
Abstract
Among central nervous system (CNS) tumors, gliomas are the most prevalent type of tumor. Single nucleotide polymorphisms (SNPs) in telomerase reverse transcriptase (TERT) gene have been identified as risk loci for gliomas by previous genome-wide association studies (GWAS). We examined association between TERT variants and glioma risk in a Korean population. For a case-control study, a total of 32 TERT SNPs from 317 patients with glioma and 480 population-based controls were genotyped. Logistic regression was used for statistical analysis of the link between TERT SNPs and risk of glioma. In this study, eight TERT variants, including four glioma-associated variants reported in previous studies, showed significant association with the risk of glioma. Conditional and stepwise analyses were conducted to validate independent associations in the group of the eight variants. Both analyses identified an intronic variant (rs56345976) as the causal variant among the eight variants. Glioma subgroup analyses indicate that rs56345976 variant is associated with the risk of WHO grade 4, glioblastoma, isocitrate dehydrogenase (IDH) wild-type, and 1p/19q non-codeletion glioma. This study presents a profound comprehension of the relationship between TERT variants and the risk of glioma. Further studies of this variant are required to investigate its effect on glioma susceptibility.
Similar content being viewed by others


Introduction
Gliomas are the most prevalent tumors which occurs in the glial or precursor cells of the brain and central nervous system (CNS)1,2, and constitute 81% of all malignant brain tumors. In 2007, the World Health Organization (WHO) classified gliomas into grades 1 to 4 based on their histological characteristics for CNS tumors3. However, in the updated 2021 WHO categorization, gliomas are categorized based on their molecular characteristics, such as isocitrate dehydrogenase (IDH) mutations and 1p/19q status4. Based on their histological and molecular characteristics, gliomas can be classified into astrocytomas, oligodendrogliomas, or glioblastomas (GBMs)1,4,5.
Genome-wide association studies (GWAS) have been conducted to verify regions correlated with the risk of glioma. Risk of glioma associated variants at 27 loci, including 8 loci correlated with all glioma (3q26.2, 5p15.33, 7p11.2, 8q24.21, 9p21.3, 11q23.3, 17p13.1, and 20q13.33), 7 loci correlated with GBM (1q31.3, 11q14.1, 12q23.3, 12q23.33, 16p.12.1, 16q.13.3, and 22q13.1), and 12 loci correlated with non-GBM glioma (1q32.1, 1q44, 2q33.3, 3p14.1, 10q24.33, 10q25.2, 11q21, 11q23.2, 12q21.2, 14q12, 15q24.2, and 16q13.3) have been reported by previous studies6,7,8,9.
Telomeres, which are located at the ends of eukaryotic chromosomes, consist of TTAGGG repeats. Telomeres play an important role in protecting chromosomes from degradation, end-to-end fusion, and abnormal recombination. Therefore, telomeres are essential for preserving chromosome unity and genomic stability10. Telomere length is maintained by telomerase, which adds the telomeric repeat sequence to the single-strand 3’ overhang. This process preserves the ends of telomeres, which gradually shorten with each cell division11. Telomerase expression is particularly low in most normal human somatic cells, however, it is higher in malignant glioma12. TERT is the most crucial factor as catalytic subunit of telomerase in determining telomerase expression13.
To follow the results of the GWAS for TERT on 5p15.33, we selected single nucleotide polymorphisms (SNPs) around association signals in TERT for glioma. In addition to studying gliomas, we conducted association analyses to identify associations with glioma subgroups, considering various clinical characteristics such as histological features, molecular properties, and grades.
TERT variants associated with glioma risk have been demonstrated by multiple studies. For instance, in the Han Chinese population, rs2853677 is associated with an increased risk of glioma14. Similarly, in European and Han Chinese populations, rs2736100 is associated with an increased risk of glioma15,16,17. In the US and UK, rs2853676 has been reported to be significantly associated with gliomas6. rs4975538 has been reported to be significantly associated with IDH-wild-type and TERT mutated gliomas in multiple ethnic groups18. In a meta-analysis, rs10069690 was found to be associated with an elevated risk of glioma regardless of sex19. Previous studies have confirmed the association between common polymorphisms of TERT and the risk of heritable glioma. However, the investigation of the association between TERT SNPs and the risk of glioma has not yet been done in Korean population.
