the KDI can be used to verify the disability of Katakori in multiple cultures other than Japan. The aim of this study was to investigate the cross-cultural validity of the KDI among people in Japan, an English-speaking country with a Western background and an English-speaking country with an Asian background.
Results
In the US group, the first part of the survey was completed by 680 participants (265 men and 415 women, mean [SD] age = 39.3 [12.5] years), revealing a prevalence of Katakori of 61.8% (420/680). In the second part of the survey, data from 149 individuals (72 men and 77 women, mean [SD] age = 43.3 [15.2] years) were analyzed, and data from 110 individuals (53 men and 57 women, mean [SD] age = 44.3 [14.7] years) were used for multigroup confirmatory factor analysis (MGCFA) and internal consistency verification. In the Singapore group, the first part of the survey was completed by 555 participants (288 men and 267 women, mean [SD] age = 44.1 [11.1] years), revealing a prevalence of Katakori of 75.1% (417/555). In the second part of the survey, data from 162 individuals (86 men and 76 women, mean [SD] age = 43.8 [13.5] years) were analyzed, and data from 144 individuals (78 men and 66 women, mean [SD] age = 44.4 [13.8] years) were used for the MGCFA and internal consistency verification. In the Japanese group, among the 515 participants, data from 404 individuals (193 men and 211 women, mean [SD] age = 45.6 [13.7] years) were used for the MGCFA and internal consistency verification.
In the MGCFA, configural invariance was confirmed first (comparative fit index [CFI] = 0.888, root mean square error of approximation [RMSEA] = 0.076). Subsequently, among 55 combinations of two items, 26 patterns showed no statistically significant differences when adjusted for partial metric invariance (Table 1). However, within these 26 patterns, all showed statistically significant differences when adjusted for partial scalar invariance. Based on these results, the cross-cultural validity of the KDI was confirmed in this study.
The internal consistency, as measured by Cronbach’s alpha (95% confidence interval), was 0.938 (0.919–0.954) for the US group, 0.934 (0.917–0.949) for the Singapore group, and 0.914 (0.901–0.926) for the Japanese group, indicating acceptable internal consistency across all groups.
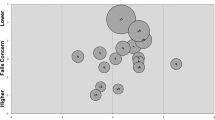
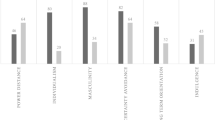
The KDI scores for each item are shown in Fig. 1. Across all items, the scores for Singapore were statistically significantly higher than those for Japan, and for all items except “watching TV,” the scores for the US were statistically significantly higher than those for Japan. A comparison of the KDI % scores among the three countries revealed that the Singapore group (mean [SD] = 59.1 [23.1] %) scored the highest, followed by the US group (50.6 [27.6] %) and the Japanese group (36.8 [21.0] %), with statistically significant differences observed among all groups (Fig. 2).

Box plots of each Katakori Disability Index score for each item across the three countries. 1: Japan, 2: US, 3: Singapore. × indicates the mean value.

Response distributions of the Katakori Disability Index % scores and the results of the Steel-Dwass method across the three countries.
Table 2 presents the KDI % scores of 30 groups categorized by country, age, and gender, and group comparisons are detailed in Appendix 1. Among the 30 age-gender-country combinations, statistically significant differences in KDI % scores were observed for 33 pairs comparing Japan and Singapore, and two pairs comparing Japan and the US, but no statistically significant differences were found within the same country. Notably, in the age- and gender-matched comparisons between countries, the 20s and 60s age groups in Singapore showed statistically significantly higher KDI % scores than their counterparts in Japan for both men and women.
Discussion
This study examined the cross-cultural validity of the KDI using data from the US, Singapore, and Japan through MGCFA analysis. The results confirmed configural invariance of the KDI’s single-factor structure. Furthermore, among 55 combinations of two items, no statistically significant differences were observed in 26 patterns when adjusted to partial metric invariance, suggesting cross-cultural validity. The internal consistency of the KDI in each country was high, with the lower bound of the 95% confidence interval exceeding 0.9. Further, a comparison of item scores across the three countries revealed that scores for Singapore were significantly higher than those for Japan for all items, while scores for the US were significantly higher than those for Japan for all items except “watching TV.” These findings indicate that there is no significant response variability across countries. The high internal consistency in each country and the absence of items with large response variations between countries support the interpretation that the KDI’s single-factor structure has cross-cultural validity.
The prevalence of Katakori in the studied populations was 61.8% in the US and 75.1% in Singapore. Additionally, the % KDI was higher in Singapore and the US than in Japan. These results suggest that Katakori is not an issue unique to Japan or Asia but is also an issue that cannot be overlooked in Western countries in terms of both prevalence and its impact on daily life. Although the adverse effects of Katakori and national prevalence surveys have not garnered much attention outside Japan, this study highlights the necessity of promoting research on Katakori not only in Japan but globally.
