
Abstract
Prior research has revealed an association between smoking, reduced ulcerative colitis (UC) risk, and improved disease severity among individuals with existing UC. Herein, we analysed the interaction between smoking habits and UC and its potential complexity, focusing on associations between smoking, incidence of UC, and therapeutic outcomes, via a meta-analysis of data from case–control studies. The PubMed, China Knowledge, WanFang, Web of Science, China Science and Technology Journal, Embase, and Scopus databases were searched, yielding nine case–control studies investigating the association between smoking and UC progression for inclusion. Compared to non-smoking or smoking cessation, smoking had a protective effect against UC, indicating that it may reduce the risk of developing UC; specifically, smoking was associated with a significant protective effect against UC compared to smoking cessation (pooled odds ratio (OR): 0.26, 95% confidence interval (CI): 0.21–0.32; P = 0.067, I2 = 45.2%). Non-smoking was also protective compared with smoking cessation (pooled OR: 1.84, 95% CI 1.13–3.30; P = 0.935, I2 = 0%). Further, smoking was significantly more protective than non-smoking (pooled OR: 0.48, 95% CI 0.40–0.56; P = 0.002, I2 = 66.4%). These results indicate that smoking offers some protection against UC onset and may reduce disease severity in patients with existing UC.
Similar content being viewed by others


Introduction
Ulcerative colitis (UC) is a form of inflammatory bowel disease (IBD) characterised by chronic, non-specific, and recurrent disease1 that affects the mucosal layers of the colon (large intestine) and, to a lesser extent, the rectum2. UC lesions typically originate in the rectum; in some patients these lesions are confined to the rectum; however, in others, they can extend proximally across the entire colon3. Patients with UC develop recurrent episodes of colonic (large bowel) inflammation and ulceration4 characterised by abdominal pain, mucopurulent bloody stools, and urgency5. Prior studies have reported that the global incidence and prevalence of UC are increasing6, particularly in Asian countries7. UC affects the health and quality of life of patients, and can also be accompanied by several complications, including toxic megacolon and colon cancer8, and may be life-threatening in severe cases. Currently, UC treatment is based on the principles of controlling inflammation, relieving symptoms, slowing progression, and improving quality of life. Available therapies encompass pharmacological treatments (such as 5-aminosalicylic acid, corticosteroids, immunosuppressants, and biologics), nutritional support, surgical treatments, and lifestyle modifications9. Despite the variety of available treatment modalities, UC remains a poorly disease, although research has shown that its development may be related to genetic, environmental, and immune factors10. The pathogenesis of UC is not yet fully understood; as such, it is not possible to directly target UC pathology.
Environmental factors have been associated with UC onset and progression11,12. Epidemiological surveys, clinical observations, and laboratory studies have all reported that external environmental factors play important roles in the development of UC13. Smoking is a significant preventable cause of global mortality14 that has a profound impact on several aspects of the health of multiple organ systems, including the respiratory, circulatory, and immune systems. Furthermore, smoking is closely associated with a variety of diseases, including cardiovascular diseases, lung cancer, and intestinal disorders15.
As an environmental risk factor, smoking exerts conflicting effects on patients with IBD, as current smokers have an increased risk of developing Crohn’s disease (CD), as well as an increased risk of adverse effects and exacerbation of symptoms in individuals with disease, compared with individuals who have never smoked16. In contrast, smoking may exert protective effects for patients with UC17. Indeed, smokers show a reduced risk of developing UC compared to non-smokers, and the symptoms of patients with UC who smoke are relatively mild. However, in patients with UC, restarting smoking after the cessation of smoking may worsen the severity and duration of UC, as observed and confirmed by clinicians treating patients with UC. One prior study reported that up to 90% of smokers with UC who had previously quit smoking achieved long-term clinical remission in the absence of conventional treatment with the intervention of low-dose smoking18. These results may be related to the action of cigarette components, such as nicotine, as suppressors of inflammatory responses and promoters of immune cell activity by affecting the mucus layer of the colon, modulating the production of cytokines, and influencing the immunomodulatory effects of the microvascular system. Patients with UC who begin to smoke again after smoking cessation are more likely than smokers to experience disease recurrence and complications, such as intestinal bleeding and perforation8. The exact mechanism underlying this phenomenon is not yet fully understood, although it may be due to the anti-inflammatory effects of nicotine, the effects of smoking on intestinal motility, or the impact on immune regulation. Nicotine may inhibit the activity of certain immune cells, including T-helper cells and macrophages, which are crucial for mediating the inflammatory response in the setting of UC19. In addition, smoking may alter intestinal motility, thereby influencing the speed of the passage of intestinal contents. Smoking may also alter the function of the intestinal immune system and decrease the ability of the gut tissues to respond, thereby reducing the aggressiveness of intestinal tissues20. Investigating the mechanisms by which smoking may offer protection to patients with UC is thus becoming increasingly important.
