
Abstract
New disposable e-cigarettes are popular, especially among young people. This study aimed to assess their addictive potential by examining puffing behaviors, subjective effects, and conducting laboratory investigations in an experimental setting. Single-center, four-arm, crossover study. Laboratory setting in Munich (LMU-University Hospital), Germany. Eighteen occasionally cigarette-smoking adults aged 19–28. Two disposable e-cigarettes of the same brand (strawberry-kiwi/ tobacco flavored) were tested with a cigarette and a conventional pod e-cigarette as comparators. Usage was ad libitum for 5 min (or the duration of smoking one cigarette) while puffing topography was recorded. Distributed over 30 min blood samples for nicotine plasma concentrations were drawn and hemodynamic parameters and subjective effects assessed. Nicotine delivery of disposable e-cigarettes (Cmax strawberry-kiwi: 7.1 ng/ml, tobacco: 6.9 ng/ml) was similar to the cigarette (8.1 ng/ml) and higher than for the pod e-cigarette (3.1 ng/ml). The nicotine plasma increase in the first minute was the fastest for disposable e-cigarettes. Tmax for the disposable e-cigarettes (strawberry-kiwi: 5 min, tobacco: 6 min) was reached faster than for the cigarette (8 min). Compared to the pod e-cigarette (6 min), tmax was reached faster with the disposable e-cigarette tobacco. Total nicotine uptake was the lowest for the pod e-cigarette. Puffing behavior differed between e-cigarettes and the cigarette and slightly between both disposable e-cigarettes. Satisfaction and motivation to consume the product again were higher for disposables with a slight preference for strawberry-kiwi flavor. New disposable e-cigarettes hold great addictive potential for young people unestablished in smoking. Besides conducting further research, it is crucial to observe usage trends and strengthen regulations.
Trial registration number: DRKS00030978. Date of registration: 21.02.2023.
Similar content being viewed by others
Introduction
The prevalence of electronic cigarette (e-cigarette) use is high among young people and increasing worldwide1,2.
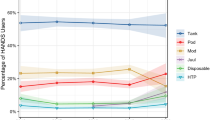
There has been a noticeable shift towards new disposable e-cigarettes, as seen in Germany3 or in the USA4. Moreover, disposables were reported as the most used device type among 13- to 40-year-old ever-users of e-cigarettes in the United States5. A British survey reports an 18-fold increase in the percentage of adult disposable users from 2021 to 2022 with the most rapid growth in the youngest age group (18 years old)6. Adolescents in the UK perceive disposable e-cigarettes as a ‘fashionable’ lifestyle ‘accessory’7.
A recent study raised safety concerns, as the investigated disposable was found to contain high levels of nicotine, flavor chemicals, and synthetic coolants whose inhalation risks are still unknown8.
E-cigarettes are offered with a great variety of over 7000 estimated different flavors9. The initiation of e-cigarette use and intention to start cigarette smoking among adolescents is more likely through flavored e-cigarettes10,11. Fruit-flavored e-cigarettes are also perceived as less harmful12.
This perception is dangerous since Electronic Nicotine Delivery System (ENDS) liquids and aerosols can, for example, contain toxicants or carcinogens besides the highly addictive nicotine13. The nicotine concentration in e-liquids is legally limited to 20 mg/ml in the European Union while e-liquids usually contain significantly more nicotine in the USA14,15.
Metanalysis has shown that e-cigarettes can be a useful tool for current cigarette smokers to quit or at least reduce their individual health risks16. Cigarette smoke contains significantly more harmful substances than e-cigarette aerosol and is accountable for 13.6% of deaths worldwide1772. However, in this paper, the focus is on the addictiveness and smoking initiation potential of e-cigarettes. E-cigarette use should not be confused with being harmless.
Tobacco is a highly addictive substance with a dependence potential ranking directly after heroin and cocaine18. Psychological and physical factors lead to tobacco dependence and its maintenance19. One major aspect is the speed of nicotine increasing in blood that differs between nicotine products20: Faster delivery leads to greater rewarding subjective effects and reinforcing behavior21,22. A rapid increase is associated with higher addictiveness20,22. Among other factors, the efficient nicotine delivery profile makes smoking the most addictive, reinforcing form of nicotine administration20,23,24. The highest measured nicotine plasma concentration (Cmax) in the plasma after smoking one cigarette typically ranges from 10 to 30 ng/ml25.
The nicotine delivery profile of e-cigarettes depends on the specific device design (such as power), liquid composition (nicotine concentration), operation conditions, and user experience26. It is possible for people who use e-cigarettes to produce a bolus cigarette-like delivery profile with a sharp plasma nicotine increase25,27. However, this applied to a study with a puffing regime, while a study with 90 min ad libitum use of e-cigarettes reported varying nicotine curve shapes with an overall slower increase over time. The authors suggest there are implications for a lower abuse liability compared with cigarettes25,28.
Studies reporting nicotine plasma concentrations during e-cigarette use show deviating results depending on the device. First-generation devices (“cig-a-likes”) were mostly found to have inefficient or negligible nicotine delivery. However, one study reported an average Cmax of 10.3 ng/ml, which is in the range of a cigarette25,29. Advanced generation e-cigarettes showed significantly higher nicotine levels compared to first-generation e-cigarettes30,31. Nevertheless, they did not reach the efficiency of cigarettes30,31.
Published research addressed aspects such as the prevalence of use6,32, perception and engagement among youth7, liquid and device characteristics8,33, patterns of sales34, or the harm reduction potential of disposable e-cigarettes35, but their pharmacokinetic (PK) or addictive potential has been hardly studied up to this point33,35. Thus, the presented four-arm crossover study focused on nicotine delivery, puffing behavior, and subjective effects of disposable e-cigarettes in comparison with a cigarette and a pod e-cigarette. Additionally, hemodynamic and negative subjective effects were measured. To investigate the effect of flavor, the disposable e-cigarette was included in two study arms, one using a fruit flavor and the other using a tobacco flavor. Due to ethical considerations, people who do not smoke were not included in the study. Instead, people who smoke occasionally were recruited as subjects, as the primary research focus was on the initiation of e-cigarette use, rather than regular smoking behavior. To our knowledge, this is the first study to examine the new disposable e-cigarettes in this kind of population.
