
Abstract
Around 50% of the variation in cardiovascular disease (CVD) risk is attributable to heritable factors, and polygenic risk scores (PRS) can now capture part of that genetic component. As personalised public health advances, polygenic risk scores (PRS) may offer a useful tool for conveying overall CVD risk, particularly in younger populations, but require evaluation in real-world clinical trials. This study evaluated the effects of integrating coronary artery disease polygenic risk scores (CAD PRS) into CVD risk estimation and risk communication among young, overweight adults (25–44 years, BMI = 25.0–29.99 kg/m2). This was a parallel-group, double-blind, randomised controlled trial with a 12-month follow-up. A total of 1020 participants were randomised into intervention (n = 510) and control (n = 510) groups. The primary outcome measure was BMI; secondary outcomes included systolic and diastolic blood pressure, total, LDL and HDL cholesterol, waist circumference, 10-year CVD risk, preventive treatment prescription, smoking prevalence, alcohol consumption, diet, and physical activity. Per-protocol analyses used t-tests for continuous data, chi-square for categorical data, ANCOVA for adjusted outcomes, linear and logistic models for risk factors, with significance at p < 0.05. Over the 12-month follow-up, the intervention produced no statistically significant differences in BMI between groups (intervention: 27.9 ± 2.5 kg/m2; control: 27.7 ± 2.5 kg/m2; p = 0.291), waist circumference, systolic or diastolic blood pressure, lipid profile, blood glucose, or combined 10-year CVD risk (all p > 0.14). Self-reported behaviours showed limited impact on smoking prevalence and physical activity (p > 0.1). Prescribing and purchasing of lipid-lowering or antihypertensive medications did not differ between groups (IRR for lipid-lowering drugs 0.93; 95% CI 0.73–1.18), underscoring that the intervention had no measurable impact on either cardiometabolic parameters or preventive treatment patterns. This trial showed that communicating high CAD polygenic risk alone did not lead to behavioural changes or improvements in key cardiovascular risk factors. Future studies should assess interventions combining lifestyle counselling and preventive treatment to more effectively evaluate their potential for long-term cardiovascular risk reduction in individuals with high CAD polygenic risk.
Trial registration: Prospectively registered on ClinicalTrials.gov NCT05603663 (03.11.2022).
Similar content being viewed by others


Introduction
Modifying health behaviour is a complex process, and assessing the effectiveness of behaviour change techniques remains challenging1,2,3. Despite decades of public health initiatives and clinical efforts aimed at preventing cardiovascular disease (CVD), its prevalence continues to be alarmingly high4. In Estonia, CVD remains a major health concern, with mortality rates exceeding the EU average and a high burden of risk factors such as hypertension, obesity, and smoking5,6. The impact of CVD extends beyond individual health, often leading to hospitalization, long-term disability, and a decline in overall quality of life7,8. Additionally, the economic burden associated with CVD is substantial, placing strain on healthcare systems and national economies due to the costs of treatment, rehabilitation, and lost productivity9,10.
Health behaviour change models such as the Health Belief Model, Transtheoretical Model, and Theory of Planned Behaviour emphasize how individuals’ perceptions, readiness, and intentions shape their actions11,12,13. Delivering these models relies on primary care workers to communicate CVD risk and provide lifestyle counselling aimed at reducing risk factors and improving patients’ self-perceived risk14,15,16. CVD prevention relies on risk factor reduction and awareness, as major risks like hypertension, obesity, and diabetes stem from poor diet and physical inactivity17. While some evidence supports the positive impact of lifestyle interventions on cardiovascular risk factor management, real-world implementation often faces challenges in achieving sustained change18,19,20.
Coronary artery disease (CAD) has a substantial genetic component, with heritability estimates between 40% and 60% in Northern European populations21,22. As genome-wide association studies (GWAS) have expanded, the polygenic architecture of CAD has become increasingly evident, accounting for over one-third of its heritability23,24. However, the emerging field of polygenic risk scores (PRS) remains relatively understudied in real-life clinical trials25,26. PRS holds potential to improve chronic disease prevention and management, offering insights into how lifestyle factors interact with genetic risk to influence health outcomes27. A significant part of PRS-based risk can be mitigated by managing other risk factors, emphasizing the importance of health behaviour change28.
Several studies have begun exploring the link between PRS and health behaviour change, investigating whether genetic risk knowledge can motivate individuals to adopt healthier lifestyles29,30. These studies suggest that personalized risk data may serve as a powerful catalyst for change, but its effectiveness may depend on age31. Our prior research in Estonia found that revealing high CAD PRS to older adults did not significantly improve health behaviours6. With this study, we aim to examine whether younger individuals are more responsive to genetic risk disclosure, potentially identifying an optimal age window for PRS-based interventions to prevent CVD in high-risk groups.
Polygenic risk scores, including coronary artery disease PRS (CAD PRS), can help identify younger individuals who may benefit most from more aggressive lifestyle modifications, encouraging early intervention and health behaviour change32,33,34. Increasingly accessible PRS testing may guide preventive decisions in primary care, offering public health benefits if supported by evidence and training33,35,36,37. Assessing the clinical utility of CAD PRS requires pragmatic trials to evaluate their role in CVD risk prediction, guide preventive interventions, and determine their value in clinical decision-making35,38,39.
