
Abstract
Cardiovascular diseases are the leading cause of mortality worldwide, contributing to one-third of global deaths. Beyond physical health, heart disease is associated with cardiac distress, an emotional response that can negatively impact recovery and well-being. Understanding the psychological and social mechanisms underlying cardiac distress is crucial for improving patient outcomes. This study examines how social health (social support and social isolation) influences cardiac distress, with loneliness and repetitive negative thinking as mediators. To evaluate a theoretical model linking social health to cardiac distress, mediated by loneliness and repetitive negative thinking in patients with heart disease. A cross-sectional, correlational study was conducted in 2024 with 400 cardiac patients from two hospitals and one private clinic in Amol, Iran. Participants completed validated questionnaires assessing cardiac distress, social support, social isolation, loneliness, and repetitive negative thinking. Structural equation modeling was used for data analysis. Social isolation (r = 0.47, p < 0.001) and repetitive negative thinking (r = 0.50, p < 0.001) were significantly associated with greater cardiac distress. Social support negatively predicted both loneliness (β = − 0.32, p < 0.001) and cardiac distress (β = − 0.25, p < 0.01). Indirect effects showed that social support reduced cardiac distress by decreasing loneliness and repetitive negative thinking (β = − 0.23, p < 0.01), while social isolation increased cardiac distress through its influence on loneliness and repetitive negative thinking (β = 0.18, p = 0.05). The model explained 47.4% of the variance in cardiac distress. These findings highlight the importance of social health in managing cardiac distress among heart disease patients. Strengthening social support may alleviate loneliness and reduce repetitive negative thinking, ultimately improving emotional well-being and health outcomes. Future research should explore targeted interventions addressing these psychosocial factors to effectively reduce cardiac distress.
Similar content being viewed by others
Introduction
Cardiovascular diseases, including ischemia, heart failure, acute coronary syndrome, arrhythmias, and cardiomyopathies, account for one-third of global mortality. Evidence shows that learning about a heart disease diagnosis can be distressing for any individual1, with such anxiety and depression referred to as cardiac distress2,3. In other words, cardiac distress is a complex and persistent negative emotional state that arises following acute cardiac events, such as heart attacks or surgeries, encompassing a wide range of psychosocial dimensions, including physical, emotional, cognitive, behavioral, and social symptoms. Cardiac distress encompasses a range of psychological responses experienced by individuals with heart disease, including anxiety, depression, and stress. These emotional states can adversely affect health behaviors and clinical outcomes. Notably, poor medication adherence among heart failure patients is a common issue that leads to increased exacerbations, reduced physical function, and a higher risk of hospital readmissions and mortality4. Furthermore, non-adherence to cardiovascular therapy has been associated with increased mortality rates5. Additionally, medication non-adherence is linked to substantial healthcare costs and is responsible for at least 10% of hospitalizations in the United States6. Despite its importance, therapeutic interventions for cardiac distress are often overlooked, although specific interventions could alleviate symptoms and improve therapeutic outcomes7,8.
One key variable in the context of cardiac distress is social health, which refers to individuals’ ability to establish and maintain meaningful relationships with others and adapt comfortably to various social situations9. Social health includes two components: social isolation and social support. Social support is a subjective concept reflecting the operationalization of social connections—whether an individual has someone to interact with or chooses a companion to talk to. In essence, social support is perceived through interaction with others. On the other hand, social isolation is an objective measure of the quantity of social connections, indicating that an individual lacks social interactions, lives alone, and socially isolates themselves10. Strong social relationships characterized by frequent contact, emotional support, and adequate financial assistance are crucial for maintaining cardiovascular health, reducing cardiac distress, and facilitating proper decision-making and effective treatment processes11.
The relationship between social isolation, social support, and cardiac distress is complex and not fully understood. Research on the association between social support and cardiac distress has yielded mixed findings. While many studies indicate that social support can positively influence health outcomes in patients with cardiovascular diseases (CVD), some evidence suggests that this relationship may not be as robust as assumed12. For instance, a systematic review found that lower social support is associated with greater healthcare utilization and poorer survival rates following cardiovascular events. However, it did not establish a direct link between social support and emotional distress outcomes in all contexts13. Conversely, a study focusing on patients with coronary artery disease found that while social support and socioeconomic status predict emotional well-being, the direct and independent effect of social support on emotional distress is less definitive. Instead, negative expectations play a more significant role in short-term emotional outcomes. This suggests that while social support is beneficial, its direct impact on cardiac distress may be moderated by other psychosocial factors, indicating a more complex interaction than previously understood14. Additionally, a narrative review revealed that low social health could be considered a consistent risk factor for CVD, though the directionality of this relationship remains unclear15. Therefore, further exploration of the role of social health, including its two components—social support and social isolation—on cardiac distress is warranted, along with identifying moderating mediators. Research has shown that psychosocial factors play a crucial role in emotional well-being. For instance, a study on older adults demonstrated that attachment influences well-being through hope, religiosity, and life satisfaction, emphasizing the significance of psychological resilience in managing emotional distress16.
Loneliness is an emotional response to social isolation and is associated with the quality of social relationships17. It is a subjective and distressing state in which individuals perceive their social needs as unmet, even when surrounded by others18. Research has shown that loneliness is linked to adverse health outcomes, including increased mortality rates, heightened anxiety, and greater susceptibility to depression10. A recent meta-analysis of 90 cohort studies found that social isolation and loneliness are associated with a 32% and 14% increased risk of all-cause mortality, respectively. This underscores the significant impact of social connections on survival rates19. Given these associations, exploring the relationship between loneliness and cardiac distress is critical for understanding the broader psychosocial impacts on heart disease patients. RNT is a cognitive process characterized by persistent and involuntary focus on distressing thoughts, often revolving around unresolved problems. Many studies indicate that RNT is common in individuals with depression, exacerbating stress and anxiety20,21. This cognitive pattern can be categorized into two subtypes: brooding rumination, which involves passive and negative self-reflection that intensifies emotional distress, and reflective rumination, which is more constructive and focused on problem-solving22. Studies suggest that loneliness and social isolation can amplify rumination, contributing to worsening depressive symptoms23. However, the extent to which social health influences cardiac distress through RNT remains unclear. Specifically, further research is needed to determine whether the relationship between social health and cardiac distress is explained by the serial mediating effects of loneliness and RNT24.