In summary, several studies have confirmed that smoking status exerts varying effects on UC. However, the relationship between smoking and UC remains unclear. Therefore, as cohort studies meeting our inclusion criteria were scarce, we conducted a meta-analysis using case–control study data. This study aimed to investigate the complex interplay between smoking habits and UC, focusing on the potential protective role of smoking in the prevention of UC and providing novel perspectives for clinical practice in reducing the incidence of UC.
Methods
This meta-analysis was registered in the PROSPERO (CRD42024593447) database, and followed the predetermined criteria and methodologies for data collection, screening, and analysis. Further, this study followed the PRISMA statement and complied with all statistical requirements.
Search strategy
Two authors conducted a comprehensive search of the PubMed, China Knowledge, WanFang, Web of Science, China Science and Technology Journal Database, Embase, and Scopus to identify relevant studies published from database creation up to June 2024, with no language restrictions. The search terms included "UC," "smoking," "cigarettes," "mitigation," and "prevention." The reference lists, relevant reviews, and meta-analyses of all eligible articles were searched to prevent the omission of any relevant studies.The complete search strategy details can be found in Supplement 1.
Study selection
Two authors independently selected and cross-checked the literature identified in the database search. An initial screening was conducted to remove duplicate articles. Subsequently, the methods sections of the identified studies were filtered. The titles and abstracts were manually screened. Finally, after excluding articles that were clearly out of scope, the full texts of the remaining articles were read.
Inclusion and exclusion criteria
This meta-analysis included case–control studies investigating the association between UC and smoking status (including patients who were current smokers or non-smokers, as well as those who had ceased smoking). The included studies reported the results of patients who had been diagnosed with UC based on clinical, endoscopic, radiological, or histological data, as well as the results of a control group.
Studies that were not case–control studies (such as systematic evaluations, meta-analyses, conference abstracts, letters, cellular or animal studies, reviews, commentaries, and dissertations), and those that did not focus on the association between UC and smoking status, were excluded from this meta-analysis, as were studies with incomplete data, those that were not available as full text documents, and duplicate studies.
Definitions
Throughout the individual studies, patients who reported smoking at the time of the study were classified as current smokers; those who had ceased smoking for at least 1 year prior to the study were classified as former smokers; and those who had never smoked were classified as non-smokers.
Data extraction
The retrieved literature was downloaded and imported into NoteExpress software (Version number: 4.0.0.9855; Website: http://www.inoteexpress.com), after which duplicate studies are eliminated through the software’s automatic screening function for duplicate literature. Two authors (YM & DA) independently screened the literature and extracted the study data. Study information, including the year of publication, first author, and title; subject information, including the sample size, age, and sex; and primary and secondary outcome indicators, including smoking status and UC diagnosis, were extracted from all included studies. Disagreements were resolved through consultation with a third independent researcher (ML).
Statistical analyses
This meta-analysis was conducted in accordance with the PRISMA 2020 Checklist, and all analyses were performed using StataMP 17.0 (64bit) (StataCorp LLC, United States, https://www.stata.com/) software. The combined odds ratio (OR) and 95% confidence intervals (CIs) were calculated, and the I2 test was applied to examine heterogeneity, with I2 ≥ 50% indicating high heterogeneity and I2 < 50% indicating low heterogeneity; with random and fixed-effects models used for such cases, respectively. Statistical significance was set at P < 0.05.
Subgroups and sensitivity analyses
Subgroup and sensitivity analyses were performed when I2 ≥ 50%, including smokers versus non-smokers, men versus women, and between age groups. Sensitivity analyses were performed using Stata17 to assess the effects of specific tests on heterogeneity and combined effects.
Publication bias
Two reviewers evaluated the risk of bias using the Newcastle–Ottawa Scale, a standard quality assessment instrument used to assess case–control studies. The scale included eight items across three domains: selection, comparability, and exposure. For each satisfied criterion, a score of 1 or 2 was assigned, with quality ratings classified as low (total of 0–3 points), moderate (total of 4–6 points), and high (total of 7–9 points) quality.
