
Abstract
The triglyceride glucose-weight adjusted waist index (TyG-WWI) has emerged as a straightforward and reliable alternative for assessing insulin resistance (IR). However, the relationship between the TyG-WWI index and the incidence of stroke, especially in individuals with different glucose metabolism status, is still unclear. The data for this study was obtained from the China Health and Retirement Longitudinal Study (CHARLS). The primary endpoint was the occurrence of stroke events. We utilized multivariate Cox proportional hazard models and restricted cubic spline (RCS) analysis to examine the relationship between the TyG-WWI index and the risk of stroke in individuals with different glycemic metabolic states. A total of 8895 participants were included in this study, 831 (9.3%) stroke events were recorded during the follow-up period. After fully adjusting for covariates, per SD increase in the TyG-WWI index was associated with a 11% increase in stroke risk (HR: 1.11, 95% CI 1.02, 1.20) in all participants. The TyG-WWI index was further categorized into quartiles, the adjusted HRs (95% CIs) for Q2, Q3, and Q4 compared to Q1 being 1.37 (95% CI 1.09, 1.72), 1.42 (95% CI 1.13, 1.78), and 1.50 (95% CI 1.17, 1.93), respectively. Furthermore, high levels of the TyG-WWI index were found to be linked to an increased risk of stroke in prediabetes mellitus (Pre-DM) participants across Cox models. However, this association was not observed in participants with normal glucose regulation (NGR) and diabetes mellitus (DM) (all P > 0.05). RCS analysis also demonstrated that higher baseline TyG-WWI index levels were associated with higher HRs for stroke in all participants and those with Pre-DM. The TyG-WWI index significantly associates with stroke risk in middle-aged and elderly Chinese populations. Moreover, this relationship exhibits distinct characteristics influenced by the individual's glucose metabolism status.
Similar content being viewed by others
Introduction
Stroke is the leading cause of death and disability among adults worldwide, presenting a significant challenge to public health1. In China, the incidence of stroke in 2019 was 1.86 times higher than in 1990, directly affecting about 2.4 million people2,3. Research indicates that metabolic abnormalities such as obesity, glucose metabolism disorders, and lipid imbalances are major risk factors for stroke, significantly burdening healthcare systems worldwide4. Therefore, it is necessary to develop cost-effective and reproducible indicators, and strengthen early identification of individuals at high risk of stroke.
Insulin resistance (IR) is defined as a diminished physiological response to insulin within the body. This condition serves as a significant pathological mechanism associated with various metabolic disorders5,6,7. Previous research has demonstrated a significant correlation between IR and both the incidence and prognosis of stroke8,9. The triglyceride-glucose (TyG) index was first proposed in 2008 and has become a reliable biomarker for IR10,11. Recent studies have emphasized the association between TyG index and stroke events, but its correlation with obesity in predicting stroke risk is still unclear12,13.
Obesity is a notable risk factor for stroke, especially among individuals with increased abdominal fat, which is closely linked to stroke incidence14,15,16. The weight-adjusted waist index (WWI) stands out as a crucial obesity indicator, effectively combining weight and waist circumference. This innovative measurement provides a significantly more accurate assessment of fat distribution, and underscores the vital role of WWI in predicting stroke risk17,18. Previous studies have demonstrated that integrating the TyG index with obesity-related indicators can serve as a robust biomarker for evaluating IR19. Therefore, combining the TyG index with the WWI has the potential to enhance the effectiveness of early stroke symptom identification. However, the association between the TyG-WWI index and stroke incidence, particularly in individuals with different glucose metabolic states, remains unclear.
To fill this gap, we analyzed the data of the China Health and Retirement Longitudinal Study (CHARLS), aiming to explore the complex relationship between TyG-WWI index and stroke risk under different glucose regulation states, and provide more evidence for the practical application of TyG-WWI in the real world.
Methods
Study population
This study utilizes data from the China Health and Retirement Longitudinal Study (CHARLS) for longitudinal research. The research methods and data collection procedures used by CHARLS have been extensively documented and published20. The initial baseline survey, known as the first wave, was conducted in 2011, using standardized questionnaires to collect relevant information from participants. Wave 1 of CHARLS gathered data from 17,708 participants representing approximately 10,000 households across 150 counties and districts, as well as 450 villages and resident committees. To date, five waves of survey data have been made available, covering the period from 2011 to 2020. The Ethics Committee of Peking University approved the CHARLS study, and all participants signed informed consent forms.