The link between social health and cardiac distress remains unclear, with mixed findings on its direct impact. The roles of loneliness and RNT as mediators are underexplored. Clarifying these mechanisms is crucial for effective interventions.
Theoretical framework
This study explores the pathways linking social health and cardiac distress, emphasizing the mediating roles of loneliness and RNT. To provide a solid theoretical foundation, this study integrates the biopsychosocial model of health, the stress-buffering model of social support, and the perseverative cognition hypothesis to explain how social health impacts cardiac distress through loneliness and RNT. The biopsychosocial model of health25 posits that health outcomes result from the interplay between biological, psychological, and social factors. In the context of cardiac distress, social health—comprising social support and social isolation—plays a critical role in determining emotional and physiological responses to illness26,27. Social support fosters resilience and mitigates distress, whereas social isolation exacerbates psychological vulnerability, increasing the risk of adverse cardiovascular outcomes28.
The stress-buffering model of social support26 further elucidates the protective role of social relationships. According to this model, social support helps individuals manage stress by providing emotional and instrumental resources, thereby reducing physiological arousal and emotional distress29. Conversely, social isolation and loneliness can heighten stress, contributing to worsened cardiac outcomes. This aligns with findings that social disconnection is associated with increased stress responses and poorer cardiovascular health30. The perseverative cognition hypothesis31 explains how repetitive negative thinking acts as a crucial mediator in the relationship between social health and cardiac distress. This theory suggests that prolonged cognitive engagement with distressing thoughts, such as worry and rumination, sustains physiological stress responses32. Persistent loneliness may contribute to excessive rumination, further exacerbating emotional distress and its physiological consequences25. By integrating these theoretical perspectives, the social health-loneliness-RNT-cardiac distress model is proposed. This model postulates that social isolation increases loneliness, which in turn triggers RNT, ultimately leading to heightened cardiac distress. Conversely, social support may mitigate cardiac distress by reducing loneliness and preventing excessive engagement in RNT. This theoretical framework provides a comprehensive explanation of the complex interactions between social, cognitive, and physiological processes in cardiac patients.
The complex relationship between social health and cardiac distress can be understood through established theoretical models. The biopsychosocial model posits that health outcomes are shaped by interactions between biological, psychological, and social factors, emphasizing the role of social support and isolation in emotional and physiological responses to illness25. The stress-buffering model suggests that social support can mitigate stress by providing emotional and instrumental resources, reducing physiological arousal and emotional distress26. Additionally, the perseverative cognition hypothesis explains how repetitive negative thinking prolongs stress-related physiological activation, contributing to adverse cardiovascular outcomes31.
Hypotheses
The current study hypotheses:
-
Hypothesis 1: Social Support will negatively predict Loneliness.
-
Hypothesis 2: Social Isolation will positively predict Loneliness.
-
Hypothesis 3: Loneliness will positively predict Repetitive Negative Thinking.
-
Hypothesis 4: Repetitive Negative Thinking will positively predict Cardiac Distress.
-
Hypothesis 5: Social Support will indirectly affect Cardiac Distress through Loneliness and Repetitive Negative Thinking.
-
Hypothesis 6: Social Isolation will indirectly affect Cardiac Distress through Loneliness and Repetitive Negative Thinking.
Methodology
Study design and participants
This cross-sectional, correlational, predictive study utilized a structural equation modeling (SEM) approach and was conducted in 2024. Data collection was carried out using convenience sampling from November to December 2024, involving cardiac patients from the heart clinics of two hospitals and a private cardiology practice in Amol, Iran. A total of 133 patients were recruited from each hospital’s heart clinic, and 134 patients were enrolled from the private practice, ensuring representation across different healthcare settings. Notably, all participants were outpatients and not bedridden during the study period.
Participants were selected based on specific inclusion and exclusion criteria that were established to ensure a well-defined study population. Eligible participants were required to be 18 years of age or older, Iranian citizens or residents, and to have had a confirmed diagnosis of heart disease by a healthcare professional. They also needed to have been in stable health, with no recent hospitalizations or major changes in treatment, to have been capable of providing informed consent, and to have been willing to complete the CDI and related assessments.
To minimize potential confounding factors, individuals were excluded if they had had a history of significant psychiatric disorders, such as schizophrenia or bipolar disorder, that could have interfered with questionnaire completion, or if they had had cognitive impairments or language barriers that could have hindered comprehension of the survey. Additionally, those who had been diagnosed with other chronic illnesses that could have independently impacted psychological distress levels, individuals who had undergone major cardiac procedures like coronary artery bypass surgery or valve replacement within the past three months, or those who had been receiving treatments that could have significantly influenced psychological responses, such as intensive psychotherapy or major psychiatric medication adjustments, were also excluded. Finally, participants who had previously taken part in similar studies within the past year were not included.
The sample size adequacy was determined using SEM guidelines33. Considering a medium effect size of 0.2534, 80% statistical power, a significance level of less than 0.05, five latent factors, and a total of 48 items across the study instruments, a minimum sample size of 229 participants was estimated. Accounting for a 10% attrition rate35, 400 participants were enrolled in the study. Ultimately, 400 cardiac patients were included in the study. During the sample collection and questionnaire completion process, the researcher was present with the participants to provide necessary clarifications and address any ambiguities. This ensured that all questions were fully understood before responses were recorded. As a result, all 400 participants completed the questionnaires in full, and there was no missing data in the dataset. This approach minimized response errors and enhanced the reliability of the collected data.
