
Abstract
Patient-Reported Outcome Measures (PROMs) are integral tools that capture real-time insights into patients’ experiences. Little is known about barriers and facilitators to PROMs implementation in the Asian context. This study explores the barriers, facilitators, and strategies for implementing PROMs from both patient and provider perspectives. We interviewed 33 patients and 27 healthcare providers from Singapore General Hospital and National University Hospital. Data were analyzed using the Consolidated Framework for Implementation Research (CFIR). The CFIR-Expert Recommendations for Implementing Change (ERIC) matching tool was utilized to match implementation strategies to the identified barriers. All five domains of the CFIR framework were elicited. Facilitators included (1) Improvement in patient-healthcare provider communication, (2) Guidance relating to clinical judgement, (3) Patient empowerment, and (4) Clinician endorsement. Barriers included 1) Lack of local adaptation, (2) Cultural concerns, (3) Lack of coordinated effort, (4) Lack of formal training and (5) Disengaged healthcare workers). In total, 48 ERIC strategies were matched to the corresponding CFIR barriers. Implementing successful and sustainable PROMs requires a multifaceted approach that addresses identified barriers while strategically leveraging facilitators. Future efforts should emphasize PROMs’ value to patients and tailor strategies for diverse populations.
Similar content being viewed by others


Introduction
Patient-Centered and Value Based Care is an approach that prioritizes patients’ preferences and values in the delivery of medical care and emphasizes shared decision-making1. This multidisciplinary model allows for personalising treatment regimens in accordance to patients’ preferences and needs, as opposed to the traditional paternalistic model where treatment decisions often lie on clinicians alone without factoring the patient’s explicit agreement2.
Studies show that clinicians typically underestimate the disease severity and burden, especially for subjective and non-visible aspects such as fatigue, emotional health, and functional impairment3,4. Such discrepancies may weaken the patient-physician relationship, reduce treatment adherence, and lower patient satisfaction5. At the systemic level, failing to properly identify patient-reported symptoms may also lead to inappropriate healthcare utilization, placing avoidable strain on healthcare resources6. PROMs offer one structured way to integrate patient experiences into clinical decision-making and facilitate a move toward value-based care. Healthcare systems are thus increasingly prioritizing the deployment and use of Patient-Reported Outcome Measures (PROMs) such as EuroQol 5Dimensionals7 and 36-Item Short Form Health Survey8 to capture meaningful, real-time insights into patients’ health experiences. These self-completed validated questionnaires obtain patients’ subjective evaluations of their own health, functional status and overall health-related quality of life in relation to their diagnosed medical condition and the treatment they have received9, providing a more comprehensive evaluation of disease burden10.
Despite the well-documented benefits of using PROMS, their routine usage remains limited11,12. This challenge reflects a broader trend across medicine, where only 20% of evidence-based practices reach routine implementation, and the average time to translate research into clinical practice is approximately 17 years13,14.Implementation science is crucial in addressing these gaps by identifying barriers to adoption and developing key strategies that will ultimately accelerate the implementation of PROMs. While there has been literature on the facilitators and barriers to PROMs implementation in some specialty fields such as oncology15 and orthopaedics16, notably none of the studies included were from Asia. Hence, it is especially pertinent to explore the facilitators and barriers to PROMs implementation through an Asian context and across different specialty fields.
The Consolidated Framework for Implementation Research (CFIR) is a theoretical framework commonly used in implementation science. It consists of five major domains (innovation, outer setting, inner setting, individuals, and implementation process)17. The CFIR-Expert Recommendations for Implementing Change (ERIC)18 matching tool, a compilation of 73 implementation strategies18 was then used to identify ERIC strategies to overcome the identified CFIR barriers19. This is the first study that aims to explore the facilitators and barriers to PROMs implementation from patient and provider perspectives using the CFIR framework20.