Fearon et al.35 investigated nicotine PKs of a new disposable e-cigarette (BIDI® Stick) in six various flavors in comparison with a cigarette and a pod e-cigarette in eighteen adults who smoke. Consumption was mixed with a puffing regime followed by ad libitum use. The results showed that the disposable e-cigarette was as effective in nicotine delivery as the cigarette and more effective than the pod e-cigarette. Subjective effects for relief, satisfaction, and aversion were similar for all products. While they focused on the possible role of disposable e-cigarettes in smoking cessation as an effective alternative35, we aimed to assess the addictiveness of e-cigarettes among people nearly unestablished in smoking to gain information concerning the initiation of e-cigarette use and acute effects.
Another recent study compared liquid characteristics and e-cigarette dependence between pod e-cigarettes and disposable e-cigarettes33. The authors conducted an online study among people who (formerly) used e-cigarettes aged 18 to 65. The results support the hypothesis of an association between nicotine flux and nicotine dependence among people who use pod e-cigarettes but did not show the same for disposable e-cigarettes. Also, they did not find an association between device power or nicotine concentration and e-cigarette dependence. Nicotine flux and nicotine concentration were generally higher for disposables than for pod e-cigarettes. The nicotine flux of many disposables reported in the study also exceeded the nicotine flux of a cigarette. This raises concerns as high nicotine flux may increase the abuse liability of a product26. Device power of all disposables was in the medium range while it broadly varied for pod e-cigarettes but was mainly in the low range33.
As the described studies touch on topics discussed in our study but with different aims and methods, our study is a valuable contribution to research regarding new disposable e-cigarettes. The main study objective was to assess the addictive potential and risk of the investigated disposable e-cigarette for young occasional smokers to start consumption compared to the cigarette and pod e-cigarette. We expected the disposable e-cigarette to facilitate the initiation of use compared to the other products. Therefore, we assessed nicotine delivery, puffing behavior, hemodynamic and subjective effects. The detailed hypotheses stated before execution of the study are listed in the supplement.
Materials and methods
The study was performed in accordance with the principles of the Declaration of Helsinki and approved by the Ethical Committee at the Medical Faculty of Ludwig-Maximilians-University Munich (No. 22-1069). Registration took place at the “Bundesinstitut für Arzneimittel und Medizinprodukte” (BfArM) (DRKS00030978). Written informed consent was obtained prior to participation. Travel and subject insurance were covered by HDI Global SE (No. 39 130537 03026/ 03440).
Four products were tested by each participant in randomized order determined by a programmed tool:
-
Disposable e-cigarette strawberry-kiwi: Elf Bar 600 Strawberry Kiwi (20 mg/ml nicotine) by iMiracle Shenzhen Technology Co. Ltd.
-
Disposable e-cigarette tobacco: Elf Bar 600 Tobacco (20 mg/ml nicotine) by iMiracle Shenzhen Technology Co. Ltd.
-
Cigarette: Marlboro Red cigarette (0.8 mg nicotine) by Philip Morris.
-
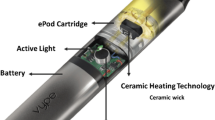
Pod e-cigarette: Myblu tobacco roasted blend (18 mg/ml nicotine) by Reemtsma.
Nicotine levels refer to product information. Products were purchased online and in stores in Germany from January to May 2023. The Elf Bar was chosen because of its popularity36,37. We decided on strawberry-kiwi flavor on the one hand to represent fruit-flavor which adolescents seem to be especially interested in trying12 and on the other hand tobacco flavor to represent a flavor similar to the cigarette and the pod e-cigarette for comparison.
18 adults (18 to 29 years old) were recruited via social media. To determine the sample size a power calculation was performed. It was estimated based on a partial eta square. All participants smoked at least once a month, up to 3 days per week, and were not tobacco dependent according to ICD-10, Fagerström Test for Cigarette Dependence (FTCD)38,38,40 or Penn State Electronic Cigarette Dependence Index (PSECDI)41. People who exceeded the inclusion criteria at any time in the past were excluded. Nicotine abstinence was required at least 12 h before an examination.
The study was performed from February to July 2023 at LMU University Hospital, Department of Psychiatry and Psychotherapy, Munich, Germany. After being screened and receiving information on the study subjects completed four sessions with one product per visit.
All study visits were performed indoors with the possibility of smoke/vapor removal by opening a window. Participants were seated during the session. Consumption was ad libitum meaning participants could use a product freely without any puffing regime. The given time frame for consumption was five min for pod e-cigarettes and disposable e-cigarettes. The use time for the cigarette ended when one cigarette was finished regardless of duration. At predefined times, blood samples were taken, hemodynamic parameters were measured, and questionnaires were completed. The testing period was 30 min. The study design is visualized in the supplement. There was no training session or presentation of study products beforehand in order to avoid distortion of acute subjective effects. A picture of the study setup can be found in the supplement.
The Modified E-Cigarette Evaluation Questionnaire (mCEQ)42 examines subjective effects of smoking on a 7-point Likert-type scale while the Comparison Of Effects After Consumption Questionnaire (ENK)43,43,45 served to assess the negative subjective effects of smoking/e-cigarette use on a scale from 1 to 10.
Each questionnaire was filled out pre consumption, post consumption, and 30 min after initiating consumption. Immediately after smoking or e-cigarette use, participants had to rate their motivation to directly consume the tested product again on a scale from 1 to 7.
Blood samples were collected using an indwelling venous catheter at nine given times: at baseline (0 min) and 1, 2, 4, 6, 8, 10, 12, and 30 min after starting the consumption. The catheter was placed on the non-dominant hand whenever possible while the participant used the other hand for holding the respective device.
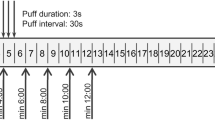
The Smoking Puff Analyzer – Mobile (SPA-M, Sodim, ORT, France) was used to examine the smoking/e-cigarette use topography46,47. This portable device was interposed between the cigarette or e-cigarette and the mouth for the whole consumption time. It recorded the flow rate, pressure drop profile, and atmospheric pressure of smoking. The number of puffs, puff volume, puff duration, average flow per puff, peak flow per puff, the interval between puffs, and the smoking duration were analyzed using the software SodAfc41 – Version 4.02.0 (Sodim, ORT, France).