Instruments
Demographic information form
This data collection form included items on age, gender, level of education, marital status.
Cardiac distress (CD)
The Cardiac Distress Assessment Tool was developed by Alun Jackson et al. in 2023. This 12-item instrument uses a five-point Likert scale ranging from 1 (“No distress”) to 5 (“High distress”). Scoring is negatively oriented, meaning higher scores reflect greater levels of distress. The total score ranges from 12 to 60, with a score above 13 indicating significant cardiac distress. The original version of the CDI consisted of eight subscales: Fear and Uncertainty, Disconnection and Hopelessness, Changes to Roles and Relationships, Overwhelm and Depletion, Cognitive Challenges, Physical Challenges, Health System Challenges, and Death Concerns. The validity and reliability of the present instrument were evaluated, and the results confirmed that it possesses acceptable psychometric properties36.
Social support (SS)
The Social Support Assessment Tool was designed by Zimet et al. in 1988. This 12-item instrument uses a seven-point Likert scale ranging from 1 (“Strongly agree”) to 7 (“Strongly disagree”). The scoring is negatively oriented, where higher scores indicate lower perceived social support. The total score ranges from 12 to 8437. The validity and reliability of the present instrument were assessed within the Iranian cultural context, and the findings indicated that it demonstrated acceptable psychometric properties38.
Social isolation (SI)
The Social Isolation Assessment Tool, developed by David M. Bass, consists of seven items measured on a four-point Likert scale from 0 (“Strongly disagree”) to 3 (“Strongly agree”). The total score ranges from 0 to 21, with higher scores indicating greater levels of social isolation39. The validity and reliability of the loneliness instrument in the present study were evaluated using the Fornell and Larcker approach40. Additionally, internal consistency was assessed to determine reliability, demonstrating acceptable validity and reliability.
Repetitive negative thinking (RNT)
The RNT was developed by McEvoy et al. in 2014. This 10-item instrument uses a five-point Likert scale ranging from 1 (“Not at all true”) to 5 (“Completely true”), with total scores ranging from 10 to 50. Higher scores indicate more intense RNT. Although the validity and reliability of the current instrument have not been specifically assessed in the Iranian cultural context, the study by McEvoy et al. demonstrated that the instrument possesses strong validity and reliability41.
Loneliness (L)
The Loneliness Assessment Tool, designed by Jenny De Jong and Theo Van Tilburg in 2006, contains six items scored on a six-point Likert scale ranging from 0 (“Never”) to 6 (“Always”). The total score ranges from 6 to 18, with higher scores indicating greater perceived loneliness42. The validity and reliability of the current instrument were assessed within the Iranian cultural context, demonstrating adequate construct validity and internal consistency43.
Questionnaire translation and adaptation
The translation of the study questionnaires followed a structured process to ensure linguistic and conceptual accuracy. Initially, the original English versions were independently translated into Persian by two bilingual experts. These two translations were then compared, and discrepancies were reconciled to produce a unified Persian version. This preliminary version was thoroughly reviewed by the research team for clarity, consistency, and cultural appropriateness. Following this review, the final Persian version was approved for use in the study.
Data analysis
In the data analysis section, we began by employing descriptive statistics to summarize and characterize the key features of the dataset. Prior to this analysis, we conducted thorough data cleaning to address any inconsistencies and missing values. Following the descriptive analysis, we utilized the Pearson correlation coefficient in SPSS (v. 26.0) to examine the strength and direction of linear relationships between pairs of variables. Finally, we applied structural equation modeling (SEM) to investigate complex relationships and test theoretical frameworks.
The Kaiser-Meyer-Olkin and Bartlett’s tests were utilized to assess the adequacy of the sample and the suitability of the model in factor analysis. A Kaiser-Meyer-Olkin test value exceeding 0.7 indicates that the model is appropriate for analysis44. To detect potential multivariate outliers, Mahalanobis distance was computed. A χ2 critical value at p < 0.001 was used as a threshold, and nine cases exceeded this criterion, suggesting they were potential outliers45. However, further examination of their influence on the overall results led to the decision to retain them, as their removal did not significantly alter the findings. For normality assessment, univariate normality was examined using skewness (± 3) and kurtosis (± 7) measures. All variables fell within the acceptable range, confirming univariate normality. Multivariate normality was assessed using Mardia’s coefficient, which resulted in a value of 7.32, falling below the critical threshold of 8, indicating that the assumption of multivariate normality was met45. Finally, structural equation modeling was performed to assess the mediating role of L and RNT in the relationship of SS and SI with CD. Bootstrapping with 2, 000 repetitions was also employed for hypothesis testing in structural modeling46. Model fit indices were root mean square error of approximation (RMSEA; < 0.08), Standardized Root Mean Square Residual (SRMR; < 0.10), comparative fit index (CFI; > 0.90), incremental fit index (IFI; > 0.90), and Tucker-Lewis index (TLI; > 0.90).
Convergent-discriminant validity and reliability
The Internal consistency was tested using Cronbach’s alpha, McDonald’s omega, AIC, and composite reliability (CR), where Cronbach’s alpha, McDonald’s omega, and CR values of more than 0.7, and AIC values of 0.2 to 0.4 were interpreted as acceptable reliability45. To achieve convergent validity for all constructs, the average variance extracted (AVE) of each construct should be higher than 0.540. On the other hand, discriminant validity is achieved by utilizing the Heterotrait-Monotrait ratio (HTMT) of the correlations criterion. This method requires that the HTMT ratio between all constructs is less than 0.85 to ensure discriminant validity47.
Path analysis
To test the hypothesized relationships, we performed a path analysis using SEM with AMOS (v. 26.0). The model included Social Support and Social Isolation as independent variables, Loneliness and RNT as mediating variables, and CD as the dependent variable. A serial mediation model was specified, where Loneliness was proposed to influence RNT, which in turn affected CD. All statistical hypotheses were two-tailed and the significance levels were set at less than 0.05.