This study aimed to assess whether including high coronary artery disease polygenic risk scores (top 20%) in cardiovascular disease risk assessment and communication affects the body mass index of young (25–44 years) overweight adults (BMI 25.0–29.99 kg/m2).
Methods
Study design
This study was a parallel-group, double-blind, randomised controlled trial (RCT). Participants were randomly assigned in a 1:1 allocation ratio to either the intervention or control arm. A second low-PRS control group was matched to the intervention arm by age group and sex to ensure that the control group participants’ PRS remained masked from the family physicians. The intervention and one control group included individuals in the highest CAD PRS quintile (top 20%), while the matched control group was in the lowest PRS quintile. The outcome analyses in this article focus solely on comparisons between the high-PRS groups.
Eligibility criteria
Study participants were selected from Estonian Biobank (EstBB) cohort participants, including healthy overweight individuals aged 25–44 years (BMI 25.0–29.99 kg/m2) whose CAD PRS score had been pre-calculated by the EstBB following the methodology described by Inouye, et al. (2018)40.
The exclusion criteria were an underlying diagnosis of ischemic heart disease (ICD codes I20-25), stroke or transient ischemic attack (I60-64, I69, G45), peripheral vascular occlusion (I65-66, I67.2, I70, I73.9), or diabetes mellitus (E10-14). Individuals currently using cholesterol-lowering medications or those with comorbid physical or mental illnesses that would hinder their ability to provide consent or participate fully in the study were also excluded.
Interventions
Study interventions were delivered by each participant’s family physician in primary care centres across Estonia. All family physicians received detailed intervention guidelines and three training sessions covering risk assessment, lifestyle counselling, dyslipidaemia management, and hypertension treatment based on estimated risk levels. The intervention entailed family physicians assessing CVD risk, sharing it with study participants, and providing counselling (Fig. 1).

A graphical representation of the intervention approach.
At the first study visit, baseline measurements were collected from study participants, and their CVD risk was calculated using a risk assessment tool41. The CVD risk model was developed using Estonian Biobank data from gene donors aged at least 25 years at recruitment with genotyping data available (n = 202 282) as of January 1, 2022. The model predictors were a combination of cardiovascular risk assessment parameters (age, sex, height, weight, smoking status, total cholesterol, HDL cholesterol, systolic BP) and PRS for coronary artery disease (Fig. 2). The cardiovascular risk assessment parameters were primarily based on the SCORE-2 framework, with two key modifications42. First, we used total cholesterol and HDL cholesterol rather than non-HDL cholesterol. Second, we incorporated height and weight into the risk model since BMI was the primary outcome measure of this study. This modification allowed us to assess CVD risk in a younger population than the SCORE-2 model typically addresses.
At baseline, only intervention arm participants were shown their risk trajectory with PRS included. The risk model produced two graphs: one showing the participant’s current risk trajectory, potential risk reduction through lifestyle changes, and average risk for peers of the same age and sex. The second graph (intervention arm only) presented the participant’s genetic risk relative to the general population. Family physicians reviewed these graphs with participants, offered health counselling, and prescribed lipid-lowering or antihypertensive medications when indicated.

Risk assessment and communication to study participants.
The second study visit, six months after the first, was a remote telemedicine session with family nurses via phone. During the call, the nurse offered counselling and collected self-reported data on participants’ weight and waist circumference.
The third study visit was conducted at the end of the 12-month follow-up, during which updated risk assessments were performed for all participants. For the control group, polygenic risk was now included in the risk assessment, unblinding both physicians and participants to their high PRS status. Changes in overall CVD risk were reviewed, and additional counselling or treatment was offered as needed.
Outcomes
The primary outcome measure was mean BMI (kg/m2) at 12 months, comparing the intervention and control groups. Secondary outcome measures included the difference in mean systolic and diastolic blood pressure (mmHg), mean total cholesterol (mmol/L), mean LDL-and HDL-cholesterol (mmol/L), mean blood glucose (mmol/L), mean waist circumference (cm), and 10-year CVD risk (percentage points) at 12 months. Smoking-related outcomes included the difference in the proportion of current smokers and the mean number of cigarettes consumed among daily smokers between groups at 12 months. Physical activity was evaluated by comparing mean MET values between groups at 12 months. Dietary outcomes included the difference in the proportion of individuals consuming at least the recommended daily amount of fruit (> 200 g) and vegetables (> 300 g). The study also compared the proportion of participants in each study arm for whom family physicians prescribed lipid-lowering or antihypertensive medications during the study period.
Self-reported measures
Online surveys were administered via REDCap at 0, 6, and 12 months to participants for recording their smoking status, alcohol consumption, diet (fruit and vegetable consumption), and physical activity43.
Physical activity was evaluated by calculating SQUASH (Short Questionnaire to Assess Health-enhancing Physical Activity) scores based on online participant surveys administered via REDCap. SQUASH is a validated tool used in research to estimate activity in different domains of daily life, making it suitable for calculating Metabolic Equivalent of Task (MET) scores to quantify energy expenditure44.
Harms
Potential adverse effects related to participation (e.g., increased anxiety, stress from risk communication) were monitored throughout the study via participant self-report and routine follow-up.