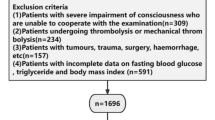
The participant screening process for this study is outlined in Fig. 1. The initial dataset consisted of 17,708 participants identified during Wave 1, which served as the baseline. We excluded 6072 participants due to missing information regarding FPG and TG at baseline. Additionally, 1838 participants were excluded for not providing waist circumference and weight data. We also removed 73 participants who did not have HbA1c data available. Furthermore, 289 participants were excluded for not disclosing their age and being under 45 years old. Moreover, 541 participants were excluded due to a history of stroke, missing stroke data, or loss to follow-up. Consequently, a total of 8813 participants were excluded, leaving 8895 participants in the final cohort of this study.

Flow chart of the study population.
Calculation of TyG-WWI index
The TyG-WWI index was obtained by using the following formula17,21: TyG = ln [FPG (mg/dL) × TG (mg/dL) / 2] ); WWI = waist circumference (cm)/√weight (kg); TyG-WWI = TyG × WWI.
Assessment of incident stroke
The primary outcome of this study is the occurrence of stroke. This was evaluated by posing the important question: “Have you ever been diagnosed with a stroke by a physician?” The timeframe for assessing the onset of stroke was defined as the interval between the most recent interview and the first recorded occurrence of the conditions22,23.
Assessments of covariates
In this study, trained investigators utilized structured questionnaires to gather demographic information from participants, including gender, age, residence, education level, and marital status. They also collected data on lifestyle factors such as smoking and drinking habits, as well as medical history regarding diseases and medications of hypertension, diabetes, and dyslipidemia. Professional examiners measured the height, weight, and waist circumference (WC) of all participants. Additionally, laboratory test results were obtained for various health indicators, including C-reactive protein (CRP), blood urea nitrogen (BUN), serum creatinine (Scr), fasting plasma glucose (FPG), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), hemoglobin A1c (HbA1c), and uric acid (UA).
Hypertension was defined by meeting one of the following criteria: (1) self-reported hypertension diagnosed by a physician, (2) taking antihypertensive medications, (3) systolic blood pressure (SBP) ≥ 140 mmHg, (4) diastolic blood pressure (DBP) ≥ 90 mmHg. Dyslipidemia was identified by TG ≥ 150 mg/dL, TC ≥ 240 mg/dL, HDL-C < 40 mg/dL, LDL-C ≥ 160 mg/dL, current use of lipid-lowering drugs, or self-reported dyslipidemia diagnosed by a physician. DM was defined by meeting at least one of the following criteria: (1) FPG ≥ 126 mg/dL, (2) HbA1c ≥ 6.5%, (3) use of antidiabetic medications, (4) self-reported diabetes diagnosed by a doctor. Pre-DM was characterized by an FPG of 100 to 125 mg/dL or an HbA1c of 5.7–6.4%. NGR was defined as FPG < 100 mg/dL and HbA1c < 5.7%.
Statistical analysis
The extent of missing data in this study is presented in Table S1. To mitigate potential bias, multiple imputations were employed to address the missing values. For quantitative variables that conform to a normal distribution, the results are represented as means and standard errors, with differences between groups assessed using analysis of variance (ANOVA). For quantitative variables that do not meet the criteria for normal distribution, the median and interquartile range are provided, and differences among groups are evaluated utilizing the Kruskal-Wallis test. Categorical variables are described using counts and percentages, with statistical evaluation conducted through the Chi-square test.
Participants were categorized into four groups based on the quartiles of the TyG-WWI index. Q1 ≤ 88.69; 88.69 < Q2 ≤ 96.05; 96.05 < Q3 ≤ 104.13 ; Q4 > 104.13. Kaplan-Meier curves and log-rank tests were employed to evaluate the incidence of stroke. To assess collinearity between the TyG-WWI index and other covariates, tolerance values and variance inflation factors (VIFs) were analyzed. The findings indicated that the VIF for TC and LDL-C exceeded 5, leading to their exclusion from the multivariate model (Table S2). The association between the TyG-WWI index and stroke incidence was examined using Cox regression models. Three distinct models were developed for a thorough analysis: Model 1 was unadjusted, Model 2 included adjustments for gender, age, residence, marital status, and education level, while Model 3 contained additional adjustments for smoking status, drinking status, hypertension, dyslipidemia, hypertension medications, dyslipidemia medications, height, CRP, BUN, Scr, HDL‑C, and UA. Furthermore, a fully adjusted restricted cubic splines (RCS) analysis was performed to investigate the dose-response relationship between the TyG-WWI index and the risk of stroke. Additionally, we conducted an assessment of the relationship between the TyG-WWI index and stroke risk across different states of glucose metabolism. This analysis included participants with NGR, Pre-DM, and DM.
