
Abstract
There is increasing evidence that air pollutants significantly increase the risk of cardiovascular disease (CVD). Nevertheless, less research has been conducted to date to reveal protective factors. Therefore, this study aims to indicate whether a healthy lifestyle can modify the effects of environmental pollution on CVD. This study screened 3010 participants from the China Health and Retirement Longitudinal Study (CHARLS) Wave 3 (2015). The study aimed to systematically demonstrate the impact of environmental pollution on CVD and elucidate the role of a healthy lifestyle. Air pollutant data were obtained from the China High Air Pollutant (CHAP) datasets. We analyzed the relationship between these pollutants and cardiovascular disease risk using generalized linear mixed models. In addition, healthy lifestyles were categorized as low, medium, and high; stratified analyses were conducted to estimate the effect of healthy lifestyles on the risk of CVD due to air pollutants. 607 had CVD among 3010 participants, and the three-year mean concentrations of the pollutants chloride ion (Cl−), nitrate ion (NO3−), particulate matter with a diameter of 10 micrometers or less (PM10), particulate matter with a diameter of 10 micrometers or less (PM1), particulate matter with a diameter of 10 micrometers or less (PM2.5) were each linked 1.37 (95%CI:1.22,1.54), 1.03 (95%CI:1.00,1.06), 1.02 (95%CI:1.01,1.03), 1.01 (95%CI:1.00,1.01), and 1.01 (95%CI:1.00,1.01) fold risk of CVD, respectively. For the subgroups of low, medium, and high according to the healthy lifestyle score in model 2, the average concentration of Cl− pollutant was each associated with 1.34 (1.12,1.62), 1.34 (1.12,1.61), and 1.32 (1.03,1.71) times risk with CVD, respectively. The NO3 − was each associated with 1.06 (1.02,1.11), 1.01 (0.97,1.05), and 0.98 (0.93,1.04) times risk with CVD, respectively. The PM1 was each associated with 1.03 (1.01,1.05), 1.01 (0.99,1.02), and 1.00 (0.97,1.02) times risk with CVD, respectively. The PM10 was each associated with 1.01 (1.00,1.01), 1.01 (0.99,1.01), and 1.00 (0.99,1.01) times risk with CVD, respectively. PM2.5 was each associated with 1.02 (1.01,1.03), 1.00 (0.99,1.01), and 1.00 (0.99,1.01) times risk with CVD, respectively. Exposure to these pollutants(Cl−, NO3−, PM10, PM1, PM2.5)is associated with higher risk of CVD, and healthier lifestyles can reduce the risk of CVD due to overall air pollutants.
Similar content being viewed by others


Introduction
Cardiovascular disease (CVD) is a general category of diseases that influence the blood vessels or the heart and is a highly prevalent disease among middle-aged and older adults worldwide1. It is estimated that the incidence of CVD in China will be on a rapid rise in the next few decades as the country enters a phase of rapid aging2. The World Health Organization has announced that by 2028, the number of people with CVD will reach 330 million in China3. The total number of CVD deaths in China has risen from 3.09 million to 4.58 million from 2005 to 20204. According to China’s mortality monitoring system, CVD is the primary disease causing death, which accounts for 47% and 48% in urban and rural areas, respectively5. The disability-adjusted life year (DALY) for CVD grew by 33% from 1990 to 2016, with men (52%) significantly higher than women (12%)6. Therefore, identifying risk and protective factors for CVD is essential for developing prevention strategies.
The traditional risk factors for cardiovascular control have a marginal decreasing effect, and researchers are focusing on finding other risk factors currently7,8. Accompanied by industrialization and urbanization, coal burning, industrial emissions, vehicle emissions, and straw burning have contributed to China’s severe air pollution, air pollution caused by industrialization is unavoidable for every individual9. Unlike traditional risk factors for cardiovascular disease, air pollution is passive and non-selective, and the long-term cumulative effect of air pollutants leads to an underestimation of the hazardous effects of chronic diseases10. Large amounts of pollutants such as soot, carbon monoxide, nitrogen oxides, sulfur dioxide, and other contaminants, and these pollutants are chemically transformed in the atmosphere to form fine particles such as PM2.5, PM10, and PM1, leading to severe air pollution11. Air pollution is a leading environmental risk factor for disease and premature death worldwide, which is strongly linked with adverse health consequences, such as cardiovascular, neurological, respiratory, and immune system diseases12. Air pollutants can act on the cardiovascular system through multiple targets such as entering the pulmonary circulation or disrupting the neuroendocrine-immune axis, which is as harmful as traditional risk factors13. Animal studies demonstrated long-term and short-term exposure to air pollutants can induce systemic inflammation and oxidative reactions, producing oxygen-free radicals, which leads to apoptosis and endothelial cell dysfunction, thereby inducing and promoting vascular calcification and increasing the risk of CVD14. Therefore, in recent years, hygiene practitioners have begun to focus on the impact of pollutants on people’s health. Most studies have revealed that a higher risk of CVD was associated with PM2.5, PM1, and PM1015,16. However, there are fewer studies on the relationship between the composition of PM2.5and cardiovascular risk17.
Most previous studies have revealed the role of individual lifestyles on CVD risk, including body mass index (BMI), dietary patterns, physical activity, sleep disorders, and other habits of daily living18,19,20,21. A meta-analysis of 142 studies from various countries, socioeconomic backgrounds, and ethnicities showed that a combination of healthy lifestyles was protective against CVD22. Simultaneously, the relationship between air pollutants and the risk of cardiovascular disease has been fully discussed in these studies23,24,25. It’s worth mentioning that another less well-studied question is whether a combined healthy lifestyle is a potential moderating protective factor for CVD risk from air pollutant exposure. Thus, it is plausible to postulate that healthy lifestyles would attenuate the adverse impact of CVD. So the study aimed to estimate the impact of air pollution and its constituents on the risk of CVD by generalized linear mixed analysis26. Second, the stratified analysis was conducted by calculating the healthy lifestyle scores, which we categorized into three subgroups: low, medium, and high, to assess the combined association between a healthy lifestyle and the risk of CVD due to exposure to air pollutants, and thus provide valuable insights into the reduction of the risk of CVD27. Third, we did the further analysis to explore the association between the air pollutant and the risk of CVD by baseline characteristic subgroups analysis.