TERT variants can cause chromosomal instability, resulting in the development of cancer. Therefore, these SNPs may be associated with telomere malfunction and cancer. For this study, prostate cancer-associated SNPs (rs13172201, rs2242652, and rs7713218)20,21,22, lung carcinoma-associated SNP (rs13167280)23, decreased telomere length in T cell-associated SNP (rs33961405)24, leukocyte telomere length-associated SNP (rs7705526)25, and epigenetic age acceleration-associated SNP (rs2736099)26 were selected.
TERT promoter hotspot mutations (C250T and C228T) are frequently observed in patients with GBM and oligodendroglioma27. These mutations create binding sites for ETS transcription factors. GABP, a member of the ETS family, enhances TERT transcription28. The increased transcription of TERT contributes to the immortality of cancer cells through the expression of telomerase29. The prevalence of TERT promoter hotspot mutations in patients with GBM varies by ethnicity30,31,32.
We initially selected SNPs of TERT to investigate this association. Additionally, we conducted an association analysis to identify the relationship between susceptibility alleles and glioma subgroups, considering various clinical characteristics such as grades, histological features, and molecular properties.
Results
Patient characteristics
Of the 317 glioma patients, the mean age was 53.43 ± 12.02 years and 50.7% were male. Patients were categorized into different subgroups according to histological characteristics: astrocytoma WHO grade 2, astrocytoma WHO grade 3, astrocytoma WHO grade 4, oligodendroglioma WHO grade 2, oligodendroglioma WHO grade 3 and GBM. Based on molecular properties of the 2021 WHO classification for CNS tumors, 84 glioma patients had IDH mutations and 67 had 1p/19q co-deletion (Table 1). The PC group comprised 480 individuals aged over 40, with a mean age of 54.8 ± 9.5 years and 49.4% male. The detailed categorizations of the patients are presented in Table 1.
Genotyping TERT genetic variants
Genotyped TERT SNPs are located on chromosome 5p15.33, as shown on physical map in Supplementary Fig. 1A. There were three LD blocks, each consisting of six, five, and five haplotypes, with a frequency of > 5% (Supplementary Fig. 1B). Detailed information, including coordinates, SNP alleles, and positions, is provided in Table 2.
Associations between TERT SNPs and glioma risk
Logistic regression analysis was conducted to confirm the causal TERT variants associated with glioma using an additive model, with adjustments for age and sex as covariates, as shown in Table 2. Eight SNPs (rs2853676, rs2736100, rs10866498, rs7713218, rs4975538, rs2242652, rs10069690, and rs56345976) were significantly associated with the risk of glioma (P < 0.009; Table 2). In addition, 16 haplotypes which frequency is over 5 were used for logistic regression analysis.
Block2-ht1 and block3-ht3 are associated with increased risk of glioma (P = 0.02 and 0.04, respectively). And block2-ht2, block2-ht3, and block3-ht1 are associated with decreased risk of glioma (P = 0.01, 0.02 and 0.01 respectively) (Supplementary Table 1).
Within the Korean population of our study, we observed the genetic effects of previously reported glioma associated TERT variants (rs2853677, rs2736100, rs10069690, rs2853676, and rs4975538). The results are summarized in Table 3.
Analysis of independency and causality of TERT variants on glioma risk
Stepwise and pairwise conditional analyses were conducted to identify the independent association among the eight significant TERT SNPs and risk of glioma. The rs56345976 SNP remained after stepwise analysis (P = 0.007) in the model with a parametric discriminant P-value (0.01). Pairwise conditional analysis also indicated that rs56345976 could be a causal variant among the eight significant variants (Table 4) when considering the remaining significances in four out of seven conditional analyses.
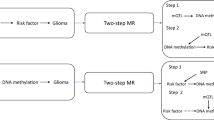
The genetic effects of rs56345976 (G > A) were subsequently investigated using additive, dominant, recessive, and referent models in the glioma subgroups (Table 5). Although significant associations were detected in all four analysis models, the A allele showed dose-dependent generic risk for glioma, e.g., the AA genotype (OR = 2.59, P = 0.0004) had a higher OR and stronger association compared to those in the GA genotype (OR = 1.16, P = 0.34) (referent model). Additionally, we investigated the genetic association among subgroups of glioma in relation to clinical characteristics, including WHO grade and histological features and molecular properties. The results indicate an association between this variant and an increased risk of glioma in the WHO grade 4, GBM, IDH wild-type, and 1p/19q non-codeletion subgroups (Table 5; Fig. 1). Stratification analyses were performed in all, male and female groups. Although the direction the trends were same, the genetic association were more apparent in female patients (Supplementary Table 2).

