
Abstract
Anxiety, characterized by an unpleasant state of anticipatory unease, manifests in approximately 19% of adolescents and children within the Lebanese population. Given the major influence of traditional mindset and the stigma concerning mental health in Lebanon, children often express anxiety differently that can go unnoticed, and leading to underreported anxiety symptoms. Having a parental perspective in a collectivist culture is important. Lebanon is known to have a strong family-oriented culture where parents have an important role in shaping children’s emotional and psychological wellbeing. Therefore, the Spence Children’s Anxiety Scale-Parent (SCAS) might be an appropriate tool to aid in the identification of anxiety. This study aims to validate the SCAS-Parent in the Arabic language, assessing reliability, validity and consistency of the scale. This cross-sectional study enrolled 502 adult parents from all over Lebanon. The data was collected through a Google form and using snowball technique during November 2023. The questionnaire included sociodemographic data, the Brief version of the Spence Children’s Anxiety Scale for the Parents (SCAS-P- 8) and the Depression Anxiety Stress Scale (DASS- 8). A confirmatory factor analysis (CFA) was conducted; calculated fit indices were the normed model chi-square (χ²/df), the root mean square error of approximation (RMSEA), the standardized root mean square residual (SRMR), the Tucker-Lewis Index (TLI) and the comparative fit index (CFI). Values ≤ 5 for χ²/df, ≤ 0.08 for RMSEA, ≤ 0.05 for SRMR and ≥ 0.95 for CFI and TLI indicate good fit of the model to the data. CFA results indicated that fit of the one-factor model of the SCAS-P- 8 scale was acceptable: χ2/df = 84.53/20 = 4.23, RMSEA = 0.080 (90% CI 0.063, 0.098), SRMR = 0.035, CFI = 0.966, TLI = 0.952. The standardized estimates of factor loadings were all adequate. The reliability of the scale was good (ω = 0.90/α = 0.90). Higher parental depression (r = 0.61; p < 0.001), anxiety (r = 0.62; p < 0.001) and stress (r = 0.48; p < 0.001) were significantly associated with higher anxiety in the child. The study validates the SCAS-P- 8 for its application in the Lebanese population, demonstrating high internal consistency, reliability, and validity, indicating its potential as a screening tool for anxiety in children in the hands of psychologists and health-care professionals. Anxious parents will most likely have anxious children, leading to a vicious cycle. Early screening of anxiety in children can potentially impact the quality of life and developmental status of children. Additionally, assessing several aspects of anxiety can help prevent its long-term consequences that can affect academic performance, social relationships, and overall well-being.
Similar content being viewed by others


Introduction
Anxiety is an unpleasant, relatively common, state of unease that involves anticipating unpredictable dangers in response to certain situations. As per the Diagnostic and Statistical Manual of Mental Disorders – fifth edition (DSM- 5), anxiety disorders involve conditions characterized by heightened worry and associated symptoms such as muscle tension and irritability, occurring for 6 months period1. While the Diagnostic and Statistical Manual of Mental Disorders (DSM- 5) outlines diagnostic criteria for anxiety disorders, recognizing key traits can help clinicians identify anxiety in children and adolescents. Common features include hypervigilance, excessive sensitivity to threats, avoidant behaviors, physical complaints, extreme emotional responses, and the impact of parental accommodation2.
Anxiety disorders are one of the most common psychiatric diseases worldwide. Hence, a systematic review, in 2016, found that anxiety in adults ranged from 3.8 to 25%, varying greatly between ethnicities3. According to World Health Organization (WHO), there was a significant rise in anxiety disorders’ prevalence due to the repercussions of the COVID- 19 pandemic4. Specifically, more than 7% of adolescents between 13 and 17 years old, and 36% of children with behavioral issues were clinically diagnosed with anxiety worldwide4. Additionally, a review of multiple studies suggests a global prevalence of about 6.5% for anxiety disorders in children5.
In Lebanon, a study published in 2022 about mental health issues, in adolescents and children, found that 32.7% of children have a psychiatric disorder, but only 5% were professionally managed5. Additionally, the prevalence of anxiety was found to be 19% in the adolescent and children population. The age group comprising 8 till 11 years old had the highest rate with 23.3%, followed by the 12–17 years old age group with about 21.6%. According to this study, anxiety is more common in girls (27.41%) than boys (15.6%), and in children aged above 12 years old6.
Studies showed that most of the clinical presentations involving anxiety are exhibited by physical symptoms7,8. Children with anxiety presents somatic symptoms, the most observed ones include restlessness, abdominal pain, palpitations, along with sweating and trembling9. Moreover, it was noted that older children, aged 12 and above, tended to report greater complaints and feel more stressed than other pediatric groups. Indeed, children find it harder to verbalize and communicate the anxiety that they feel than older age groups, therefore, they resort to avoidant coping mechanisms leading to underdiagnosis in the pediatric population10.
It is worth noting that early diagnosis and intervention is key in children suffering from anxiety. Understanding the complex multifaceted conditions linked to the flourishing of anxiety prematurely will aid practitioners in managing and controlling long-term effects of anxiety on children’s lives11. Recent studies stated that the presence of anxiety significantly influences various aspects of children’s and adolescents’ lives, persistently impacting cognitive, behavioral, and social aspects, such as academic underachievement, diminished self-esteem and confidence and even the onset of depression and other psychiatric disorders.9,12,13.
It is important to note that children of parents with an anxiety disorder are four times more likely to experience anxiety compared to children whose parents do not have anxiety disorders14. Hence, investigations revealed that children tend to exaggerate the reception of threats and engage in avoidant behaviors after conversations with their anxious parents15. Previous theories have identified two primary ways through which parents can influence the development of anxiety in their children: modeling a fear response, where the child can imitate the parent’s anxious behavior in response to certain stimuli or situation, and overprotective behavior that may unintentionally hinder the child’s ability to cope with stress14. Theoretically, it was suggested that overprotective parents showed the world to be a harmful place preventing the child to acquire the necessary skills to cope with stressful situations in life10. Other studies showed that when parents exhibited both behaviors simultaneously, modeling a fear response and an overprotective behavior, it correlated with higher anxiety levels in their children14.