Sample size
The sampling frame included all Estonian Biobank (EstBB) cohort participants (202,282 as of 1 January 2022). Eligible participants were aged 25–44, overweight (BMI 25–29.99), undiagnosed with cardiovascular disease or diabetes, and belonging to either the top or bottom quintile for CAD PRS. Preliminary data identified ~ 2,000 individuals in each quintile meeting these criteria. From these, 1300 high-PRS individuals were selected for the intervention and first control group, and ~ 650 low-PRS individuals for a second control group, anticipating a 70% response rate and a final sample of ~ 1,500 (500 intervention, 1,000 controls). Power calculations indicated that this sample size would detect an expected BMI difference of 0.4 kg/m2 one year after the start of the study, a type I error of 0.05, and a study power of 0.8. This is deliberately conservative compared to typical RCTs showing at least 2 kg weight loss45,46. We anticipated smaller effects given our pragmatic primary care setting, with less intensive support and a comprehensive CVD focus rather than weight-loss alone. Sampling also considered family physician practice lists, prioritising those with more eligible participants.
Randomisation
Sequence generation
The study employed simple randomisation using a computer-generated algorithm. A statistician from the EstBB not involved in participant recruitment carried out the randomisation. Randomisation was performed only for the high-PRS intervention and control group. The secondary control group with the lowest quintile PRS was matched to the intervention group based on 5-year age-group and sex.
Blinding
Control group participants and family physicians were blinded to the CAD PRS of control arm participants until the end of the trial. This was done by matching a secondary control group with the lowest quintile PRS to the intervention group based on 5-year age-group and sex. Incorporating a secondary control group for blinding purposes was done to ensure that family physicians were masked to the PRS (high or low) of attending control group participants, thus minimizing any potential influence on the study participants through counselling or other interventions.
Statistical methods
A p-value < 0.05 was considered statistically significant. The primary analyses followed a per-protocol approach, including only high-PRS participants who consented and completed the intervention as planned at all time points. Continuous baseline variables were described using means and standard deviations and compared by t-tests. In case of a skewed distribution, median and interquartile ranges were presented, categorical variables were expressed as frequencies and relative frequencies, and compared by chi-square tests. Cardiovascular risk factors were compared between the two groups at baseline, 6 months, and 12 months. Outcome assessments for visits 2 and 3 were analysed using ANCOVA, adjusting to baseline values to correct for potential baseline imbalances and to increase the precision. A Wilcoxon rank-sum test was used for 10-year CVD risk comparison. Within-group differences from baseline were assessed using paired t-tests. The number of prescriptions purchased per follow-up year was compared with of a negative-binomial model adjusted to age and sex, IRR (incidence rate ratio), and 95% confidence intervals are presented. The analysis was performed using Stata 14.2 and R (version 2024.12.0 + 467).
Results
Recruitment and participant flow
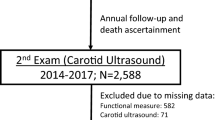
We invited 2864 eligible individuals to participate (Fig. 3) during April 2022- August 2023. Of those, 1286 were excluded (1087 declined to participate, and in 199 cases their GP declined to participate). A total of 1020 participants were randomised into an intervention (n = 510) and a control group (n = 510). The drop-out rate before the first trial visit was 9.0% in the intervention arm and 12.0% in the control arm, resulting in baseline data being analysed for intervention (n = 464) and control group (n = 449) participants. Pregnant individuals at the baseline visit were omitted from the data analysis (n = 20). A higher proportion of younger individuals were lost between randomisation and the first study visit. However, the intervention and control groups remain comparable, with both groups consisting of slightly older participants than those who initially consented to join the trial. The overall dropout rate from randomisation to the last trial visit was 18.2% for the intervention arm and 18.8% for the control arm. The last participant completed follow-up in November 2024.

Participant flowchart. The flowchart presents the analysis for the primary outcome, with secondary outcome analyses involving a varying number of observations. FP family physician.
Baseline data
The baseline characteristics of the high-PRS intervention and control arm participants are presented in Table 1. The mean (SD) age of the study population was 37.7 (5.4) years, and 45.5% were women. The mean BMI was 27.7 (2.2) kg/m2. The study population had low behavioural risk impact, with minimal smoking and moderate alcohol consumption, with over half reporting no or very infrequent consumption, and only 1.8% drinking daily. There were no significant intergroup differences except for smoking status (p = 0.043).
Changes in BMI and cardiovascular risk factors
Regarding BMI, no significant differences were observed between the intervention and control groups at 6 months (p = 0.713) or 12 months (adj. Δ = 0.11 kg/m2, 95% CI = − 0.09 to 0.30, p = 0.291) (Table 2). Waist circumference increased slightly in both groups at the 6-month mark, but by the end of the trial, the difference between the groups was not statistically significant (p = 0.143).
There were no statistically significant differences between groups at 12 months in systolic blood pressure (0.60 mmHg, 95% CI − 1.97 to 0.77, p = 0.393), or other parameters of interest. Systolic blood pressure slightly decreased in both groups throughout the trial, but the change was not statistically significant (intervention group: p = 0.496, control group: p = 0.724).
Baseline 10-year CVD risk calculations differed and were not directly comparable, as the intervention group’s score at baseline included both traditional risk factors and PRS (median 2.1, IQR = 1.1–3.7), while the control group’s score was based only on traditional factors (median 1.8, IQR = 0.9–3.2). At the 12 months visit, the risk scores were calculated for both groups using a combination of traditional risk factors and PRS, making them comparable. The median risk in the intervention group rose to 2.2 (SD = 1.2–3.8) and in the control group to 2.1 (SD = 1.2–3.9) mainly due to the population age increase. No statistically significant differences were observed between the study groups’ combined risk scores at the end of the trial.