The association result of rs56345976 between glioma subgroups and PCs. Logistic regression between glioma subgroups and PCs (n = 480) under additive model, adjusted by age and sex as covariates, was used for calculating ORs (95% CI) and P-values at rs56345976. Each plot indicates the point estimate of ORs on the X-axis shown with 95% CI on the error bars. Significant associations are bolded. PC population control, WHO world health organization, AST astrocytomas, GBM glioblastomas, IDH-mutant IDH1 or IDH2-mutated gliomas, IDH-wildtype IDH-wildtype gliomas, 1p/19q (+) 1p/19q non-codeletion, OR odds ratio, PCs population control, CI confidence interval.
We extended our investigation by examining whether SNP rs56345976 was linked to gene expression in brain tissue using eQTL calculators within the GTEx database (https://gtexportal.org/home/testyourown)33. As results, the risk allele showed 1.12 times higher gene expression than the reference allele (G) (P = 0.042) (Table 6), which possibly corresponds to higher telomerase activity and mRNA levels in malignant glioma12,34. Human Splicing Finder (https://www.genomnis.com/access-hsf), indicated that “A” allele of rs56345976 developed 4 new exonic splicing enhancer motifs and 1 deleted enhancer motif site (Table 7). And another software, FORGE2-TF (https://forge2-tf.altiusinstitute.org/) indicates that regulatory factor X 1 (RFX1) binds to rs56345976 (Table 8).
Discussion
TERT is crucial for reconstituting telomerase activity and enabling its function. In most human cancers, telomerase reactivation occurs during carcinogenesis owing to TERT expression35. TERT somatic mutations are the most common non-coding mutations in human cancer cells. Overexpression of TERT is linked to the development of cancers and the creation of tumors36,37, and TERT regulation is important for cancer cell maintenance.
Our results indicated that a specific locus in TERT (rs56345976) is associated with an increased risk of glioma. Furthermore, rs56345976 might have causal, independent, and dose-dependent genetic effects on the risk of glioma. In the subgroup analysis, the genetic effects in the WHO grade 4, astrocytoma, and GBM subgroups were obvious. In this study consisted of Korean population, we could replicate the genetic effects of 5 SNPs, which were previously reported in Chinese Han, European, US, UK, and multiethnic populations. In silico analysis, eQTL calculators, Human Splicing Finder, and FORGE2-TF revealed different gene expressions, splicing enhancer motifs, and transcript factor that binds to rs56345976 which possibly corresponds to higher telomerase activity and mRNA levels in malignant glioma12,34. Two hotspot TERT promoter mutations (C228T and C250T), which is prevalent in glioma38, have been reported that create binding sites of Ets/TCF transcription factors, and it is associated with 2 to 4 times increased transcription28. Previous study examined interaction between TERT promoter hotspot mutation and TERT SNP by comparing mRNA expression39. Similarly, the transcription factor that binds to TERT can interact with rs56345976, thereby increasing TERT transcription efficiency. ‘A’ allele of rs56345976 increases mRNA level in basal ganglia tissue (Table 6). RFX1 is a tumor suppressive transcription factor that directly downregulates CD44 expression in glioblastoma40. ‘A’ allele of rs56345976 may affect RFX1 binding and transcript efficiency. These results could be a complement to the association between rs56345976 and risk of glioma.
Recently, progress in gene expression analysis, such as molecular profiling, has offered greater predictive information than the WHO classification of glioma41. Mutations in IDH1 and IDH2 are commonly detected in patients with astrocytoma and oligodendroglioma42. In addition, wild-type IDH is typically detected in GBM43. A previous study found that wild-type IDH was more frequent in primary GBM patients44. In this study, all GBM patients showed wild-type IDH. This indicated that the risk of GBM disease was associated with wild-type IDH. In this study, rs56345976 was found to be associated with wild-type IDH (P = 0.003). IDH wildtype is a molecular feature of glioblastoma and pediatric glioma4. Increased levels of TERT have been demonstrated to be associated with improved DNA repair mechanisms45. Recently, SNPs in genes which are related to base excision repair (BER) pathway, nucleotide excision repair (NER) pathway, developmental processes and differentiation of stem cells were reported as risk factors of pediatric glioma46,47,48. So, rs56345976 may be associated with pediatric glioma and BER or NER pathway.