Results
The mean age of the participants was 42.87 years (SD = 14.05). The sample predominantly consisted of women, with 227 participants (56.8%) identifying as female. Additionally, a significant proportion of the participants had attained a high school education, comprising 144 individuals (36.0%). Furthermore, the majority of the participants were married, with 327 individuals (81.8%) reporting marital status as married.
Results of the measurement model assessment are shown in Table 1. All constructs demonstrated satisfied internal consistency, and construct reliability. As shown, AVE for social support, loneliness and RNT were greater than 0.5, but AVE for cardiac distress and social isolation were slightly less than 0.5. Hence, with the high level of CR, all constructs have achieved convergent validity. As for discriminant validity, all values of the HTMT matrix were less than 0.85, establishing discriminant validity of all constructs (Table 2).
The correlation analysis between cardiac distress and various independent variables revealed several noteworthy associations. Social isolation (r = 0.47, p < 0.001) and repetitive negative thinking (r = 0.50, p < 0.001) showed a moderate positive correlation with cardiac distress. Similarly, loneliness had a weak positive correlation with cardiac distress (r = 0.12, p = 0.012), indicating that higher levels of loneliness are associated with slightly increased cardiac distress. Conversely, social support level demonstrated a negative correlation with cardiac distress (r = -0.30, p < 0.001).
Hypothesis testing
The results of this study provided support for all six hypotheses. Specifically, greater social support was associated with lower levels of loneliness, while higher social isolation was linked to increased loneliness. In turn, loneliness was found to contribute to more frequent engagement in repetitive negative thinking, which subsequently led to greater cardiac distress. Furthermore, social support indirectly reduced cardiac distress by first lowering loneliness, which then decreased repetitive negative thinking and, ultimately, distress levels. Conversely, social isolation indirectly increased cardiac distress by heightening loneliness, which led to more repetitive negative thinking and, as a result, greater distress. These findings align with our proposed model and highlight the interconnected roles of social support, social isolation, loneliness, and repetitive negative thinking in influencing cardiac distress.
Direct effects
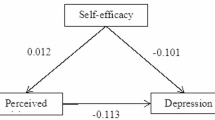
According to the Fig. 1, social support was found to negatively predict both loneliness and cardiac distress. Specifically, higher levels of social support were associated with a reduction in loneliness (β = -0.32, p < 0.001) and cardiac distress (β = -0.25, p < 0.001). In contrast, social isolation exhibited a positive relationship with loneliness (β = 0.41, p < 0.001) and repetitive negative thinking (β = 0.28, p < 0.001). Additionally, Social isolation was positively associated with cardiac distress (β = 0.18, p = 0.04), indicating that higher levels of social isolation were linked to greater cardiac distress. Also it was observed that elevated levels of loneliness (β = 0.17, p < 0.001) and repetitive negative thinking (β = 0.27, p < 0.001) were significantly associated with increased cardiac distress. Finally, our analysis revealed a significant positive association between loneliness and repetitive negative thinking, with increasing levels of loneliness associated with heightened repetitive negative thinking (β = 0.07, p < 0.001).

The serial mediation model, ***p<0.00; *p<0.05; Model controls age, gender, and education level.
Indirect effects
The total indirect effect of social support on cardiac distress through both loneliness and repetitive negative thinking was significant, with a coefficient of β = -0.23 (p < 0.001). This suggests that social support may be associated with lower cardiac distress through its potential role in decreasing loneliness, which in turn may be linked to reduced repetitive negative thinking. Similarly, the indirect effect of social isolation on cardiac distress through loneliness and repetitive negative thinking was significant (β = 0.18, p = 0.05). This indicates that social isolation may be associated with greater cardiac distress through its potential impact on loneliness, which in turn may contribute to increased repetitive negative thinking.
Mediation effects
Loneliness significantly predicted repetitive negative thinking (β = 0.34, p < 0.001). Furthermore, repetitive negative thinking was found to significantly predict higher levels of cardiac distress (β = 0.41, p < 0.001). These results suggest that loneliness may play a key role in the experience of cardiac distress through its potential influence on repetitive negative thinking.
The overall model fit showed that SS and SI explained 21.2% of the variance in L (R2 = 0.212), and SI explained 16.7% of the variance in RNT (R2 = 0.167). Together with the mediators, the independent variables explained 47.4% of the variance in CD (R2 = 0.474).
The hypothesized path model was tested using structural equation modeling. The model exhibited good fit to the data, with the following fit indices: χ26 = 12.45, p = 0.05, CFI = 0.97, TLI = 0.94, RMSEA = 0.05 (90% CI [0.00, 0.10]), SRMR = 0.04. These indices indicate that the model is an acceptable representation of the data.
Discussion
The present study highlights the complex interplay between social factors, psychological processes, and cardiac distress in patients with heart disease. The findings indicate that social isolation and repetitive negative thinking are moderately associated with increased cardiac distress, while loneliness has a weaker but significant association. Conversely, social support plays a protective role by reducing both loneliness and cardiac distress. Mediation analyses reveal that loneliness and repetitive negative thinking serve as key pathways through which social factors influence cardiac distress. Notably, social support indirectly reduces cardiac distress by mitigating loneliness and repetitive negative thinking, whereas social isolation exacerbates it through similar mechanisms. The overall model explained a substantial portion (47.4%) of the variance in cardiac distress, underscoring the importance of both social and cognitive factors in patients’ well-being. The findings of this study provide significant insights into the mediating role of loneliness and repetitive negative thinking in the relationship between social factors (social support and social isolation) and cardiac distress in patients with heart disease.
The relatively young mean age of our study sample (42.87 years) warrants careful consideration regarding the generalizability of our findings to older cardiac patients. In Iran, CVDs predominantly affect older adults; for instance, a population-based study reported that individuals aged 65–70 years had a CVD prevalence of 27.9%, compared to 7.5% in those aged 35–45 years48. Additionally, projections indicate that by 2025, more than 70.3% of the burden of cardiovascular diseases in Iran will occur in individuals under 65 years of age, reflecting a significant impact on the younger population49. Furthermore, studies have shown that the mean age of myocardial infarction patients in Iran is approximately 61.20 years, with men experiencing these events at a younger age than women50.