Publication bias was further visually assessed using funnel plots created using Stata 17. Funnel plots were created using OR as the horizontal coordinate and the logarithm of OR (logOR) as the vertical coordinate. An asymmetric funnel plot indicated bias, while P > 0.05 indicated no potential publication bias.
Results
Literature search and study characteristics
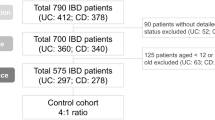
The initial screening of the databases revealed 1290; following the removal of 713 duplicates, 577 studies were retained. Of these, 532 studies were excluded based on the title and abstract screening. The remaining 45 studies underwent screening of the full-text. Ultimately, nine studies21,22,23,24,25,26,27,28,29 were included in this meta-analysis (Fig. 1). These studies included a total of 4226 patients, including 930 smokers, 2429 never-smokers, and 867 former smokers (Table 1). The publication bias investigation identified that some of the included studies were of low quality and therefore at risk of publication bias (Table 2).

Flow diagram of study selection and identification.
Meta-analysis
Impact of current smoking and non-smoking on UC
The impact of smoking versus non-smoking on the occurrence of UC was assessed in nine case–control studies21,22,23,24,25,26,27,28,29 including 3,179 patients (930 smokers and 2,249 non-smokers). Heterogeneity testing revealed significant variability (P = 0.002, I2 = 66.4%), the sources of which were explored using a subgroup analysis, for which the specific results are presented in Section "Subgroup analyses". Subgroup analyses. Compared to not smoking, smoking exhibited a protective effect against UC (combined OR: 0.48, 95% CI: 0.40–0.56). The risk of UC was significantly different between smokers and non-smokers, and smoking was associated with a reduction in the likelihood of developing UC (Fig. 2).

Meta-analysis of smoking and non-smoking on UC forest plots. te number of smokers who developed UC, tt number of smokers who did not develop UC, ce2 number of non-smokers who developed UC, ct2 number of non-smokers who did not develop UC.
Impact of current smoking and former smoking on UC
Nine case–control studies21,22,23,24,25,26,27,28,29 reported data regarding the effects of smoking cessation on the likelihood of developing UC. This meta-analysis included 1,797 patients, including 930 current smokers and 867 former smokers. Heterogeneity testing indicated limited variability (P = 0.067, I2 = 45.2%). The meta-analysis revealed that smoking significantly protected patients from developing UC compared with smoking cessation (combined OR: 0.26, 95% CI: 0.21–0.32). These results indicate that smoking is associated with a significant reduction in the risk of developing UC compared with smoking cessation (Fig. 3).

Meta-analysis of smoking and smoking cessation on UC forest plots. te the count of smokers who contracted UC, tt the count of smokers who did not contract UC, ce1 the count of former smokers who contracted UC, ce2 the count of former smokers who did not contract UC.
Impact of former and never smoking on UC
Nine case–control studies21,22,23,24,25,26,27,28,29 reported data on the effects of smoking cessation on the development of UC. This analysis included 3296 patients (867 non-smokers and 2429 former smokers). The heterogeneity assessment revealed minimal heterogeneity among the studies (P = 0.935, I2 = 0). Former smokers showed a protective effect against UC, which was significantly greater than the effect of never smoking (combined OR: 1.84, 95% CI 1.13–3.30). Former smokers also showed a significant protective effect compared to that of non-smokers (P = 0.935, I2 = 0). Therefore, smoking cessation provided a protective effect against developing UC. In addition, smoking cessation provided a more protective effect than never smoking (Fig. 4).

Meta-analysis of forest plot of UC for smoking cessation versus no smoking. ce2 number of non-smokers who developed UC, number of ct2 non-smokers who did not develop UC. ce1 number of quitters who developed UC, ct1 number of quitters who did not develop UC.
Analysis of bias
The symmetry of the funnel plots and the even distribution of the scatter points indicated the results were reliable, and that the distribution of effect sizes was relatively balanced with the different study sizes (Supplement 2, Figs. S1–S3). These results indicate no obvious publication bias.