A previous study demonstrated that introns can enhance transcription efficiency49. Another study reported that the transcription levels of genes with introns were higher compared to those without introns in yeast50. In mammals, gene expression involves complex interactions between promoters and enhancers, which are often located at considerable distances within the genome, recent research indicates that certain promoters may interact with regulatory sequences located within introns51. After splicing, most introns are degraded, however, some are only partially degraded and can give rise to functional non-coding RNA byproducts52. The factors that determine whether a splice site is recognized as genuine or as a pseudo splice site remain unclear, particularly given the significant diversity observed in actual splice site sequences53,54.
TERT promoter hotspot mutations, C250T and C228T, are commonly observed in patients with GBM and oligodendroglioma27. The prevalence of TERT promoter hotspot mutations in patients with oligodendroglioma is high55; however, in patients with GBM, the prevalence is specific to race (Supplementary Table 3)30,31,32. A previous study reported that 66.3% of patients diagnosed with GBM and 94.1% of those diagnosed with oligodendroglioma at Seoul National University Hospital have TERT promoter mutations32. Another study reported that TERT promoter hotspot mutations are associated with 1p/19q co-deletion55. However, many patients with GBM do not exhibit 1p/19q co-deletion, whereas oligodendroglioma patients typically do. The variant rs56345976 is significantly associated with GBM but not with oligodendroglioma or 1p/19q co-deletion. Therefore, rs56345976 may be a biomarker for GBMs with TERT promoter hotspot mutations, independent of the TERT promoter hotspot mutations associated with 1p/19q co-deletion status. However, the association between rs56345976 and TERT promoter hotspot mutations requires further study.
Owing to the limitations in statistical power, including small sample sizes in the subgroup analyses of gliomas, caution is required when interpreting the results of this study. While we used age- and sex-matched PCs, the study lacked comprehensive clinical information regarding susceptibility to glioma, which resulted in limited inclusion and exclusion criteria. In spite of using these PCs, and given the challenges in acquiring a large number of control samples, this study could be regarded as substitutive approach to ascertain the genetic influences on gliomas56. So, further clinical research, including mRNA and protein analyses, is required to determine the genetic effects of rs56345976 on gliomas in the Korean population. Additional support from functional studies would be required to establish if the identified SNP is causal.
This study aimed to explore the genetic link between TERT SNPs and glioma risk in a Korean population. This study provides initial evidence suggesting that the intronic polymorphism rs56345976 could play a role in glioma susceptibility in the Korean population. Moreover, it emphasizes that it is crucial for researchers to conduct association studies of TERT variants using glioma samples from local populations.
Materials and methods
Study subjects
This study analyzed 797 participants, comprising 317 patients and 480 controls. Patients with glioma (n = 317) were diagnosed between 2006 and 2016 and recruited from Yonsei University Severance Hospital and cooperating hospitals. The patients were categorized into subgroups of glioma based on histological and molecular properties, as classified by the WHO grading system for CNS tumors between 2007 and 20213,4. Patients with other cancers were excluded after reviewing their clinical records. The population control (PC) samples (n = 480), which excluded individuals with other types of cancer, were obtained from the Korean Genome and Epidemiology Study (KoGES) Consortium and National Biobank of Korea57. The controls, which consist of quality-controlled biospecimen collections, were obtained from population-based cohorts. This included a total of 10,038 blood donors whose ages ranged from 40 to 60 years from the Ansung-Ansan Community-based Cohort in 2001. The Wizard Genomic DNA Purification Kit (Promega, Madison, WI, USA) was used to extract genomic DNA from blood samples.
The IDH mutation and 1p/19q codeletion were analyzed by following established methods at Yonsei University Severance Hospital58. The molecular profiles of the patients were analyzed, including the analysis of O-6-methylguanine-DNA methyltransferase (MGMT) promoter methylation, IDH mutation status, and 1p/19q co-deletion. Immunostaining was performed to detect the IDH1-R132H mutation using a Ventana BenchMark XT Autostainer (Ventana Medical Systems Inc., Tucson, AZ, USA) and an anti-human IDH1 R132H mouse monoclonal antibody (Clone H09L, diluted 1:80; Dianova, Hamburg, Germany). When a mutation in IDH1-R132H was not detected by immunohistochemistry, the sequence of IDH1 codon 132 and IDH2 codon 172 was analyzed. To evaluate the 1p/19q status, fluorescence in situ hybridization (FISH) analysis was performed using LSI 1p36/1q25 and 19q13/19p13 Dual-Color Probe Kits (Abbott Molecular Inc., Abbott Park, IL, USA). Following the Euro-CNS protocols59, an experienced neuropathologist analyzed the acquired images. If the number of “deleted” nuclei was more than 50%, the tumor was classified as “deletion” for the targeted chromosome.