Methods
Study design and population
We selected the study population from the nationally prospective population-based study CHARLS data, which the Biomedical Ethics Review Committee of Peking University authorized28. The study was conducted among community-dwelling elderly residents in 28 provinces in China29. A standardized questionnaire was administered to collect information on demographic characteristics (age, gender, residence, and marital status) by trained health workers, socioeconomic (education background, regional category, and annual household expenditure), health lifestyle characteristics (BMI, sleep duration, health physical activity, drinking status, and smoking status) and CVD conditions(hypertension, heart disease, and stroke). Participants were followed up every two years after signing the informed consent form from 2011 to 2020. 17,708 participants from wave 3 (2015) were recruited for the cross-sectional study. After excluding participants with missing data on age and gender (N = 657), missing information on marital status, residence, and education Status (N = 12), missing information on smoking status and drinking status (N = 59), missing information on sleep duration (N = 710), missing information on BMI (N = 1,701), missing information on annual household expenditure(N = 2,199), missing information on cooking fuel use(N = 2,139), missing information on hypertension, heart disease and stroke (N = 2,964). Finally, 3,010 individuals remained in the study, and the participant selection process is shown in Fig. 1.

The flowchart of enrolled participants.
Assessment of healthy lifestyle
The study team constructed a healthy lifestyle system including five items: smoking status, drinking status, sleep duration at night, healthy body mass index, and physical exercise27. First, no smoking is regarded as a healthy lifestyle in two ways: for ex-smokers who have never smoked or who have quit smoking, current smoking is viewed as an unhealthy lifestyle. Secondly, not drinking alcohol is considered a healthy lifestyle. In contrast, other drinking status (once a month, two to three times per month, one time per week, two to three times per week, four to six times per week, once a day, twice a day, and more than twice a day) were considered unhealthy drinking habits. Third, a complete sleep cycle consists of 3 stages of light sleep, deep sleep and rapid eye movement (REM), the total duration lasts 90 min, 7 h of sleep (about 4.5 cycles) is more likely to wake up naturally at the end of the sleep cycle, reducing sleepiness and fatigue brought about by sleep inertia30,31. So sleeping more than 7 h per day is identified as a healthy and ideal sleep duration in accordance with the National Sleep Foundation(NSF)32. Fourth, a body mass index (BMI) of less than 24 and more than 18.5 kg/m2is regarded as a healthy BMI33. Fifth, healthy physical activity is thirty minutes of moderate and strenuous physical activity thrice a week. Moderate exercise comprised rhythmic cycling, Tai chi, and fast walking. Strenuous exercise was aerobic, heavy physical labor, plowing, and weighted cycling. For each lifestyle factor, we assigned one score to the healthy level and zero to the unhealthy level27. Therefore, the healthy lifestyle score is the sum of five items, ranging from 0 to 5; lower scores reflect less healthy lifestyles27. The healthy lifestyle was categorized into three levels, including low health lifestyle (0, 1, and 2 healthy lifestyle scores), medium health lifestyle(3 healthy lifestyle scores), and high healthy lifestyle scores (4).
Assessment of air pollutants
We obtained data on ambient pollutants from the China High Air Pollutants (CHAP) (=https://weijing-rs.github.io/product.html)34. These datasets were derived from a space-time stochastic tree model that integrates provincial emission inventories, comprehensive atmospheric analyses, geo-remote sensing, and ground-based observations35. The daily concentration levels of PM1, PM2.5, PM10, and O3 were projected at a spatial resolution of 1 km × 1 km., and the daily concentration levels of NO3− and SO42−, NH4+, and Cl−were projected at a spatial resolution of 10 km × 10 km36, all these pollutants are measured in micrograms per cubic meter (µg/m3). The cross-validated root-mean-square errors for these datasets ranged from 0.80 to 0.92, which was high quality37. Following the confidentiality principles of this survey, participants were geocoded at the city level of their location. Therefore, for CHARLS database matching, air pollution exposures were included in the provincial averages, and participants residing in provinces shared the same air pollution exposure29. Based on previous literature, we used the average concentration of the 3 years before the year of the survey as the air pollution exposure36. We also used the average mean concentration with a lag of 2 years for sensitivity analyses34. The average concentration of pollutants in each province and city for the last three years (2013 - 2014 - 2015) is shown in Fig. 2. First, NO3− and SO42−, NH4+, and Cl− are important components of PM2.5 and PM1, the correlation between these pollutants were displayed in Fig. 3. Second, NO3− SO42−, and NH4+ mainly from human industrial production, agricultural activities and fossil fuel combustion, Cl−is mainly from the combustion of coal and garbage38. These pollutants are widespread in daily life and have a better water solubility of ions, which makes it easier for them to be inhaled by the respiratory system to settle in the alveoli and enter the blood circulation, thus affecting the biological function of the cardiovascular system39,40,41. Third, these pollutants have well-established detection methods, and the data are publicly available, easily accessible, and easy to analyze, so NO3−, SO42−, NH4+, and Cl−were chosen for the independent variable42.

The average concentration of pollutants in each province for the last three years (2013 - 2014 - 2015).

The Spearman’s correlation between each pollutant.
Assessment of outcomes
The status of CVD was based on self-reporting. Regarding high blood pressure, participants were asked: “Have you been previously diagnosed with hypertension?” For heart disease, “Have you been medically diagnosed with a heart attack, coronary congestive heart disease, angina pectoris, heart failure, or other heart problems?” For stroke, “Have you been diagnosed by a doctor with cerebrovascular disease (cerebrovascular accident, stroke)?“.
Covariates
These covariates selected for the study included age, gender(categorized as male and female), and residence (categorized as rural and city). Marital status was categorized as married (married with or without living with a spouse) and single (divorced, widowed, never married, and separate). Education status was grouped into elementary school or below and middle school or above. Regional category was categorized as western, eastern, and midland. The Eastern region includes Guangdong, Shanghai, Liaoning, Hebei, Zhejiang, Fujian, Beijing, Shandong, Jiangsu, Tianjin, and Hainan Provinces. The midland region includes the Inner Mongolia Autonomous Region, Hubei, Shanxi, Jiangxi, Henan, Hunan, Anhui, and Guangxi Provinces. The western region includes Ningxia Hui Autonomous Region, Sichuan, Yunnan, Shaanxi, Guizhou, Xinjiang Uygur Autonomous Region, Chongqing, Qinghai, Tibet Autonomous Region, Gansu, Jilin and Heilongjiang Provinces36. Cooking fuel use was classified as clean fuel and solid fue. Cleaner fuels include natural liquefied petroleum gas (LPG), biogas, and electricity, while solid fuels include crop residue, coal, and wood combustionl43. Annual household expenditures were categorized into quartile 1(Q1), quartile 2 (Q2), quartile 3(Q3), and quartile 4(Q4) based on a four-point scale from lowest to highest.