Sensitivity analyses
A high degree of stability and reliability in the study results was observed (Supplement 2, Fig. S4). When individual studies were sequentially excluded from the analysis, the overall results did not show any significant fluctuatation, indicating that no individual study had a decisive effect on the combined results. This symmetrical and even distribution further confirms that the results of the meta-analysis were relatively stable and less susceptible to interference from outliers or bias in specific studies.
Subgroup analyses
Subgroup analyses were conducted to assess the influence of smoking status, sex, and age on heterogeneity.
Smoking status
Nine studies21,22,23,24,25,26,27,28,29 reported data regarding the patients’ smoking status. Smoking exerted a protective effect against UC compared with not smoking (combined OR: 0.42, 95% CI 0.28–0.63). The heterogeneity test revealed significant variability among the studies (P = 0.006, I2 = 69.1). Therefore, the smoking status of the included patients was not determined to be a source of heterogeneity (Fig. 5).

Subgroup analysis of the proportion of smokers and non-smokers in An. Group 1 has less than 1/3 of the non-smoking group. Group 2 has 1/3 of the smoking group over the non-smoking group.
Sex
Six studies21,22,23,24,25,27 reported data regarding the sex of the patients in the smoking and non-smoking groups. Overall, smoking exerted a protective effect against UC compared to not smoking (pooled OR: 0.42, 95% CI 0.28–0.63). This effect was more pronounced as the proportion of men decreased. The heterogeneity test revealed significant variability among the studies (P = 0.006, I2 = 69.1), although the heterogeneity within the subgroups was reduced in group 1 (in which males were more prevalent than females; pooled OR: 0.63, 95% CI 0.46–0.85) and group 2 (in which females were more prevalent than males; pooled OR: 0.42, 95% CI 0.28–0.63). Therefore, the distribution of sex in the smoking and non-smoking groups may be a source of heterogeneity (Fig. 6).

Subgroup analyses by number of men and women in the smoking group compared to the non-smoking group. Group 1 has a mean age ≥ 40. Group 2 has a mean age < 40.
Age
Five studies21,22,24,27,28 reported data regarding the age of the patients in the smoking and non-smoking groups. Among patients aged ≥ 40 years, smoking exerted a protective effect against UC compared with not smoking (OR: 0.63, 95% CI 0.46–0.85). Among patients aged < 40 years, smoking did not exert a significant protective effect against UC compared to not smoking (OR: 0.36, 95% CI 0.10–1.23, I2 = 61%, P = 0.036). The heterogeneity assessment indicated considerable inconsistencies across the studies (P = 0.005, I2 = 87.1). Therefore, age was not a source of heterogeneity in this study (Fig. 7).

Subgroup analyses differentiated by age segments. Group 1 has a mean age ≥ 40. Group 2 has a mean age < 40.
Risk of bias analysis for subgroup analyses
The results of subgroup analyses for sex (Supplement 2, Fig. S5) and age (Supplement 2, Fig. S6) revealed that the data were reliable and had good symmetry. In addition, the distribution of the effect sizes was relatively balanced among different studies; no obvious publication bias was observed. In addition, the results were determined to be reliable, though publication bias or other influencing factors could not be ruled out (Supplement 2, Fig. S7).
Discussion
The impact of smoking on UC remains controversial in the medical community. Although it has been suggested that smoking exhibits a protective effect against UC30, this hypothesis has not been universally accepted, and the relationship between smoking and the pathophysiology of UC currently remains unclear. As such, in the present study, we conducted a meta-analysis of nine case–control studies21,22,23,24,25,26,27,28,29 to assess the association between smoking status and UC incidence. This meta-analysis revealed a significant protective effect of smoking against UC. Specifically, smokers showed a significantly lower risk of developing UC than non-smokers, with an overall OR of 0.48 (95% CI 0.40–0.56), indicating that smokers have nearly half the likelihood of developing UC than non-smokers. These results support the hypothesis that smoking may influence the pathogenesis of UC in a protective manner. Furthermore, the results were even more pronounced when smokers were compared with former smokers. Smokers demonstrated a marked protective effect against UC, with a combined OR of 0.26 (95% CI 0.21–0.32), further emphasising the protective role of smoking against the development of UC. In contrast, former smokers exhibited an increased risk of UC, with a combined OR of 1.84 (95% CI 1.13–3.30), indicating that smoking cessation may reverse the protective effects of smoking. These findings thus highlight the dynamic and temporal nature of the effects of smoking.