Anxiety is difficult to diagnose in the pediatric population for many reasons, but mostly, the denial of parents that their children can be suffering from mental health issues is the most incriminated cause of underdiagnosed cases16. The denial, as a defense mechanism, may be due to traditional cultural disbeliefs in anxiety disorders or even to ignorance; consequently, parents recognizing and communicating anxiety symptoms regarding their children can significantly aid clinicians in their determination to conduct a more comprehensive and thorough assessment. Hence, it is important and logical to get the point of views of both parents and children concerning the child’s anxiety17.
There are several screening scales for children’s anxiety, containing both the child’s and the parent’s versions, among them: the Screen for Child Anxiety Related Emotional Disorders (SCARED), the Multidimensional Anxiety Scale for Children (MASC), and the Spence Children’s Anxiety Scale (SCAS). The SCARED examines five subscales: generalized anxiety, separation anxiety, social anxiety, panic or somatic symptoms, and school avoidance18. As for the MASC, it has four subscales: physical symptoms, harm avoidance, social anxiety, and separation/panic19.
The Spence Children’s Anxiety Scale (SCAS) that is translated to at least 22 languages20, was seen to be suitable for assessing anxiety disorder symptoms in adolescents in Germany, United Kingdom, Cyprus, Sweden, and in Italy21. The child’s version SCAS-C operates as a self-report tool designed to assess anxiety symptoms in children aged between 8 and 15 years old. It has 44 items targeting several aspects of anxiety, mainly separation anxiety disorder, social phobia, obsessive-compulsive disorder, panic attack and agoraphobia, physical injury fears, and generalized anxiety disorder. Each item requires the child to rate the frequency of experiencing the indicated symptom on a four-point Likert scale, spanning from ‘never’ (0) to ‘always’ (3). The Parent version (SCAS-P), translated to at least 25 languages22, comprises 38 items, filled by the parent of the children in question, aligning with the structure of the child version. Compared to SCARED, SCAS is shorter and more direct23, and addresses a more extensive array of anxiety disorders. In addition, there are variations in the content of subscales, including those targeting symptoms of the same anxiety disorder. For example, while all items in the SCARED’s generalized anxiety disorder subscale focus on worry symptoms, the SCAS’s subscale allocates half of its items to physical symptoms24, which is important in our case where, as mentioned before, most of the children’s anxiety presentation is physical in nature. No studies to this time compared all three scales (SCAS, SCARED, MASC).
Mental health problems in the Arab world are driven by stigma, viewing mental health care as less important than physical health, and outdated healthcare systems that don’t meet current needs25. These issues are made worse by war28, economic struggles and the reluctance to talk about or treat mental health. Therefore, it is important to have a validation of the SCAS-P in the Arabic language specific to Arabic speaking countries, which are culturally and socially different from Western countries.
The SCAS-P, according to previous studies, is valid and reliable in assessing the parent’s perception of their children’s anxiety18. A previous study12 showed that it achieved an overall correct classification rate of approximately half of the children, demonstrating notable accuracy in identifying separation anxiety, social phobia, panic/agoraphobia, and obsessive–compulsive disorder. It also showed good convergent validity and internal reliability and had the ability to differentiate between healthy and anxious children17.
A short form was developed, consisting of 8 items13, designed to assess social anxiety, separation anxiety, panic/agoraphobia and generalized anxiety, and it was translated to different languages including Spanish26, English and Ecuadorian13. With a score between 0 and 24, the SCAS-P- 8 showed strong psychometric characteristics, featuring invariance across gender, a satisfactory level of internal consistency indicated by a coefficient alpha (α) of 0.82.
The present study
Lebanon has navigated through a series of economic and health crises, blasts, refugees and recently wars, in addition to the heavy impact of inflation and unemployment on parents27. This created an environment where adults struggle with uncontrollable levels of stress and anxiety. On their side, children are exposed to these factors plus family conflicts that could result from economic pressures, as well as academic and social media pressures27–29. Recognizing and dealing with anxiety among children, as well as understanding parental perceptions of it in Lebanon is crucial, yielding the need of Arabic translation and validation of the SCAS-Parent. The SCAS-P- 8 provides a cost-effective, efficient, and reliable way to assess anxiety in children and adolescents. This tool is essential for early intervention and ongoing mental health monitoring. The SCAS-P- 8 is particularly valuable in situations without adequate resources that require quick screenings30, ensuring children get the right care based on accurate and comprehensive information. Ultimately, it guarantees that mental health care in Lebanon is based on valid tools tailored to the local context, improving outcomes for children with anxiety31. On the other hand, DASS- 8 was used to assess depression, anxiety and stress in parents. Its use is particularly relevant in Lebanon for multiple of reasons. First, we know from previous studies that Parental mental health is directly correlated with anxiety in children32, which is why this measure was chosen for concurrent validity in the present study. Secondly, due to the financial instability, social pressure, educational expectations, Lebanese parents may experience high stress. Therefore, DASS- 8 may be more adapted than the original version developed in Western countries31. Thirdly, this tool, unlike DASS- 21, is time efficient and can maintain psychometric strength with fewer items and is a more logical choice than longer versions33.