Materials and methods
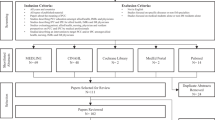
This qualitative study recruited patients and healthcare providers from Singapore General Hospital (SGH) and National University Hospital (NUH), which are the anchor hospitals of the two largest academic medical centers in Singapore. Inclusion criteria for patients included being aged 21 and above, cognitively intact and able to communicate in English or Mandarin, and receiving care within SGH and NUH. Inclusion criteria for healthcare providers included doctors, nurses, or other providers employed within SGH and NUH. Potential participants were approached by a research staff member who explained the purpose of the study. Both patients and healthcare providers were purposively sampled based on gender, age, ethnicity, and medical discipline. The objectives and methods of the study were explained to all participants, and PROM-naïve participants received a short briefing on the purpose and process of PROMs prior to the interviews. The study was approved by the National Healthcare Group’s Domain Specific Review Board (Ref No. 2023/00698) and SingHealth Centralised Institutional Review Board (Ref No. 2023-2182). The study was conducted in compliance with the principles of the 1964 Declaration of Helsinki. Informed consent was obtained from all participants prior to their involvement in the study.
Semi-structured interviews were conducted in English, in person, or virtually over Zoom by interviewers trained in qualitative interviews (CYS, DJY, NQBIL, EC, TP, BC, and CXR). Field notes were taken, and the interviews were audio-recorded and transcribed, verbatim. Interviews conducted in Mandarin were translated and transcribed in English. Informed consent was obtained, and the participants were reimbursed for their time. Data saturation was reached with 25 healthcare providers and 31 patients, determined by group consensus that no new themes were emerging in the most recent round of iterative coding.
Interviews with healthcare providers focused on barriers to the integration of PROMs into clinical care, facilitators for improving patient uptake, and gaps in clinical practice that PROMs could fill. Interviews with patients focused on their previous experiences with PROMs, perceived benefits, barriers, and facilitators (Supplementary Fig. 1). The interview guide was adapted from the CFIR interview guide tool21. The study team had multiple rounds of discussion, and we collectively identified the interview questions that were most appropriate for our objectives of understanding the facilitators and barriers of PROMs implementation in our local context.
Data analysis was conducted using NVivo 14.23.4 and ATLAS.ti V.8.0.19. Thematic coding was independently performed by at least two coders (CYS, DJY, NQBIL, EC, TP, BC, WTH, KYH, and CXR) and reviewed to ensure agreement. Similar codes were grouped together and organized into the constructs under five domains of the CFIR framework22. The CFIR constructs were adopted as the coding template, and the 67 CFIR constructs and subconstructs were identified as a priori codes for an initial codebook23,24. During coding, we continuously refined the codebook through ongoing analysis and discussions. This iterative process enabled us to reach a consensus with credibility and rigour on the constructs and subconstructs and generate the finalized codebook. The interview guide was updated in each round to reflect new learning and avenues for further probing before further participants were recruited through theoretical sampling. Codings were iteratively checked and updated, and reflexivity was emphasized through documentation of perspectives and reflections. The study was reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Supplementary Table 1)25.
The CFIR-ERIC matching tool was utilized to develop and outline the expert-endorsed Level 1 and 2 strategies. The identified CFIR barriers were input into the CFIR–ERIC matching tool. The tool’s algorithm is derived from an expert consensus panel that ranked how well different implementation strategies address specific CFIR barriers. It then generates a prioritised list of strategies by aggregating the importance ratings assigned by experts across the selected domains18,19. In the development of the CFIR-ERIC matching tool, experts were invited to endorse their top seven strategies for overcoming a specific CFIR barrier18. Level 1 strategies and Level 2 strategies were endorsed by more than 50% of experts, and between 20 and 50% of experts respectively. The CFIR-ERIC output was then analyzed to determine suitable implementation strategies to overcome the main barriers identified. The themes that were discovered in our study to be related to the Asian context were also presented.