In this meta-analysis, the effects of smoking on UC were systematically assessed. The risk of UC was found to be lower in smokers than that in non-smokers. Current smokers exhibited a relatively lower risk of developing UC than former smokers. This finding is consistent with prior studies suggesting that smoking is a protective factor against UC, and that smoking cessation increases the risk of developing UC. Similar prior studies included those by Jiang et al.31 (Compared to non-smokers, smokers had an OR of 0.28 [95% CI 0.16–0.48, P = 0.0001], while former smokers had an OR of 4.36 [95% CI 1.46–13.04, P = 0.008]), de Saussure et al.32 (compared to smokers, both non-smokers and former smokers had an OR of 2.40 [95% CI 1.31–4.38, P = 0.004]), and Treton et al.33 (compared to non-smokers, smokers had an OR of 0.6 [95% CI 0.4–1.0], while former smokers had an OR of 2.0 [95% CI 1.1–3.7]), which all suggested that smoking may serve as a protective facto against UC, while smoking cessation increases the risk of developing the condition31,32,33. The results of the current study further support the hypothesis that smoking may reduce the risk of UC, and that the protective effects of smoking may dissipate after quitting. While the exact mechanism underlying the protective effect of smoking remains unclear, potential mechanisms include immunomodulatory, vascular, and intestinal.
One of the key mechanisms proposed to explain the protective effect of smoking in UC is its modulation of immune responses within the gut. Smoking, primarily through the component nicotine, triggers an interaction with nicotinic acetylcholine receptors (nAChRs) on immune cells, particularly T cells and macrophages. This interaction is thought to inhibit the production of pro-inflammatory cytokines, such as tumour necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), which play pivotal roles in the inflammatory pathways associated with UC34. Further, nicotine induces an anti-inflammatory effect by skewing the immune response towards a Th2-dominant profile, while simultaneously suppressing Th1-mediated responses. This shift reduces the production of inflammatory cytokines, thereby contributing to a decrease in the intensity of the immune activation characteristic of UC35. From a vascular perspective, smoking exerts both acute and chronic effects on endothelial function, which may influence the pathophysiology of UC. Initially, smoking enhances the production of nitric oxide (NO), a vasodilator that improves blood flow and oxygen delivery to the gut36. This temporary improvement in endothelial function and vascular perfusion could provide some degree of protection against the tissue hypoxia and ischemia commonly observed in UC, particularly in the active disease phases. Another crucial aspect underlying the protective effect of smoking on UC lies in its impact on the intestinal epithelial barrier. The epithelial barrier serves as the first line of defence against microbial invasion, and its integrity is vital for maintaining gut health. Smoking appears to enhance the production of mucins and strengthens the epithelial cell layer, which may help to prevent pathogen translocation and reduce inflammatory responses37,38. Moreover, smoking influences the gut microbiota, which plays a critical role in maintaining intestinal homeostasis. Specifically, evidence suggests that smoking induces a shift in the gut microbiota composition, promoting the growth of certain beneficial microbes, such as Lachnospira39. This microbial shift could exert a protective role in UC by promoting the production of short-chain fatty acids (SCFAs), which reduce the production of inflammatory cytokines, contributing to the overall protective effect of smoking in UC40. However, it is important to note that while smoking may initially promote the growth of beneficial bacteria, long-term smoking can lead to dysbiosis, which can exacerbate inflammation and impair mucosal healing. Furthermore, smoking induces several molecular changes, including epigenetic modifications, such as DNA methylation and histone modifications, which can alter the expression of genes involved in immune responses and mucosal integrity. These changes are believed to play a role in the modulation of the inflammatory response in UC, with some studies indicating that smoking can promote the expression of genes that protect against inflammation in the short term, while also inducing detrimental long-term effects41. However, the precise role of these molecular alterations in the pathogenesis of UC remains an area of active research.
While smoking can offer certain protective effects against UC, a substantial body of evidence highlights the significant associated health risks. On an individual level, smoking severely compromises the immune system, weakening the body’s natural defences, and making individuals more susceptible to infections. It also increases the likelihood of developing other chronic diseases. Smoking is particularly damaging to the vital organs, such as the lungs, heart, and blood vessels, significantly raising the risk of heart attacks, strokes, and chronic obstructive pulmonary disease (COPD). Furthermore, smoking impairs physical fitness, leading to reduced stamina and chronic fatigue. In addition, it exacerbates mental health issues, including stress and anxiety, which negatively affect overall well-being. Importantly, in pregnant women, smoking poses severe risks to the mother and baby, being associated with preterm birth, low birth weight, and complications during labour, which can have lasting effects on the health of the unborn child. At a societal level, smoking represents a major public health challenge, contributing significantly to healthcare costs worldwide, and placing an avoidable strain on healthcare systems. This impact extends beyond smokers themselves, as non-smokers exposed to second-hand smoke are also at risk of health complications due to the harmful chemicals and toxins present in tobacco smoke. As such, it is inappropriate to advocate smoking merely due to its potential protective effect against UC.