Subgroup analyses were conducted to assess whether the effect of the TyG-WWI index on the incidence of stroke varied among different demographic groups. These analyses were stratified by several factors, including gender, age (45–60 years and 60 years or older), residence, marital status, education level, smoking status, drinking status, hypertension, dyslipidemia, and body mass index (BMI) (BMI: < 24, 24–28, and ≥ 28 kg/m2). To strengthen the reliability of our findings, we performed three robust sensitivity analyses. Firstly, we excluded non-fasting participants from the data set before conducting further analysis. Secondly, we reanalyzed the dataset after removing all missing values. Thirdly, we calculated the E-value to quantify the minimum strength of association that an unmeasured confounder would require with both TyG-WWI index and stroke risk to explain away the observed associations24. All statistical analyses were conducted using Stata 17.0 and R version 4.2.2, with P-values < 0.05, which was considered statistically significant.
Results
Baseline characteristics of participants
The baseline information of all participants was described across the TyG-WWI index quartiles in Table 1. The study included 8895 participants from the CHARLS, with a gender distribution of 4780(53.7%) female and 4115(46.3%) male. The average age of participants was 59.31 ± 9.22 years. Additionally, individuals with higher quartiles of the TyG-WWI index were more likely to be older, female, urban, had lower education levels, never smokers, never drinkers, and tended to have hypertension, diabetes, and dyslipidemia than those with lower quartiles of the TyG-WWI index. For laboratory test, higher TyG-WWI index quartiles was associated with increased CRP, FPG, TC, and UA. In contrast, higher quartiles of the TyG-WWI index were associated with lower levels of height, BUN, Scr and HDL-C.
Association between the TyG-WWI index and the risk of incident stroke
831 (9.3%) stroke events were recorded during the follow-up period. According to the TyG-WWI index quartiles, the incidences of stroke from Q1 to Q4 were 133(6.0%), 197(8.9%), 225(10.1%), and 276(12.4%), respectively. The analysis of the Kaplan–Meier cumulative incidence curve indicates a progressive increase in stroke events from the Q1 to Q4 groups, with statistically significant differences identified (Fig. 2A, log-rank test P < 0.001). Furthermore, the Cox proportional hazard models demonstrated a significant association between the TyG-WWI index and an elevated incidence of stroke in the fully adjusted model (Model 3). When the TyG-WWI index was analyzed as a continuous variable, we found that each standard deviation (SD) increment in the TyG-WWI index was associated with an 11% increase in stroke risk, as indicated by a HR of 1.11 (95% CI 1.02, 1.20). Additionally, when the TyG-WWI index was examined as a four-category variable, and after full covariate adjustment (Model 3), the adjusted HRs with their 95% CIs for categories Q2, Q3, and Q4, compared to Q1, were as follows: Q2 had an HR of 1.37 (95% CI 1.09, 1.72), Q3 had an HR of 1.42 (95% CI 1.13, 1.78), and Q4 had an HR of 1.50 (95% CI 1.17, 1.93). These findings indicate that individuals in categories Q2, Q3, and Q4 experienced a 27%, 35%, and 44% increase in stroke risk, respectively, compared to those in Q1 (Table 2).


The Kaplan–Meier curves analysis depict the cumulative incidence of stroke across the TyG-WWI index quartiles for total participants (A), participants with NGR (B), participants with Pre-DM (C), and participants with DM (D).
Further RCS analyses showed a significant linear relationship between the TyG-WWI index and stroke events. According to the RCS analysis, when the TyG-WWI index > 85, the risk of stroke incidence significantly increases (Fig. 3A).


Association of the TyG-WWI index and the risk of stroke using a multivariable-adjusted restricted cubic spines model. (A) total participants; (B) participants with NGR; (C) participants with Pre-DM. (D) participants with DM.
Associations between the TyG-WWI index and incident stroke regulated by individual glucose metabolic states
During the follow-up period, 270(7.7%) participants with NGR, 377(9.7%) participants with Pre-DM, and 184(12.3%) participants with DM were identified as having experienced their first stroke. The Kaplan-Meier curves indicated a significant difference in the cumulative incidence of stroke for both the NGR group (Fig. 2B) (P = 0.0015) and the Pre-DM group (Fig. 2C) (P < 0.0001) across the four TyG-WWI index groups. However, no significant difference was found in the DM group (Fig. 2D) (P = 0.3167).