Each average value is calculated per participant and puff whereas the respective mean average value is calculated from all 18.
Hemodynamic parameters have been assessed at baseline (0 min) as well as 7, 15, and 30 min after starting the consumption. The utilized device is the validated Mobil-O-Graph™ (software version HMS CS 4.2, I.E.M. GmbH) for measurement and calculation of heart rate, central blood pressure, peripheral blood pressure, and parameters of arterial stiffness (total vascular resistance (TVR), pulse wave velocity (PWV), and the augmentation index adjusted for heart rate 75 bpm (AIX@75)).
As PK parameters, the Cmax, total plasma nicotine uptake (area under the curve for the testing period of 30 min = AUC0−30 min, calculated with the linear trapezoidal rule), and the time of Cmax (tmax) were calculated.
SPSS26 was used for statistical analyses. Means, standard deviations, and ranges were calculated for participant characteristics. For puffing behavior and subjective effects, a repeated measures ANOVA was employed, and the according p-value for within-subject effects was considered. Pairwise t-tests for comparisons between products were calculated subsequently.
For Cmax and AUC, geometric means and coefficients of variation were determined, and two-sided, paired t-tests with logarithmized values were performed. For tmax, median and range were determined followed by analysis via two-sided, paired t-tests.
The statistical analysis for the cardiovascular parameters was carried out after verification of the normal distribution via the Kolmogorov-Smirnov test via two-sided, paired t-tests within the parameters against the baseline, via an ANOVA at the individual time points between the products. In addition, a two-way repeated measures ANOVA, based on baseline measurements, was used to estimate a correlation between the product used and time.
More detailed information and additional p-values (including non-significant values) can be found in the supplement.
Results
Participants’ mean age was 24 (± 2.1), 9 being female and 9 being male. The mean number of days on which participants had smoked within the last 30 days was 4.1 (± 2.6).
Nicotine delivery and plasma nicotine concentrations
Higher mean levels of Cmax were reached in the cigarette (p < 0.001), disposable e-cigarette strawberry-kiwi (p < 0.001), and disposable e-cigarette tobacco (p < 0.001) arms compared with the pod e-cigarette. Tmax was reached faster with the disposable e-cigarette strawberry-kiwi (p = 0.047) and the disposable e-cigarette tobacco (p = 0.012) than with the cigarette. Tmax was also reached faster with the disposable e-cigarette tobacco than with the pod e-cigarette (p = 0.027). Regarding the comparison of tmax, the difference in mean total smoking duration between the cigarette and the e-cigarette must also be considered (see below). The AUC0−30 min was higher for the cigarette than for the disposable e-cigarette strawberry-kiwi (p < 0.007). It was at the lowest for the pod e-cigarette: significantly lower than for disposable e-cigarettes and the cigarette (p < 0.003 compared to the disposable e-cigarette strawberry-kiwi; p < 0.001 compared to cigarette and disposable e-cigarette tobacco). There were no significant differences in Cmax (p = 0.88), tmax (p = 0.95), and AUC0−30 min (p = 0.93) between both disposable e-cigarettes. The explained parameters are listed in Table 1.
Mean plasma nicotine concentrations as well as a magnification of the acute phase (plasma concentrations in the first six min after start of consumption) are displayed in Figs. 1a) and 1b).

Plasma nicotine curves (arithmetic mean and 95% confidence interval (CI)).
1 min after the start of consumption, mean nicotine levels had increased faster for disposables than for cigarettes (p < 0. 03 for comparison of nicotine concentrations) and the pod e-cigarette (p < 0.01).
Puffing behavior
The mean average puff volume, as well as the mean average puff duration, were significantly higher for the disposable e-cigarette strawberry-kiwi (p < 0.001 for volume, p < 0.001 for duration), the disposable e-cigarette tobacco (p < 0.001 for volume, p = 0.024 for duration) and the pod e-cigarette (p < 0.001 for volume, p = 0.005 for duration) than for the cigarette. They are displayed in Fig. 2. Moreover, the mean puff duration was higher for the disposable e-cigarette strawberry-kiwi than for disposable e-cigarette tobacco (p = 0.034). The mean average puff frequency was also higher for disposable e-cigarette tobacco (p < 0.001), the pod e-cigarette (p < 0.001), and the disposable e-cigarette strawberry-kiwi (p < 0.001) than for the cigarette. Similarly, the mean average flow per puff and the mean peak flow per puff were higher for the disposable e-cigarette strawberry-kiwi (p < 0.001 for average flow, p < 0.001 for peak flow), disposable e-cigarette tobacco (p < 0.001 for average flow, p < 0.001 for peak flow) and the pod e-cigarette (p < 0.001 for average flow, p < 0.001 for peak flow) than for the cigarette. The mean average intervals between puffs were significantly higher for the cigarette compared with all other products (p = 0.01 compared with disposable e-cigarette strawberry-kiwi and pod e-cigarette, p < 0.001 compared with disposable e-cigarette tobacco). The mean total smoking duration was higher for the cigarette compared with the given time frame for using e-cigarettes (p < 0.001 for disposable e-cigarette strawberry-kiwi and pod e-cigarette, p < 0.001 for disposable e-cigarette tobacco). From these results, it was construed that the total number of puffs did not significantly differ between the products.
In summary, values for puffing behavior showed significant differences between e-cigarettes and cigarettes, but no significant differences between disposable e-cigarettes and pod e-cigarette. The only difference between both disposable e-cigarettes was in puff duration. The explained parameters are listed in Table 2.

Selected values for puffing behavior (mean and 95% CI).