Gender- and education-stratified analyses for BMI showed no significant differences between groups. Similarly, BMI analysis in high CVD-risk individuals (Q3) found no significant variation (Table S1). Comparisons between the intervention and low-PRS control arm have been provided in Table S2.
Preventive treatment patterns
Family physicians prescribed anti-hypertensive (C03–C09) or lipid-lowering (C10) medications to 15.5% of participants in the intervention group and 19.2% in the control group (Table 3). The number of prescriptions for these medications was similar across groups, indicating no significant effect of the intervention on medication prescribing behaviour.
In negative-binomial regression models adjusted for age and sex, the incidence rate ratio (IRR) of package purchases in the intervention group compared to the control group was 0.93 (95% CI: 0.73–1.18) for lipid-lowering drugs and 0.97 (95% CI: 0.79–1.21) for anti-hypertensive drugs, indicating no significant effect of the intervention on medication purchasing behaviour.
We also compared the number of prescriptions issued in the first versus last 90 days of follow-up between intervention and control arms using a negative-binomial model with an offset for person-years and found no significant differences between arms.
Self-reported CVD risk factor outcomes
Self-reported smoking behaviour remained largely unchanged over 12 months, with a non-significant 1.9% decline in daily smoking in the intervention arm (McNemar’s χ2 = 0.64, p = 0.40) and a 0.8% decline in controls (χ2 = 0, p = 0.999), and no between-group difference in cigarettes per day (t = − 0.30, p = 0.76). Alcohol consumption saw a modest net increase in abstinence (2.3%), driven by significantly more participants quitting than starting drinking (χ2 = 6.09, p = 0.014), with similar patterns present in both study arms. Physical activity (MET score) between-group differences at 12 months were non-significant (W = 75 974, p = 0.35). Dietary analyses of recommended intake for vegetables and fruit did not reveal between-group differences. A detailed overview of these self-reported outcomes, along with illustrative figures and full statistical results, has been provided in the Supplementary Materials.
Discussion
In this randomised controlled trial of 1020 young overweight individuals, we found no evidence that communicating high CAD polygenic risk would result in behaviour changes sufficient to reduce cardiovascular risk factors over 12 months. However, our findings provide valuable insights that may help inform the development and evaluation of alternative approaches for incorporating polygenic risk into CVD primary prevention.
Knowledge about polygenic risk can help identify individuals at higher relative risk of early CVD31. However, genetic risk may be perceived as predetermined rather than a motivator for behaviour change and in a generally healthy population like ours, with slight overweight, good education, low risk factors, minimal alcohol and tobacco use, and mildly elevated LDL, such information may be less effective in driving further lifestyle improvements47,48,49. Additionally, the young age of our participants may have contributed to limited intervention effectiveness. Older adults demonstrate greater weight loss in lifestyle interventions, motivated by health decline and comorbidity awareness45,50. In contrast, young adults are primarily driven by appearance and social factors rather than long-term health concerns51.
Another consideration is the one-on-one counselling used in this trial, reflecting routine primary care. More frequent contact and alternative delivery methods may be needed to support behaviour change in this age group52,53,54. Studies show that weight loss interventions achieve better long-term results when supported by ongoing personal contact, with recommendations for at least quarterly or preferably monthly visits55,56.
In pragmatic trials, using participants’ own family physicians to deliver interventions has been shown to potentially reduce the impact on behaviour change, as such trials reflect routine care with minimal alteration to usual practice, which can weaken intervention delivery57,58. While we achieved much lower attrition than similar lifestyle RCTs, younger participants typically demonstrate higher dropout rates in weight loss trials, and retention difficulties may have still contributed to the trial being underpowered59,60,61.
In addition, the novelty of polygenic risk — not yet widely adopted in clinical practice or fully covered in medical education until recently — may further complicate its integration into risk communication between physicians and patients62. As a result, many physicians may find it challenging to interpret, even after receiving training on the subject63,64.
Trial participation may increase social desirability, resulting in over-reporting of behaviours, as heightened risk awareness can introduce bias into self-reported outcomes65,66. This may have led to more accurate self-reporting of behavioural risk factors such as smoking prevalence, slightly contributing to the rise in 10-year CVD risk. However, this increase was likely primarily driven by aging during the trial, as age is a major determinant of cardiovascular risk. Assessing how participants perceived their own weight could have been informative, as those viewing themselves as having normal weight may employ smoking as a weight management tool—a consideration particularly relevant given our cohort was only slightly overweight rather than obese67. Although the study population was generally inactive, with average MET scores below 3 (the threshold for health-protective activity), trial participation may have influenced the control group’s increased activity levels, possibly due to their unawareness of polygenic risk or a Hawthorne effect, where behaviour changes simply from being observed68,69,70.
Although no significant difference in prescribing lipid-lowering or blood pressure medications was observed between study arms, the fact that physicians initiated preventive treatment in 25–44-year-olds—who typically would not qualify under current guidelines—represents an important finding. This suggests that participation in the trial increased clinical attention to early cardiovascular risk, even without a PRS-driven effect.
This pragmatic, real-life trial offers valuable insights, yet its one-year duration may not capture long-term behaviour changes that develop gradually or occur outside the structured RCT framework. In this context, a realist evaluation could provide valuable insights, focusing not just on outcomes but on the underlying mechanisms and contextual factors behind the intervention delivery71. This approach may help identify whether adjustments in delivery methods, target populations, or other factors are needed to improve strategies for integrating genetic risk into CVD primary prevention and to evaluate its long-term cost effectiveness72,73.