This study aims to examine the psychometric properties of the SCAS-Parent (Spence Children’s Anxiety Scale), thus, assessing its reliability and validity, investigating its structure for consistency, and establishing evidence supporting its use as a valid measurement tool for assessing childhood anxiety in a parent-report format in Lebanon. We expect that the Arabic SCAS-Parent version would replicate the original one factor structure of the scale, have high internal consistency and be invariant across sex. In addition, we anticipate that children with anxiety disorders are likely to have parents experiencing the same ailment, i.e. that high depression and anxiety in parents are correlated with higher anxiety among children.
Methods
Procedures
During November 2023, data for this cross-sectional study was collected through a Google Form link. The research team first invited a small number of people who fit the criteria for the study to complete the survey; these participants were chosen based on their knowledge and involvement in the research topic. After involving these initial participants, the research team asked them to refer to others who meet the study’s criteria. This process continued, with each new participant potentially referring to more individuals and sharing the link with them, following the snowball sampling technique. Participants were invited via social media applications (WhatsApp, Instagram, Messenger). Noting that the snowball sampling was chosen because it effectively helps researchers access hard-to-reach or hidden populations, despite its potential for bias and lack of generalizability.
The research team tried to include those participants from all governorates of the country. Inclusion criteria comprised being an adult (aged 18 and above) who resides in and is a citizen of Lebanon and who has a child aged between 7 and 13 years. Exclusions encompassed individuals declining to complete the questionnaire. The survey was conducted anonymously, and participation was voluntary and without compensation.
Translation procedure
Prior to utilization in the current study, permission to translate and validate the SCAS-P scale was obtained from Pr. Susan Spence. The scale underwent translation for adaptation for the Arabic language and cultural context. The translation aimed to attain semantic equivalence between the original measures and their Arabic counterparts, adhering to international recommendations34. A Lebanese translator, unaffiliated with the study, independently translated the English version into Arabic. Following that, a Lebanese psychologist, proficient in English, translated the Arabic version back into English. To ensure accuracy, a committee of experts, comprising two psychiatrists, one psychologist, and the research team, compared the original and translated English versions, identifying and correcting any inconsistencies35. Following this, a pilot study involving 20 participants was conducted to validate the clarity of all questions. No modifications were made after the completion of the pilot study.
Minimum sample size
A minimum sample varying between 39 and 260 participants was deemed necessary to conduct a confirmatory factor analysis following a recommendation between 3 and 20 times the number of the scale’s variables36.
Measures
We first asked about sociodemographic information, including age, sex (males/females), education level (secondary or less/university) and socioeconomic status (reflected by the household crowding index, which is calculated by dividing the number of persons by that of the rooms in the house except the kitchen and bathrooms)37.
The Brief version of the Spence Children’s anxiety Scale for the Parents (SCAS-P- 8). It is a short form consisting of eight items with an aim to evaluate the parent’s perception of the children’s anxiety20. It assesses several aspects of anxiety: two items for social anxiety, two for separation anxiety, one for panic/agoraphobia, and three for generalized anxiety. The response is noted using the four-point scale (0–3; never-always) with a total score between 0 and 24. Higher scores indicates higher child anxiety.
Depression Anxiety Stress Scale (DASS- 8)31, validated in Arabic38, is designed to provide a more concise evaluation of symptoms related to depression, anxiety and stress. It consists of 8 items divided into three subscales: depression (3 items), anxiety (3 items), and stress (2 items). Participants rate the extent to which they have experienced each symptom during the week using a 4-point Likert scale (0 = Not applicable at all to me 3 = Very applicable or most of the time). Higher scores equate to a higher level of symptom affirmation.
Analytic strategy
There were no missing responses in the dataset. To examine the factor structure of the SCAS-P- 8, we used FACTOR 12.04.0139 to perform the Exploratory Factor Analysis (EFA) and the SPSS AMOS v.29 program to carry out the Confirmatory Factor Analysis (CFA). For this purpose, we randomly divided the sample into two subsamples using the SPSS random sample of cases option. We carried out an EFA in the first subsample, made up of 33% (1/3) of the total sample (170 subjects), and a CFA in the second subsample (332 subjects). To check that the data was suitable for EFA we used KMO and Bartlett’s test of sphericity. A preliminary analysis of the items was conducted using the Measure of Sampling Adequacy (MSA) at the item level [2], with values below 0.50 leading to item elimination40. The exploratory factor analysis was carried out with a polychoric correlation matrix given the ordinal nature of the variables41. The method of estimation was Unweighted Least Squares (ULS), following international recommendations42. We determined the number of factors using the Optimal Implementation of Parallel Analysis (PA) procedure43,44.
Subsequently, to confirm the dimensionality indicated by the EFA, we performed a CFA with the remaining 66% (2/3) of the sample based on the factor structure obtained from the EFA. Parameter estimates were obtained using the maximum likelihood method. Calculated fit indices were the normed model chi-square (χ²/df), the root mean square error of approximation (RMSEA), the standardized root mean square residual (SRMR), the Tucker-Lewis Index (TLI) and the comparative fit index (CFI). Values ≤ 5 for χ²/df, ≤ 0.08 for RMSEA, ≤ 0.05 for SRMR and ≥ 0.95 for CFI and TLI indicate good fit of the model to the data45. Multivariate normality was not verified at first (Bollen-Stine p = 0.018); therefore, we performed non-parametric bootstrapping procedure.
To examine sex invariance of SCAS-P- 8 scores, we conducted multi-group CFA46, using the total sample. Measurement invariance was assessed at the configural, metric, and scalar levels47. We accepted ΔCFI ≤ 0.010 and ΔRMSEA ≤ 0.015 or ΔSRMR ≤ 0.010 as evidence of invariance48. Comparison between males and females was done using the Student t-test only if scalar or partial scalar invariance.