Results
A total of 33 patients and 27 healthcare providers were recruited between December 2023 and August 2025. (Table 1).
Facilitators to PROMs implementation mapped to the CFIR construct
To focus on the most salient findings, we organized the analysis and present the results around four key facilitators (Table 2). The additional facilitators were reported in Supplementary Table 2.
Relative advantage
Some patients perceived PROMs to have positively impacted their communication with their doctors. A few patients mentioned that PROMs can serve as a reminder for doctors to bring up symptoms that the patient forgets and the doctor can better “understand where I am.” (Table 2).
Healthcare providers mentioned that PROMs are critical in guiding their clinical judgment. PROMs are especially significant in disease areas where the use of PROMs is mandated, and doctors are required to assess disease activity with PROMs.
Individual—innovation recipients
Both patients and healthcare providers agreed that PROMs allowed patients to feel empowered to make decisions about their care and raised their self-awareness of their health conditions. Patients mentioned that “because it helps me to assess my own condition … I think I like it this way.” Patients appreciated the opportunity to “understand their conditions” better through PROMs. (Table 2).
Engaging—innovation recipients
Some patients reported that healthcare providers, particularly doctors, played a central role in their uptake of new interventions. As one patient noted, “I think doctors are the most influential here…” highlighting the importance of clinician endorsement in engaging and encouraging patients to adopt PROMs. (Table 2).
Barriers to PROMs implementation mapped to the CFIR constructs
Findings were consolidated into five barriers (Table 3), alongside Level 1 or highest level 2 recommended ERIC strategies to improve implementation. The additional barriers were reported in Supplementary Table 2.
Innovation (design)
A key limitation raised in the design of PROMs was the lack of adaptation to the local context. As one participant pointed out, “most of them are developed in Europe or North America … when we ask about activities such as skiing, it doesn’t make sense to people in Singapore.” (Table 3).
Recommended ERIC strategies
No Level 1 ERIC strategies were recommended for the CFIR barrier of innovation design. The most expert-recommended ERIC strategy was promoting adaptability at 48%, which fell short of the 50% threshold necessary to classify it as a Level 1 strategy.
Outer setting (local conditions)
Most patients expressed apprehension towards utilizing digital PROMs due to concerns over potential scams. In addition, patients were concerned that some would encounter language barriers when answering the PROMs if they were administered only in English. The patients mentioned that the PROMs may be challenging for those “not very strong in language, for example, dialect speakers.”
Healthcare providers also reported a lack of concerted efforts from institutions. They were unsure how to operationalize the implementation of PROMs “that’s acceptable under very unclear regulations.” (Table 3) They were concerned that the current systems used for PROMs implementation were not integrated and therefore posed a challenge when utilizing PROMs across different systems.
Recommended ERIC strategies
There were no Level 1 ERIC strategies recommended for this domain.
Inner setting (access to knowledge and information)
Healthcare providers were concerned that they had not been formally trained to administer PROMs. They were not fully aware of the purpose of PROMs and found it difficult to answer patients’ questions. Additionally, they found it hard “to keep track of who should be given the questionnaire.” (Table 3).
Recommended ERIC strategies
The Level 1 ERIC strategies recommended to mitigate the barrier access to Knowledge and Information were to conduct educational meetings (79%), develop (59%) and distribute (55%) educational materials.
Implementation process (engaging-innovation deliverer)
Healthcare providers raised concerns that time pressure and throughput-driven key performance indicators (KPIs) were barriers to PROMs implementation. They pointed out that consultation times are lengthened after the PROMs were utilized and it “easily exceed half an hour because there’s so much more to do.” (Table 3) This was an especially important barrier as the performance of healthcare providers was dependent “on the number of patients they see” (Table 3), which would be reduced if the consultation time lengthens. Hence, healthcare providers were worried that their performance will be negatively affected by the implementation of PROMs.
Recommended ERIC strategies
The Level 1 ERIC strategy recommended to mitigate the barrier of engaging—innovation deliverer is to identify and prepare champions (63%).