Statistical analysis
The baseline characteristic was described as means and standard deviation (SDs) for continuous variables, and frequencies and percentages were used to characterize the categorical variables. Differences in the characteristics of the participants at baseline were calculated using chi-square and t-tests, and associations for each ambient pollution were computed using the Spearman correlation coefficient. Generalized linear mixed models assessed the association between environmental pollutants and CVD based on the healthy lifestyle score44. We performed a stratified analysis based on baseline characteristics to identify these potential risk factors. The crude model was unadjusted; model 1 was adjusted for age, gender, residence, education status, marital status, and annual household expenditure. Model 2 was adjusted for these covariates from model 1 plus cooking fuel use. The average environmental pollution concentration in the latter two years (2016, 2017) was used as the independent variable to test the robustness of the results. The subgroups were used to test the robustness of the results. Further subgroup analyses explored trends between high and low lifestyle scores and the risk of CVD due to air pollution. Furthermore, the effects of overall air pollutants on CVD based on healthy lifestyle scores were analysis by weighted quantile sum (WQS) regression analysis, and weight values greater than 0.125 (1/N= 1/Number of pollutants) are considered statistically significant45. All statistical analyses were conducted by R Studio (4.4.2), a double-sided P value of less than 0.05 is considered statistically significant.
Results
Baseline characteristics
Table 1 showed the baseline characteristics of the 3010 participants in the study. The average age of the total population was (59.99 ± 9.73) years. There were 1,368 (45.45%) female, 1,866 (61.99%) rural household residents, 2,509 (83.36%) married, 1,995 (66.28%) with primary education or lower, 1,530 (50.83%) with healthy smoking habits, 2,595 (86.21%) with healthy drinking habits, 412 (46.21%) with more than 7 h sleep per day, 1420 (47.18%) with healthy body mass index, 1730 (57.48%) with using clean fuel, 1695 (56.31%) with healthy physical activity, the total health scores was 2.82 ± 1.09. The air pollutants were as follows: Cl−, NO3−, PM10, PM1, PM2.5, NH4+, O3, SO42−, descriptive statistics of 3-year levels of air pollution in 2013, 2014 and 2015 were listed in Table S1 in micrograms per cubic meter (µg/m3). The Spearman’s correlation between each pollutant was displayed in Fig. 3.
Relationship between air pollutants and CVD
Table 2 showed that air pollutants were associated with a high risk of cardiovascular disease in the general population. In the crude model, the average concentration of Cl−, NH4+, NO3−, PM1, PM10, and PM2.5 was associated with the increasing risk of CVD; the odds ratio was 1.37 (95% CI:1.22,1.53), 1.05 (95% CI:1.00,1.10), 1.03 (95% CI:1.01,1.06), 1.02 (95% CI:1.01,1.03), 1.01 (95% CI:1.00,1.01), and 1.01 (95% CI:1.00,1.01), respectively. After adjusting these covariates, including age, gender, residence, marital status, education status, regional category, and annual household expenditure, the average concentration of Cl−, NO3−, PM1, PM10, and PM2.5 was associated with the increasing risk of CVD; these odds ratios were 1.38 (95% CI:1.23,1.54), 1.03 (95% CI:1.00,1.06), 1.02 (95% CI:1.00,1.03), 1.01 (95% CI:1.00,1.01), and 1.01 (95% CI:1.00,1.01) in model 1, respectively. After adjusting these covariates including age, gender, residence, marital status, education status, regional category, annual household expenditure, and cooking fuel use, the average concentration of Cl−, NO3−, PM1, PM10, and PM2.5 was associated with the risk of CVD, these odds ratios were 1.37 (95% CI:1.22,1.54), 1.03 (95% CI:1.00,1.06), 1.02 (95% CI:1.01,1.03), 1.01 (95% CI:1.00,1.01), and 1.01 (95% CI:1.00,1.01) in model 2, respectively.
Analysis of the relationship between air pollutants and cardiovascular disease stratified by healthy lifestyle score
As shown in Table 2, the average concentration of Cl− was associated with an increasing risk of CVD after a stratified analysis according to the healthy lifestyle scores, with odds ratios of 1.34 (95% CI:1.12,1.62), 1.34 (95% CI:1.12,1.61) and 1.32 (95% CI: 1.03,1.71) respectively, for low, medium, and high healthy lifestyles subgroups in model 2. Mean NH4+ concentrations and odds ratios for CVD in the low, healthy lifestyle score subgroups were 1.09 (95% CI: 1.02,1.17) in model 2. Mean NO3− concentrations and odds ratios for CVD in the low healthy lifestyle score subgroups were 1.06 (95% CI: 1.02,1.11) in model 2. Mean PM1 concentrations and odds ratios for CVD in the low healthy lifestyle score subgroups were 1.03 (95% CI: 1.01,1.05) in model 2. Mean PM10 concentrations and odds ratios for CVD in the low healthy lifestyle score subgroups were 1.01 (95% CI: 1.00,1.01) in model 2. Mean PM2.5 concentrations and odds ratios for CVD in the low healthy lifestyle score subgroups were 1.02 (95% CI: 1.01,1.03) in model 2.
Subgroup analysis
The stratified analysis was shown in Table 3, where the mean concentrations of Cl− were significantly associated with an increased risk of CVD, except for group Q4 in annual household expenditures. In eastern China, the association between cardiovascular disease risk and NO3− was significant among married men who had an elementary school education or less, smoked, did not drink alcohol, slept less than 7 h per day, were physically inactive, and had low annual household expenditures. The association between CVD risk and PM1 was significant except for these participants who were female, more educated, did not smoke, drink alcohol, slept more than 7 h, had an unhealthy body mass index, were from the middle region, were physically active in a healthy way, and had higher annual household expenditures. The association between CVD risk and PM10 was significant except for participants from the western region with higher education levels and yearly household expenditures. The association between CVD risk and PM2.5 was significant except for women in the central region who were better educated, did not smoke, did not drink alcohol, slept more than 7 h, and had higher annual household expenditures.
Weighted quantile sum (WQS) regression analysis
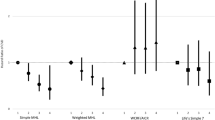
Figure 4 showed the weighted indices for different pollutants by weighted quantile sum (WQS) regression analysis. Figure 4-A showed the weighting indices for different pollutants, the weight index were 0.63 and 0.25 for Cl− and PM10, respectively for the overall population. Figure 4-B showed the weighting indices for different pollutants, the weight index were 0.63 and 0.25 for Cl− and PM10, respectively for these low health lifestyle scores population. Figure 4-C showed the weighting indices for different pollutants, the weight index were 0.52 and 0.33 for Cl− and PM10, respectively for these medium health lifestyle scores population. Figure 4-D showed the weighting indices for different pollutants, the weight index were 0.53, 0.25, and 0.19 for Cl−, O3 and PM10, respectively for these high health lifestyle scores population. Table 4 showed the effect of overall air pollutants on the risk of developing CVD based on the healthy lifestyle score through weighted quantile sum (WQS) regression analysis. After adjusting these covariates including age, gender, residence, marital status, education status, and regional category, the odds ratios of overall air pollutants to CVD risk were 1.28 (1.10–1.48) and 1.32 (1.04–1.67) for overall participants and low-scoring lifestyle participants, respectively (P < 0.05).

The weighted indices for different pollutants by weighted quantile sum (WQS) regression analysis.