Social support and loneliness
As hypothesized, social support negatively predicted loneliness (Hypothesis 1). This aligns with previous research highlighting the protective role of social support in mitigating feelings of loneliness27,51. Supportive relationships likely provide emotional resources, companionship, and a sense of belonging, which act as buffers against loneliness52. Supportive relationships play a critical role in mitigating the effects of loneliness and enhancing overall well-being. Research indicates that social support can significantly buffer the negative impacts of loneliness53. For instance, one study emphasizes that perceived support from others not only alleviates feelings of isolation but also improves life satisfaction54. Similarly, another article investigates the relationship between social support and health outcomes, finding that community networks can help mitigate the adverse effects of loneliness, underscoring the importance of supportive relationships in coping with loneliness and maintaining physical health. Furthermore, additional research highlights that perceived social support from family and friends is negatively associated with loneliness, reinforcing the notion that these supportive connections provide essential emotional resources that help individuals navigate feelings of isolation55. Collectively, these findings illustrate the profound impact of social support on enhancing life satisfaction and promoting better health outcomes by acting as a buffer against loneliness.
Social support serves as a crucial protective factor in mitigating the negative psychological and emotional consequences associated with cardiac distress. Consistent with previous research demonstrating the positive role of social support in chronic disease management56, our findings highlight that strong social connections can buffer against loneliness and reduce the likelihood of engaging in repetitive negative thinking. Supportive relationships provide emotional reassurance, practical assistance, and a sense of belonging, which collectively contribute to better mental well-being and improved cardiovascular health outcomes. By fostering resilience and enhancing self-efficacy, social support may play a vital role in alleviating the psychological burden of heart disease, ultimately reducing cardiac distress.
Social isolation and loneliness
Social isolation was found to positively predict loneliness (Hypothesis 2), consistent with prior studies demonstrating that limited social interactions and perceived isolation increase the risk of loneliness57. The association highlights the detrimental impact of social isolation, which often coexists with chronic conditions like heart disease, exacerbating emotional and psychological vulnerabilities58. Research indicates that greater social isolation and reduced social support are significantly linked to heightened feelings of loneliness. These feelings, in turn, correlate with increased levels of depression and poorer self-rated health. The findings emphasize the mediating role of loneliness in the connection between social isolation and various health outcomes. Specifically, individuals with limited social networks or functional limitations are more likely to experience intensified loneliness and associated health risks59. Also social isolation is associated with an increased risk of dementia, coronary artery disease, stroke, and all-cause mortality60,61.
Loneliness has been shown to negatively affect satisfaction with life, as it undermines individuals’ sense of meaning, belonging, and emotional well-being. Persistent loneliness can lead to lower life satisfaction by fostering negative cognitive patterns and reducing overall psychological resilience. However, the perception of God may play a crucial moderating role in this relationship. Individuals who perceive a close relationship with God or a higher spiritual presence often experience greater emotional comfort and a stronger sense of purpose, which can mitigate the adverse effects of loneliness on life satisfaction. Faith and spirituality may provide a sense of companionship and existential meaning, reducing the impact of loneliness on overall well-being62.
Loneliness and repetitive negative thinking
The study identified a significant positive relationship between loneliness and RNT (Hypothesis 3), aligning with evidence suggesting that loneliness fosters maladaptive cognitive processes, including ruminative thinking. A significant association between loneliness and increased RNT, indicating that higher levels of loneliness statistically predict more ruminative thoughts. Frequent feelings of loneliness can trigger and perpetuate ruminative thinking, thereby strengthening the link between loneliness and depressive symptoms. This finding aligns with established theoretical frameworks, such as the Perseverative Cognition Hypothesis, which posits that loneliness acts as a stressor that fosters maladaptive cognitive processes like RNT. Such processes can exacerbate mental health issues, including depression, highlighting the detrimental impact of loneliness on psychological well-being63. Feeling lonely during social distancing can intensify self-focused thoughts on isolation, leading to chronic stress and adverse effects on mental health. This emphasizes how persistent reflection on loneliness can exacerbate depression and other psychological issues64. Loneliness may heighten self-focused attention and exacerbate negative appraisals, creating a fertile ground for RNT. This pathway is critical, as it links social experiences to cognitive vulnerabilities that perpetuate emotional distress and poor health outcomes65.
Repetitive negative thinking and cardiac distress
Repetitive negative thinking was found to positively predict cardiac distress (Hypothesis 4). This is consistent with literature emphasizing the deleterious effects of RNT on cardiovascular health through mechanisms such as heightened sympathetic activation, systemic inflammation, and impaired emotional regulation66. RNT has been shown to significantly impact cardiovascular health through various physiological mechanisms. Research indicates that RNT can lead to increased heart rate, elevated blood pressure, and heightened cortisol levels, all of which contribute to cardiovascular distress32. The mechanisms through which RNT affects cardiovascular health include prolonged sympathetic nervous system activation and systemic inflammation. These physiological changes can accelerate the development of atherosclerosis and increase the risk of acute cardiac events such as heart attacks and arrhythmias67. By sustaining a state of psychological stress, RNT likely exacerbates cardiac distress, highlighting its relevance as a target for therapeutic interventions.