Implementation strategies
In this context, the implementation strategies outlined in the Expert Recommendations for ERIC18 could provide actionable pathways to overcome these barriers and enhance the adoption and sustainability of PROMs in clinical practice. The CFIR-ERIC matching tool produced a total of 48 Level 1 and Level 2 strategies (Table 4). There were 12 Level 1 strategies, which had an expert agreement of more than 50%. All Level 1 ERIC strategies cut across all three barriers of innovation design, access to knowledge & information and engaging—innovation deliverers. All Level 1 ERIC strategies focused on sharing information, highlighting the importance of key stakeholders in the PROMs implementation process.
Themes relating to the Asian context
Some patients expressed a fear of stigmatization regarding sensitive health issues and a concern for mishandling or leakage of personal data. In particular, patients are uncomfortable with “not know[ing] who is accessing [their] photos or information”, as well as potential sensitive questions such as “[have you ever tried] try to commit suicide”. A few patients express an inclination towards trusting doctors with the decision-making role instead of placing themselves in that role. A few patients mentioned that they will “trust that the doctor will know what to do with [the PROMs they have filled up]”. Healthcare providers have mentioned that “allowing [patient’s] caregivers or their next-of-kin to help them with the online submission” may support patients who require help with PROMs completion. (Supplementary Table 2).
Discussion
In this study, we sought to identify and better understand the facilitators and barriers to PROMs implementation using the CFIR-ERIC framework. Facilitators included (1) Improvement in patient-healthcare provider communication, (2) Guidance of clinical judgement, (3) Patient empowerment, (4) Clinician endorsement. Barriers included (1) Lack of local adaptation, (2) Cultural concerns, (3) Lack of coordinated effort, (4) Lack of formal training (5) Disengagement in clinicians). While the challenges to PROMs implementation present similar findings to other international studies, there are some findings unique to the Asian context.
A key barrier found in our study was the lack of adaptation of PROMs developed overseas to the local context, and language of administration barriers. This aligns with previous research on PROMs validation in Asia which has shown that social functioning is conceptualised differently in Asia compared to the West26, where majority of PROMs are developed. Therefore, cross-cultural adaptation is especially important in the Asian context to ensure the understandability of PROMs for locals27. The suggested ERIC strategy “promote adaptability” in this context would mean cross-culturally adapting PROMs that were developed overseas. Participants expressed the importance of supporting patients who are not proficient in English and face challenges in completing PROMs independently. Additionally, there are IT barriers to the implementation of PROMs from both patient and healthcare provider perspectives. The prevalence of unwanted marketers and scammers in today’s digital environment, coupled with growing skepticism towards digital applications and processes, poses a significant barrier to the implementation of PROMs. Although no specific ERIC strategies address the “local conditions” CFIR barrier, we propose incorporating PROMs into existing IT solutions. An example would be utilizing whitelisted sites or existing pre-consultation SMS links and chatbots as a platform to administer PROMs. This approach could address the growing skepticism towards potential scams, as patients would be familiar with these platforms.
There is a perceived lack of institutional-wide efforts to implement PROMs. Some of the challenges raised by healthcare providers were a lack of training, standardized workflows, outcome-focused KPIs, and a well-integrated IT system that connects PROMs to existing clinical systems. These are common barriers faced by healthcare providers28,29. These challenges are not unique to Asia30,31, and such operational barriers and infrastructural gaps impede the implementation of PROMs. The ERIC strategies recommend sharing information through educational meetings, educational materials, learning collaborative educational outreach visit. Additionally, the ERIC strategies also concentrate on engaging local shareholders by capturing and sharing local knowledge, conducting local consensus discussions, and informing local leaders. In the local context, this means conducting outreach meetings and engaging key shareholders at the micro, meso, and macro levels. An example would be for institutions to create strategic workgroups that comprise of relevant stakeholders (e.g. physicians, nurses, healthcare administrators, IT experts, etc.) to explore the implementation of PROMs holistically across the institutions.