An interesting finding is that there is a statistically significant difference among the three countries, with Singapore having the highest KDI % scores, followed by the US, and Japan having the lowest. The reasons behind this disparity remain unclear, highlighting the need for further research. Takanashi et al.12 investigated 1,000 Japanese individuals with “Katakori” and 660 Americans with “neck pain.” While stiffness and pain were common to both groups, they reported significant differences in the nature of “pain” between the Japanese group with Katakori and the American group with neck pain, as well as in the nature of “stiffness” between the Japanese group and the American group with neck pain that included stiffness. Kutsunogi and Kuroiwa11 found no differences in prevalence, gender, age distribution, or pathophysiology between Japanese Katakori and Western neck pain. However, they observed a stronger correlation between Katakori and psychosocial stress in Japan. Traditionally in Japan, the term “Kata” has been used not only to denote a physical body part as the shoulder but also to express emotions, fate, human relationships, and mental burdens or tension. It is said that Japanese people tend to avoid psychological explanations for the causes of emerging symptoms as much as possible and attribute them to physical characteristics such as constitution13. Furthermore, Iijima et al.14 compared perceived cause of Katakori between Japanese and American and reported that a higher percentage of Japanese thought Katakori was caused by physical fatigue, while a higher percentage of Americans thought Katakori was caused by mental fatigue. Therefore, the difference in KDI % scores among the three countries may be due to differences in the way people think about the causes, severity, treatment, and prognosis of certain symptoms when they are aware of them, which is derived from their own culture (i.e., the exploratory model)15. Further investigations into the factors related to KDI % scores would be necessary to better understand the differences on the % KDI scores and the exploratory model among the three countries.
In the comparison of KDI % scores across all combinations of age, gender, and country, statistically significant differences were observed in only 33 pairs between Japan and Singapore and 2 pairs between Japan and the US. No statistically significant differences were found within comparisons conducted within a single country. When comparing matched age and gender groups between countries, both male and female participants in their 20s and 60s in Singapore showed significantly higher KDI % scores than their counterparts in Japan. These findings support the necessity of examining cross-cultural validity not only by gender or age but also across the three countries.
Limitations
This study has several limitations. First, as only the KDI was used to collect valid data, while the cross-cultural validity of the psychological traits measured by the KDI across the three countries can be inferred through MGCFA, it remains unclear whether there are differences in the factors related to the KDI. Further, the possibility that some influence during and after the COVID-19 pandemic, e.g., differences in the impact on lifestyle factors, might have influenced the differences in KDI scores cannot be ruled out because Japanese data and US/Singapore data were collected at different times. Therefore, further investigations are required for understanding of the KDI score comparability between countries and relevant factors. Second, in the KDI % score calculation method, importance and bothersomeness have the same weights (i.e., a person scoring “5 [extremely important] × 3 [slightly bothersome] = 15” and another scoring “3 [slightly important] × 5 [extremely bothersome] = 15” receive the same score). However, there has been no statistical verification of the plausibility of this calculation method; and thus, when the score calculation algorithm is modified in the future, the results of the cross-cultural validity can be changed, and re-investigation will be required. Third, the COSMIN guideline does not provide clear criteria for cross-cultural validity, and in this study, considering the criticism that the evaluation by the MGCF is too strict, it was considered to have cross-cultural validity if no statistically significant difference was found after changing to the partial metric invariance16. Additionally, the model fit was considered acceptable if the CFI was greater than 0.95 or the RMSEA was less than 0.08, as recommended by COSMIN. However, stricter application of these criteria could potentially yield different results. Future research should establish standardized methodologies for assessing cross-cultural validity. Lastly, this study compared only three countries: Japan, Singapore (as a representative of an Asian region where English is the primary language), and the US (as a representative of English-speaking Western culture). The observed differences in KDI scores between Singapore and the US, despite both being English-speaking countries, suggest that other countries might also exhibit unique KDI score characteristics. Further international comparisons and analyses of the cross-cultural validation of the KDI are warranted.
Conclusion
In conclusion, the cross-cultural validity of the KDI in Japan, Singapore, and the US suggests that one concept measured by the KDI is not substantially different among the three countries. However, there were differences in KDI scores among the three countries, suggesting that factors associated with KDI may differ among each population. Katakori is not a problem unique to Japan, but is also a problem that cannot be ignored in English-speaking countries, both in terms of prevalence and impact on daily life. Research aimed at developing preventive measures for Katakori worldwide, based on the KDI, is considered necessary.
Methods
Design
This study included data from two cross-sectional anonymous surveys: one was conducted in Japan to develop the final format of the KDI (11 items and one dummy item) from a provisional KDI (30 items and one dummy item)9, and the other was conducted for this study for people in the US as an English-speaking country with a Western background and Singapore as an English-speaking country with an Asian background. The latter two countries were selected by considering cost for the survey.