Sensitivity analysis
We applied two methods to validate the robustness of the results. First, the average ambient pollution concentrations in the latter two years (2016 and 2017) were used as independent variables, and the results were presented in the supplementary material (Supplementary Table S2-S5) for low, medium, high and overall groups. Secondly, low, medium, and high subgroups were assessed using a healthy lifestyle score and analyses, as shown in the supplementary material (Supplementary Table S6-S8).
Discussion
Based on a national survey, the study assessed the association between air pollutant exposure and CVD. First, the results indicated a positive relationship between CVD and these air pollutants(Cl−, NO3−, PM1, PM10, and PM2.5). Second, the study was the first to assess the relationship between NH4+, SO42−, and Cl− with the risk of CVD. Third, the study evaluated the modifying effect of healthy lifestyles on CVD and found that a moderate to high rating of a healthy lifestyle attenuated CVD risk in Table 2. Forth, the study also assessed the effect of overall air pollutants on CVD based on healthy lifestyle scores through weighted quantile sum (WQS) regression analysis, we found the PM10, and Cl− had the highest weighted indices for CVD in Fig. 4, and moderate to high ratings of healthy lifestyles reduced the risk of cardiovascular disease in Table 4. This study was the first attempt to simultaneously evaluate the effects of pollutants and a healthy lifestyle on CVD. It provided insights into potential CVD strategies for prevention and health promotional decision-making.
PM2.5was the environment’s primary pollutant, particulate matter with a diameter smaller than or equivalent to 2.5 micrometers and a very complex composition16. Sun H et al. indicated that persistent exposure to PM2.5and its components were strongly correlated with increased hypertension46. Hayes RB et al.found PM2.5 exposure linked to mortality from ischemic heart disease and stroke47. Zhang S et al. also showed that higher PM2.5levels were related to a greater transition probability of disease progression and that the mediating role of air pollution became more pronounced as CVD progressed into the middle and late stages of life26. A meta-analysis from Krittanawong C, which enrolled 18 studies, has proved that an increasing level of PM2.5exposure results in a growing risk of CVD48. Recent studies have shown a positive correlation between air pollutants and CVD in other countries, regions, and ethnicities49,50,51. The mechanism is that PM2.5induces the body to produce reactive oxygen species (ROS), ROS-mediated inflammatory response, oxidative stress, and endoplasmic reticulum stress, further leading to dysfunction of vascular endothelial cells, proliferation and phenotypic transformation of blood vessel smooth muscle cells, and macrophage activation, which contributes to the occurrence of vascular calcification, and raises the risk of cardiovascular sclerosis such as myocardial infarction and cerebral infarction52.
Furthermore, exposure to PM1 and PM10can also increase the risk of CVD, which aligns with these previous studies6,48,51. As one of the common air pollutants, PM1is most closely associated with CVD, with a higher risk odds ratio, consistent with Yang BY’s study44. Mechanistically, the minor diameter PM1, which has a larger surface area-to-mass ratio, is more likely to be inhaled into the alveoli and enter the circulation and is more likely to carry more toxic components than PM10 and PM2.551,52.
We found the highest odds ratios between Cl− exposure and CVD risk among all these pollutants, which was consistent with the results of weighted quantile sum (WQS) regression analysis. The primary sources of Cl− (chlorine ions) in the atmosphere are coal being released to form gaseous chlorine after the combustion process, waste incineration with a relatively large proportion of HCl and Cl−, straw combustion, cooking, petrochemicals, rubber industry, and the paper industry are other sources of Cl−53. Given the pattern of industrial and agricultural development in the western part of the country, the average concentration of Cl− is also much higher than in the central and eastern regions of China, which was in line with previous studies showing that Cl−(chlorine ions) exposure was associated with CVD risk44,54,55. First, Cl−, a major component of PM2.5, increases the hygroscopicity of particulate matter and promotes deep alveolar deposition56. Cl−is usually combined with transition heavy metals (Pb, Cu) or organic carbon to form soluble complexes and enhance their biological activity, generating 3–5 times the excess of ROS compared to a single heavy metal pollutant, ROS demonstrated to lead to vascular endothelial cell damage, oxidative free radical production, and mitochondrial telomerase apoptosis54,57. Second, the Cl−activates the NF-κB pathway and increases the release of pro-inflammatory factors such as IL- 6 and TNF-α by promoting Toll-like receptor (TLR4) on the surface of alveolar macrophages58. Meanwhile, Cl−enhanced neutrophil infiltration and released myeloperoxidase (MPO)59. These inflammatory factors enter the blood circulation to further damage the vascular endothelium and accelerate endothelial atherosclerotic plaque formation60. Third, some experiments demonstrated that Cl−exposure activates carotid body chemoreceptors, leading to increased sympathetic excitability, which induces hypertension and tardive dyskinesia61. The study indicated that the Cl−concentration was correlated parasympathetic inhibition with reduced heart rate variability(HRV)59. Fourth, Cl- may promote platelet activation and increased fibrinogen levels through activation of reactive oxygen species(ROS), further elevating blood viscosity and contributing to the development of stroke58.
Atmospheric NO3−comes mainly from the combustion of petroleum fuels, coal, and natural gas and the emission of ammonia-containing wastes62,63. Li J et al.found an apparent correlation between prolonged exposure to NO3−and elevated systolic blood pressure (SBP) in the younger population64. Zhang S et al. also indicated that long-term NOx exposure was correlated with a higher transition probability from pre-hypertension to hypertension and or pre-hypertension to CVD26. In addition, these previous studies also confirmed a positive association between NO3−exposure and CVD in older people65,66,67.
The first finding is a strong association between air pollutants and the risk of CVD, which aligns with these previous findings. However, fewer studies are addressing the association between a healthy lifestyle and CVD risk attributed to air pollution. Therefore, the study scored participants’ healthy lifestyles and developed a generalized linear model to evaluate the association between the risk of CVD prevalence due to exposure to air pollutants and healthy lifestyles. Furthermore, the weighted quantile sum (WQS) regression analysis was applied to evaluate the effect of the overall air pollutants on CVD disease risk. The second meaningful finding is that a healthy lifestyle plays a mitigating role in pollutant exposure and CVD risk, even among participants exposed to atmospheric pollutants, which has not been reported in previous studies. In Table 2, we found that the mitigating effect was more pronounced in the subgroup with moderately high healthy lifestyle scores, thus suggesting that populations with higher healthy lifestyle scores have lower odds ratios for CVD due to air pollutants exposure. The attenuating effect of a healthy lifestyle on the risk of CVD due to air pollutant exposure is more pronounced for these particles and their constituents, including Cl−, NO3−, PM2.5, PM1, and PM10. In Table 4, the attenuating effect of healthy lifestyles is also shown in the effect of overall air pollutants on CVD disease risk. Wei Chen et al. found that people with healthy lifestyles had a lower risk of cardiometabolic diseases due to indoor air pollution, emphasizing that maintaining a healthy lifestyle can reduce the absolute risk of developing cardiometabolic multimorbidity (CMM)68.