Nevertheless, some healthcare providers persist in the use of PROMs despite these challenges. A main facilitator is the role of PROMs in guiding clinical judgement. In some disease areas such as rheumatoid arthritis and heart failure, PROMs such as Disease Activity Score-28 (DAS28) and Kansas City Cardiomyopathy Questionnaire respectively are integrated in the disease management and drug reimbursement guidelines32,33. An example would be the use of DAS28 in the National Institute for Health and Care Excellence guidelines for the management of rheumatoid arthritis34.
Our findings of facilitators from the patient perspective such as patient empowerment, improvement in patient-healthcare provider communication, and clinician endorsement are congruent with other studies evaluating the barriers and facilitators of PROMs. A review by Hansen et al. support our findings, whereby the implementation of PROMs is dependent on the quality of patient-provider relationships, fostering essential conversations that empower patients to voice their therapeutic needs32.
In addition to the facilitators and barriers mentioned, there is a need to highlight the themes discovered in our study relevant to the Asian context. While IT barriers were identified above, special emphasis should be placed on these barriers as they are especially salient in the Asian context. Compared to Western countries, countries in Asia have comparatively wider disparity in digital literacy35. PROMs implementation across Asia should take into consideration the local digital literacy rate to assess If implementation of digital PROMs is suitable. Additionally, patients are concerned with the leakage of personal data, especially since there is a perceived stigma related to health. This aligns with previous studies showing that there is a greater stigma in Asia related to health conditions36,37,38. As there is an increasing push towards digitalisation of PROMs, there have also been concerns regarding the handling of sensitive health information. A few patients may not readily respond or truthfully to PROMs related to sensitive health information in fear of data leakage and stigmatization. The relationship between patients and healthcare providers differ between Asian and Western countries. Our findings in this study are that some patients express a preference for a doctor-driven approach which Is congruent with studies that evaluate patient-healthcare provider relationship in Asia. A qualitative study by Lee et al. found that patients were confused or surprised when they were put in the decision-making role instead of healthcare providers39. The shift away from a paternalistic approach towards shared decision making will require targeted efforts to empower and educate patients. The approach towards health management in Asia is not individualistic, but is instead a collective one that involves the family as a whole40. Hence, PROMs implementation could be facilitated through the support of family members with helping patients not proficient with digital technologies or the language of administration.
Strengths and limitations
The strengths of the study include the use of the CFIR-ERIC framework, which provides a robust structure for the development of real-world actionable strategies, as it provides a template to organize research findings. Having clear and well-defined facilitators and barriers allows for the building of knowledge for PROMs implementation24. The inclusion of a wide range of perspectives, including the diverse demographics of our patient population as well as different stakeholder roles amongst our healthcare providers, enhanced the internal validity of these findings. Moreover, insights might also be transferable to comparable institutions, given operational and cultural similarities.
One limitation is that a quantitative score of intercoder reliability (ICR) was not calculated for this study. An assessment of ICR may have improved the systematicity and transparency of the coding process. However, we adopted a qualitative-based measure of intercoder reliability that is compatible with the interpretivist paradigm of qualitative research41. Another limitation of this study was that only participants from tertiary hospitals were included. Patients and healthcare providers from community or secondary hospitals were not included. They might have a different perspective on the implementation of PROMs due to differing demographics and workflow. Future studies should include participants from community and secondary hospitals to capture a more holistic view of PROMs implementation. Furthermore, not all medical and surgical specialties were captured in the sampling of healthcare providers. Healthcare providers from different specialties might have yielded different experiences of PROMs implementation. However, the sample of specialties is relatively wide; hence, we believe that the findings from this study are still relatively generalizable across the spectrum of healthcare providers.