Our findings indicate that merely knowing one’s polygenic risk for coronary artery disease is not sufficient to drive significant health behaviour change. However, previous research suggests value in equipping primary care professionals with more precise risk assessments, allowing them to proactively initiate preventive treatments such as lipid-lowering or blood pressure medications. This approach may prove more effective than relying solely on individual motivation for lifestyle modifications74.
Strengths and limitations
This is the first clinical trial to test CAD PRS risk communication in a real-life primary care setting with younger individuals. Until now, it was unclear whether young people with high polygenic risk would feel compelled to adopt healthier behaviours, but this randomised trial strongly suggests that risk communication alone, even using novel indicators like PRS, is insufficient to drive short-term behaviour change and likely not enough for long-term change either. This finding highlights the need to further explore and test various primary prevention strategies for high-PRS individuals.
A key limitation of the study was participant drop-out between randomisation and the first study visit, primarily due to a slow randomisation process that delayed family physicians in scheduling appointments. Although the combined risk assessment model underwent extensive pre-implementation testing, we have not published the specific model used in this trial. However, a similar model utilizing the same clinical parameters with an updated PRS has recently been published75. Challenges in risk communication may have impacted the intervention’s effectiveness, as family physicians had to navigate both new software and the relatively recent concept of polygenic risk when explaining cardiovascular risk to patients.
Conclusion
This trial showed that communicating high CAD PRS alone is not enough to prompt meaningful behaviour change in a young population. Our results highlight that polygenic risk behaves like any other cardiovascular risk factor and should be considered within the broader context of an individual’s overall risk profile.
Data availability
The data underlying this study protocol will be shared upon reasonable request to the investigators (A.P or M.J).
References
Kelly, M. P. & Barker, M. Why is changing health-related behaviour so difficult? Public. Health. 136, 109–116. https://doi.org/10.1016/j.puhe.2016.03.030 (2016).
Wallander, J. L., Fradkin, C. & Scott, S. M. Issues in Adolescent Adherence and Health-Behavior Change (Oxford University Press, 2013). https://doi.org/10.1093/oxfordhb/9780199795833.013.008.
Michie, S., West, R., Sheals, K. & Godinho, C. A. Evaluating the effectiveness of behavior change techniques in health-related behavior: a scoping review of methods used. Transl. Behav. Med. 8 (2), 212–224. https://doi.org/10.1093/tbm/ibx019 (2018).
Mensah, G. A. et al. Global Burden of cardiovascular diseases and risks, 1990–2022. J. Am. Coll. Cardiol. 82 (25), 2350–2473. https://doi.org/10.1016/j.jacc.2023.11.007 (2023).
Timmis, A. et al. European Society of Cardiology: the 2023 Atlas of Cardiovascular Disease Statistics. Eur. Heart J. 45(38), 4019–4062. https://doi.org/10.1093/eurheartj/ehae466 (2024).
Viigimaa, M. et al. Effectiveness and feasibility of cardiovascular disease personalized prevention on high polygenic risk score subjects: a randomized controlled pilot study. Eur. Heart J. Open. https://doi.org/10.1093/ehjopen/oeac079 (2022).
Phyo, A. Z. Z. et al. Health-related quality of life and incident cardiovascular disease events in community-dwelling older people: A prospective cohort study. Int. J. Cardiol. 339, 170–178. https://doi.org/10.1016/j.ijcard.2021.07.004 (2021).
Nieminen, M. S. et al. The patient perspective: quality of life in advanced heart failure with frequent hospitalisations. Int. J. Cardiol. 191, 256–264. https://doi.org/10.1016/j.ijcard.2015.04.235 (2015).
Luengo-Fernandez, R. et al. Economic burden of cardiovascular diseases in the European Union: a population-based cost study. Eur. Heart J. 44 (45), 4752–4767. https://doi.org/10.1093/eurheartj/ehad583 (2023).
Lui, J. N. M. et al. Impact of new cardiovascular events on quality of life and hospital costs in people with cardiovascular disease in the united Kingdom and united States. JAHA 12 (19), e030766. https://doi.org/10.1161/JAHA.123.030766 (2023).
Becker, M. H. The health belief model and personal health behavior. Health Educ. Monogr. 2, 324–473 (1974).
Prochaska, J. O. & Velicer, W. F. The transtheoretical model of health behavior change. Am. J. Health Promot. 12 (1), 38–48. https://doi.org/10.4278/0890-1171-12.1.38 (Sept. 1997).
Ajzen, I. The theory of planned behavior, Org. Behav. Hum. Decis. Processes 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-T (1991).
Bakhit, M. et al. Cardiovascular disease risk communication and prevention: A meta-analysis. Eur. Heart J. 45(12), 998–1013. https://doi.org/10.1093/eurheartj/ehae002 (2024).
Sharma, M. Theoretical Foundations of Health Education and Health Promotion (Jones & Bartlett Learning, 2021).
Khani Jeihooni, A. et al. The application of the theory of planned behavior to nutritional behaviors related to cardiovascular disease among the women. BMC Cardiovasc. Disord. 21(1), 589. https://doi.org/10.1186/s12872-021-02399-3 (2021).