Subjective effects
According to the mCEQ consumption of the disposable e-cigarette strawberry-kiwi was the most satisfying (p = 0.007 compared to disposable e-cigarette tobacco; p < 0.001 compared to cigarette; p < 0.001 compared to pod e-cigarette), followed by the disposable e-cigarette tobacco (p = 0.024 compared to cigarette; p = 0.01 compared to pod e-cigarette). Satisfaction scored lowest for the cigarette and the pod e-cigarette (p = 0.627 for comparison of cigarette and pod e-cigarette). Enjoyment of respiratory tract sensations was higher regarding the disposable e-cigarette strawberry-kiwi than for the cigarette (p = 0.005) and the pod e-cigarette (p < 0.001) with no significant difference between both disposable e-cigarettes (p = 0.7). Aversion to the cigarette was higher than to the pod e-cigarette (p = 0.026). Psychological reward and craving reduction demonstrated no significant effects between the products.
The motivation to directly consume the tested product again is illustrated in the supplement. It was significantly higher for the disposable e-cigarette strawberry-kiwi (2.9) and the disposable e-cigarette tobacco (2.7) than for the pod e-cigarette (1.5, p = 0.005 compared to disposable e-cigarette strawberry-kiwi and p = 0.006 when compared to disposable e-cigarette tobacco) and the cigarette (1.3, p = 0.001 compared to disposable e-cigarette strawberry-kiwi and disposable e-cigarette tobacco). It was generally low ranging from “does not apply at all” (cigarette) to “does rather not apply” (disposable e-cigarette strawberry-kiwi and e-cigarette tobacco). The explained parameters are listed in Table 3.
Hemodynamic parameters
The peripheral as well as the central hemodynamics showed comparable results, so that in all experimental conditions significant increases for both systolic and diastolic blood pressure could be shown compared to baseline (p < 0.05, mostly p < 0.01), except for the peripheral systolic value in the disposable e-cigarette strawberry-kiwi group after 30 min with no significant difference in the mean values of the measurement time points (p > 0.05). For the heart rate, there was a significant difference in the mean values at any time point compared to the baseline of the time in the follow-up period with an increase in the mean values (p < 0.05). A comparable result was shown for the parameters of arterial vascular stiffness (TVR, PWV, and AIx@75 – p < 0.05 and p < 0.01), wherein two time points showed higher mean values of the groups without any significant difference (TVR – disposable e-cigarette strawberry-kiwi after 30 min p = 0.085, PWV – cigarette after 30 min p = 0.053). A comparison of the mean values for the individual time points between the experimental conditions did not reveal any statistically significant differences (p > 0.05). When looking at the results for the repeated measures ANOVA, there were no significant differences observed for the experimental condition, but there was a significant difference for all examined parameters for the time course (p < 0.001) and the heart rate, taking into account the experimental condition and the elapsed time (p < 0.05).
Negative subjective effects
A summary of negative subjective effects and adverse events can be found in the supplement. The mean expression of negative subjective effects according to ENK was determined to be low to moderate.
Discussion
The main finding of this study is the nicotine delivery profile of the investigated disposable e-cigarettes which is similar to the cigarette and more effective than for the pod e-cigarette. The higher scores in satisfaction and motivation to consume the product again showed the subjective preference for disposables. Puffing behavior was different for e-cigarettes and the cigarette.
Nicotine delivery is significantly associated with users’ experience. Plasma nicotine increase is higher for people who are experienced in e-cigarette use than for people who smoke but are e-cigarette-naïve48,49. People experienced in e-cigarette use in a real-world environment using their own device can reach effective nicotine delivery profiles comparable to cigarette smoking25, but this may increase their e-cigarette dependence potential49. An alarming conclusion is that in our study population of people who occasionally smoke with little to no e-cigarette experience or adjustment time to e-cigarette use50, the new disposable e-cigarettes immediately showed a highly effective nicotine delivery and uptake comparable to the cigarette. In the present study, the increase in nicotine plasma concentrations after 1 min was faster for disposable e-cigarettes than for the cigarette and the pod e-cigarette. Considering the plasma nicotine curves during the acute phase, our findings imply the highest nicotine-mediated addictive potential for the new disposable e-cigarette among the tested products.
The Cmax for disposable e-cigarettes and cigarette did not significantly differ whereas the Cmax for the pod e-cigarette was exceeded by far. The AUC0−30 min for disposable e-cigarettes was also remarkably higher than for the pod e-cigarette. In the present study, disposable e-cigarettes seem to be more effective in regards to nicotine delivery and potentially have a higher abuse liability compared to conventional pod e-cigarettes. Regarding nicotine delivery, they are much more effective than first-generation disposables.
The AUC0−30 min for the cigarette was still higher than for the disposable e-cigarette strawberry-kiwi. Nevertheless, it should be noted that the total duration was significantly higher for smoking one cigarette compared to the predetermined time frame for e-cigarette use. It cannot be ruled out that a similar amount of nicotine would have been reached with the disposable e-cigarette strawberry-kiwi within the same time taken for the smoking of one cigarette.
Puffing topography is conflicting in terms of cigarettes and e-cigarettes. Literature has reported longer puff duration51,52 and shorter intervals between puffs52 for e-cigarettes which our findings are in alignment with.
Underlining the different puffing behavior of e-cigarettes and cigarettes, our findings concerning average puff volume, puff frequency, as well as average flow and peak flow per puff were significantly higher for all e-cigarettes than for the cigarette. While the larger puff volume for e-cigarettes is in alignment with a previous study53, the puff velocity was reported to be lower in the respective study. This difference is likely explained by the study population of people experienced in e-cigarette use. As longer puffs lead to an increased nicotine yield in e-cigarette use but greater velocity only occurs in cigarette smoking, they may have learned to not expend the energy needed for high-velocity puffs54.
Noteworthy here is that there was no significant difference in puffing topography between disposable e-cigarettes and the pod e-cigarette. Consequently, it can be assumed that device design and liquid composition led to the evident difference in nicotine delivery26. Further arguments for the greater threat to public health of the new disposable e-cigarettes are provided by Talih et al., who investigated the design of different disposable e-cigarettes in comparison to a pod e-cigarette (not including the brands used in this study). They found lower construction quality in disposable e-cigarettes without a microcontroller circuit for temperature and power control, as well as higher nicotine concentrations as labeled. Moreover, they reported a greater emission of carcinogenic carbonyls, e.g. formaldehyde and acetaldehyde, as compared to the pod e-cigarette55.