The exact moderating mechanisms between air pollutants and higher healthy lifestyles on CVD risk are unclear, the protective effect of a healthier lifestyle against air pollution-induced harm to the cardiovascular system is biologically plausible. First, mounting evidence supported regular exercise can prevent the development of CVD from observational and cohort studies69,70,71,72. Vega RB et al. showed that long-term physical activity promotes cardiac remodeling by antagonizing the pathological pathway insulin-like growth factor 1/PI3 K/Akt pathway73. Kim SR et al. found that reduced physical activity was strongly associated with elevated cardiovascular disease risk when exposure to low to medium concentrations of PM2.5 or PM1074. A meta-analysis from Juneja Gandhi T revealed that the positive effects of outdoor physical activity on cardiovascular health exceeded the harmful effects of air pollution on the cardiovascular system75. Secondly, long-term healthy sleep patterns can counteract the harmful effects of air pollutants on the organism by increasing GHS levels, melatonin and immune cell activity, and by promoting accelerated regeneration of respiratory mucosal cells76,77. Third, the smoking process produces large amounts of free radicals that directly attack endothelial cells and cause mitochondrial damage78. Nicotine, by inhibiting endothelial-type nitric oxide synthase (eNOS), contributes to the promotion of a constricted state of the vasculature, promotes the expression of the P2Y12 receptor on the platelet surface, and facilitates platelet aggregation and cross-linking of fibrinogen, resulting in the formation of thrombi79,80. Similarly, after alcohol consumption, ethanol results in metabolism of ethanol dehydrogenase (ADH) to acetaldehyde producing cardiomyocytotoxicity, causing lipid metabolism disorders, and contributing to inflammation and fibrosis in cardiomyocytes81,82. Moreover, numerous experiments have shown that concurrent alcohol and cigarette smoking have a synergistic effect, with ROS leading to multiplication of oxidative damage, amplification of inflammatory cascades, and epigenetic modifications83,84. Non-drinking and non-smoking are considered to be healthy lifestyles that greatly reduce the damage of these harmful substances on the body85. Forth, it is widely acknowledged by the public that a normal BMI is a protective factor against CVD86. Participants with a healthy body mass index have higher insulin sensitivity, vascular elasticity, endothelial cell repair, and lower levels of visceral fat, all of which protect against the harmful effects of air pollutants on the body87.
The effects of air pollution are unavoidable and show geographic variability, so we focused on the role of healthy lifestyles in preventing cardiovascular disease caused by air pollutants in this study. Therefore, we propose a new concept of “environment-behavior-physiology” model of dynamic interactions, which defines a healthy lifestyle as a “biofilter” of the toxic effect of the environment, primarily through the modulation of exogenous exposures and the enhancement of endogenous resistance to reduce the risk of causing air pollutants that contribute to cardiovascular disease risk88. The attenuating effect on the risk of air pollution-induced CVD only became apparent with the increasing healthy lifestyle score. In the study, the interesting finding of this study was this mitigating effect on environmental pollution was only observed in participants with lifestyle scores greater than 2, which may be due to a bioaccumulative effect or synergistic interaction89. The combined antioxidant, anti-inflammatory or metabolite antitoxic effects can only reach the physiological offset threshold for toxic loads from air pollutants when health behaviors accumulate to critical levels90. First, coordinated defense is an important mechanism in attenuating effect, the benefits of healthy lifestyle behaviors with low scores do not offset the harmful effects of environmental pollution on the cardiovascular system, it is only through the combination of multiple behaviors that high scoring healthy lifestyle scorers reach complementary pathways and form an integrated defense network that can be manifested at the epidemiological level in the population91,92. Second, the bioaccumulative effect may arise from a nonlinear dose-response equation in which multiple health behaviors work simultaneously a threshold effect only occurs when health behaviors accumulate to a critical level93.
Therefore, adherence to a healthier lifestyle is beneficial in reducing the risk of cardiovascular disease caused by air pollution. In summary, a healthy lifestyle can reduce systemic inflammation and oxidative stress, which tend to be increased by exposure to air pollutants and are correlated with a higher risk of developing CVD94. A healthy lifestyle also can increase anti-inflammatory markers and boost the body’s antioxidant defenses, thereby helping to reduce air pollutant-induced inflammation95. Second, as the most critical component of healthy lifestyles, healthy physical activity can reduce cortisol levels, which physiologically promotes vasoconstriction, elevated blood pressure, elevated blood glucose, and increased levels of free fatty acids in the blood96, thus making the individual less susceptible to the harmful effects of air pollutants97.
Cl−, NO3−, PM2.5, PM1, and PM10 were associated with higher CVD risk, whereas NH4+, O3 − and SO42− were not. Stratified analyses showed that males with elementary school education or less, smokers, insufficient sleep, no healthy physical activity, and from low-income households were more sensitive to the adverse impact of PM10, PM1, PM2.5, and its constituents (NO3 − and Cl−). In terms of association with CVD risk, the interaction of Cl−, PM10, PM1, and PM2.5 was significant in the educational status subgroup, the interaction of NO3−, PM1, and PM2.5 was significant in the subgroup for sleep duration, and the interaction of Cl − and PM1 were significant in the subgroup for the regional category. Although the specific mechanisms of the complicated interactions between air pollutants and these demographic characteristics remain unknown, our findings provide scientific evidence for preventing CVD.
Some strengths should be acknowledged in the study. First, previous studies have demonstrated the relationship between specific air pollutants of different diameters and CVD risk, but have not examined the relationship between the specific constituents of these substances and CVD risk. The present study evaluated the relationship between the specific constituents of these specific air pollutants (NH4+, SO42−, and Cl−) and CVD risk for the first time. Second, we apply two methods to test the robustness of our results; the average air pollutant concentration for the following two years was used as the dependent variable. The subgroups were conducted according to the healthy lifestyle scores, and the same trend was shown in the stratified analysis. Third, we used three models to evaluate the association between pollutants and the risk of CVD and adjusted for cooking fuel as a covariate to control the effects of household pollution. Fourth, the study reports for the first time the mitigating impact of a healthy lifestyle on the risk of CVD due to air pollutants. Fifth, the weighted quantile sum (WQS) regression analysis was applied to evaluate the effect of the overall air pollutants on CVD disease risk.
Meanwhile, some limitations should be noted. First, the ventilation coefficient, thermal inversions, and potential covariates were considered to adjust for model effects. Second, the dependent variable in this study was the CVD situation via self-reporting, which was a lack of more objective diagnostic records or laboratory tests.