The analysis of the TyG-WWI index as a continuous variable demonstrated a significant association with an elevated risk of stroke among individuals with Pre-DM. In Model 3, the HR was found to be 1.19 (95% CI 1.04, 1.37). For individuals categorized with Pre-DM, the HRs were 1.37 (95% CI 0.98, 1.90) for Q2, 1.44 (95% CI 1.02, 2.02) for Q3, and 1.52 (95% CI 1.04, 2.22) for Q4, with a p-trend of 0.042. However, whether the TyG-WWI index was treated as a continuous or categorical variable, no significant differences were observed among the TyG-WWI index groups in individuals with NGR and DM in Model 3 (all P > 0.05)(Table 3).
The RCS analysis showed a notable increase in the risk of stroke in individuals with Pre-DM as baseline TyG-WWI index rises, demonstrating a linear relationship (P for nonlinear = 0.926) (Fig. 3C). Conversely, the analysis did not reveal a significant dose-response correlation between the TyG-WWI index and the risk of stroke in individuals with NGR (Fig. 3B) and DM (Fig. 3D).
Subgroup analysis
A subgroup analysis was conducted to further investigate the relationship between the TyG-WWI index and the occurrence of stroke events. Significant positive associations were found between the TyG-WWI index and the risk of stroke in several demographics: patients aged 45 to 60 years; females; individuals living in rural areas; married people; those with primary school, high school or above; never or current smokers; non-drinkers; as well as patients with or without hypertension, and non-dyslipidemia (Table 4). Notably, a significant interaction was observed between the TyG-WWI index and education level (P value for interaction = 0.011). However, no significant interactions were detected between the TyG-WWI index and any other variables (all P values for interaction > 0.05) (Table 4).
Sensitivity analysis
To assess the robustness of the findings, we conducted three sensitivity analyses. The results did not materially change after excluding all non-fasting participants (Table S3 and S4). Additionally, when we removed all missing data and reanalyzed the results, Cox regression analyses generated consistent results with the primary analysis (Table S5 and S6). Furthermore, the E-value for TyG-WWI index was calculated based on Model 3, revealing a E-value of 1.46. The E-values suggest that relatively large unmeasured confounding effects could account for the observed hazard ratios.
Discussion
This study is the first to explore the relationship between the TyG-WWI index and stroke risk in middle-aged and elderly patients using large-scale cohort data. Our investigation revealed two noteworthy findings. First, the baseline TyG-WWI index has a significant impact on stroke risk. Second, this relationship is evaluated according to the state of glucose metabolism, which is particularly prominent in the Pre-DM population. The practical significance of this study is far-reaching. The baseline the TyG-WWI index may be a reliable biomarker for stroke risk stratification, and maintaining a low level of the TyG-WWI index may be beneficial to the primary prevention of stroke in individuals with Pre-DM. Our research provides more evidence for the practical application of the TyG-WWI index in the real world.
IR and obesity are significant components of metabolic syndrome, both of which can elevate the risk of stroke25,26. The TyG index has emerged as a reliable indicator of IR. Several studies have demonstrated that the baseline TyG index, changes in the TyG index, and cumulative exposure to the TyG index are closely related to the risk of stroke27,28,29,30.While the BMI serves as a widely accepted standard for assessing obesity and general health, it does not account for variations in fat distribution. This limitation can lead to differing risks of stroke among individuals with similar BMI values, contributing to what is recognized as the “obesity paradox“31. In contrast, the WWI offers a more nuanced approach by integrating weight and waist circumference, thereby focusing on local fat distribution. This enhanced measure improves the predictive capacity for stroke outcomes18,32,33. Recent studies have investigated the relationship between the accumulation and changes in the TyG-WWI index and cardiovascular diseases, revealing that these factors are associated with a higher incidence of cardiovascular diseases34. Nonetheless, the relationship between the baseline levels of the TyG-WWI index and the occurrence of strokes, particularly among individuals with different states of glucose metabolism, remains to be fully elucidated. This study aims to provide, for the first time, critical insights into the predictive value of baseline TyG-WWI index levels regarding stroke risk.