All procedures involving participants in this study were carried out in compliance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all the participants. The protocol for collecting blood samples from donors and isolating genomic DNA from the blood was reviewed and approved by the Public Institutional Review Board designated by the Ministry of Health and Welfare, Korea (P01-201507-31-004).
SNP selection and genotyping
Candidate TERT SNPs with a minor allele frequency (MAF) of over 5% in the Japanese and Han Chinese population from 1000 the Genomes database were selected for genotyping. Based on their positions and linkage disequilibrium (LD) with other SNPs, 27 SNPs in the TERT were selected. Additionally, five SNPs (rs2853677, rs2736100, rs10069690, rs2853676, and rs4975538) that were previously reported as glioma risk-associated SNPs were selected. The primer tool was designed using for Fluidigm SNP Type™ (San Francisco, CA, USA) to detect candidate SNPs. Genotyping was conducted on 797 subjects (317 patients and 480 controls) using the Fluidigm EP1 system (Fluidigm 96.96 SNPtype™). Priming was conducted using 96.96 Dynamic Array™ IFC Controller HX. Polymerase Chain Reaction (PCR) was performed using FC1™ Cycler. Signal intensities were measured using EP1™ Reader Data Collection Software after genotyping reaction. Genotype data were analyzed using the BioMark SNP Genotyping analysis software (version 4.3.2).
Statistical analysis
LD analysis of each genotyped SNPs was performed using Haploview v4.2 software developed by the Broad Institute (http://www.broadinstitute.org/mpg/haploview). To estimate each haplotypes, the PHASE 2.1 software was used60. Logistic regression analysis with an additive model was used to analyze the association with TERT variants by computing P-values, odds ratios (ORs), and 95% confidence intervals. Age and sex were adjusted as covariates using Golden Helix SVS8 software (Bozeman, MT, USA). The genotype distribution, Hardy-Weinberg equilibrium (HWE), and MAF of each SNP were compared between patients with glioma and PCs. Stepwise and conditional logistic analyses were performed using Statistical Analysis System (SAS) software (version 9.4; SAS Inc., Cary, NC, USA) to verify independent associations between significant TERT variants. Subsequently, to identify the detailed genetic effects, a reference model analysis based on the allele distribution of the SNP rs56345976 was conducted using Golden Helix SVS8 software. In silico analysis were performed using the GTEx eQTL calculator (https://gtexportal.org/home/testyourown), Human Splicing Finder (https://www.genomnis.com/access-hsf), and FORGE2-TF (https://forge2-tf.altiusinstitute.org/).
Data availability
The data produced and analyzed in our study will be deposited into the dbSNP repository https://www.ncbi.nlm.nih.gov/SNP/snp_viewTable.cgi?handle=GDLABSOGANGLF.
Abbreviations
- CNS:
-
Central nervous system
- SNP:
-
Single nucleotide polymorphism
- TERT:
-
Telomerase reverse transcriptase
- GWAS:
-
Genome-wide association studies
- WHO:
-
World Health Organization
- IDH:
-
Isocitrate dehydrogenase
- GBM:
-
Glioblastoma
- OR:
-
Odds ratio
- CI:
-
Confidence intervals
- HWE:
-
Hardy-Weinberg Equilibrium
- SAS:
-
Statistical Analysis System
- RFX1:
-
Regulatory factor X 1
- BER:
-
Base excision repair
- NER:
-
Nucleotide excision repair
- PC:
-
Population control
- MGMT:
-
O-6-Methylguanine-DNA methyltransferase
- MAF:
-
Minor allele frequency
- LD:
-
Linkage disequilibrium
- PCR:
-
Polymerase Chain Reaction
References
Chen, R., Smith-Cohn, M., Cohen, A. L. & Colman, H. Glioma subclassifications and their clinical significance. Neurotherapeutics 14, 284–297. https://doi.org/10.1007/s13311-017-0519-x (2017).
Modrek, A. S., Bayin, N. S. & Placantonakis, D. G. Brain stem cells as the cell of origin in glioma. World J. Stem Cells. 6, 43–52. https://doi.org/10.4252/wjsc.v6.i1.43 (2014).
Louis, D. N. et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 114, 97–109. https://doi.org/10.1007/s00401-007-0243-4 (2007).
Louis, D. N. et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-oncology 23, 1231–1251, (2021). https://doi.org/10.1093/neuonc/noab106
Namgoong, S. et al. Association analysis of RTEL1 variants with risk of adult gliomas in a Korean population. PLoS One. 13, e0207660. https://doi.org/10.1371/journal.pone.0207660 (2018).