Composite reliability was assessed using McDonald’s ω and Cronbach’s alpha, with values greater than 0.70 reflecting adequate composite reliability. Normality of the SCAS-P- 8 score was verified since the skewness and kurtosis values for each item of the scale varied between − 1 and + 145. To assess convergent and concurrent validity, a linear regression was conducted taking the SCAS-P- 8 as the dependent variable. Standardized Beta values between 0.10 and 0.30 were classified as small effect size, between 0.30 and 0.50 as medium effect size and ≥ 0.50 as large effect size respectively49.
Results
Description of the sample
Five hundred two parents filled the survey, with a mean age of 36.24 ± 8.29 years, 74.5% females, 72.9% with a university level of education and a mean household crowding index of 1.09 ± 0.44 person/room. The description of each item of the SCAS- 8-P and DASS- 8 scales’ items are found in Table 1.
Exploratory factor analysis of the SCAS- 8-P (subsample 1)
The KMO test and Bartlett’s test values confirmed the suitability of the data for analysis (KMO = 0.896; Bartlett’s statistic = 1146.4, df = 28; p < 0.001). None of the items was suggested to be removed based on the MSA values, with values greater than 0.50 for all items. Results indicated an adequate fit to a unidimensional structure as suggested by the parallel analysis, which explained 71.80% of the variance. Results were supported by the GFI (GFI = 0.99) being greater than 0.95, the UniCo (UniCo = 0.98) index greater than 0.95, the I-ECV (I-ECV = 0.92) greater than 0.85 and MIREAL (MIREAL = 0.19) lower than 0.30. The reliability was excellent (ω = 0.92 [95% CI 0.90; 0.94]; α = 0.92 [95% CI 0.90; 0.94]).
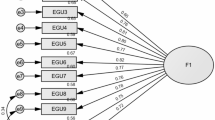
Confirmatory factor analysis of the SCAS- 8-P (subsample 2)
CFA indicated that fit of the one-factor model of the SCAS- 8-P scale obtained from the EFA analysis was acceptable: χ2/df = 65.61/20 = 3.28, RMSEA = 0.083 (90% CI 0.061, 0.106), SRMR = 0.041, CFI = 0.959, TLI = 0.943. The standardized estimates of factor loadings were all adequate (≥ 0.4) (Table 2), which indicates that the items in the scale are all related to the underlying factor they are intended to measure (anxiety in children). The AVE was borderline (= 0.49). The reliability of the SCAS-P- 8 scale was good (ω = 0.89 [95% CI 0.86; 0.90]/α = 0.88 [95% CI 0.86; 0.90]).
Sex invariance of the SCAS- 8-P scale (total sample)
We were able to show the invariance across sex at the configural, metric, and scalar levels (Table 3). No significant difference in terms of anxiety was found between fathers and mothers (8.07 ± 6.01 vs. 7.03 ± 5.27, t(500) = 1.74, p = 0.084, Cohen’s d = 0.190 [95% CI − 0.011; 0.391]).
This is important in the validation of the SCAS-P, it proves that it can be used for both genders equally, no gender is superior to its counterpart. the scale functions similarly for both boys and girls, making it a fair and unbiased tool for evaluating anxiety symptoms across sexes. This ensures that any differences in anxiety scores are not due to the scale itself, but rather reflect actual differences in anxiety levels.
Convergent and concurrent validity of the SCAS scale
The results of the linear regression, taking anxiety in the child as the dependent variable, were adjusted over the following variables: age, gender, education level and household crowding index of the parents. Results showed that higher depression (Beta = 0.68) and anxiety (Beta = 0.78) in parents were significantly associated with higher anxiety in the child (Table 4).
Discussion
Our study sought to examine the psychometric properties of a parent-reported scale designed to capture children’s anxiety. Our results suggested that the SCAS-P has appropriate psychometric properties and can be considered valid and reliable in Lebanese parents. Findings of the confirmatory factor analysis of the SCAS-P verified that the one factor model of the scale was acceptable. The unidimensional model demonstrated good internal consistency and validity in our sample. Our results also showed its invariance across sex and established the concurrent validity of the instrument.
First, our study indicated a one-factor model form which is consistent with the Spanish18 brief version of the SCAS-P and SCAS50. The fit indices of the one-factor model were good, except for the RMSEA value (= 0.083) that was slightly higher than the limit (= 0.080). However, these cut-off values should not be interpreted rigidly51,52 and values between 0.08 and 0.10 for RMSEA can indicate acceptable but mediocre fit to the data53. In contrast, a study conducted in China using the short version of the SCAS found that the five-factor model was more adequate54.
Second, the results of our study showed a good internal consistency (ω = 0.90/α = 0.90), in congruence to a previous study conducted in China, where the brief questionnaire scores displayed acceptable to good internal consistency α = 0.8555, and in other findings where the SCAS-Short version was given for a sample of Chinese children and their mothers to fill (α = 0.84)54. As for the results of the SCAS-P- 8 validation in Ecuador, the same can be applicable where it showed a reasonable internal consistency of 0.8519.
Third, our study showed sex invariance in the measurement properties of the SCAS-P at the configural, metric, and scalar levels, which is consistent with previous studies.21,50 This suggests that the SCAS measures anxiety manifestations in a consistent and unbiased way across sex in Lebanon, which is consistent with the results of previous studies13,21, 50. In contrast, a recent investigation in Mainland China suggested that the variations in anxiety levels between genders, assessed by SCAS and SCAS-P, might be more important, with girls having higher anxiety levels than boys, and that the gender difference is more noticeable during adolescence than in childhood56.