This study presents evidence for the first time that a high baseline TyG-WWI index is associated with an elevated risk of new strokes. This finding stands in contrast to the research conducted by Cui et al., which indicated no significant correlation between the baseline TyG-waist circumference (TyG-WC) index and stroke risk in a cohort of 7115 middle-aged and older adults, incorporating traditional obesity measurements such as waist circumference35. A comprehensive study involving 21,750 participants over a period of nine years showed that compared to other obesity indicators, WWI demonstrated extraordinary discrimination and accuracy in predicting cardiovascular disease. This investigation underscores the significant influence of baseline WWI on cardiovascular disease risk36. Furthermore, a cross-sectional study has established a correlation between elevated WWI and increased prevalence of stroke, emphasizing the critical role of WWI in stroke prevention and management strategies18. Our research indicates that for each one SD increase in the TyG-WWI index, there is an associated 11% increase in the risk of stroke. Furthermore, the RCS demonstrates that a TyG-WWI index exceeding 85 significantly correlates with an elevated stroke risk. To effectively reduce the risk of stroke, it is imperative to maintain the TyG-WWI index below a value of 85. Accordingly, it is recommended to strengthen intervention and management strategies for patients whose TyG-WWI index exceeds this threshold.
This study conducted a comprehensive analysis of the relationship between the TyG-WWI index level and the incidence of stroke across various glucose metabolism states, which is of considerable clinical relevance. Notably, a significant association was identified between the baseline TyG-WWI index level and stroke risk within the Pre-DM population. In contrast, no significant association was found in the NGR and DM groups. In the Pre-DM population, each SD increase in the TyG-WWI index corresponds to a 19% increase in the risk of stroke. Additionally, the RCS analysis did not reveal a dose-response relationship between the TyG WWI and stroke in patients with NGR and DM. However, in patients with Pre-DM, the risk of stroke significantly increased with higher levels of the TyG-WWI index, showing a significant positive linear relationship. Therefore, it is essential to closely monitor and adjust the TyG-WWI index in the Pre-DM population to help reduce the risk of stroke. Consequently, a comprehensive subgroup analysis was conducted, which identified significant positive associations between the TyG-WWI index and the risk of stroke across various demographic groups. This indicates that our results apply to a significant portion of the population.
Although the exact mechanism linking the TyG-WWI index to stroke is not fully understood, several potential explanations have been proposed. Primarily, the TyG-WWI index is recognized as a reliable marker of IR, which is known to contribute to the development of atherosclerosis. This condition leads to intimal hyperplasia of blood vessels and the formation of atherosclerotic plaques, which are significantly associated with the incidence of stroke37,38. Additionally, IR can hinder the utilization of nitric oxide, which adversely impacts vascular endothelial function. This impairment results in vascular damage, thereby increasing the probability of stroke occurrence39,40. Furthermore, individuals with IR often exhibit various metabolic abnormalities, including hyperlipidemia, diabetes, and obesity, all of which are established risk factors for stroke. The TyG-WWI index incorporates multiple indicators, including blood glucose levels, lipid profiles, body weight, and waist circumference, potentially enhancing its capacity to identify individuals at risk for stroke41,42,43. In conclusion, a higher TyG-WWI index may reflect underlying vascular and organ damage that elevates stroke risk. Nonetheless, further research is essential to elucidate the precise mechanisms by which the TyG-WWI index influences the risk of stroke.
This study focuses on the Chinese population, which presents unique metabolic risk characteristics that may differ from those of other races and nationalities. These differences could limit the generalizability of our research findings. Specifically, the Chinese population varies from other ethnic groups in terms of genetics, diet, lifestyle, and environmental factors, all of which can influence the risk of metabolic abnormalities, insulin resistance, and related diseases44,45,46.For instance, research has indicated that different Asian ethnic groups exhibit distinct biological risk factors associated with the development of DM. Additionally, the risk of insulin resistance and lipid metabolism abnormalities varies among various ethnic groups, and it cannot be fully explained by the difference in obesity47,48,49. In our study, these factors significantly impact stroke risk. While our findings may be highly representative of the Chinese population, their applicability to other ethnic groups requires further investigation. Future research should involve a broader range of racial groups to determine whether these findings are universally applicable and to explore how metabolic risk factors across different races influence the pathogenesis of stroke.
The study presents several notable advantages. Firstly, it is the first to examine the association between the TyG-WWI index and stroke. Secondly, as a prospective national longitudinal cohort study with a substantial sample size, the findings are enhanced in terms of reliability. Thirdly, this research uniquely investigates the relationship between the TyG-WWI index and stroke across various glucose metabolic states, while also conducting subgroup analyses that provide valuable clinical insights. Lastly, we undertook three sensitivity analyses to ensure the robustness of our results.