Shete, S. et al. Genome-wide association study identifies five susceptibility loci for glioma. Nat. Genet. 41, 899–904. https://doi.org/10.1038/ng.407 (2009).
Kinnersley, B. et al. Genome-wide association study identifies multiple susceptibility loci for glioma. Nat. Commun. 6, 8559. https://doi.org/10.1038/ncomms9559 (2015).
Melin, B. S. et al. Genome-wide association study of glioma subtypes identifies specific differences in genetic susceptibility to glioblastoma and non-glioblastoma tumors. Nat. Genet. 49, 789–794. https://doi.org/10.1038/ng.3823 (2017).
Kinnersley, B., Houlston, R. S. & Bondy, M. L. Genome-Wide Association Studies in Glioma. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 27, 418–428, (2018). https://doi.org/10.1158/1055-9965.EPI-17-1080
Blackburn, E. H. Telomeres and telomerase: their mechanisms of action and the effects of altering their functions. FEBS Lett. 579, 859–862. https://doi.org/10.1016/j.febslet.2004.11.036 (2005).
Collins, K. & Mitchell, J. R. Telomerase in the human organism. Oncogene 21, 564–579. https://doi.org/10.1038/sj.onc.1205083 (2002).
Le, S., Zhu, J. J., Anthony, D. C., Greider, C. W. & Black, P. M. Telomerase activity in human gliomas. Neurosurgery 42, 1120–1124; discussion 1124–1125, (1998). https://doi.org/10.1097/00006123-199805000-00099
Zhang, A. et al. Frequent amplification of the telomerase reverse transcriptase gene in human tumors. Cancer Res. 60, 6230–6235 (2000).
Zhao, Y. et al. Fine-mapping of a region of chromosome 5p15.33 (TERT-CLPTM1L) suggests a novel locus in TERT and a CLPTM1L haplotype are associated with glioma susceptibility in a Chinese population. Int. J. Cancer. 131, 1569–1576. https://doi.org/10.1002/ijc.27417 (2012).
Zhao, Y. et al. Development of risk prediction models for glioma based on genome-wide association study findings and comprehensive evaluation of predictive performances. Oncotarget 9, 8311–8325. https://doi.org/10.18632/oncotarget.10882 (2018).
Chen, H. et al. Two novel genetic variants in the STK38L and RAB27A genes are associated with glioma susceptibility. Int. J. Cancer. 145, 2372–2382. https://doi.org/10.1002/ijc.32179 (2019).
Walsh, K. M. et al. Variants near TERT and TERC influencing telomere length are associated with high-grade glioma risk. Nat. Genet. 46, 731–735. https://doi.org/10.1038/ng.3004 (2014).
Eckel-Passow, J. E. et al. Adult diffuse glioma GWAS by molecular subtype identifies variants in D2HGDH and FAM20C. Neuro-oncology 22, 1602–1613, (2020). https://doi.org/10.1093/neuonc/noaa117
Ostrom, Q. T. et al. Sex-specific glioma genome-wide association study identifies new risk locus at 3p21.31 in females, and finds sex-differences in risk at 8q24.21. Sci. Rep. 8, 7352. https://doi.org/10.1038/s41598-018-24580-z (2018).
Chen, F. et al. Evidence of novel susceptibility variants for prostate cancer and a multiancestry polygenic risk score associated with aggressive disease in men of African ancestry. Eur. Urol. 84, 13–21. https://doi.org/10.1016/j.eururo.2023.01.022 (2023).
Schumacher, F. R. et al. Association analyses of more than 140,000 men identify 63 new prostate cancer susceptibility loci. Nat. Genet. 50, 928–936. https://doi.org/10.1038/s41588-018-0142-8 (2018).
Kote-Jarai, Z. et al. Fine-mapping identifies multiple prostate cancer risk loci at 5p15, one of which associates with TERT expression. Hum. Mol. Genet. 22, 2520–2528. https://doi.org/10.1093/hmg/ddt086 (2013).
Dai, J. et al. Identification of risk loci and a polygenic risk score for lung cancer: a large-scale prospective cohort study in Chinese populations. Lancet Respiratory Med. 7 (19), 881–891. https://doi.org/10.1016/S2213-2600 (2019).
Andreu-Sanchez, S. et al. Genetic, parental and lifestyle factors influence telomere length. Commun. Biology. 5, 565. https://doi.org/10.1038/s42003-022-03521-7 (2022).