Indirect effects of social support and social isolation
The indirect effects observed in this study highlight the pathways through which social factors influence cardiac distress. Social support indirectly reduced cardiac distress via loneliness and RNT (Hypothesis 5), whereas social isolation had the opposite effect, exacerbating cardiac distress (Hypothesis 6). These findings align with the biopsychosocial model of health, which underscores the interaction of social, psychological, and physiological factors in shaping health outcomes26. Low social support is linked to an increased risk of CVD and poorer recovery after cardiac events, as it influences stress and depressive symptoms—both known risk factors for cardiac distress. Loneliness, a key mediator, is associated with higher mortality and worsened CVD outcomes68,69,70,71. Additionally, RNT, shaped by low social support and loneliness, contributes to emotional distress and deteriorating cardiac health. Similarly, social isolation is a critical risk factor for CVD, as it increases loneliness and fosters RNT, further intensifying cardiac distress68,70,72. The mediating role of loneliness and RNT highlights the need to address both social and psychological factors in cardiac care. Interventions that enhance social support and reduce isolation may help mitigate loneliness and interrupt maladaptive cognitive processes like RNT, ultimately improving cardiac outcomes.
Clinical implications
From a clinical perspective, these findings highlight the need for a multidimensional approach to managing cardiac distress. Interventions that enhance social support—such as support groups, family-focused therapy, and community engagement—could mitigate loneliness and its downstream effects. Additionally cognitive-behavioral strategies aimed at reducing RNT may prove effective in addressing the psychological mechanisms contributing to cardiac distress73. Incorporating psychosocial interventions into standard cardiac care could significantly enhance patient outcomes.
Limitations and future directions
While this study provides valuable insights, certain limitations warrant consideration. The cross-sectional design precludes causal inferences, necessitating longitudinal studies to confirm the observed pathways. Additionally, self-reported measures of social support and isolation may be subject to bias. Future research could incorporate objective physiological and behavioral measures, such as heart rate variability or activity tracking, to complement self-reported data. Additionally, examining the role of other psychological mediators, such as anxiety, depression, or stress reactivity, could provide a more comprehensive understanding of the complex dynamics between social health and cardiac distress.
Conclusion
In conclusion, this study highlights the intricate relationships between social factors, loneliness, RNT, and cardiac distress in heart disease patients. The findings underscore the critical role of social support and isolation in shaping psychological processes that impact cardiac health. Interventions targeting both social and psychological domains hold promise for improving outcomes in this vulnerable population.
Data availability
The data supporting the findings of this study can be obtained from the corresponding author upon request. Please feel free to reach out for access to the data.
References
Susinski, S. et al. Psychological interventions targeting mental health and stress among females with cardiac disease: A scoping review. Can. J. Physiol. Pharmacol. (2024).
Jackson, A. C. et al. Unraveling the complexity of cardiac distress: A study of prevalence and severity. Front. Psychiatry. 13, 808904 (2022).
Murphy, B., Le Grande, M., Alvarenga, M., Worcester, M. & Jackson, A. Anxiety and depression after a cardiac event: prevalence and predictors. Front. Psychol. 10, 3010 (2020).
Ruppar, T. M., Cooper, P. S., Mehr, D. R., Delgado, J. M. & Dunbar-Jacob, J. M. Medication adherence interventions improve heart failure mortality and readmission rates: Systematic review and meta‐analysis of controlled trials. J. Am. Heart Assoc. 5 (6), e002606 (2016).
Kolandaivelu, K., Leiden, B. B., O’Gara, P. T. & Bhatt, D. L. Non-adherence to cardiovascular medications. Eur. Heart J. 35 (46), 3267–3276 (2014).
Iuga, A. O. & McGuire, M. J. Adherence and health care costs. Risk Manag. Healthc. Policy 35–44 (2014).
Cunningham, S. C., Keleman, A., Brandon, R., Groninger, H. & BrintzenhofeSzoc, K. Cardiac related psychosocial distress and traumatic distress in individuals with advanced heart failure. J. Soc. Work End-of-Life Palliat. Care. 19 (2), 103–117 (2023).
Kang, Q. & Luo, A. The efficacy of mindfulness-based intervention for heart diseases: A meta-analysis of randomized controlled trials. Medicine 101 (39), e29649 (2022).
Hassanpour, T., Mehrabi, S., Poursamad, A., ZandiGhashghaie, K. & Sharifi, M. Social support and social health. Iran. J. War Public. Health. 13 (3), 189–193 (2021).
Freak-Poli, R., Hu, J., Phyo, A. Z. Z. & Barker, F. Does social isolation, social support or loneliness influence health or well‐being after a cardiovascular disease event? A narrative thematic systematic review. Health Soc. Care Commun. 30 (1), e16–e38 (2022).
Azpiazu, L., Antonio-Agirre, I., Fernández-Zabala, A. & Escalante, N. How does social support and emotional intelligence enhance life satisfaction among adolescents? A mediational analysis study. Psychol. Res. Behav. Manag. 2341–2351 (2023).
Cené, C. W. et al. Effects of objective and perceived social isolation on cardiovascular and brain health: A scientific statement from the American heart association. J. Am. Heart Assoc. 11 (16), e026493 (2022).
Coyte, A. et al. Social relationships and the risk of incident heart failure: Results from a prospective population-based study of older men. Eur. Heart J. Open. 2 (1), oeab045 (2022).
Freak-Poli, R., Hu, J., Phyo, A. Z. Z. & Barker, S. F. Social isolation and social support influence health service utilisation and survival after a cardiovascular disease event: A systematic review. Int. J. Environ. Res. Public Health. 20 (6), 4853 (2023).
Blikman, M. J., Jacobsen, H. R., Eide, G. E. & Meland, E. How important are social support, expectations and coping patterns during cardiac rehabilitation. Rehabil. Res. Pract. 2014 (1), 973549 (2014).
Pahlevan Sharif, S. et al. Attachment: The mediating role of hope, religiosity, and life satisfaction in older adults. Health Qual. Life Outcomes. 19 (1), 57 (2021).
Teshale, A. B. et al. The relationship between social isolation, social support, and loneliness with cardiovascular disease and shared risk factors: A narrative review. Arch. Gerontol. Geriatr. 111, 105008 (2023).
Xia, N. & Li, H. Loneliness, social isolation, and cardiovascular health. Antioxid. Redox. Signal. 28 (9), 837–851 (2018).