It is important to acknowledge the limitations inherent in this study. Firstly, this is an observational study, and therefore, causality cannot be established between TyG- WWI index and the risk of stroke risk. Secondly, our analysis was based on the TyG-WWI index at baseline, which constrains our ability to evaluate the influence of dynamic changes in indicators on stroke risk. Thirdly, stroke diagnoses were self-reported by participants based on evaluations from their healthcare providers, which may not accurately reflect the actual incidence of stroke. Nevertheless, prior validation supports the reliability of these self-reported stroke events, thereby bolstering their credibility50,51. In the future, we will conduct further exploration to address the possibility of misclassification bias and its impact on the results. Fourthly, while multivariate adjustments were made to account for potential confounding factors, it is still possible that undiscovered confounders may influence the results (such as dietary patterns, physical activity, or socioeconomic status). However, the calculated E-value indicates that our findings are robust, suggesting that unexamined confounding factors are unlikely to have a significant impact on the study’s outcomes. Fifthly, while the diagnostic criteria for glucose metabolic status have been clearly established, there remains a risk of misclassification for participants presenting with critical glucose conditions. Lastly, it is pertinent to note that this study exclusively focused on middle-aged and older individuals in China, which may limit the generalizability of the findings to broader populations.
Conclusion
In middle-aged and elderly Chinese population, this study revealed a significant association between TyG-WWI index and stroke risk. In different glucose metabolic status, high levels of TyG-WWI index were found to be linked to an increased risk of stroke in individuals with Pre-DM. However, this association was not observed in individuals with NGR and DM. The results of this study may emphasize the need for risk management strategies for different glucose metabolic states to prevent patients from developing stroke.
Data availability
The data supporting the findings of this study are available on the CHARLS website (http://charls.pku.edu.cn/).
Abbreviations
- CHARLS:
-
China health and retirement longitudinal study
- IR:
-
Insulin resistance
- FPG:
-
Fasting plasma glucose
- HbA1c:
-
Hemoglobin A1c
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- HDL-C:
-
High-density lipoprotein-cholesterol
- LDL-C:
-
Low-density lipoprotein-cholesterol
- WC:
-
Waist circumference
- WWI:
-
Weight-adjusted waist index
- TyG-WWI:
-
Triglyceride glucose-weight adjusted waist index
- GMS:
-
Glucose metabolic states
- NGR:
-
Normal glucose regulation
- Pre-DM:
-
Prediabetes mellitus
- DM:
-
Diabetes mellitus
References
Global National burden of stroke and its risk factors, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet Neurol. 20(10), 795–820 (2021).
Ma, Q. et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: an analysis for the global burden of disease study 2019. Lancet Public. Health. 6(12), e897–e906 (2021).
Wu, S. et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 18(4), 394–405 (2019).
Mensah, G. A., Fuster, V., Roth, G. A. A. & Heart-healthy and stroke-free world: Using data to inform Global Action J. Am. Coll. Cardiol. 82(25), 2343–2349. (2023).
Kim, S. H. Reaven gobesity and insulin resistance: an ongoing saga. Diabetes 59(9), 2105–2106 (2010).
Lee, S. H. & Park, S. Y. Choi CSInsulin resistance: from mechanisms to therapeutic strategies. Diabetes Metab. J. 46(1), 15–37 (2022).
Gans ROInsulin resistance. N Engl. J. Med. 326(9), 646–647. (1992).
Ding, P. F. et al. Insulin resistance in ischemic stroke: Mechanisms and therapeutic approaches. Front. Endocrinol. (Lausanne) 13, 1092431. (2022).
Kernan, W. N. et al. Insulin resistance and risk for stroke.Neurology, 59(6), 809–815 (2002).
Simental-Mendía, L. E. & Rodríguez-Morán, M. Guerrero-Romero FThe product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab. Syndr. Relat. Disord. 6(4), 299–304 (2008).
Tao, L. C. et al. Triglyceride-glucose index as a marker in cardiovascular diseases: Landscape and limitations. Cardiovasc. Diabetol. 21(1), 68 (2022).
Wang, A. et al. Triglyceride-glucose index and the risk of stroke and its subtypes in the general population: An 11-year follow-up. Cardiovasc. Diabetol. 20(1), 46 (2021).
Zhao, Y. et al. Elevated triglyceride-glucose index predicts risk of incident ischaemic stroke: The rural Chinese cohort study. Diabetes Metab. 47(4), 101246 (2021).