Conclusion
In conclusion, this qualitative study provides an Asian perspective on the current and potential barriers and facilitators of PROMs implementation in routine clinical care. Moving forward, with an emphasis on value in healthcare, PROMs will likely become a key metric for value-driven outcomes, facilitating patient-centered optimization of medication and treatment. With PROMs still in a relatively early stage of implementation, this study seeks to contribute to foundational research on PROMs in Asia. The strategies gleaned from our study are pertinent and reflective of the local context and serve as a good starting point for sustainable, long-term PROMs implementation in routine clinical care.
Data availability
The datasets presented in this article are not readily available because of participant confidentiality and privacy. Requests to access the datasets should be directed to phakyh@nus.edu.sg and ellie_choi@nuhs.edu.sg.
References
Coulter, A. & Oldham, J. Person-centred care: What is it and how do we get there?. Future Hosp. J. 3(2), 114–116. https://doi.org/10.7861/futurehosp.3-2-114 (2016).
Tan KH. 2022 Enhancing Patient Safety: From Paternalistic Care to Person-Centred Care and Patient-Partnered Care. JPSHQ. https://doi.org/10.59439/V01N02C01
Long, V. et al. Understanding discordant perceptions of disease severity between physicians and patients with eczema and psoriasis using structural equation modeling. JAMA Dermatol. 159(8), 811. https://doi.org/10.1001/jamadermatol.2023.2008 (2023).
Basch, E. et al. Patient versus clinician symptom reporting using the national cancer institute common terminology criteria for adverse events: Results of a questionnaire-based study. Lancet Oncol. 7(11), 903–909. https://doi.org/10.1016/S1470-2045(06)70910-X (2006).
Sewitch, M. J., Abrahamowicz, M., Dobkin, P. L. & Tamblyn, R. Measuring differences between patients’ and physicians’ health perceptions: The patient-physician discordance scale. J. Behav. Med. 26(3), 245–264. https://doi.org/10.1023/A:1023412604715 (2003).
Karpouzas, G. A. et al. Discordant patient–physician assessments of disease activity and its persistence adversely impact quality of life and work productivity in US Hispanics with rheumatoid arthritis. RMD Open 3(2), e000551. https://doi.org/10.1136/rmdopen-2017-000551 (2017).
Kingsley, C. & Patel, S. Patient-reported outcome measures and patient-reported experience measures. BJA Educ. 17(4), 137–144. https://doi.org/10.1093/bjaed/mkw060 (2017).
Lins, L. & Carvalho, F. M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 4, 2050312116671725. https://doi.org/10.1177/2050312116671725 (2016).
Weldring, T. & Smith, S. M. S. Article commentary: Patient-reported outcomes (PROS) and patient-reported outcome measures (PROMs). Health Serv. Insights. https://doi.org/10.4137/HSI.S11093 (2013).
Tan, Y. H., Siew, J. X., Thomas, B. & Ng, K. C. Patient-reported outcome measures and value-based medicine in paediatrics: A timely review. Singapore Med. J. 64(5), 285–293. https://doi.org/10.11622/smedj.2021102 (2023).
Van Engen, V. et al. Enhancing clinicians’ use of electronic patient-reported outcome measures in outpatient care: Mixed methods study. J. Med. Internet Res. 26, e60306. https://doi.org/10.2196/60306 (2024).
Huberts, A. S. et al. Facilitators and barriers in the implementation and adoption of patient-reported outcomes measurements in daily practice. Value Health. 27(9), 1235–1242. https://doi.org/10.1016/j.jval.2024.05.020 (2024).
Morris, Z. S., Wooding, S. & Grant, J. The answer is 17 years, what is the question: Understanding time lags in translational research. J. R. Soc. Med. 104(12), 510–520. https://doi.org/10.1258/jrsm.2011.110180 (2011).
Rubin, R. It takes an average of 17 years for evidence to change practice-the burgeoning field of implementation science seeks to speed things up. JAMA 329(16), 1333–1336. https://doi.org/10.1001/jama.2023.4387 (2023).