Conclusion
This study provides more evidence that air pollution increases the risk of CVD, which including Cl−, NO3−, PM2.5, PM1, and PM10. For these air pollution constituents, including Cl−, NO3−, PM2.5, PM1, and PM10, moderate and high lifestyle scores were associated with lower risk of cardiovascular disease due to air pollution. The attenuating effect of healthy lifestyles was also reflected in the overall effect of air pollutants on CVD risk by gWQS analysis after adjusting these covirates.
Data availability
Data is provided within the manuscript or supplementary information files.
References
Chen, Y. et al. Early adulthood BMI and cardiovascular disease: a prospective cohort study from the China kadoorie biobank. Lancet Public. Health. 9 (12), e1005–e1013 (2024).
Diao, T. et al. Changes in sleep patterns, genetic susceptibility, and incident cardiovascular disease in China. JAMA Netw. Open. 7 (4), e247974 (2024).
Du, X., Patel, A., Anderson, C. S., Dong, J. & Ma, C. Epidemiology of cardiovascular disease in China and opportunities for improvement: JACC international. J. Am. Coll. Cardiol. 73 (24), 3135–3147 (2019).
Li, F. et al. Association between the cumulative average triglyceride glucose-body mass index and cardiovascular disease incidence among the middle-aged and older population: a prospective nationwide cohort study in China. Cardiovasc. Diabetol. 23 (1), 16 (2024).
Wang, L. et al. A prospective study of waist circumference trajectories and incident cardiovascular disease in China: the Kailuan cohort study. Am. J. Clin. Nutr. 113 (2), 338–347 (2021).
Liang, F. et al. Long-Term exposure to fine particulate matter and cardiovascular disease in China. J. Am. Coll. Cardiol. 75 (7), 707–717 (2020).
Mehta, L. S. Cardiovascular Disease Risk Factors in Women: The Impact of Race and Ethnicity: A Scientific Statement From the American Heart Association. 147(19):1471–1487. (2023).
Teo, K. K. & Rafiq, T. Cardiovascular risk factors and prevention: A perspective from developing countries. Can. J. Cardiol. 37 (5), 733–743 (2021).
Lan, J. et al. Effects of ambient air pollution on outpatient visits for psoriasis in Wuhan, China: a time-series analysis. Br. J. Dermatol. 188 (4), 491–498 (2023).
Bhatnagar, A. Cardiovascular effects of particulate air pollution. Annu. Rev. Med. 73, 393–406 (2022).
Shan, Y., Wang, X. & Wang, Z. The pattern and mechanism of air pollution in developed coastal areas of China: from the perspective of urban agglomeration. 15(9):e0237863. (2020).
Sing, T. F., Wang, W. & Zhan, C. Tracking industry pollution sources and health risks in China. Sci. Rep. 13 (1), 22232 (2023).
Lederer, A. M., Fredriksen, P. M., Nkeh-Chungag, B. N. & Everson, F. Cardiovascular effects of air pollution: current evidence from animal and human studies. 320(4):H1417–h1439. (2021).
Fitriyah, A. et al. Exposure to ambient air pollution and osteoarthritis; an animal study. Chemosphere 301, 134698 (2022).
Wang, J. et al. Direct and indirect consumption activities drive distinct urban-rural inequalities in air pollution-related mortality in China. Environ. Health Perspect. 69 (4), 544–553 (2024).
Yang, Z. et al. Understanding China’s industrialization driven water pollution stress in 2002-2015-A multi-pollutant based net Gray water footprint analysis. J. Environ. Manage. 310, 114735 (2022).
Yu, L. J. et al. Short-Term exposure to ambient air pollution and influenza: A multicity study in China. 131(12):127010. (2023).
Kaminsky, L. A. et al. The importance of healthy lifestyle behaviors in the prevention of cardiovascular disease. Prog. Cardiovasc. Dis. 70, 8–15 (2022).
Huang, Y. et al. Healthy lifestyle habits, educational attainment, and the risk of 45 age-related health and mortality outcomes in the UK: A prospective cohort study. J. Nutr. Health Aging. 29 (5), 100525 (2025).
Shan, Y., Bertrand, K. A., Petrick, J. L., Sheehy, S. & Palmer, J. R. Planetary health diet index in relation to mortality in a prospective cohort study of united States black females. Am. J. Clin. Nutr. 121 (3), 589–596 (2025).
Tian, F. et al. Post-cardiovascular disease healthy lifestyle, inflammation and metabolic biomarkers, and risk of dementia: a population-based longitudinal study. Am. J. Clin. Nutr. 121 (3), 511–521 (2025).
Zhang, Y. B. et al. Combined lifestyle factors, all-cause mortality and cardiovascular disease: a systematic review and meta-analysis of prospective cohort studies. J. Epidemiol. Commun. Health. 75 (1), 92–99 (2021).
Peralta, A. A. et al. Low-level PM 2.5 exposure, cardiovascular and nonaccidental mortality, and related health disparities in 12 US States. Epidemiol. (Cambridge Mass). 36 (2), 253–263 (2025).
Wu, D. et al. Effect of PM(2.5) and its constituents on hospital admissions for cardiometabolic Multimorbidity in Urumqi, China. Sci. Rep. 15 (1), 6394 (2025).
Zou, Z. et al. Heat wave, fine particulate matter, and cardiovascular disease mortality: A time-stratified case-crossover study in Shenzhen, China. Ecotoxicol. Environ. Saf. 292, 117944 (2025).
Zhang, S., Qian, Z. M. & Chen, L. Exposure to air pollution during Pre-Hypertension and subsequent hypertension, cardiovascular disease, and death: A trajectory analysis of the UK biobank cohort. 131(1):17008. (2023).
Guo, C. et al. Associations of healthy lifestyle and three latent socioeconomic status patterns with physical Multimorbidity among middle-aged and older adults in China. Prev. Med. 175, 107693 (2023).
Yao, Y., Wang, K. & Xiang, H. Association between cognitive function and ambient particulate matters in middle-aged and elderly Chinese adults: evidence from the China health and retirement longitudinal study (CHARLS). Sci. Total Environ. 828, 154297 (2022).
Han, S. et al. Systemic inflammation accelerates the adverse effects of air pollution on metabolic syndrome: findings from the China health and retirement longitudinal study (CHARLS). Environ. Res. 215 (Pt 1), 114340 (2022).
Patterson, F., Grandner, M. A., Lozano, A., Satti, A. & Ma, G. Transitioning from adequate to inadequate sleep duration associated with higher smoking rate and greater nicotine dependence in a population sample. Addict. Behav. 77, 47–50 (2018).
Patterson, F. et al. Interactive effects of sleep duration and morning/evening preference on cardiovascular risk factors. Eur. J. Pub. Health. 28 (1), 155–161 (2018).
Nelson, K. L. & Davis, J. E. Sleep quality: an evolutionary concept analysis. 57(1):144–151. (2022).