Dorajoo, R. et al. Loci for human leukocyte telomere length in the Singaporean Chinese population and trans-ethnic genetic studies. Nat. Commun. 10, 2491. https://doi.org/10.1038/s41467-019-10443-2 (2019).
Gibson, J. et al. A meta-analysis of genome-wide association studies of epigenetic age acceleration. PLoS Genet. 15, e1008104. https://doi.org/10.1371/journal.pgen.1008104 (2019).
Arita, H. et al. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 126, 267–276. https://doi.org/10.1007/s00401-013-1141-6 (2013).
Brennan, C. W. et al. The somatic genomic landscape of glioblastoma. Cell 155, 462–477. https://doi.org/10.1016/j.cell.2013.09.034 (2013).
Horn, S. et al. TERT promoter mutations in Familial and sporadic melanoma. Science 339, 959–961. https://doi.org/10.1126/science.1230062 (2013).
Arita, H. et al. A combination of TERT promoter mutation and MGMT methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas. Acta Neuropathol. Commun. 4 https://doi.org/10.1186/s40478-016-0351-2 (2016).
Mosrati, M. A. et al. Promoter mutations and polymorphisms as prognostic factors in primary glioblastoma. Oncotarget 6, 16663–16673. https://doi.org/10.18632/oncotarget.4389 (2015).
Lee, Y., Park, C. K. & Park, S. H. Prognostic impact of TERT promoter mutations in Adult-Type diffuse gliomas based on WHO2021 criteria. Cancers 16 https://doi.org/10.3390/cancers16112032 (2024).
Consortium, G. T. The Genotype-Tissue expression (GTEx) project. Nat. Genet. 45, 580–585. https://doi.org/10.1038/ng.2653 (2013).
Boldrini, L. et al. Telomerase activity and hTERT mRNA expression in glial tumors. Int. J. Oncol. 28, 1555–1560. https://doi.org/10.3892/ijo.28.6.1555 (2006).
Dratwa, M., Wysoczanska, B., Lacina, P., Kubik, T. & Bogunia-Kubik, K. TERT-Regulation and roles in cancer formation. Front. Immunol. 11, 589929. https://doi.org/10.3389/fimmu.2020.589929 (2020).
Royle, N. J. Telomeres and disease. The Journal of pathology 180, 233–235, doi:10.1002/ (SICI)1096-9896 (199611)180:3<233::AID-PATH675>3.0.CO;2-8 (1996).
Calado, R. & Young, N. Telomeres in disease. F1000 Med. Rep. 4 https://doi.org/10.3410/M4-8 (2012).
Liu, X. et al. Highly prevalent TERT promoter mutations in bladder cancer and glioblastoma. Cell. Cycle. 12, 1637–1638. https://doi.org/10.4161/cc.24662 (2013).
Labussiere, M. et al. TERT promoter mutations in gliomas, genetic associations and clinico-pathological correlations. Br. J. Cancer. 111, 2024–2032. https://doi.org/10.1038/bjc.2014.538 (2014).
Feng, C. Z. et al. Regulatory factor X1 is a new tumor suppressive transcription factor that acts via direct downregulation of CD44 in glioblastoma. Neuro-oncology 16, 1078–1085. https://doi.org/10.1093/neuonc/nou010 (2014).
Theeler, B. J., Yung, W. K., Fuller, G. N. & De Groot, J. F. Moving toward molecular classification of diffuse gliomas in adults. Neurology 79, 1917–1926. https://doi.org/10.1212/WNL.0b013e318271f7cb (2012).
Yan, H. et al. IDH1 and IDH2 mutations in gliomas. N Engl. J. Med. 360, 765–773. https://doi.org/10.1056/NEJMoa0808710 (2009).
Wesseling, P. & Capper, D. WHO 2016 classification of gliomas. Neuropathol. Appl. Neurobiol. 44, 139–150. https://doi.org/10.1111/nan.12432 (2018).
Li, Y. et al. Murine models of IDH-wild-type glioblastoma exhibit Spatial segregation of tumor initiation and manifestation during evolution. Nat. Commun. 11, 3669. https://doi.org/10.1038/s41467-020-17382-3 (2020).
Palamarchuk, A. I., Kovalenko, E. I. & Streltsova, M. A. Multiple actions of telomerase reverse transcriptase in cell death regulation. Biomedicines 11 ARTN 109110.3390/biomedicines11041091 (2023).