Ignarro, L. J., Balestrieri, M. L. & Napoli, C. Nutrition, physical activity, and cardiovascular disease: an update. Cardiovascular. Res. 73 (2), 326–340 (2007).
Makin, H., Chisholm, A., Fallon, V. & Goodwin, L. Use of motivational interviewing in behavioural interventions among adults with obesity: A systematic review and meta-analysis. Clin. Obes. 11 (4), e12457. https://doi.org/10.1111/cob.12457 (2021).
Jeemon, P. et al. Efficacy of a family-based cardiovascular risk reduction intervention in individuals with a family history of premature coronary heart disease in India (PROLIFIC): an open-label, single-centre, cluster randomised controlled trial. Lancet Global Health. 9 (10), e1442–e1450. https://doi.org/10.1016/S2214-109X(21)00319-3 (Oct. 2021).
Elias, S. et al. Shared Decision-Making in cardiovascular risk factor management: A systematic review and Meta-Analysis. JAMA Netw. Open. 7 (3), e243779. https://doi.org/10.1001/jamanetworkopen.2024.3779 (2024).
Wienke, A., Holm, N. V., Skytthe, A. & Yashin, A. I. The heritability of mortality due to heart diseases: a correlated frailty model applied to Danish twins. Twin Res. 4(4), 266–274. https://doi.org/10.1375/1369052012399 (2001).
Zdravkovic, S. et al. Heritability of death from coronary heart disease: a 36-year follow‐up of 20 966 Swedish twins. J. Internal Med. 252(3), 247–254. https://doi.org/10.1046/j.1365-2796.2002.01029.x (2002).
Aragam, K. G. et al. Discovery and systematic characterization of risk variants and genes for coronary artery disease in over a million participants. Nat. Genet. 54(12), 1803–1815. https://doi.org/10.1038/s41588-022-01233-6 (2022).
Rocheleau, G. et al. Rare variant contribution to the heritability of coronary artery disease. Nat. Commun. 15 (1), 8741. https://doi.org/10.1038/s41467-024-52939-6 (2024).
Ali Torkamani, A. et al. The personal and clinical utility of polygenic risk scores. Nat. Rev. Genet. 19(9), 581–590. https://doi.org/10.1038/s41576-018-0018-x (2018).
Fahed, A. & Natarajan, P. Clinical applications of polygenic risk score for coronary artery disease through the life course. Atherosclerosis 117356–117356. https://doi.org/10.1016/j.atherosclerosis.2023.117356 (2023).
Sabatello, M. et al. Return of polygenic risk scores in research: stakeholders’ views on the eMERGE-IV study. Hum. Genet. Genomics Adv. 5 (2). https://doi.org/10.1016/j.xhgg.2024.100281 (2024).
Said, M. A., Verweij, N. & Van Der Harst, P. Associations of combined genetic and lifestyle risks with incident cardiovascular disease and diabetes in the UK biobank study. JAMA Cardiol. 3 (8), 693. https://doi.org/10.1001/jamacardio.2018.1717 (2018).
Sutoh, Y. et al. Healthy lifestyle practice correlates with decreased obesity prevalence in individuals with high polygenic risk: TMM CommCohort study. J Hum. Genet Aug. https://doi.org/10.1038/s10038-024-01280-3 (2024).
Widén, E. et al. How communicating polygenic and clinical risk for atherosclerotic cardiovascular disease impacts health behavior: an observational Follow-up study. Circ: Genomic Precision Med. 15 (2). https://doi.org/10.1161/CIRCGEN.121.003459 (2022).
Khera, A. V. et al. Genetic Risk, adherence to a healthy Lifestyle, and coronary disease. N Engl. J. Med. 375, 2349–2358. https://doi.org/10.1056/NEJMoa1605086 (2016).
Iribarren, C. et al. Interplay between lifestyle factors and polygenic risk for incident coronary heart disease in a large multiethnic cohort. Int. J. Cardiol. Cardiovasc. Risk Prev. 23, 200350. https://doi.org/10.1016/j.ijcrp.2024.200350 (2024).
Iribarren, C., Lu, M., Elosua, R. & Rana, J. Utility of a polygenic risk score for incident CHD: interplay with lifestyle in a multi-ethnic cohort of more than 60,000 individuals. Eur. Heart J. 44(Supplement_2), ehad655-2448 (2023).
Muse, E. D. et al. Impact of polygenic risk communication: an observational mobile application-based coronary artery disease study. Npj Digit. Med. 5(1), 30. https://doi.org/10.1038/s41746-022-00578-w (2022).
Schunkert, H. et al. Clinical utility and implementation of polygenic risk scores for predicting cardiovascular disease. Eur. Heart J. 649, ehae. https://doi.org/10.1093/eurheartj/ehae649 (2025).
The China Kadoorie Biobank Collaborative Group. Joint impact of polygenic risk score and lifestyles on early- and late-onset cardiovascular diseases. Nat. Hum. Behav. 8 (9), 1810–1818. https://doi.org/10.1038/s41562-024-01923-7 (2024).
McBride, C. M., Koehly, L. M., Sanderson, S. C. & Kaphingst, K. A. The behavioral response to personalized genetic information: will genetic risk profiles motivate individuals and families to choose more healthful behaviors? Annu. Rev. Public Health 31(1), 89–103. https://doi.org/10.1146/annurev.publhealth.012809.103532 (2010).