Lebanon has been going through difficult times, ranging from economic crises, explosions and most recently a devastating war57. Recent studies showed that more than 82% of the Lebanese residents live in poverty. This has impacted the citizens’ mental health greatly, with a frightening increase in suicide rates. Lebanese individuals face an elevated risk of poor health due to the psychological stressors they have endured over the past few years58. Previous research in Lebanon showed an increased risk of mental health disorder with the increase exposure to wars59. As this situation can affect adults, children and young adults are also at risk of developing psychological issues. Negative childhood experiences elevate the risk of developing late onset psychiatric disorders, such as anxiety in different ways. In some cultures, psychological terms to describe anxiety and depression are explicitly used. In other cultures, the subject is more of a stigma and people usually describe somatic symptoms like headaches or abdominal pain instead of expressing anxiety concerns. Also, parenting style has a heavy impact on the ways children express anxiety symptoms. Parents that are overprotective and exercise rejection are associated with more anxiety in all cultures, particularly Caucasians. Also, a study found that Asian adolescents reported higher anxiety than their European counterparts60. On the other hand, cultural values play a role in shaping anxiety in children. A culture that is more open to expression and individuality can offer protective factors for anxiety in contrast with cultures of conformity where we find more internalized anxiety in children61.
Beyond the measurement properties of the scale, higher parental depression was found to be moderately associated with higher anxiety levels in the child, which is in concurrence with other findings21,50, where parents’ depression had a strong correlation with children’s psychological and behavioral problems. Furthermore, depression of parents, with earlier onset and longer duration, is correlated with higher levels of anxiety, and increased internalizing and externalizing symptoms62. In addition, a recent longitudinal study showed an important association between maternal depression and anxiety development in children63. This highlights the influential role of parental mental health on the psychological well-being of the child. Several factors such as marital conflicts, sibling rivalry or parent-child conflicts within the household may contribute to the atmosphere of negative energy and anxiety in the children64,65.
In addition to parental depression and stress, we concluded a moderate association between parental anxiety and increased anxiety in children, a result that was highlighted by previous studies15,21,26. Parental anxiety may serve as a model for the child, shaping their own anxious tendencies66. For example, an anxious parent may unconsciously transmit the sense of threat or danger to the child, leading to a biased perception of the world67.
Clinical implications
It is important to tackle the issue of anxiety in children, as it can go unrecognized or misunderstood. It can manifest itself as behavioral problems or social difficulties. As healthcare professionals, this anxiety scale can help in early detection and intervention. Additionally, since children with anxiety can have comorbid conditions such as ADHD or depression, it can help with early recognition and adequate treatment plans. For example, assessing anxiety in children can be done during regular doctor’s visits, after traumatic events (bullying, death…) or in the presence of physical symptoms without medical cause after investigations. As our study is the first to aim for the validation of the SCAS-P in Arabic, it is important to develop and validate scales that are culturally appropriate, due to the presence of different socio-economic backgrounds and ethnics groups. Also, researchers are strongly encouraged to carry out studies to screen for anxiety in different age groups, especially younger children. In addition, more studies are needed to assess anxiety in children with developmental disabilities or delays. Finally, with the advancement of technology, studies should explore the effectiveness of digital and online versions of anxiety scales that can provide real time feedback, self-assessments, and easy tracking over time.
Limitations
While our study aimed to validate the Arabic Spence Children’s Anxiety Scale-Parent Version, which is the first study of its kind, it is important to acknowledge certain setbacks that may impact the interpretation of our findings. Firstly, the investigation of the parent reporting anxiety of the child is based on the accuracy of measuring instruments, therefore there might be a possibility of a biased and subjective response. Secondly, the lack of results regarding the child and parent relationship limits our understanding of how it can impact the child’s anxiety. Thirdly, the study did not identify the presence or absence of the influence of socioeconomic factors and parental education levels. There are some limitations (selection bias) pertaining to the snowball sampling technique followed during the recruitment process via the Google forms, particularly the potential for bias due to the non-random selection of participants. Moreover, the lack of random sampling and potential measurement bias limit the generalizability of the results; future studies should employ random sampling methods to improve representativeness. Some psychometric properties were not assessed, such as the test-retest reliability. Furthermore, researchers have less control over the sample composition and size, which would make the findings not generalizable to the broader population as the sample is not randomly selected. Add to this that the lack of direct child assessment of anxiety and the unknown refusal rate of participants. Finally, there are no results regarding age invariance in children in the Spence Children’s Anxiety Scale-Parent Version, which elicits prudence in generalizing the scale’s applicability across different age groups. These limitations highlight the need for further precise studies to enhance the scale’s reliability and utility.
Conclusion
In summary, the SCAS-P was successfully translated into the Arabic language and demonstrated satisfactory psychometric properties when applied to a clinical sample in Lebanon. This tool is essential for clinical practice, offering the potential to impact over 22 countries and 360 million Arabic speakers. Its adoption could greatly enhance mental health assessments and support better care across Arabic-speaking communities. These results suggest its effectiveness as a tool for screening anxiety in children by psychologists and healthcare providers. Since children of anxious parents are more likely to experience anxiety themselves, early detection can help disrupt this cycle. Identifying anxiety in children at an early stage can positively influence their overall well-being, helping them learn healthy coping strategies and improve their emotional state. Also, early intervention can shape future decisions, and influence developmental progress, ultimately contributing to healthier mental and emotional growth. Future studies should aim at validating the scale in other Arabic-speaking countries, exploring multi-factor models, and investigating age invariance.
Data availability
All data generated or analyzed during this study are not publicly available due the restrictions from the ethics committee. Reasonable requests can be addressed to the corresponding author (SH).
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th edn (American Psychiatric Association, 2013).
Chiu, A., Falk, A. & Walkup, J. T. Anxiety disorders among children and adolescents. FOCUS 14 (1), 26–33. https://doi.org/10.1176/appi.focus.201500 (2016).
Remes, O., Brayne, C., van der Linde, R. & Lafortune, L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 6 (7), e00497. https://doi.org/10.1002/brb3.497 (2016).
https://www.who.int/news-room/fact-sheets/detail/anxiety-disorders
Kowalchuk, A., Gonzalez, S. J. & Zoorob, R. J. Anxiety disorders in children and adolescents. Am. Fam Physician. 106 (6), 657–664 (2022). PMID: 36521463.