Wang, F. et al. A systematic review and meta-analysis of 90 cohort studies of social isolation, loneliness and mortality. Nat. Hum. Behav. 7 (8), 1307–1319 (2023).
Blakoe, M., Berg, S. K., Højskov, I. E., Palm, P. & Bernild, C. Who cares? Perception of loneliness in patients treated for coronary heart disease. Global Qual. Nurs. Res. 9, 23333936211073613 (2022).
Trick, L., Watkins, E. R., Henley, W., Gandhi, M. M. & Dickens, C. Perseverative negative thinking predicts depression in people with acute coronary syndrome. Gen. Hosp. Psychiatry. 61, 16–25 (2019).
Guan, Y. Y. et al. Impact of rumination on severity and persistence of anxiety and depression in cardiac patients. Heart Mind. 5 (1), 9–16 (2021).
Tunheim, K. et al. Relationships between depression, anxiety, type D personality, and worry and rumination in patients with coronary heart disease. Front. Psychol. 13, 929410 (2022).
Yun, R. C., Fardghassemi, S. & Joffe, H. Thinking too much: How young people experience rumination in the context of loneliness. J. Community Appl. Social Psychol. 33 (1), 102–122 (2023).
Engel, G. L. The need for a new medical model: A challenge for biomedicine. Science 196 (4286), 129–136 (1977).
Cohen, S. & Wills, T. A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 98 (2), 310 (1985).
Uchino, B. N. Social support and health: A review of physiological processes potentially underlying links to disease outcomes. J. Behav. Med. 29, 377–387 (2006).
Cacioppo, J. T., Hawkley, L. C. & Thisted, R. A. Perceived social isolation makes me Sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago health, aging, and social relations study. Psychol. Aging. 25 (2), 453 (2010).
Aldao, A., Nolen-Hoeksema, S. & Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 30 (2), 217–237 (2010).
Nolen-Hoeksema, S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J. Abnorm. Psychol. 109 (3), 504 (2000).
Brosschot, J. F., Gerin, W. & Thayer, J. F. The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. J. Psychosom. Res. 60 (2), 113–124 (2006).
Ramesh, S., Besharat, M. A. & Nough, H. Relationship between worry, and anger rumination with cardiovascular disease severity: Social loneliness as a moderator. Arch. Iran. Med. 23 (3), 175–180 (2020).
Westland, J. C. Lower bounds on sample size in structural equation modeling. Electron. Commer. Res. Appl. 9 (6), 476–487 (2010).
Sun, S., Pan, W. & Wang, L. L. A comprehensive review of effect size reporting and interpreting practices in academic journals in education and psychology. J. Educ. Psychol. 102 (4), 989 (2010).
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E. & Tatham, R. Multivariate Data Analysis: Pearson Education (Upper Saddle River, 2010).
Le Grande, M. R. et al. Development of a short form of the cardiac distress inventory. BMC Cardiovasc. Disord. 23 (1), 408 (2023).
Zimet, G. D., Dahlem, N. W., Zimet, S. G. & Farley, G. K. The multidimensional scale of perceived social support. J. Pers. Assess. 52 (1), 30–41 (1988).
Bagherian-Sararoudi, R., Hajian, A., Ehsan, H. B., Sarafraz, M. R. & Zimet, G. D. Psychometric properties of the Persian version of the multidimensional scale of perceived social support in Iran. Int. J. Prev. Med. 4 (11), 1277–1281 (2013).
Bass, D. M. et al. Findings from a real-world translation study of the evidence-based partners in dementia care. Innov. Aging. 3 (3), igz031 (2019).
Fornell, C. & Larcker, D. F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 18 (1), 39–50 (1981).
McEvoy, P. M., Thibodeau, M. A. & Asmundson, G. J. Trait repetitive negative thinking: A brief transdiagnostic assessment. J. Exp. Psychopathol. 5 (3), 1–17 (2014).
Blakoe, M. et al. Prognostic value of a brief loneliness questionnaire for patients with coronary heart disease: Proposal for a prediction model. J. Clin. Nurs. 31 (11–12), 1686–1696 (2022).
Hosseini, L., Froelicher, E. S., Sharif Nia, H. & Ashghali Farahani, M. Psychometrics of Persian version of the 11 items de Jong Gierveld loneliness scale among an Iranian older adults population. BMC Public. Health. 21 (1), 2056 (2021).
Hou, D., Al-Tabbaa, A., Chen, H. & Mamic, I. Factor analysis and structural equation modelling of sustainable behaviour in contaminated land remediation. J. Clean. Prod. 84, 439–449 (2014).
Hosseini, L., Sharif Nia, H. & Ashghali Farahani, M. Development and psychometric evaluation of family caregivers’ hardiness scale: A sequential-exploratory mixed-method study. Front. Psychol. 13, 807049 (2022).
Pahlevan Sharif, S. et al. Retaining nurses via organizational support and pay during COVID-19 pandemic: The moderating effect between intrinsic and extrinsic incentives. Nurs. Open. 10 (1), 123–134 (2023).
Henseler, J., Ringle, C. M. & Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 43 (1), 115–135 (2015).
Saki, N. et al. Prevalence of cardiovascular diseases and associated factors among adults from Southwest Iran: Baseline data from Hoveyzeh cohort study. BMC Cardiovasc. Disord. 22 (1), 309 (2022).
Sadeghi, M., Haghdoost, A. A., Bahrampour, A. & Dehghani, M. Modeling the burden of cardiovascular diseases in Iran from 2005 to 2025: The impact of demographic changes. Iran. J. Public. Health. 46 (4), 506–516 (2017).
Beyranvand, M. R., Manhoobi, H., Shahraz, S. & Kolahi, A. A. Myocardial infarction in Iran: Epidemiology, management, and prognosis. J. Tehran Heart Cent. 18 (2), 82–86 (2023).
Hawkley, L. C. & Cacioppo, J. T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 40 (2), 218–227 (2010).