Lewis, A. C. F. et al. Patient and provider perspectives on polygenic risk scores: implications for clinical reporting and utilization. Genome Med. 14 (1), 114. https://doi.org/10.1186/s13073-022-01117-8 (2022).
Ford, I., Norrie, J. & Trials, P. N Engl. J. Med., 375, 5, 454–463. https://doi.org/10.1056/NEJMra1510059 (2016).
Inouye, M. et al. Genomic risk prediction of coronary artery disease in 480,000 adults: implications for primary prevention. J. Am. Coll. Cardiol. 72 (16), 1883–1893. https://doi.org/10.1016/j.jacc.2018.07.079 (2018).
Institute of Computer Science, University of & Tartu Combined ischaemic heart disease risk calculator. [Online]. Available: https://prs-cad2022v1.dev.gi.ut.ee/ (2022).
SCORE2 working group and ESC Cardiovascular risk collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 42 (25), 2439–2454. https://doi.org/10.1093/eurheartj/ehab309 (2021).
Harris, P. A. et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 95, 103208. https://doi.org/10.1016/j.jbi.2019.103208 (2019).
Wendel-Vos, G. W., Schuit, A. J., Saris, W. H. & Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 56 (12), 1163–1169 (2003).
Svetkey, L. P. et al. Cell phone intervention for you (CITY): A randomized, controlled trial of behavioral weight loss intervention for young adults using mobile technology. Obesity (Silver Spring) 23(11), 2133–2141. https://doi.org/10.1002/oby.21226 (2015).
Rotunda, W. et al. Weight loss in short-term interventions for physical activity and nutrition among adults with overweight or obesity: a systematic review and meta-analysis. Prev. Chronic Dis. 21, 230347. https://doi.org/10.5888/pcd21.230347 (2024).
Hardcastle, S. J. et al. Motivating the unmotivated: how can health behavior be changed in those unwilling to change? Front. Psychol. 6 https://doi.org/10.3389/fpsyg.2015.00835 (2015).
VanBuskirk, K. A. & Wetherell, J. L. Motivational interviewing with primary care populations: a systematic review and meta-analysis. J. Behav. Med. 37 (4), 768–780. https://doi.org/10.1007/s10865-013-9527-4 (2014).
Morton, K. et al. The effectiveness of motivational interviewing for health behaviour change in primary care settings: a systematic review. Health Psychol. Rev. 9 (2), 205–223. https://doi.org/10.1080/17437199.2014.882006 (2015).
DeLuca, L., Toro-Ramos, T., Michaelides, A., Seng, E. & Swencionis, C. Relationship between age and weight loss in noom: Quasi-Experimental study. JMIR Diabetes. 5 (2), e18363. https://doi.org/10.2196/18363 (2020).
LaRose, J. G., Leahey, T. M., Hill, J. O. & Wing, R. R. Differences in motivations and weight loss behaviors in young adults and older adults in the national weight control registry. Obesity 21(3), 449–453. https://doi.org/10.1002/oby.20053 (2013).
Tronieri, J. S., Wadden, T. A., Chao, A. M. & Tsai, A. G. Primary care interventions for obesity: review of the evidence. Curr. Obes. Rep. 8 (2), 128–136. https://doi.org/10.1007/s13679-019-00341-5 (2019).
Laddu, D. et al. Health behavior change programs in primary care and community practices for cardiovascular disease prevention and risk factor management among midlife and older adults: A scientific statement from the American heart association. Circulation 144 (24). https://doi.org/10.1161/CIR.0000000000001026 (2021).
McGuire, H. L. et al. Comprehensive lifestyle modification and blood pressure control: a review of the PREMIER trial. J. Clin. Hypertens. (Greenwich). 6 (7), 383–390. https://doi.org/10.1111/j.1524-6175.2004.03147.x (2004).
Wadden, T. A. et al. A two-year randomized trial of obesity treatment in primary care practice. N. Engl. J. Med. 365(21), 1969–1979. https://doi.org/10.1056/NEJMoa1109220 (2011).
Svetkey, L. P. Comparison of strategies for sustaining weight lossthe weight loss maintenance randomized controlled trial. JAMA 299 (10), 1139. https://doi.org/10.1001/jama.299.10.1139 (2008).
Kanzler, K. E. et al. Conducting a pragmatic trial in integrated primary care: key decision points and considerations. J. Clin. Psychol. Med. Settings. 29 (1), 185–194. https://doi.org/10.1007/s10880-021-09790-4 (2022).
Oude Rengerink, K. et al. Series: pragmatic trials and real world evidence: paper 3. Patient selection challenges and consequences. J. Clin. Epidemiol. 89, 173–180. https://doi.org/10.1016/j.jclinepi.2016.12.021 (2017).
Bouzalmate Hajjaj, A., Massó Guijarro, P., Khan, K. S., Bueno-Cavanillas, A. & Cano-Ibáñez, N. A systematic review and meta-analysis of weight loss in control group participants of lifestyle randomized trials. Sci. Rep. 12 (1), 12252. https://doi.org/10.1038/s41598-022-15770-x (2022).
Rogers, M., Lemstra, M., Bird, Y., Nwankwo, C. & Moraros, J. Weight-loss intervention adherence and factors promoting adherence: a meta-analysis. PPA 10, 1547–1559. https://doi.org/10.2147/PPA.S103649 (2016).
Moroshko, I., Brennan, L. & O’Brien, P. Predictors of dropout in weight loss interventions: a systematic review of the literature. Obes. Rev. 12 (11), 912–934. https://doi.org/10.1111/j.1467-789X.2011.00915.x (2011).