More research regarding the association between smoking and UC is required. For example, the protective mechanisms of smoking against UC, such as the roles of nicotine and carbon monoxide in the intestinal tract, need to be elucidated. In addition, the identification of the specific active components and targets of action and the effective use of cigarette components in the treatment of UC require further investigation. Further research is also needed to determine the variability of different populations (based on characteristics such as age, sex, and pregnancy) affected by smoking, and the reasons for such differences in the development of effective treatments. Extended monitoring and tracking is also required to determine the impact of smoking on patients with UC. The effects of e-cigarettes or other nicotine substitutes must also be investigated. In addition, studies regarding how the duration and quantity of smoking correlate with UC are needed. These studies could thus help to determine how cigarette components could be used to treat UC. Studies investigating the relationship among smoking time, smoking volume, and UC are thus necessary. Such investigations will help researchers to understand the complex relationship between smoking and UC, and provide better treatment options for patients.
To the best of our knowledge, this is the first meta-analysis to demonstrate the effect of smoking status on UC by comparing different smoking statuses. Overall, this meta-analysis found that smoking had a protective effect on UC, which may present innovative perspectives for the treatment of UC. However, this study is not without limitations. First, the results of this meta-analysis were dependent on the quality of the included studies and the accuracy of the experimental studies; therefore, the extent to which they can be generalised for clinical application remains to be tested. Second, as the sample sizes, study populations, durations of smoking, and severities of UC differed in the included studies, the results of this study may be heterogeneous, which could affect the study conclusions. Third, the number of included studies was small, which may introduce a risk of bias. Finally, this study did not investigate the mechanisms involved in the protective effects of smoking against UC, nor did it determine which specific components of cigarettes play a role in the association between smoking and UC.
Conclusion
Overall, the present study found that smoking exhibited a protective effect against the development of UC. However, this protective effect may be influenced by a variety of factors, including sex, age, duration of smoking, and volume of smoking. As smoking is associated with numerous health risks, including increased risks of lung cancer and hypertension, it should not be encouraged, despite its protective effects against UC. Nevertheless, future studies should further explore the pathogenesis of UC and the specific components of tobacco that protect against UC to develop safe and effective ways to utilise this association for alleviating patient suffering and improving quality of life.
Data availability
Original contributions presented in the study are included in the article/supplementary material and further queries can be directed to the corresponding author:Minhui Li (prof_liminhui@yeah.net).
References
Guan, Q. et al. A comprehensive review and update on the pathogenesis of inflammatory bowel disease. J. Immunol. Res. 2019, 7247238. https://doi.org/10.1155/2019/7247238 (2019).
He, J., Ni, Z. & Li, Z. Intercellular adhesion molecule 1 and selectin l play crucial roles in ulcerative colitis. Medicine (Baltimore) 102, e36552. https://doi.org/10.1097/MD.0000000000036552 (2023).
Correction: British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 70, 1 (2021). https://doi.org/10.1136/gutjnl-2019-318484corr1.
Zou, J., Liu, C., Jiang, S., Qian, D. & Duan, J. Cross talk between gut microbiota and intestinal mucosal immunity in the development of ulcerative colitis. Infect. Immun. 89, e0001421. https://doi.org/10.1128/IAI.00014-21 (2021).
Sun, Y., Zhang, Z., Zheng, C. Q. & Sang, L. X. Mucosal lesions of the upper gastrointestinal tract in patients with ulcerative colitis: a review. World J. Gastroenterol. 27, 2963–2978. https://doi.org/10.3748/wjg.v27.i22.2963 (2021).
Zhang, S. et al. An assessment system for clinical and biological interpretability in ulcerative colitis. Aging (Albany NY) 16, 3856–3879. https://doi.org/10.18632/aging.205564 (2024).