The slightly higher puff duration for the disposable e-cigarette strawberry-kiwi compared with the disposable e-cigarette tobacco is indicative of adapted puffing behavior caused by flavors which has previously been reported for people experienced in e-cigarette use56. The authors suggest differences in subjective liking, nicotine-, and sensory effects being related to lower liquid pH as an explanation56.
The presented findings on subjective effects support the assumption of disposable e-cigarettes being more appealing for people who occasionally smoke compared to a pod e-cigarette and a cigarette with slight indications of preference for the strawberry-kiwi flavored disposable. Their attractiveness despite possible health risks57,57,59 can be dangerous for youth. The slight preference for the flavored e-cigarette seen in this study is supported by previous findings60,60,61,63. However, this is problematic since ingredients used in e-cigarettes to create flavors (including tobacco flavor) can pose a health risk64.
In our study, aversion was significantly higher for the cigarette vs. the pod e-cigarette which can partly be explained by the much higher nicotine uptake. The low scores for psychological reward and alternatively the scores for craving reduction without significant differences between the products as well as the general tendency to low/neutral scores in subjective measurements might have been caused by study population selection. People who smoke occasionally may not feel nicotine-induced reward in the same way as people with nicotine-dependency would and their craving for a cigarette was resolved by each product – possibly because there was no noteworthy craving to start with.
In terms of side effects, hemodynamic effects were mainly expected to be triggered by nicotine, although the effects of different flavors were still unclear. Overall, the results, even if only acute effects after a single use were investigated in this work, point in a comparable direction, as preliminary studies have already shown65,65,67. One study for example, comparing a pod-based e-cigarette with a cigarette showed a similar negative effect on cerebral and peripheral vascular function for both conditions68.
There is not only an increase in heart rate and blood pressure values but also alterations in the area of arterial stiffness. Consequential damage after long-term consumption based among others on the pathologically altered surrogate parameters of arterial stiffness can lead to major cardiovascular events69. Mechanistically, in addition to the activation of the autonomic nervous system via nicotine, the direct effect of vapor, as shown and postulated in the work of Lee et al.70, with a corresponding inflammatory reaction and increased reactive oxygen species, remains to be discussed. Further measurements, also directly in the area of endothelial dysfunction, which would be expected based on inflammation, would be expedient.
To conclude, our results provide an indication that the tested disposable e-cigarettes carry a high addictive potential for young people nearly unestablished in smoking. This is reflected in their effective nicotine delivery profile comparable to cigarettes. It was significantly more effective compared to a pod e-cigarette, although puffing behavior did not differ significantly between e-cigarettes, likely due to device design26,55. Higher scores for satisfaction and motivation to immediately re-consume the product in the disposable e-cigarette arms underline these objective results with subjective findings showing a slight preference for the strawberry-kiwi flavored disposable.
Limitations
Further investigations with larger sample sizes are needed to confirm our findings. Other limitations are the high number of exclusions due to technical reasons and practical deviations during testing (like delays in measurements, positioning of the blood pressure cuff, or distraction of participants from consumption during blood sampling) also influencing participant comfort. Incidentally, there was likely a misunderstanding concerning the completion of the ENK: some participants reported a nicotine flash at baseline without having consumed nicotine beforehand. The study setting was not reflective of a real-life scenario as many people who occasionally smoke tend to smoke in social situations or simultaneously with alcohol consumption71. In this study, they consumed nicotine alone during the daytime and without the cofactors associated with their usual smoking behavior. Furthermore, conclusions about people who do not smoke should be drawn with great caution, as they are not directly comparable to people who occasionally smoke. Since we investigated on acute effects, we did not monitor participants after the last study visit. Consequently, we cannot provide information on how their usage behavior changed after the study which would indeed provide a valuable insight. Similarly, we cannot report on how the usage profile of the first tested disposable may differ from the second one or how puffing behavior evolved from the first to the last puff during one visit. Noteworthy also as a limitation is the difference in mean total duration of use which was imposed by the study design. Further, the duration of five minutes that we imposed for e-cigarette use does not correspond to the usual usage pattern of e-cigarettes. This time frame remained constant because we focused on the acute effects of consumption. A study on pod e-cigarettes, cigarettes and heated tobacco products with ad libitum consumption for 90 min among experienced users was previously performed by our study group44.
Conclusion
Despite e-cigarettes’ potential usefulness in terms of smoking cessation, the conceivable role of new disposable e-cigarettes as regards acquiring dependence is alarming. With this in mind, it is necessary to observe disposable e-cigarette use trends and strengthen regulations including marketing-, flavor- or even product bans. Moreover, further research is needed to expand the knowledge about disposable e-cigarettes, usage patterns, and health-related risks.
Data availability
Data is available on request from the authors (contact information: Christin.Falarowski@med.uni-muenchen.de).
References
Society for Adolescent Health and Medicine. Protecting youth from the risks of electronic cigarettes. J. Adolesc. Health. 66, 127–131. https://doi.org/10.1016/j.jadohealth.2019.10.007 (2020).
Yoong, S. L. et al. Prevalence of electronic nicotine delivery systems (ENDS) use among youth globally: a systematic review and meta-analysis of country level data. Aust N Z J Public Health 42, 303-308. https://doi.org:10.1111/1753-6405.12777 (2018).
Klosterhalfen, S., Viechtbauer, W. & Kotz, D. Disposable e-cigarettes: prevalence of use in Germany from 2016 to 2023 and associated user characteristics. Addiction 120, 557–567. https://doi.org/10.1111/add.16675 (2025).
Park-Lee, E. et al. Notes from the field: E-Cigarette and nicotine pouch use among middle and high school Students - United States, 2024. MMWR Morb Mortal. Wkly. Rep. 73, 774–778. https://doi.org/10.15585/mmwr.mm7335a3 (2024).
McCauley, D. M., Gaiha, S. M., Lempert, L. K., Halpern-Felsher, B. & Adolescents Young adults, and adults continue to use E-Cigarette devices and flavors two years after FDA discretionary enforcement. Int. J. Environ. Res. Public. Health. 19 https://doi.org/10.3390/ijerph19148747 (2022).
Tattan-Birch, H., Jackson, S. E., Kock, L., Dockrell, M. & Brown, J. Rapid growth in disposable e-cigarette vaping among young adults in great Britain from 2021 to 2022: a repeat cross-sectional survey. Addiction 118, 382–386. https://doi.org/10.1111/add.16044 (2023).