Jaakonmäki, N. et al. Obesity and the risk of cryptogenic ischemic stroke in young Adults. J. Stroke Cerebrovasc. Dis. 31(5), 106380 (2022).
Katsiki, N. & Ntaios, G. Vemmos KStroke, obesity and gender: A review of the literature. Maturitas 69(3), 239–243 (2011).
Keihani, S. et al. Abdominal obesity phenotypes and risk of cardiovascular disease in a decade of follow-up: The Tehran lipid and glucose Study. Atherosclerosis 238(2), 256–263 (2015).
Park, Y. et al. A novel adiposity index as an integrated predictor of cardiometabolic disease morbidity and mortality. Sci. Rep. 8(1), 16753 (2018).
Ye, J. et al. Association between the weight-adjusted waist index and stroke: A cross-sectional study BMC Public. Health 23(1), 1689 (2023).
Zhao, Y. et al. Comparison of six surrogate insulin resistance indexes for predicting the risk of incident stroke: The rural Chinese cohort Study. Diabetes Metab. Res. Rev. 38(7), e3567 (2022).
Zhao, Y. et al. Cohort profile: The China health and retirement longitudinal study (CHARLS). Int. J. Epidemiol. 43(1), 61–68 (2014).
Li, F. et al. Association between the cumulative average triglyceride glucose-body mass index and cardiovascular disease incidence among the middle-aged and older population: A prospective nationwide cohort study in China. Cardiovasc. Diabetol. 23(1), 16 (2024).
Li, H. et al. Association of depressive symptoms with incident cardiovascular diseases in Middle-Aged and older Chinese Adults. JAMA Netw. Open. 2(12), e1916591 (2019).
Zheng, F. et al. Progression of cognitive decline before and after incident stroke. Neurology 93(1), e20–e28. (2019).
VanderWeele, T. J. Ding psensitivity analysis in observational research: Introducing the E-Value. Ann. Intern. Med. 167(4), 268–274 (2017).
DeBoer, M. D. et al. Risk of ischemic stroke increases over the spectrum of metabolic. Syndrome Severity Stroke. 51(8), 2548–2552 (2020).
He, Q. et al. Genetic insights into the risk of metabolic syndrome and its components on stroke and its subtypes: Bidirectional Mendelian randomization. J. Cereb. Blood Flow. Metab. 43(2_suppl), 126–137 (2023).
Huo, R. R. et al. Interacting and joint effects of triglyceride-glucose index (TyG) and body mass index on stroke risk and the mediating role of TyG in middle-aged and older Chinese adults: A nationwide prospective cohort study. Cardiovasc. Diabetol. 23(1), 30 (2024).
Jiang, Y. et al. Association of triglyceride glucose index with stroke: From two large cohort studies and Mendelian randomization analysis. Int. J. Surg. 110(9), 5409–5416 (2024).
Wang, X. et al. Relationship of cumulative exposure to the triglyceride-glucose index with ischemic stroke: A 9-year prospective study in the Kailuan cohort. Cardiovasc. Diabetol. 21(1), 66 (2022).
Wu, Y. et al. The change of triglyceride-glucose index May predict incidence of stroke in the general population over 45 years old. Cardiovasc. Diabetol. 22(1), 132 (2023).
Neeland, I. J. et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 7(9), 715–725 (2019).
Dallongeville, J. et al. Relation between body mass index, waist circumference, and cardiovascular outcomes in 19,579 diabetic patients with established vascular disease: The REACH Registry. Eur. J. Prev. Cardiol. 19(2), 241–249 (2012).
Sadafi, S. et al. Weight-adjusted waist index and cardiovascular disease: A population-based study in Ravansar. Iran Arch. Public. Health 82(1), 219 (2024).
Duan, C. et al. Associations of baseline and changes in the triglyceride glucose-weight adjusted waist index and cardiovascular disease risk: Evidence from middle-aged and older individuals. Cardiovasc. Diabetol. 23(1), 415 (2024).
Cui, C. et al. Comparison of triglyceride glucose index and modified triglyceride glucose indices in prediction of cardiovascular diseases in middle aged and older Chinese adults. Cardiovasc. Diabetol. 23(1), 185 (2024).
Liu, S. et al. Weight-adjusted waist index as a practical predictor for diabetes, cardiovascular disease, and non-accidental mortality risk. Nutr. Metab. Cardiovasc. Dis. 34(11), 2498–2510 (2024).
Johansen, M. C. et al. Association between ischemic stroke subtype and stroke severity: The atherosclerosis risk in communities Study. Neurology 101(9), e913–e921 (2023).