Dugmore, J. A., Winten, C. G., Niven, H. E. & Bauer, J. Effects of weight-neutral approaches compared with traditional weight-loss approaches on behavioral, physical, and psychological health outcomes: a systematic review and meta-analysis. Nutr. Rev. 78 (1), 39–55 (2020).
Zhao, Q., Feng, Q. & Seow, W. J. Impact of air pollution on depressive symptoms and the modifying role of physical activity: evidence from the CHARLS study. J. Hazard. Mater. 482, 136507 (2024).
Chen, N., Ma, L. L., Zhang, Y. & Yan, Y. X. Association of household solid fuel use and long-term exposure to ambient air pollution with estimated 10-year high cardiovascular disease risk among postmenopausal women. Environmental pollution (Barking, Essex: 2024, 342:123091. (1987).
Jiang, H. et al. Does physical activity attenuate the association between ambient PM(2.5) and physical function? Sci. Total Environ. 874, 162501 (2023).
Yu, Y. et al. Association of residential greenness, air pollution with adverse birth outcomes: results from 61,762 mother–neonatal pairs in project ELEFANT (2011–2021). Sci. Total Environ. 912, 169549 (2024).
Niu, L., Ye, H., Xu, C., Yao, Y. & Liu, W. Highly time- and size-resolved fingerprint analysis and risk assessment of airborne elements in a megacity in the Yangtze river delta, China. Chemosphere 119, 112–121 (2015).
Environmental health: a global access science source.
Gao, N. et al. Lung function and systemic inflammation associated with short-term air pollution exposure in chronic obstructive pulmonary disease patients in Beijing. China 19 (1), 12 (2020).
Wu, X., Chen, B., Wen, T., Habib, A. & Shi, G. Concentrations and chemical compositions of PM(10) during hazy and non-hazy days in Beijing. J. Environ. Sci. 87, 1–9 (2020).
Yang, S. et al. Haze formation indicator based on observation of critical carbonaceous species in the atmosphere. Environmental pollution (Barking, Essex: 2019, 244:84–92. (1987).
Xu, T. et al. Association between solid cooking fuel and cognitive decline: three nationwide cohort studies in middle-aged and older population. Environ. Int. 173, 107803 (2023).
Yang, B. Y. et al. Association of Long-term exposure to ambient air pollutants with risk factors for cardiovascular disease in China. JAMA Netw. Open. 2 (3), e190318 (2019).
Jiang, Y., Du, C. & Chen, R. Differential effects of fine particulate matter constituents on acute coronary syndrome onset. 15(1):10848. (2024).
Sun, H. & Chen, X. Association between Long-Term exposure to PM(2.5) inorganic chemical compositions and cardiopulmonary mortality: A 22-Year cohort study in Northern China. 2(8):530–540. (2024).
Hayes, R. B. et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int. J. Epidemiol. 49 (1), 25–35 (2020).
Krittanawong, C. et al. PM2.5 and cardiovascular health risks. Curr. Probl. Cardiol. 48 (6), 101670 (2023).
Wang, M. et al. Ambient air pollution, healthy diet and vegetable intakes, and mortality: a prospective UK biobank study. 51(4):1243–1253. (2022).
de Bont, J. et al. Ambient air pollution and cardiovascular diseases: an umbrella review of systematic reviews and meta-analyses. 291(6):779–800. (2022).
Hayes, R. B. et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Environ. Health Perspect. 49 (1), 25–35 (2020).
Ding, R., Huang, L., Yan, K., Sun, Z. & Duan, J. New insight into air pollution-related cardiovascular disease: an adverse outcome pathway framework of PM2.5-associated vascular calcification. Cardiovascular. Res. 120 (7), 699–707 (2024).
Wang, X. et al. The role of sources and meteorology in driving PM(2.5)-bound Chlorine. J. Hazard. Mater. 441, 129910 (2023).
Vieira de Oliveira Salerno, P. R. et al. The cardiovascular disease burden attributable to particulate matter pollution in South America: analysis of the 1990–2019 global burden of disease. Public. Health. 224, 169–177 (2023).
Vienneau, D. et al. More than clean air and tranquillity: residential green is independently associated with decreasing mortality. Environ. Int. 108, 176–184 (2017).
Bravo-Linares, C. et al. Source identification, apportionment and toxicity of indoor and outdoor PM2.5 airborne particulates in a region characterised by wood burning. Environ. Sci. Processes Impacts. 18 (5), 575–589 (2016).
Cui, M. et al. Chemical composition of PM2.5 from two tunnels with different vehicular fleet characteristics. Sci. Total Environ. 550, 123–132 (2016).
Osornio-Vargas, A. R. et al. In vitro biological effects of airborne PM₂.₅ and PM₁₀ from a semi-desert City on the Mexico-US border. Chemosphere 83 (4), 618–626 (2011).
Valdés, A. et al. Elemental concentrations of ambient particles and cause specific mortality in Santiago, Chile: a time series study. Environ. Health: Global Access. Sci. Source. 11, 82 (2012).
Wang, X. et al. [Pollution characteristics and source apportionment of PM₂.₅, in Lanzhou City]. Huan Jing Ke xue = Huanjing Kexue. 37 (5), 1619–1628 (2016).
Yang, L. et al. Impacts of firecracker burning on aerosol chemical characteristics and human health risk levels during the Chinese new year celebration in Jinan, China. Sci. Total Environ. 476–477, 57–64 (2014).
Cao, M. et al. Domestic wastewater causes nitrate pollution in an agricultural watershed, China. Sci. Total Environ. 823, 153680 (2022).
Wang, H. et al. Formation mechanism and control strategy for particulate nitrate in China. J. Environ. Sci. 123, 476–486 (2023).
Li, J. et al. Long-term effects of PM(2.5) components on blood pressure and hypertension in Chinese children and adolescents. Environ. Int. 161, 107134 (2022).
Feng, J. et al. The effects of long-term exposure to air pollution on incident mental disorders among patients with prediabetes and diabetes: findings from a large prospective cohort. Sci. Total Environ. 897, 165235 (2023).
Wu, Y. et al. Ambient air pollution associated with incidence and dynamic progression of type 2 diabetes: a trajectory analysis of a population-based cohort. 20(1):375. (2022).
Zou, H. et al. Ambient air pollution associated with incidence and progression trajectory of cardiometabolic diseases: A multi-state analysis of a prospective cohort. BMC Med. 862, 160803 (2023).
Chen, W. et al. Household air pollution, adherence to a healthy lifestyle, and risk of cardiometabolic Multimorbidity: results from the China health and retirement longitudinal study. Sci. Total Environ. 855, 158896 (2023).
Fukuie, M. et al. The effect of Head-Out aquatic exercise on arterial stiffness in Middle-Aged and elderly people. Pulse (Basel Switzerland). 7 (1–4), 51–59 (2020).