Smith, M. J., MacKintosh, A. M., Ford, A. & Hilton, S. Youth’s engagement and perceptions of disposable e-cigarettes: a UK focus group study. BMJ Open. 13, e068466. https://doi.org/10.1136/bmjopen-2022-068466 (2023).
Omaiye, E. E., Luo, W., McWhirter, K. J., Pankow, J. F. & Talbot, P. Disposable puff bar electronic cigarettes: chemical composition and toxicity of E-liquids and a synthetic coolant. Chem. Res. Toxicol. 35, 1344–1358. https://doi.org/10.1021/acs.chemrestox.1c00423 (2022).
Zhu, S. H. et al. Four hundred and sixty brands of e-cigarettes and counting: implications for product regulation. Tobacco Control 23, iii3-iii9 (2014). https://doi.org/10.1136/tobaccocontrol-2014-051670
Zare, S., Nemati, M. & Zheng, Y. A systematic review of consumer preference for e-cigarette attributes: flavor, nicotine strength, and type. PLoS One. 13, e0194145. https://doi.org/10.1371/journal.pone.0194145 (2018).
Dai, H. & Hao, J. Flavored electronic cigarette use and smoking among youth. Pediatrics 138 https://doi.org/10.1542/peds.2016-2513 (2016).
Pepper, J. K., Ribisl, K. M. & Brewer, N. T. Adolescents’ interest in trying flavoured e-cigarettes. Tob. Control. 25 (ii62-ii66). https://doi.org/10.1136/tobaccocontrol-2016-053174 (2016).
Walley, S. C., Jenssen, B. P. & Section on Tobacco Control. Electron. Nicotine Delivery Syst. Pediatr. 136, 1018–1026 https://doi.org/10.1542/peds.2015-3222 (2015).
Snell, L. M. et al. Emerging electronic cigarette policies in European member States, Canada, and the united States. Health Policy. 125, 425–435. https://doi.org/10.1016/j.healthpol.2021.02.003 (2021).
European Commission. Questions & Answers: New rules for tobacco products (2014). https://europa.eu/rapid/press-release_MEMO-14-134_en.htm
Hartmann-Boyce, J. et al. Electronic cigarettes for smoking cessation. Cochrane Database Syst. Reviews. https://doi.org/10.1002/14651858.CD010216.pub7 (2022).
Benowitz, N. L., Helen, S., Liakoni, E. & G. & Clinical Pharmacology of electronic nicotine delivery systems (ENDS): implications for benefits and risks in the promotion of the combusted tobacco endgame. J. Clin. Pharmacol. 61 (Suppl 2), S18–s36. https://doi.org/10.1002/jcph.1915 (2021).
Nutt, D., King, L. A., Saulsbury, W. & Blakemore, C. Development of a rational scale to assess the harm of drugs of potential misuse. Lancet 369, 1047–1053. https://doi.org/10.1016/s0140-6736(07)60464-4 (2007).
Sohn, M., Hartley, C., Froelicher, E. S. & Benowitz, N. L. Tobacco use and dependence. Semin Oncol. Nurs. 19, 250–260. https://doi.org/10.1053/j.soncn.2003.08.002 (2003).
Henningfield, J. E. & Keenan, R. M. Nicotine delivery kinetics and abuse liability. J. Consult Clin. Psychol. 61, 743–750. https://doi.org/10.1037/0022-006x.61.5.743 (1993).
de Wit, H., Bodker, B. & Ambre, J. Rate of increase of plasma drug level influences subjective response in humans. Psychopharmacol. (Berl). 107, 352–358. https://doi.org/10.1007/bf02245161 (1992).
Benowitz, N. L. Nicotine addiction. Prim. Care. 26, 611–631. https://doi.org/10.1016/s0095-4543(05)70120-2 (1999).
Hukkanen, J., Jacob, P., Benowitz, N. L. & 3rd & Metabolism and disposition kinetics of nicotine. Pharmacol. Rev. 57, 79–115. https://doi.org/10.1124/pr.57.1.3 (2005).
Benowitz, N. L., Porchet, H. & Jacob, P. in Nicotine Psychopharmacology: Molecular, Cellular, and Behavioural Aspects (eds S. Wonnacott, M. A. H. Russell, & I. P. Stolerman) 0Oxford University Press (1990).
Voos, N., Goniewicz, M. L. & Eissenberg, T. What is the nicotine delivery profile of electronic cigarettes? Expert Opin. Drug Deliv. 16, 1193–1203. https://doi.org/10.1080/17425247.2019.1665647 (2019).
Shihadeh, A. & Eissenberg, T. Electronic cigarette effectiveness and abuse liability: predicting and regulating nicotine flux. Nicotine Tob. Res. 17, 158–162. https://doi.org/10.1093/ntr/ntu175 (2015).
St Helen, G., Havel, C., Dempsey, D. A., Jacob, P., Benowitz, N. L. & 3rd & Nicotine delivery, retention and pharmacokinetics from various electronic cigarettes. Addiction 111, 535–544. https://doi.org/10.1111/add.13183 (2016).
St Helen, G. et al. Nicotine delivery and vaping behavior during ad libitum E-cigarette access. Tob. Regul. Sci. 2, 363–376. https://doi.org/10.18001/trs.2.4.8 (2016).
Vansickel, A. R. & Eissenberg, T. Electronic cigarettes: effective nicotine delivery after acute administration. Nicotine Tob. Res. 15, 267–270. https://doi.org/10.1093/ntr/ntr316 (2013).
Hajek, P., Przulj, D., Phillips, A., Anderson, R. & McRobbie, H. Nicotine delivery to users from cigarettes and from different types of e-cigarettes. Psychopharmacol. (Berl). 234, 773–779. https://doi.org/10.1007/s00213-016-4512-6 (2017).
Voos, N. et al. Randomized within-subject trial to evaluate smokers’ initial perceptions, subjective effects and nicotine delivery across six vaporized nicotine products. Addiction 114, 1236–1248. https://doi.org/10.1111/add.14602 (2019).