Ramos, G. P. & Papadakis, K. A. Mechanisms of disease: Inflammatory bowel diseases. Mayo Clin. Proc. 94, 155–165. https://doi.org/10.1016/j.mayocp.2018.09.013 (2019).
Yokoyama, Y. et al. Current diagnostic and therapeutic approaches to cytomegalovirus infections in ulcerative colitis patients based on clinical and basic research data. Int. J. Mol. Sci. 21, 2438. https://doi.org/10.3390/ijms21072438 (2020).
Niu, Y., Zhang, J., Shi, D., Zang, W. & Niu, J. Glycosides as potential medicinal components for ulcerative colitis: A review. Molecules 28, 5210. https://doi.org/10.3390/molecules28135210 (2023).
Zhang, K., Guo, J., Yan, W. & Xu, L. Macrophage polarization in inflammatory bowel disease. Cell Commun. Signal. 21, 367. https://doi.org/10.1186/s12964-023- (2023).
Wang, B. & Zhou, G. Relationship of inflammatory bowel disease with dietary habits and smoking. J. Nantong Univ. (Med. Ed.) 39, 203–205. https://doi.org/10.16424/j.cnki.cn32-1807/r.2019.03.013 (2019).
Singh, N. & Bernstein, C. N. Environmental risk factors for inflammatory bowel disease. United Eur. Gastroenterol. J. 10, 1047–1053. https://doi.org/10.1002/ueg2.12319 (2022).
Yao, H., Cai, Y. & Fang, S. Research progress on the effects of environmental factors on inflammatory bowel disease. J. Med. Res. 51, 144–147 (2022).
Yuan, S. et al. Smoking, alcohol consumption, and 24 gastrointestinal diseases: Mendelian randomization analysis. Elife 12, e84051. https://doi.org/10.7554/eLife.84051 (2023).
Miller, T. J. et al. The harm-reduction quandary of reducing adult smoking while dissuading youth initiation. Am. J. Public Health 110, 788–789. https://doi.org/10.2105/AJPH.2020.305688 (2020).
Piovani, D. et al. Environmental risk factors for inflammatory bowel diseases: An umbrella review of meta-analyses. Gastroenterology 157, 647-659.e4. https://doi.org/10.1053/j.gastro.2019.04.016 (2019).
Wang, P. et al. Smoking and inflammatory bowel disease: A comparison of China, India, and the USA. Dig. Dis. Sci. 63, 2703–2713. https://doi.org/10.1007/s10620-018-5142-0 (2018).
Nicolaides, S., Vasudevan, A., Long, T. & van Langenberg, D. The impact of tobacco smoking on treatment choice and efficacy in inflammatory bowel disease. Intest. Res. 19, 158–170. https://doi.org/10.5217/ir.2020.00008 (2021).
AlQasrawi, D., Qasem, A. & Naser, S. A. Divergent effect of cigarette smoke on innate immunity in inflammatory bowel disease: A nicotine-infection interaction. Int. J. Mol. Sci. 21, 5801. https://doi.org/10.3390/ijms21165801 (2020).
Li, L. F. et al. Cigarette smoking and gastrointestinal diseases: The causal relationship and underlying molecular mechanisms (review). Int. J. Mol. Med. 34, 372–380. https://doi.org/10.3892/ijmm.2014.1786 (2014).
Nishikawa, A. et al. Active and passive smoking and risk of ulcerative colitis: A case-control study in Japan. J. Gastroenterol. Hepatol. 37, 653–659 (2022).
De Saussure, P. et al. Appendectomy, smoking habits and the risk of developing ulcerative colitis: A case-control study in a private practice setting. Gastroenterol. Clin. Biol. 31, 493–497 (2007).
Regueiro, M., Kip, K. E., Cheung, O., Hegazi, R. A. & Plevy, S. Cigarette smoking and age at diagnosis of inflammatory bowel disease. Inflamm. Bowel Dis. 11, 42–47 (2005).
Silverstein, M. D., Lashner, B. A. & Hanauer, S. B. Cigarette smoking and ulcerative colitis: A case-control study. Mayo Clin. Proc. 69, 425–429 (1994).
Nakamura, Y. & Labarthe, D. R. A case-control study of ulcerative colitis with relation to smoking habits and alcohol consumption in Japan. Am. J. Epidemiol. 140, 902–911 (1994).
Katschinski, B. D. et al. Smoking and sugar intake in ulcerative colitis: A case-control study. Eur. J. Gastroenterol. Hepatol. 5, 91–95 (1993).