Garnvik, L. E. et al. Physical activity, cardiorespiratory fitness, and cardiovascular outcomes in individuals with atrial fibrillation: the HUNT study. Eur. Heart J. 41 (15), 1467–1475 (2020).
Lima, T. R., González-Chica, D. A., Moreno, Y. M. F. & Silva, D. A. S. Healthy lifestyle moderates the relationship between cardiovascular disease with blood pressure, body composition, carotid intima-media thickness, and glycated hemoglobin among adults. Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme 45(5):539–546. (2020).
Speer, K. E., Semple, S., Naumovski, N. & McKune, A. J. Heart rate variability for determining autonomic nervous system effects of lifestyle behaviors in early life: A systematic review. Physiol. Behav. 217, 112806 (2020).
Vega, R. B., Konhilas, J. P., Kelly, D. P. & Leinwand, L. A. Molecular mechanisms underlying cardiac adaptation to exercise. Cell Metabol. 25 (5), 1012–1026 (2017).
Kim, S. R., Choi, S., Keum, N. & Park, S. M. Combined effects of physical activity and air pollution on cardiovascular disease: A Population-Based study. J. Am. Heart Association. 9 (11), e013611 (2020).
Juneja Gandhi, T., Garg, P. R. & Kurian, K. Outdoor physical activity in an air polluted environment and its effect on the cardiovascular System-A systematic review. 19(17). (2022).
Chatburn, A., Lushington, K. & Kohler, M. J. Complex associative memory processing and sleep: a systematic review and meta-analysis of behavioural evidence and underlying EEG mechanisms. Neurosci. Biobehav. Rev. 47, 646–655 (2014).
Ohayon, M. M., Carskadon, M. A., Guilleminault, C. & Vitiello, M. V. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep 27 (7), 1255–1273 (2004).
England, L. J. et al. Developmental toxicity of nicotine: A transdisciplinary synthesis and implications for emerging tobacco products. Neurosci. Biobehav. Rev. 72, 176–189 (2017).
Levy, D. T. et al. A framework for evaluating the public health impact of e-cigarettes and other vaporized nicotine products. Addict. (Abingdon England). 112 (1), 8–17 (2017).
Schauer, G. L., Rosenberry, Z. R. & Peters, E. N. Marijuana and tobacco co-administration in blunts, spliffs, and mulled cigarettes: A systematic literature review. Addict. Behav. 64, 200–211 (2017).
Barve, S., Chen, S. Y., Kirpich, I., Watson, W. H. & McClain, C. Development, prevention, and treatment of Alcohol-Induced organ injury: the role of nutrition. Alcohol Research: Curr. Reviews. 38 (2), 289–302 (2017).
Piano, M. R. Alcohol’s effects on the cardiovascular system. Alcohol Research: Curr. Reviews. 38 (2), 219–241 (2017).
Fernandez-Bustamante, A. & Repine, J. E. Chronic inflammatory diseases and the acute respiratory distress syndrome (ARDS). Curr. Pharm. Design. 20 (9), 1400–1408 (2014).
Vrdoljak, D. et al. Lifestyle intervention in general practice for physical activity, smoking, alcohol consumption and diet in elderly: a randomized controlled trial. Arch. Gerontol. Geriatr. 58 (1), 160–169 (2014).
Wilson, D. E. et al. Lifestyle factors in hypertension drug research: systematic analysis of articles in a leading Cochrane report. Int. J. Hypertens. 2014, 835716 (2014).
Ricci, G., Pirillo, I., Tomassoni, D., Sirignano, A. & Grappasonni, I. Metabolic syndrome, hypertension, and nervous system injury: Epidemiological correlates. Clinical and experimental hypertension (New York, NY: 2017, 39(1):8–16. (1993).
Due, A. et al. The effect of three different ad libitum diets for weight loss maintenance: a randomized 18-month trial. Eur. J. Nutr. 56 (2), 727–738 (2017).
Palacz-Poborczyk, I. & Chamberlain, K. ‘A healthy lifestyle is a journey’: exploring health perceptions and self-defined facilitators to health through photo-elicitation. 40(4):652–680. (2025).
Feng, Y. et al. Lifestyle behaviours and physical, psychological, and cognitive Multimorbidity among older hypertensive population in remote areas of China. Sci. Rep. 241, 24–32 (2025).
Jowshan, M. R., Pourjavid, A. & Amirkhizi, F. Adherence to combined healthy lifestyle and odds of metabolic syndrome in Iranian adults: the PERSIAN dena cohort study. 15(1):5164. (2025).
Qiao, L. et al. Combined healthy lifestyle behaviors and all-cause mortality risk in middle-aged and older US adults: A longitudinal cohort study. Arch. Gerontol. Geriatr. 130, 105702 (2025).
Zuo, W. & Yang, X. Joint association of diet quality and physical activity with obstructive sleep apnea: A cross-sectional study. Prev. Med. 192, 108226 (2025).
Yuan, Y., Tian, P., Li, L. & Qu, Q. Comparison of the associations between life’s essential 8 and life’s simple 7 with stroke: NHANES 1999–2018. J. Stroke Cerebrovasc. Diseases: Official J. Natl. Stroke Association. 34 (3), 108238 (2025).
Li, Y. et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: prospective cohort study. BMJ (Clinical Res. ed). 368, l6669 (2020).
Han, H. et al. Association of a healthy lifestyle with All-Cause and Cause-Specific mortality among individuals with type 2 diabetes: A prospective study in UK biobank. 45(2):319–329. (2022).
Kaminsky, L. A. et al. The importance of healthy lifestyle behaviors in the prevention of cardiovascular disease. BMJ (Clinical Res. ed). 70, 8–15 (2022).
Zhang, Y. B. et al. Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies. 373:n604. (2021).
Funding
This work was supported by the Program for Research Fund for Key Programs at the University Level (Humanities and Social Sciences, WK2024SZD03), 2020 Provincial Student Innovation and Entrepreneurship Program Project (No: S202010368023), 2023 Provincial Student Innovation and Entrepreneurship Program Project (No: S202310368040); 2024 Provincial and National Student Innovation and Entrepreneurship Program Project (No: S202410368044; No: 202410368044).
Author information
Authors and Affiliations
Contributions
C-z W and MW conception and design of this study, C-z W wrote the main manuscript text, MW analyzed the data, C-z W and MW revised and reviewed the thesis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The data are openly assessed as microdata at http://opendata.pku.edu.cn/dataverse/ CHARLS, with no direct contact with all participants. According to the Declaration of Helsinki, related norms, and the Medical Ethics Committee, all partners signed an informed consent form and all steps and methods before enrollment. The research was approved by the Medical Ethics Committee of Wannan Medical College in China(approval number 20240003).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, C., Wang, M. Healthier lifestyles can modify the air pollutants effect on cardiovascular disease among the middle-aged and elderly. Sci Rep 15, 14293 (2025). https://doi.org/10.1038/s41598-025-97093-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97093-1