Chen, Y. P. et al. Association between genetic polymorphisms of base excision repair pathway and glioma susceptibility in Chinese children. World J. Pediatr. 18, 632–635. https://doi.org/10.1007/s12519-022-00562-0 (2022).
Chen, Y. et al. Association of ERCC1 and XPF polymorphisms with pediatric glioma susceptibility. Chin. Med. J. 136, 746–748. https://doi.org/10.1097/CM9.0000000000002126 (2023).
Guo, H. Q. et al. Association between gene polymorphisms and glioma susceptibility in Chinese children. Cancer Control: J. Moffitt Cancer Cent. 28, (2021). doi:Artn 1073274821104000910.1177/10732748211040009.
Brinster, R. L., Allen, J. M., Behringer, R. R., Gelinas, R. E. & Palmiter, R. D. Introns increase transcriptional efficiency in Transgenic mice. Proc. Natl. Acad. Sci. U.S.A. 85, 836–840. https://doi.org/10.1073/pnas.85.3.836 (1988).
Juneau, K., Miranda, M., Hillenmeyer, M. E., Nislow, C. & Davis, R. W. Introns regulate RNA and protein abundance in yeast. Genetics 174, 511–518. https://doi.org/10.1534/genetics.106.058560 (2006).
Stadhouders, R. et al. Transcription regulation by distal enhancers: who’s in the loop? Transcription 3, 181–186. https://doi.org/10.4161/trns.20720 (2012).
Bortolin, M. L. & Kiss, T. Human U19 intron-encoded snorna is processed from a long primary transcript that possesses little potential for protein coding. Rna 4, 445–454 (1998).
Roca, X., Sachidanandam, R. & Krainer, A. R. Intrinsic differences between authentic and cryptic 5’ splice sites. Nucleic Acids Res. 31, 6321–6333. https://doi.org/10.1093/nar/gkg830 (2003).
Roca, X., Krainer, A. R. & Eperon, I. C. Pick one, but be quick: 5’ splice sites and the problems of too many choices. Genes Dev. 27, 129–144. https://doi.org/10.1101/gad.209759.112 (2013).
Heidenreich, B. et al. TERT promoter mutations and telomere length in adult malignant gliomas and recurrences. Oncotarget 6, 10617–10633. https://doi.org/10.18632/oncotarget.3329 (2015).
Ruano-Ravina, A., Perez-Rios, M. & Barros-Dios, J. M. Population-based versus hospital-based controls: are they comparable? Gac Sanit. 22, 609–613. https://doi.org/10.1016/s0213-9111 (2008). (08)75363-9.
Cho, S. Y. et al. Opening of the National biobank of Korea as the infrastructure of future biomedical science in Korea. Osong Public. Health Res. Perspect. 3, 177–184. https://doi.org/10.1016/j.phrp.2012.07.004 (2012).
Hong, J. B. et al. Predicting survival using the 2016 world health organization classification for anaplastic glioma. Clin. Neuropathol. 39, 188–195. https://doi.org/10.5414/NP301228 (2020).
Woehrer, A. et al. FISH-based detection of 1p 19q codeletion in oligodendroglial tumors: procedures and protocols for neuropathological practice - a publication under the auspices of the research committee of the European confederation of neuropathological societies (Euro-CNS). Clin. Neuropathol. 30, 47–55. https://doi.org/10.5414/npp30047 (2011).
Stephens, M., Smith, N. J. & Donnelly, P. A new statistical method for haplotype reconstruction from population data. Am. J. Hum. Genet. 68, 978–989 (2001). doi:Doi 10.1086/319501.
Acknowledgements
We are grateful to the contributors, especially the Brain Tumor Center staff at Yonsei Severance Hospital for collecting the samples used in this study, as well as the patients and their families.
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2021R1F1A105994712).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Ho Yeon Lim, Hyun Sub Cheong, Seok Namgoong. Lyoung Hyo Kim, Hyoung Doo Shin, Jong Hee Chang contributed to the interpretation of the results and discussion. Ho Yeon Lim, and Lyoung Hyo Kim took the lead in writing the manuscript and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The protocol for collecting blood samples from donors and isolating genomic DNA from the blood was reviewed and approved by the Public Institutional Review Board designated by the Ministry of Health and Welfare, Korea (P01-201507-31-004).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lim, H.Y., Cheong, H.S., Namgoong, S. et al. A novel variant of telomerase reverse transcriptase (TERT) associated with risk of glioma in a Korean population. Sci Rep 15, 14346 (2025). https://doi.org/10.1038/s41598-025-96929-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96929-0