Maalouf, F. T. et al. Psychopathology in children and adolescents in Lebanon study (PALS): a National household survey. Soc. Psychiatry Psychiatr Epidemiol. 57, 761–774. https://doi.org/10.1007/s00127-021-02208-4 (2022).
Henningsen, P., Zimmermann, T. & Sattel, H. Medically unexplained physical symptoms, anxiety, and depression: a meta-analytic review. Psychosom. Med. 65 (4), 528–533 (2003).
Larson, G. E., Booth-Kewley, S., Merrill, L. L. & Stander, V. A. Physical symptoms as indicators of depression and anxiety. Mil. Med. 166 (9), 796–799 (2001).
Racine, N. et al. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. 175 (11), 1142–1150 (2021).
Emslie, G. J. Pediatric anxiety–underrecognized and undertreated. N Engl J Med. 359(26), 2835-2836. (2008). https://doi.org/10.1056/NEJMe0809401. PMID: 19109579.
Haig-Ferguson, A., Cooper, K., Cartwright, E., Loades, M. E. & Daniels, J. Practitioner review: health anxiety in children and young people in the context of the COVID-19 pandemic. Behav. Cogn. Psychother. 49 (2), 129–143 (2021).
Mohammadi, M. R. et al. Prevalence, comorbidity and predictors of anxiety disorders among children and adolescents. Asian J. Psychiatry. 102059 https://doi.org/10.1016/j.ajp.2020.102059 (2020).
Orgilés, M., Galán-Luque, T., Hervás, D., Idrobo, A. & Morales, A. A brief parent version of the spence children’s anxiety scale (SCAS-P-8): factor structure, reliability, and invariance in Ecuadorian children. Revista Latinoam. De Psicología. 55, 227–235 (2023).
Emerson, L. M., Ogielda, C. & Rowse, G. A systematic review of the role of parents in the development of anxious cognitions in children. J. Anxiety Disord. https://doi.org/10.1016/j.janxdis.2018.11.002 (2018).
Burstein, M. & Ginsburg, G. S. The effect of parental modeling of anxious behaviors and cognitions in school-aged children: an experimental pilot study. Behav. Res. Ther. 48 (6), 506–515. https://doi.org/10.1016/j.brat.2010.02.006 (2010).
Teagle, S. E. Parental problem recognition and child mental health service use. Ment. Health Serv. Res. 4, 257–266 (2002).
Nauta, M. H. et al. A parent-report measure of children’s anxiety: psychometric properties and comparison with child-report in a clinic and normal sample. Behav. Res. Ther. 42 (7), 813–839. https://doi.org/10.1016/s0005-7967(03)00200-6 (2004).
Birmaher, B. et al. The screen for child anxiety related emotional disorders (SCARED): scale construction and psychometric characteristcis. J. Am. Acad. Child. Adolesc. Psychiatry. 36, 545–553 (1997).
Behrens, B., Swetlitz, C., Pine, D. S. & Pagliaccio, D. The screen for child anxiety related emotional disorders (SCARED): informant discrepancy, measurement invariance, and Test-Retest reliability. Child. Psychiatry Hum. Dev. 50 (3), 473–482. https://doi.org/10.1007/s10578-018-0854-0 (2019). PMID: 30460424; PMCID: PMC7339086.
Ahlen, J., Vigerland, S. & Ghaderi, A. Development of the spence children’s anxiety Scale - Short version (SCAS-S). J. Psychopathol. Behav. Assess. 40 (2), 288–304. https://doi.org/10.1007/s10862-017-9637-3 (2018). Epub 2017 Nov 21. PMID: 29937623; PMCID: PMC5978831.
Essau, C. A., Sasagawa, S., Anastassiou-Hadjicharalambous, X., Guzmán, B. O. & Ollendick, T. H. Psychometric properties of the spence child anxiety scale with adolescents from five European countries. J. Anxiety Disord. 25 (1), 19–27 (2011). Epub 2010 Jul 13. PMID: 20685072.
Peter Muris, H., Schmidt, H. & Merckelbach Correlations among two self-report questionnaires for measuring DSM-defined anxiety disorder symptoms in children: the Screen for Child Anxiety Related Emotional Disorders and the Spence Children’s Anxiety Scale, Personality and Individual Differences, Volume 28, Issue 2, Pages 333–346, ISSN 0191–8869, (2000). https://doi.org/10.1016/S0191-8869(99)00102-6
Muris, P., Merckelbach, H., Ollendick, T., King, N. & Bogie, N. Three traditional and three new childhood anxiety questionnaires: their reliability and validity in a normal adolescent sample. Behav Res Ther. 40(7), 753 – 772. (2002). https://doi.org/10.1016/s0005-7967(01)00056-0. PMID: 12074371.
Khatib, H. E., Alyafei, A. & Shaikh, M. Understanding experiences of mental health help-seeking in Arab populations around the world: a systematic review and narrative synthesis. BMC Psychiatry. 23 (1), 324 (2023).
Orgiles, M., Morales, A., Espada, J. P. & Rodriguez-Menchon, M. Early detection of anxiety problems in childhood: Spanish validation of the brief spence children’s anxiety scale for parents. Clin. Child Psychol. Psychiatry. 27 (3), 836–851 (2022).
El Zouki, C. J., Chahine, A., Mhanna, M., Obeid, S. & Hallit, S. Rate and correlates of post-traumatic stress disorder (PTSD) following the Beirut blast and the economic crisis among Lebanese university students: a cross-sectional study. BMC Psychiatry. 22 (1), 532 (2022).