Wang, T. W. et al. Disposable E-Cigarette use among U.S. Youth - An emerging public health challenge. N Engl. J. Med. 384, 1573–1576. https://doi.org/10.1056/NEJMc2033943 (2021).
Do, E. K. et al. E-cigarette device and liquid characteristics and E-cigarette dependence: A pilot study of pod-based and disposable E-cigarette users. Addict. Behav. 124, 107117. https://doi.org/10.1016/j.addbeh.2021.107117 (2022).
Diaz, M. C., Silver, N. A., Bertrand, A. & Schillo, B. A. Bigger, stronger and cheaper: growth in e-cigarette market driven by disposable devices with more e-liquid, higher nicotine concentration and declining prices. Tob. Control. https://doi.org/10.1136/tc-2023-058033 (2023).
Fearon, I. M., Gilligan, K., Seltzer, R. G. N. & McKinney, W. A randomised, crossover, clinical study to assess nicotine pharmacokinetics and subjective effects of the BIDI(®) stick ENDS compared with combustible cigarettes and a comparator ENDS in adult smokers. Harm Reduct. J. 19, 57. https://doi.org/10.1186/s12954-022-00638-0 (2022).
Birdsey, J. et al. Tobacco product use among U.S. Middle and high school Students - National youth tobacco survey, 2023. MMWR Morb Mortal. Wkly. Rep. 72, 1173–1182. https://doi.org/10.15585/mmwr.mm7244a1 (2023).
East, K. et al. Use of ‘elf bar’ among youth and young adults who currently vape in England: cross-sectional associations with demographics, dependence indicators and reasons for use. Addiction 120, 414–422. https://doi.org/10.1111/add.16463 (2025).
Fagerstrom, K. O. & Schneider, N. G. Measuring nicotine dependence: a review of the Fagerstrom tolerance questionnaire. J. Behav. Med. 12, 159–182. https://doi.org/10.1007/bf00846549 (1989).
Heatherton, T. F., Kozlowski, L. T., Frecker, R. C. & Fagerström, K. O. The Fagerström test for nicotine dependence: a revision of the Fagerström tolerance questionnaire. Br. J. Addict. 86, 1119–1127. https://doi.org/10.1111/j.1360-0443.1991.tb01879.x (1991).
Fagerström, K. Determinants of tobacco use and renaming the FTND to the Fagerstrom test for cigarette dependence. Nicotine Tob. Res. 14, 75–78. https://doi.org/10.1093/ntr/ntr137 (2012).
Foulds, J. et al. Development of a questionnaire for assessing dependence on electronic cigarettes among a large sample of ex-smoking E-cigarette users. Nicotine Tob. Res. 17, 186–192. https://doi.org/10.1093/ntr/ntu204 (2015).
Cappelleri, J. C. et al. Confirmatory factor analyses and reliability of the modified cigarette evaluation questionnaire. Addict. Behav. 32, 912–923. https://doi.org/10.1016/j.addbeh.2006.06.028 (2007).
Vukas, J. et al. Two different heated tobacco products vs. Cigarettes: comparison of nicotine delivery and subjective effects in experienced users. Toxics 11 https://doi.org/10.3390/toxics11060525 (2023).
Rabenstein, A. et al. Usage pattern and nicotine delivery during ad libitum consumption of pod E-Cigarettes and heated tobacco products. Toxics 11 https://doi.org/10.3390/toxics11050434 (2023).
Mallock, N. et al. Nicotine delivery and relief of craving after consumption of European JUUL e-cigarettes prior and after pod modification. Sci. Rep. 11, 12078. https://doi.org/10.1038/s41598-021-91593-6 (2021).
Mikheev, V. B. et al. The application of commercially available mobile cigarette topography devices for E-cigarette vaping behavior measurements. Nicotine Tob. Res. 22, 681–688. https://doi.org/10.1093/ntr/nty190 (2018).
Vansickel, A. R. et al. Characterization of puff topography of a prototype electronic cigarette in adult exclusive cigarette smokers and adult exclusive electronic cigarette users. Regul. Toxicol. Pharmacol. 98, 250–256. https://doi.org/10.1016/j.yrtph.2018.07.019 (2018).
Hiler, M. et al. Electronic cigarette user plasma nicotine concentration, puff topography, heart rate, and subjective effects: influence of liquid nicotine concentration and user experience. Exp. Clin. Psychopharmacol. 25, 380–392. https://doi.org/10.1037/pha0000140 (2017).
Farsalinos, K. E. et al. Nicotine absorption from electronic cigarette use: comparison between experienced consumers (vapers) and Naïve users (smokers). Sci. Rep. 5, 11269. https://doi.org/10.1038/srep11269 (2015).
Lee, Y. H., Gawron, M. & Goniewicz, M. L. Changes in puffing behavior among smokers who switched from tobacco to electronic cigarettes. Addict. Behav. 48, 1–4. https://doi.org/10.1016/j.addbeh.2015.04.003 (2015).
Farsalinos, K. E., Romagna, G., Tsiapras, D., Kyrzopoulos, S. & Voudris, V. Evaluation of electronic cigarette use (vaping) topography and Estimation of liquid consumption: implications for research protocol standards definition and for public health authorities’ regulation. Int. J. Environ. Res. Public. Health. 10, 2500–2514. https://doi.org/10.3390/ijerph10062500 (2013).
Strasser, A. A. et al. Nicotine replacement, topography, and smoking phenotypes of E-cigarettes. Tob. Regul. Sci. 2, 352–362. https://doi.org/10.18001/trs.2.4.7 (2016).
Spindle, T. R., Breland, A. B., Karaoghlanian, N. V., Shihadeh, A. L. & Eissenberg, T. Preliminary results of an examination of electronic cigarette user puff topography: the effect of a mouthpiece-based topography measurement device on plasma nicotine and subjective effects. Nicotine Tob. Res. 17, 142–149. https://doi.org/10.1093/ntr/ntu186 (2015).
Talih, S. et al. Effects of user puff topography, device voltage, and liquid nicotine concentration on electronic cigarette nicotine yield: measurements and model predictions. Nicotine Tob. Res. 17, 150–157. https://doi.org/10.1093/ntr/ntu174 (2015).