Harp, N. R. & Neta, M. Tendency to share positive emotions buffers Loneliness-Related negativity in the context of shared adversity. J. Res. Pers. 102 (2023).
Mook K. V. The Buffering Effect of Social Support in the Relation Between Loneliness and Life Satisfaction in Dutch MBO Students (2024).
Yazawa, A. et al. Can social support buffer the association between loneliness and hypertension? A cross-sectional study in rural China. PLoS One. 17 (2), e0264086 (2022).
Kim, H. H. & Jung, J. H. Negative ties, social support buffering, and loneliness: Findings from a cross-national survey. J. Social Personal Relat. 02654075241288721 (2024).
Parviniannasab, A. M., Faramarzian, Z., Hosseini, S. A., Hamidizadeh, S. & Bijani, M. The effect of social support, diabetes management self-efficacy, and diabetes distress on resilience among patients with type 2 diabetes: A moderated mediation analysis. BMC Public. Health. 24 (1), 477 (2024).
Coyle, C. E. & Dugan, E. Social isolation, loneliness and health among older adults. J. Aging Health. 24 (8), 1346–1363 (2012).
Holt-Lunstad, J., Smith, T. B. & Layton, J. B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 7 (7), e1000316 (2010).
Czaja, S. J., Moxley, J. H. & Rogers, W. A. Social support, isolation, loneliness, and health among older adults in the PRISM randomized controlled trial. Front. Psychol. 12, 728658 (2021).
Donovan, N. J. & Blazer, D. Social isolation and loneliness in older adults: Review and commentary of a National academies report. Am. J. Geriatr. Psychiatry. 28 (12), 1233–1244 (2020).
Gerlach, L. B., Solway, E. S. & Malani, P. N. Social isolation and loneliness in older adults. JAMA (2024).
Kaya, F. How does loneliness affect satisfaction with life? What is the role of the perception of god in this interaction? Front. Psychol. 16:1550108.
Luo, J. et al. A network analysis of rumination on loneliness and the relationship with depression. Nat. Ment. Health 1–12 (2024).
Finley, A. J. & Schaefer, S. M. Affective neuroscience of loneliness: Potential mechanisms underlying the association between perceived social isolation, health, and well-being. J. Psychiatr Brain Sci. 7(6) (2022).
Borawski, D. Authenticity and rumination mediate the relationship between loneliness and well-being. Curr. Psychol. 40 (9), 4663–4672 (2021).
McPhillips, R., Salmon, P., Wells, A. & Fisher, P. Qualitative analysis of emotional distress in cardiac patients from the perspectives of cognitive behavioral and metacognitive theories: Why might cognitive behavioral therapy have limited benefit, and might metacognitive therapy be more effective? Front. Psychol. 9, 2288 (2019).
Karki, M., Mahara, G., Heart & Diseases Anxiety disorders, and negative thoughts. Heart Mind. 6 (1), 22–25 (2022).
Fong, T. C., Leung, I. C., Wong, C. K., Jackson, A. C. & Ho, R. T. H. Psychometric validation of the cardiac distress Inventory-Short form among people with cardiac diseases in Hong Kong. Front. Psychiatry. 15, 1412264 (2024).
Levine, G. N. et al. Psychological health, well-being, and the mind-heart-body connection: A scientific statement from the American heart association. Circulation 143 (10), e763–e83 (2021).
Rossi, A. et al. The anxiety-buffer hypothesis in the time of COVID-19: When self-esteem protects from the impact of loneliness and fear on anxiety and depression. Front. Psychol. 11, 2177 (2020).
Singh, M. et al. Impact of social support on cardiovascular risk prediction models: A systematic review. Cureus 15 (9), e45836 (2023).
Fong, T. C., Lo, T. L. & Ho, R. T. Indirect effects of social support and hope on quality of life via emotional distress among stroke survivors: A three-wave structural equation model. Front. Psychiatry. 13, 919078 (2022).
Watkins, E. R. Rumination-Focused Cognitive-Behavioral Therapy for Depression (Guilford, 2018).
Acknowledgements
We express our sincere gratitude to all the patients who took part in this study and generously shared their valuable experiences with us. Additionally, we extend our thanks to the dedicated hospital staff in Amol, Iran, for their assistance in recruiting eligible participants and gathering pertinent data.
Author information
Authors and Affiliations
Contributions
Performance of data gathering: FM, SS; Planning and supervision of the work: HSH, SHH; Performance of the analysis: HSH, Manuscript draft: FM, AJ and All authors; and comment on the final manuscript: AJ and All authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Ethics Committee of Mazandaran University of Medical Sciences in Sari, Iran (code: IR.MAZUMS.REC.1403.338). Prior to data collection, participants received detailed information about the study’s objectives, procedures, potential risks, and benefits. They were given the opportunity to ask questions before providing written informed consent. For minors or individuals unable to consent independently, written consent was obtained from their legal guardians. The consent forms emphasized voluntary participation, confidentiality, anonymity, and the right to withdraw at any time without consequences. All procedures adhered to relevant ethical guidelines, including those set by the World Medical Association. Permissions to use data collection tools were obtained from their developers. The study was designed to minimize risks while safeguarding participant rights and well-being. Data were handled in compliance with institutional guidelines, ensuring secure storage and transparency regarding data usage in research dissemination.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sharif-Nia, H., Jackson, A.C., Salehi, S. et al. Loneliness and repetitive negative thinking mediate the link between social health and cardiac distress in heart disease patients. Sci Rep 15, 11804 (2025). https://doi.org/10.1038/s41598-025-96968-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96968-7
Keywords
This article is cited by
-
Psychokardiologie
Der Nervenarzt (2026)
-
Explainable AI models for identifying anxiety and distress in cardiac patients with ICDs
BMC Medical Informatics and Decision Making (2025)
-
Psychometric properties of the repetitive thinking questionnaire among Iranian patients with heart disease: validity and reliability assessment
BMC Psychology (2025)