Obeid, S. et al. Factors associated with depression among the Lebanese population: results of a cross-sectional study. Perspect. Psychiatr. Care. 56 (4), 956–967 (2020).
Mhanna, M., El Zouki, C.-J., Chahine, A., Obeid, S. & Hallit, S. Dissociative experiences among Lebanese university students: association with mental health issues, the economic crisis, the COVID-19 pandemic, and the Beirut Port explosion. Plos One 17(11), e0277883. https://doi.org/10.1371/journal.pone.0277883 (2022).
Orgilés, M., Rodríguez-Menchón, M., Fernández-Martínez, I., Morales, A. & Espada, J. P. Validation of the parent report version of the spence children’s anxiety scale (SCAS-P) for Spanish children. Clin. Child Psychol. Psychiatry. 24 (4), 776–790 (2019).
Ali, A. M., Alkhamees, A. A., Hori, H., Kim, Y. & Kunugi, H. The depression anxiety stress scale 21: development and validation of the depression anxiety stress scale 8-Item in psychiatric patients and the general public for easier mental health measurement in a post COVID-19 world. Int. J. Environ. Res. Public Health. 18 (19), 10142 (2021).
Michals, S. & Reeder, K. Parental mental health impacts a child’s Well-being: Parent-focused interventions can help. J. Student Res. 12 (3). https://doi.org/10.47611/jsrhs.v12i3.4608 (2023).
Amira, M. et al. The depression anxiety stress scale 8: investigating its cutoff scores in relevance to loneliness and burnout among dementia family caregivers, 14 April 2023, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-2790618/v1]
Van Widenfelt, B. M., Treffers, P. D., de Beurs, E., Siebelink, B. M. & Koudijs, E. Translation and cross-cultural adaptation of assessment instruments used in psychological research with children and families. Clin. Child. Family Psychol. Rev. 8(2), 135–147. https://doi.org/10.1007/s10567-005-4752-1 (2005).
Ambuehl, B. & Inauen, J. Contextualized measurement scale adaptation: A 4-Step tutorial for health psychology research. Int. J. Environ. Res. Public Health. 19 (19), 12775 (2022).
Mundfrom, D. J., Shaw, D. G. & Ke, T. L. Minimum sample size recommendations for conducting factor analyses. Int. J. Test. 5 (2), 159–168 (2005).
Melki, I. S. et al. Household crowding index: a correlate of socioeconomic status and inter-pregnancy spacing in an urban setting. J. Epidemiol. Community Health. 58 (6), 476–480. https://doi.org/10.1136/jech.2003.012690 (2004).
Ali, A. M. et al. The Depression Anxiety Stress Scale 8: investigating its cutoff scores in relevance to loneliness and burnout among dementia family caregivers. Sci. Rep. 14(1), 13075. https://doi.org/10.1038/s41598-024-60127-1 (2024).
Lorenzo-Seva, U. & Ferrando, P. J. A Simulation-Based scaled test statistic for assessing Model-Data fit in Least-Squares unrestricted Factor-Analysis solutions. Methodology 19 (2), 96–115 (2023).
Kaiser, H. F. & Rice, J. Little Jiffy, mark IV. Educ. Psychol. Meas. 34 (1), 111–117 (1974).
Muthén, B. & Kaplan, D. A comparison of some methodologies for the factor analysis of non-normal likert variables. Br. J. Math. Stat. Psychol. 38 (2), 171–189 (1985).
Lloret-Segura, S., Ferreres-Traver, A., Hernandez-Baeza, A. & Tomas-Marco, I. Exploratory item factor analysis: A practical guide revised and updated. Anales De Psicología. 30 (3), 1151–1169 (2014).
Timmerman, M. E. & Lorenzo-Seva, U. Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol. Methods. 16 (2), 209 (2011).
Calderón Garrido, C., Navarro González, D., Lorenzo Seva, U. & Ferrando Piera, P. J. Multidimensional or essentially unidimensional? A multi-faceted factoranalytic approach for assessing the dimensionality of tests and items. Psicothema (2019).
Hair, J. F. Jr, Sarstedt, M., Ringle, C. M. & Gudergan, S. P. Advanced Issues in Partial Least Squares Structural Equation Modeling (saGe, 2017).
Chen, F. F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equation Modeling: Multidisciplinary J. 14 (3), 464–504 (2007).
Vadenberg, R. & Lance, C. A review and synthesis of the measurement in variance literature: suggestions, practices, and recommendations for organizational research. Organ. Res. Methods. 3, 4–70 (2000).
Swami, V. et al. Psychometric properties of an Arabic translation of the functionality appreciation scale (FAS) in Lebanese adults. Body Image. 42, 361–369. https://doi.org/10.1016/j.bodyim.2022.07.008 (2022).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences 2nd edn (Lawrence Erlbaum Associates,, 1988).
Rodríguez-Menchón, M., Orgilés, M., Espada, J. P. & Morales, A. Validation of the brief version of the spence children’s anxiety scale for Spanish children (SCAS-C-8). J. Clin. Psychol. 78 (6), 1093–1102. https://doi.org/10.1002/jclp.23263 (2022). Epub 2021 Oct 18. PMID: 34661915.
Heene, M., Hilbert, S., Draxler, C., Ziegler, M. & Bühner, M. Masking misfit in confirmatory factor analysis by increasing unique variances: a cautionary note on the usefulness of cutoff values of fit indices. Psychol. Methods. 16 (3), 319–336. https://doi.org/10.1037/a0024917 (2011).
Perry, J. L., Nicholls, A. R., Clough, P. J. & Crust, L. Assessing model fit: caveats and recommendations for confirmatory factor analysis and exploratory structural equation modeling. Meas. Phys. Educ. Exerc. Sci. 19 (1), 12–21. https://doi.org/10.1080/1091367X.2014.952370 (2015).