Sandler, R. S., Sandler, D. P., McDonnell, C. W. & Wurzelmann, J. I. Childhood exposure to environmental tobacco smoke and the risk of ulcerative colitis. Am. J. Epidemiol. 135, 603–608 (1992).
Lindberg, E., Tysk, C., Andersson, K. & Järnerot, G. Smoking and inflammatory bowel disease: A case-control study. Gut 29, 352–357 (1988).
Boyko, E. J., Koepsell, T. D., Perera, D. R. & Inui, T. S. Risk of ulcerative colitis among former and current cigarette smokers. N. Engl. J. Med. 316, 707–710 (1987).
Yang, A. Z. & Jostins-Dean, L. Environmental variables and genome-environment interactions predicting IBD diagnosis in a large UK cohort. Sci. Rep. 12, 10890 (2022).
Jiang, L. et al. Risk factors for ulcerative colitis in a Chinese population—An age-matched and sex-matched case-control study. J. Clin. Gastroenterol. 41, 280–284 (2007).
De Saussure, P. et al. Appendectomy, smoking habits and the risk of developing ulcerative colitis: A case-control study in private practice setting. Gastroenterol. Clin. Biol. 31, 493–497 (2007).
Treton, X. Risk of ulcerative colitis among former and current cigarette smokers. Colon Rectum 5, 256–258 (2011).
Mahmoudzadeh, L., Abtahi Froushani, S. M., Ajami, M. & Mahmoudzadeh, M. Effect of nicotine on immune system function. Adv. Pharm. Bull. 13, 69–78 (2023).
Nordman, J. C. et al. The α4 nicotinic receptor promotes CD4+ T-cell proliferation and a helper T-cell immune response. Mol. Pharmacol. 85, 50–61 (2014).
Hahad, O. et al. Tobacco smoking and vascular biology and function: Evidence from human studies. Pflugers Arch. 475, 797–805 (2023).
Świrkosz, G. et al. The role of the microbiome in the pathogenesis and treatment of ulcerative colitis: A literature review. Biomedicines 11, 3144 (2023).
An, J. et al. The role of intestinal mucosal barrier in autoimmune disease: A potential target. Front. Immunol. 13, 871713 (2022).
Zhu, Z. et al. Altered interaction network in the gut microbiota of current cigarette smokers. Eng. Microbiol. 4, 100138 (2024).
Imade, E. E. & Obayagbona, N. O. Impact of cigarette smoking on gut microbial dysbiosis: A structured literature review. Gut Microbiome (Camb.) 5, e13 (2024).
Yan, A. Q. et al. Differential impact of smoking on methylome and transcriptome in Crohn’s disease and ulcerative colitis. Inflamm. Bowel Dis. 30, 981–991 (2024).
Acknowledgements
I would like to express my sincere gratitude to Minhui Li, Shenghua Shi, and Rigen Mo for their support with the research design, research supervision, and funding acquisition for this study. I would also like to thank Yue Tan for her assistance with the data retrieval and methodological support. I am also deeply indebted to Yangyang Yu and Dawei An for their help with the data screening and extraction.
Funding
This work received support from the following projects: The Inner Mongolia Autonomous Region Traditional Chinese Medicine Young Talents Project [Neiwei Zhong (Mongolia) Heritage Zi (2022) No. 108]; The Inner Mongolia Autonomous Region Health Science and Technology Plan Project [NO.202201123, NO.202202141]; The Inner Mongolia Autonomous Region Health Commission’s Project for the Construction of High-Level Clinical Specialties in Public Hospitals in the Capital Region [NO.2023SGGZ046]; The Science and Technology Project of the Joint Public Hospital Research Fund [NO.2023GLLH0162].
Author information
Authors and Affiliations
Contributions
Minhui Li, Shenghua Shi, and Rigen Mo: Designed the research, oversaw the study, and acquired funding. Yong Mi: Searched, screened, and extracted the data, analysed the data, and wrote the original draft. Dawei An and Yangyang Yu: Screened and extracted the data. Yue Tan: Data curation and methodology. All of the authors have read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mi, Y., Tan, Y., Yu, Y. et al. Relationship between smoking status and ulcerative colitis: a meta-analysis based on a case–control study. Sci Rep 15, 13329 (2025). https://doi.org/10.1038/s41598-025-97617-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97617-9