This study was granted by an institutional research ethics committee (Saitama Prefectural University, #24015), and all methods were performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants. Data were collected by survey companies via recruitment on the web among its monitors (the Japanese group was conducted by NEO MARKETING, INC., Tokyo, Japan, and the US and Singapore group was conducted by Cross-Marketing, Inc., Tokyo, Japan).
Participants
For the three groups, the same inclusion criteria were used: (1) those with subjective Katakori, and (2) age of 20–69 years.
For the US and Singapore groups, an online survey that was composed of 2 parts was conducted over 2 weeks in 2024. The first part of the survey asked for a Yes/No answer to the following question: “Do you have a nonspecific symptom including discomfort or dull pain around the occiput through the cervical spine to the acromion and scapular area?” In the second part, those who answered “yes” to the first part were invited to respond to the final version of the KDI. Data in the second part were not eligible to this study when (1) those who did not complete the survey, (2) those who provided an inadequate response to the dummy item in the KDI, and (3) those who have not done any activities in the KDI, resulting in no KDI score. The minimum sample size of valid data in the second part was estimated to be 100 from each country to satisfy the “very good” criterion in the COSMIN guideline (i.e., 7 times number of items and ≥ 100 participants per each group) for factor analysis. Therefore, they tried to collect eligible data of more than 10 male and female individuals of each age group (20’s, 30’s, 40’s, 50’s, and 60’s) for each country in the second part of the survey.
For the Japan group, data of the provisional KDI were collected for 2 weeks in 2022. As the same as the US and Singapore groups, data were not eligible to this study when (1) those who did not complete the survey, (2) those who provided an inadequate response to the dummy item in the KDI, and (3) those who have not done any activities in the KDI, resulting in no KDI score. The survey company tried to collect valid data from approximately 50 male and female individuals of each age group (20’s, 30’s, 40’s, 50’s, and 60’s)9. Finally, valid data from 515 participants (244 men and 271 women, mean [SD] age = 45.8 [13.9] years) were analyzed to create the final format of the KDI9, which was shared in the current study.
KDI
The KDI uses a semi-individualized format designed to allow comparison of conditions across individuals and to reflect the individuality of them. In this format, participants were asked to rate both the importance and their perception of the bothersomeness caused by Katakori on 11 items using a 6-point scale. In addition, to ensure that respondents are responding mindfully, one dummy item is included with instructions to put a specific number for importance and bothersomeness.
Participants are asked to recall their experience with Katakori over the past week and respond accordingly. The Importance scale consists of six categories: “not important at all” or “have not done at all over the past week”; 1, “not important”; 2, “not important so much”; 3, “slightly important”; 4, “important”; and 5, “extremely important.” The Bothersomeness due to Katakori is also rated on six categories: 0, “not bothersome at all”; 1, “not bothersome”; 2, “not bothersome so much”; 3, “slightly bothersome”; 4, “bothersome”; and 5, “extremely bothersome.” Items rated as “not important at all” or “have not done at all over the past week” in the Importance scale are excluded from further score calculations and treated as missing values.
The product of the Importance and Bothersomeness scores is calculated (i.e., 0, 1, 2, 3, 4, 5, 6, 8, 9, 10, 12, 15, 16, 20, and 25). These products are then transformed into a 15-point scale (0–14) in decreasing order (e.g., a product of 0 = 0, a product of 25 = 14). As a result, each item score is either a missing value or falls within the range of 0–14. Finally, the following formula is used to calculate a percentage score, where a higher score indicates a greater disability of Katakori on daily life.
Analysis
Cross-cultural validity was assessed using the MGCFA as suggested by the COSMIN guideline. The analysis was conducted using SPSS (Amos™ 20.0, NY, US). Data of the participant with a missing value of the KDI were excluded from the MGCFA because the MGCFA requires no missing data. Although the COSMIN guideline does not provide clear criteria for cross-cultural validity, since the KDI is a unidimensional PROM, the model fit of a configuration with no constraints on factor loadings or intercepts must first be acceptable (i.e., confirmation of configural invariance). Model fit was considered acceptable if the CFI was greater than 0.95 or the RMSEA was less than 0.08, as outlined by COSMIN. Once configural invariance was confirmed, cross-cultural validity was determined if there were no statistically significant differences when transitioning from the unconstrained model to the models shown in Table 317. In this study, considering criticisms that the evaluation by the MGCF is too strict, cross-cultural validity was deemed to exist if no statistically significant difference was found after changing to the partial metric invariance16. Since confirmatory factor analysis does not accommodate missing data, samples with missing values were excluded from the assessment of cross-cultural validity.