Hooper, D., Coughlan, J. & Mullen, M. R. Structural Equation Modelling: Guidelines for Determining Model Fit. The Electronic Journal of Business Research Methods Volume 6 Issue 1 2008, pp. 53–60, available online at www.ejbrm.com.
Gong, J. et al. Measurement invariance and psychometric properties of the spence children’s anxiety scale-short version (SCAS-S) in Chinese students. Curr. Psychol. 42, 9312–9323. https://doi.org/10.1007/s12144-021-02237-x (2023).
Reardon, T., Spence, S. H., Hesse, J., Shakir, A. & Creswell, C. Identifying children with anxiety disorders using brief versions of the spence children’s anxiety scale for children, parents, and teachers. Psychol. Assess. 30 (10), 1342–1355. https://doi.org/10.1037/pas0000570 (2018). Epub 2018 Jun 14. PMID: 29902050; PMCID: PMC6179143.
Zhao, J., Xing, X. & Wang, M. Psychometric properties of the Spence Children’s Anxiety Scale (SCAS) in Mainland Chinese children and adolescents. J Anxiety Disord. ;26(7):728 – 36. (2012). https://doi.org/10.1016/j.janxdis.2012.05.006. Epub 2012 Jun 23. PMID: 22858899.
Farran, N. Mental health in Lebanon: tomorrow’s silent epidemic. Ment Health Prev. 24, 200218. https://doi.org/10.1016/j.mhp.2021.200218 (2021). Epub 2021 Sep 24. PMID: 34660191; PMCID: PMC8503814.
Jaspal, R., Assi, M. & Maatouk, I. Potential impact of the COVID-19 pandemic on mental health outcomes in societies with economic and political instability: case of Lebanon. Mental Health Rev. J. 25 No (3), 215–219. https://doi.org/10.1108/MHRJ-05-2020-0027 (2020).
Karam, E. et al. Textbook of Global Mental Health: Trauma and Recovery219 (A Companion Guide for Field and Clinical Care of Traumatized People Worldwide, 2011). Mental Health Lessons Learned from the Lebanon War Studies (1989 to 2007).
Mousavi, S. E., Low, W. Y. & Hashim, A. H. Perceived parenting styles and cultural influences in adolescent’s anxiety: A Cross-Cultural comparison. J. Child. Fam Stud. 25, 2102–2110. https://doi.org/10.1007/s10826-016-0393-x (2016).
Essau, C. A., Anastassiou-Hadjicharalambous, X., Demetriou, C. & Pourseied, K. Cultural factors and anxiety in children and adolescents: implications for treatment. In The Wiley-Blackwell Handbook of the Treatment of Childhood and Adolescent Anxiety (157–175). (The Wiley-Blackwell Handbook of the Treatment of Childhood and Adolescent Anxiety). Wiley. https://doi.org/10.1002/9781118315088.ch8. (2012).
National Research Council (US) and Institute of Medicine (US) Committee on Depression, Parenting Practices, and the Healthy Development of Children; England MJ, Sim LJ, editors. Depression in Parents, Parenting, and Children: Opportunities to Improve Identification, Treatment, and Prevention. Washington (DC): National Academies Press (US). 4, Associations Between Depression in Parents and Parenting, Child Health, and Child Psychological Functioning. (2009). Available from: https://www.ncbi.nlm.nih.gov/books/NBK215128/
Sajeevika, S., Daundasekara, Jennifer, E. S., Beauchamp, D. C. & Hernandez Parenting stress mediates the longitudinal effect of maternal depression on child anxiety/depressive symptoms. J. Affect. Disord. 295, 33–39. https://doi.org/10.1016/j.jad.2021.08.002 (2021). ISSN 0165–0327.
El-Sheikh, M. & Erath, S. A. Family conflict, autonomic nervous system functioning, and child adaptation: state of the science and future directions. Dev. Psychopathol. 23 (2), 703–721 (2011). PMID: 23786705; PMCID: PMC3695441.
Păsărelu, C. R., Dobrean, A., Florean, I. S. & Predescu, E. Parental stress and child mental health: a network analysis of Romanian parents. Curr. Psychol. 2022 Aug 4:1–13. https://doi.org/10.1007/s12144-022-03520-1. Epub ahead of print. PMID: 35967498; PMCID: PMC9362691.
Ho, L. L. K. et al. Impact of poverty on Parent-Child relationships, parental stress, and parenting practices. Front. Public. Health. 10, 849408. https://doi.org/10.3389/fpubh.2022.849408 (2022). PMID: 35548071; PMCID: PMC9081330.
Aktar, E. Intergenerational transmission of anxious information processing biases: an updated conceptual model. Clin. Child. Fam Psychol. Rev. 25 (1), 182–203. https://doi.org/10.1007/s10567-022-00390-8 (2022). Epub 2022 Feb 26. PMID: 35218453; PMCID: PMC8948131.
Acknowledgements
The authors would like to thank all participants.
Author information
Authors and Affiliations
Contributions
FFR, SO and SH designed the study; MJM, AC drafted the manuscript and collected the data; SH carried out the analysis and interpreted the results; SEK, FS and MD collected the data; DM reviewed the paper for intellectual content; all authors reviewed the final manuscript and gave their consent.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of the School of Pharmacy at the Lebanese International University (2023ERC- 127-LIUSOP). Participants were asked to get their parents’ approval before filling the survey; an electronic informed consent was considered obtained from each participant when submitting the online form. All methods were carried out in accordance with relevant guidelines and regulations.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Milane, MJ., Chahine, A., Malaeb, D. et al. Psychometric properties of the Arabic spence children’s anxiety scale parent in a sample of Arabic speaking adults. Sci Rep 15, 12982 (2025). https://doi.org/10.1038/s41598-025-96856-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96856-0