Yanes, T. et al. Development and evaluation of a novel educational program for providers on the use of polygenic risk scores. Genet. Med. 25(8), 100876. https://doi.org/10.1016/j.gim.2023.100876 (2023).
Lewis, C. M. & Vassos, E. Polygenic risk scores: from research tools to clinical instruments. Genome Med. 12(1), 44. https://doi.org/10.1186/s13073-020-00742-5 (2020).
Rosenberg, N. A., Edge, M. D., Pritchard, J. K. & Feldman, M. W. Interpreting polygenic scores, polygenic adaptation, and human phenotypic differences. Evol. Med. Public. Health. 2019 (1), 26–34. https://doi.org/10.1093/emph/eoy036 (2019).
Scheuermann, T. S. et al. Accuracy of self-reported smoking abstinence in clinical trials of hospital-initiated smoking interventions. Addiction 112(12), 2227–2236. https://doi.org/10.1111/add.13913 (2017).
Ravelli, M. N. & Schoeller, D. A. Traditional Self-Reported dietary instruments are prone to inaccuracies and new approaches are needed. Front. Nutr. 7, 90. https://doi.org/10.3389/fnut.2020.00090 (2020).
Coa, K. I., Augustson, E. & Kaufman, A. The impact of weight and weight-related perceptions on smoking status among young adults in a text-messaging cessation program. Nicotine Tob. Res. 20 (5), 614–619. https://doi.org/10.1093/ntr/ntx053 (2018).
WHO Guidelines on Physical Activity and Sedentary Behaviour, 1st ed. Geneva: World Health Organization, (2020).
Byrne, N. M., Hills, A. P., Hunter, G. R., Weinsier, R. L. & Schutz, Y. Metabolic equivalent: one size does not fit all. J. Appl. Physiol. vol. 99 (3), 1112–1119. https://doi.org/10.1152/japplphysiol.00023.2004 (2005).
Parsons, H. M. What happened at Hawthorne? New evidence suggests the Hawthorne effect resulted from operant reinforcement contingencies. Science 183 (4128), 922–932 https://doi.org/10.1126/science.183.4128.922 (1974).
Driver, M. N., Kuo, S. I. C. & Dick, D. M. Returning complex genetic risk information to promote better health-related behaviors: a commentary of the literature and suggested next steps. Transl. Behav. Med. 13 (2), 115–119 (2023). https://doi.org/10.1093/tbm/ibac071
Hesketh, K. D. et al. Long-term outcomes (2 and 3.5 years post-intervention) of the INFANT early childhood intervention to improve health behaviors and reduce obesity: cluster randomised controlled trial follow-up. Int. J. Behav. Nutr. Phys. Act 17(1), 95. https://doi.org/10.1186/s12966-020-00994-9 (2020).
Mustonen, E. et al. Eight-year post‐trial follow‐up of health care and long‐term care costs of tele‐based health coaching. Health Serv. Res. 55(2), 211–217. https://doi.org/10.1111/1475-6773.13251 (2020).
Ebrahim, S., Beswick, A., Burke, M. & Davey Smith, G. Multiple risk factor interventions for primary prevention of coronary heart disease, in Cochrane Database of Systematic Reviews, The Cochrane Collaboration, Ed., Chichester, UK: John Wiley & Sons, Ltd, p. CD001561.pub2. https://doi.org/10.1002/14651858.CD001561.pub2 (2006).
Puusepp, T. et al. Development and validation of a risk prediction algorithm for high-risk populations combining genetic and conventional risk factors of cardiovascular disease. PLoS One. 20 (10), e0335064. https://doi.org/10.1371/journal.pone.0335064 (2025).
World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA 310 (20), 2191. https://doi.org/10.1001/jama.2013.281053 (2013).
Acknowledgements
We would like to thank the large team involved in making this trial possible—the family physicians who facilitated the study visits, the IT team of the University of Tartu Institute of Genomics and the dedicated study support staff ensuring the implementation of the trial.
Funding
This project was done as part of the INTERVENE EU Horizon project (www.interveneproject.eu) and received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 101016775.
The work of AE was supported by Estonian Research Council (grant PRG2078). The work of MV was supported by the Estonian Research Council (grant PRG2629).
Author information
Authors and Affiliations
Contributions
Design and conception: M.J., H.A., A.E., M.V., K.P. Data analysis: K.T., A.P. Writing of the manuscript: A.P, K.T. Review of the manuscript: M.J., A.E., M.V., A.I., L.C.N., K.F., L.M., H.A., J.A., K.P., T.T., R.K., E.W., S.R. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the principles of the Declaration of Helsinki76. Participation in the clinical trial was voluntary, informed consent was obtained from all individual participants included in the study. Ethical approval was granted by the Estonian Bioethics and Human Research Council (No. 1.1–12/1726, 17.08.2021), the trial registration number on ClinicalTrials.gov: NCT05603663.
Consent for publication
Not applicable, as this trial does not include any details, images, or videos relating to individual participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Põld, A., Toompere, K., Elken, A. et al. Evaluating the impact of communicating high polygenic risk for coronary artery disease on the health behaviour of young overweight adults: a pragmatic randomised controlled trial. Sci Rep 16, 4907 (2026). https://doi.org/10.1038/s41598-026-35027-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-35027-1