For the US and Singapore groups, the presence of Katakori was investigated from all data completed in the first part of the survey. Additionally, the internal consistency of the KDI in each country was assessed using Cronbach’s alpha by excluding data of the participant with missing values from valid data in the second part of the survey. The values were interpreted as follows: acceptable, ≥ 0.7; and not acceptable, < 0.718.
To investigate the scoring characteristics of the KDI, multiple comparisons of % KDI scores were performed using the Steel-Dwass method for: (1) the three countries, and (2) 30 groups divided by five age groups and gender. The analysis was conducted using JMP version 18 (SAS Institute Inc., SAS Campus Drive, Cary, North Carolina 27513, US) for the Steel-Dwass method and IBM SPSS Statistics for Windows version 28.0 (IBM Corp., Armonk, NY, US) for the other analyses, with a significance level set at 5%.
Data availability
All data generated or analyzed during this study are provided in Appendix 2.
References
Yabuki, S. Pathogenesis of the Neck-shoulder stiffness (Katakori). Rinsho Seikei Geka (Clinical Orthop. Surg.) 42, 413–417 (2007).
Takagishi, K. et al. Project study on Katakori (2004–2006). J. Jpn. Orthop. Assoc. 82, 901–911 (2008).
Japan Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions (2019). http://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/dl/04.pdf.
Yoshimoto, T., Oka, H., Fujii, T., Nagata, T. & Matsudaira, K. The economic burden of lost productivity due to presenteeism caused by health conditions among workers in Japan. J. Occup. Environ. Med. 62, 883–888 (2020).
The Committee for Clinical Practice Guideline for the Management of Chronic Pain. In Clinical Practice Guideline for Chronic Pain (Shinko Trading Company Ltd., 2021).
Aoki, K., Hall, T. & Takasaki, H. Reporting on the level of validity and reliability of questionnaires measuring Katakori severity: a systematic review. SAGE Open. Med. 7, 2050312119836617 (2019).
Takasaki, H. & Handa, Y. Initial development of a patient-reported outcome measure of disability due to Katakori via evaluating patient comprehensibility and comprehensiveness. J. Phys. Ther. Sci. 34, 13–17 (2022).
Natsume, K., Handa, Y. & Takasaki, H. Determination of the conceptual structures of the disturbed activities of daily living due to Katakori by evaluating patients’ values or perceptions using a patient-elicitation technique. J. Phys. Ther. Sci. 33, 683–688 (2021).
Takasaki, H. Developing a final format of a patient-reported outcome measure for disability in daily living due to stiff neck/shoulders, Katakori disability index, through internal structure assessments. Musculoskelet. Care 22, e1861 (2024).
Ishida, H. The existence of the disease concept of ‘katakori’ in Western countries. Japan Med. J. 3439, 132–133 (1990).
Kutsunugi, M. & Kuroiwa, M. Characteristics of Katakori as physical complaints among Japanese people-a comparison with neck pain in the Western countries. Japanese J. Mental Health 25, 61–66 (2010).
Tomoaki, T., Hiroyoshi, Y., Miho, T. & Nobuari, T. Reinvestigation of Katakori (neck/shoulder stiffness) in Japan: comparing with neck pain in the US. (2024). https://kaken.nii.ac.jp/report/KAKENHI-PROJECT-19K01233/19K012332022hokoku.
Kaida, A. Studies on cognition of illness. Bull. Nishogakusha Univ. 44, 37–57 (2001).
Katsumi, I., Masato, S. & Wayne, K. The research on shoulder discomfort.(2).The comparison of cause and coping behavior in Japan vs. United States. Japan Med. J. 1992, 27–30 (1992).
Kleinman, A., Eisenberg, L. & Good, B. Culture, illness, and care: clinical lessons from anthropologic and cross-cultural research. Ann. Intern. Med. 88, 251–258 (1978).
Manabe, K., Maeda, T. & Shimizu, K. Measurement equivalence/invariance in Cross-National/Cross-Cultural research: a review of the literature focusing on MGCFA. Kansai Gakuin Univ. School Sociol. J. 2021, 1–28 (2021).
Steenkamp, J. E. M. & Baumgartner, H. Assessing measurement invariance in Cross-National consumer research. J. Consum. Res. 25, 78–90 (1998).
Mokkink, L. B. et al. COSMIN risk of bias checklist for systematic reviews of patient-Reported outcome measures. Qual. Life Res. 27, 1171–1179 (2018).
Funding
This work has been funded by Saitama Prefectural University.
Author information
Authors and Affiliations
Contributions
H.T. contributed all.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Takasaki, H. The Katakori disability index has cross-cultural validity for disability due to stiff neck/shoulder across Japan, the US, and Singapore. Sci Rep 15, 12087 (2025). https://doi.org/10.1038/s41598-025-96449-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96449-x