Talih, S. et al. Electrical features, liquid composition and toxicant emissions from ‘pod-mod’-like disposable electronic cigarettes. Tob. Control. 31, 667–670. https://doi.org/10.1136/tobaccocontrol-2020-056362 (2022).
St Helen, G., Shahid, M., Chu, S. & Benowitz, N. L. Impact of e-liquid flavors on e-cigarette vaping behavior. Drug Alcohol Depend. 189, 42–48. https://doi.org/10.1016/j.drugalcdep.2018.04.032 (2018).
Lin, H. C., Buu, A. & Su, W. C. Disposable E-Cigarettes and associated health risks: an experimental study. Int. J. Environ. Res. Public. Health. 19 https://doi.org/10.3390/ijerph191710633 (2022).
McGrath-Morrow, S. A. et al. The effects of nicotine on development. Pediatrics 145 https://doi.org/10.1542/peds.2019-1346 (2020).
Rosenthal, H., Chow, N., Mehta, S., Pham, D. & Milanaik, R. Puff bars: a dangerous trend in adolescent disposable e-cigarette use. Curr. Opin. Pediatr. 34, 288–294. https://doi.org/10.1097/mop.0000000000001123 (2022).
Audrain-McGovern, J., Strasser, A. A. & Wileyto, E. P. The impact of flavoring on the rewarding and reinforcing value of e-cigarettes with nicotine among young adult smokers. Drug Alcohol Depend. 166, 263–267. https://doi.org/10.1016/j.drugalcdep.2016.06.030 (2016).
Soule, E. K., Lopez, A. A., Guy, M. C. & Cobb, C. O. Reasons for using flavored liquids among electronic cigarette users: A concept mapping study. Drug Alcohol Depend. 166, 168–176. https://doi.org/10.1016/j.drugalcdep.2016.07.007 (2016).
Soneji, S. S., Knutzen, K. E. & Villanti, A. C. Use of flavored E-Cigarettes among adolescents, young adults, and older adults: findings from the population assessment for tobacco and health study. Public. Health Rep. 134, 282–292. https://doi.org/10.1177/0033354919830967 (2019).
Goldenson, N. I. et al. Effects of sweet flavorings and nicotine on the appeal and sensory properties of e-cigarettes among young adult vapers: application of a novel methodology. Drug Alcohol Depend. 168, 176–180. https://doi.org/10.1016/j.drugalcdep.2016.09.014 (2016).
Ween, M. P. et al. E-cigarettes and health risks: more to the flavor than just the name. Am. J. Physiol. Lung Cell. Mol. Physiol. 320, L600–l614. https://doi.org/10.1152/ajplung.00370.2020 (2021).
Gernun, S. et al. Cardiovascular functions and arterial stiffness after JUUL use. Tob. Induc. Dis. 20, 34. https://doi.org/10.18332/tid/144317 (2022).
Franzen, K. F. et al. E-cigarettes and cigarettes worsen peripheral and central hemodynamics as well as arterial stiffness: A randomized, double-blinded pilot study. Vasc Med. 23, 419–425. https://doi.org/10.1177/1358863x18779694 (2018).
Antoniewicz, L., Brynedal, A., Hedman, L., Lundbäck, M. & Bosson, J. A. Acute effects of electronic cigarette inhalation on the vasculature and the conducting airways. Cardiovasc. Toxicol. 19, 441–450. https://doi.org/10.1007/s12012-019-09516-x (2019).
Ben Taleb, Z. et al. Pod-based e-cigarettes versus combustible cigarettes: the impact on peripheral and cerebral vascular function and subjective experiences. Tob. Induc. Dis. 21, 71. https://doi.org/10.18332/tid/162366 (2023).
Ashraf, M. T. et al. Association between e-cigarette use and myocardial infarction: a systematic review and meta-analysis. Egypt. Heart J. 75, 97. https://doi.org/10.1186/s43044-023-00426-6 (2023).
Lee, W. H. et al. Modeling cardiovascular risks of E-Cigarettes with Human-Induced pluripotent stem Cell-Derived endothelial cells. J. Am. Coll. Cardiol. 73, 2722–2737. https://doi.org/10.1016/j.jacc.2019.03.476 (2019).
Brown, A. E., Carpenter, M. J. & Sutfin, E. L. Occasional smoking in college: who, what, when and why? Addict. Behav. 36, 1199–1204. https://doi.org/10.1016/j.addbeh.2011.07.024 (2011).
GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet 397, 2337-2360. https://doi.org:10.1016/s0140-6736(21)01169-7 (2021).
Acknowledgements
We thank S. De Jonge, S. Malke, N. Dreiack, K. Neumeier, and R. Lehmair for their excellent technical assistance.
Funding
Open Access funding enabled and organized by Projekt DEAL.
The study was funded by intermural funding from the German Federal Institute for Risk Assessment (BfR), grant No. BfR-CPS-23-60-0102-02.P627.
Author information
Authors and Affiliations
Contributions
C.F.:Conceptualization, Data Curation, Investigation, Methodology, Project administration, Visualization, Original Draft PreparationE.P.: Conceptualization, Review & EditingA.R.: Conceptualization, Methodology, Project administration, Review & EditingN.M-O.: Conceptualization, Methodology, Visualization, Review & Editing N.B.: Formal Analysis, Software, Review & EditingK.F.: Formal Analysis, Methodology, Original Draft PreparationM.G.:Conceptualization, Review & EditingG.K.: Conceptualization, Review & EditingD.N.: Conceptualization, Review & EditingA.Ra.: Conceptualization, Methodology, Review & EditingB.R.: Conceptualization, Methodology, Review & EditingG.K.: Data curation, Investigation, Review & EditingT.S.: Conceptualization, Methodology, Review & EditingE.S.: Data curation, Formal Analysis, Review & EditingP.L.: Supervision, Review & EditingA.L.: Funding Acquisition, Supervision, Review & EditingT.R.: Conceptualization, Methodology, Supervision, Review & Editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Falarowski, C., Pieper, E., Rabenstein, A. et al. Disposable e-cigarettes and their nicotine delivery, usage pattern, and subjective effects in occasionally smoking adults. Sci Rep 15, 16270 (2025). https://doi.org/10.1038/s41598-025-97491-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97491-5