Shimoyama, T. et al. Quantitative CTA vascular calcification, atherosclerosis burden, and stroke mechanism in patients with ischemic stroke. J. Neurol. Sci. 449, 120667. (2023).
Hill, M. A. & Jaisser, F. Sowers JRRole of the vascular endothelial sodium channel activation in the genesis of pathologically increased cardiovascular stiffness. Cardiovasc. Res. 118(1), 130–140 (2022).
Hill, M. A. et al. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism 119, 154766 (2021).
Patel, T. P. et al. Insulin resistance: An additional risk factor in the pathogenesis of cardiovascular disease in type 2 diabetes. Heart Fail. Rev. 21(1), 11–23 (2016).
Koliaki, C. & Liatis, S. Kokkinos aobesity and cardiovascular disease: revisiting an old relationship. Metabolism 92, 98–107. (2019).
Adeva-Andany, M. M. et al. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab. Syndr. 13(2), 1449–1455 (2019).
Wu, Z. et al. Structural variants in the Chinese population and their impact on phenotypes, diseases and population adaptation. Nat. Commun. 12(1), 6501 (2021).
Ng, T. P. et al. Ethnic differences in quality of life in adolescents among Chinese, Malay and Indians in Singapore. Qual. Life Res. 14(7), 1755–1768 (2005).
Zuo, H. et al. Dietary patterns are associated with insulin resistance in Chinese adults without known diabetes. Br. J. Nutr. 109(9), 1662–1669 (2013).
Seah, J. Y. H. et al. Differences in type 2 diabetes risk between East, South, and Southeast Asians living in Singapore: the multi-ethnic cohort. BMJ Open. Diabetes Res. Care 11(4). (2023).
Hall, L. M. et al. Fat oxidation, fitness and skeletal muscle expression of oxidative/lipid metabolism genes in South Asians: Implications for insulin resistance?. PLoS One 5(12), e14197 (2010).
Khoo, C. M. et al. Ethnicity modifies the relationships of insulin resistance, inflammation, and adiponectin with obesity in a multiethnic Asian population. Diabetes Care 34(5), 1120–1126 (2011).
Yuan, X. et al. Validity of self-reported diabetes among middle-aged and older Chinese adults: The China health and retirement longitudinal Study. BMJ Open. 5(4), e006633 (2015).
Choe, S. et al. Validity of Self-reported stroke and myocardial infarction in Korea: The health examinees (HEXA) Study. J. Prev. Med. Public. Health. 52(6), 377–383 (2019).
Acknowledgements
This study utilized data from the CHARLS database. The authors express their gratitude to the CHARLS research team and all individuals who participated in the study.
Funding
This work was supported by the Suzhou “Science and Education Revitalize Health” Youth Science and Technology Project (KJXW2021031) and the Jiangsu Medical Association Interventional Medicine Phase III Special Fund Project (SYH-3201140-0089).
Author information
Authors and Affiliations
Contributions
GH conceived and designed the study and wrote the main manuscript text. GH, ZT and YT analyzed the data. JC and JH conducted the literature search and prepared figures. GH and DZ performed the manuscript review. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
CHARLS was approved by the Institutional Review Board of Peking University (approval number: IRB00001052-11015 for the household survey and IRB00001052-11014 for blood samples), and all participants provided written informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huo, G., Tan, Z., Tang, Y. et al. Association between triglyceride glucose weight adjusted waist index and stroke risk in different glucose metabolism status. Sci Rep 15, 15813 (2025). https://doi.org/10.1038/s41598-025-99618-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-99618-0
Keywords
This article is cited by
-
Association of C-reactive protein/high-density lipoprotein cholesterol ratio with stroke in Chinese adults across different glycemic status
Lipids in Health and Disease (2026)
-
The novel triglyceride‒glucose-weighted adjusted waist index as a supplementary diagnostic tool for heart failure: evidence of improved reclassification beyond traditional TyG-related indices from a cross-sectional study
Cardiovascular Diabetology (2025)
-
Association of novel triglyceride-glucose-related indices with incident stroke in early-stage cardiovascular-kidney-metabolic syndrome
Cardiovascular Diabetology (2025)
-
Triglyceride glucose-weight-adjusted waist index as a cardiovascular mortality predictor: incremental value beyond the establishment of TyG-related indices
Cardiovascular Diabetology (2025)
-
Joint association of triglyceride-glucose index and obesity indicators with stroke risk: a nationwide prospective cohort study
Scientific Reports (2025)