Lyu, J. et al. Facilitators and barriers to implementing patient-reported outcomes in clinical oncology practice: A systematic review based on the consolidated framework for implementation research. Implement. Sci. Commun. 5(1), 120. https://doi.org/10.1186/s43058-024-00654-0 (2024).
Heath, E. L., Harris, I. A., Romero, L. & Ackerman, I. N. A systematic review of qualitative studies examining barriers and facilitators to orthopaedic surgeon engagement with patient-reported outcome measures data. J. Patient Rep. Outcomes. 8(1), 144. https://doi.org/10.1186/s41687-024-00820-x (2024).
Damschroder, L. J. et al. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 4(1), 50. https://doi.org/10.1186/1748-5908-4-50 (2009).
Powell, B. J. et al. A refined compilation of implementation strategies: Results from the expert recommendations for implementing change (ERIC) project. Implement. Sci. 10(1), 21. https://doi.org/10.1186/s13012-015-0209-1 (2015).
Waltz, T. J., Powell, B. J., Fernández, M. E., Abadie, B. & Damschroder, L. J. Choosing implementation strategies to address contextual barriers: Diversity in recommendations and future directions. Implement. Sci. 14(1), 42. https://doi.org/10.1186/s13012-019-0892-4 (2019).
Schwartzman, G., Reddy, S. A., Berg, S. H., Currie, B. J. & Saavedra, A. P. Cutaneous melioidosis: An updated review and primer for the dermatologist. J. Am. Acad. Dermatol. 89(6), 1201–1208. https://doi.org/10.1016/j.jaad.2023.07.1032 (2023).
CFIR Research Team-Center for Clinical Management Research. CFIR Interview Guide Tool. https://cfirguide.org/guide/app/#/guide_select
Braun, V. & Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa (2006).
Reardon, C. M. et al. The consolidated framework for implementation research (CFIR) user guide: A five-step guide for conducting implementation research using the framework. Implement. Sci. 20(1), 39. https://doi.org/10.1186/s13012-025-01450-7 (2025).
Lam, H. et al. Identifying actionable strategies: Using consolidated framework for Implementation research (CFIR)-informed interviews to evaluate the implementation of a multilevel intervention to improve colorectal cancer screening. Implement Sci. Commun. 2(1), 57. https://doi.org/10.1186/s43058-021-00150-9 (2021).
Tong, A., Sainsbury, P. & Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042 (2007).
Tseng HM, Lu J fen R, Gandek B. Cultural Issues in Using the SF-36 Health Survey in Asia: Results from Taiwan.
Krogsgaard, M. R. et al. How to translate and locally adapt a PROM. Assessment of cross-cultural differential item functioning. Scandinavian Med. Sci. Sports. 31(5), 999–1008. https://doi.org/10.1111/sms.13854 (2021).
Nguyen, H. et al. Using patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs) in routine head and neck cancer care: What do health professionals perceive as barriers and facilitators?. J. Med. Imag. Rad. Onc. 64(5), 704–710. https://doi.org/10.1111/1754-9485.13048 (2020).
Consolo, L. et al. Barriers and facilitators of electronic patient-reported outcome measures (e-PROMs) for patients in home palliative cancer care: A qualitative study of healthcare professionals’ perceptions. BMC Palliat Care. 22(1), 111. https://doi.org/10.1186/s12904-023-01234-0 (2023).
Schepers, S. A., Haverman, L., Zadeh, S., Grootenhuis, M. A. & Wiener, L. Healthcare professionals’ preferences and perceived barriers for routine assessment of patient-reported outcomes in pediatric oncology practice: Moving toward international processes of change. Pediatr. Blood Cancer 63(12), 2181–2188. https://doi.org/10.1002/pbc.26135 (2016).
Hubbard, J. M., Grothey, A. F., McWilliams, R. R., Buckner, J. C. & Sloan, J. A. Physician perspective on incorporation of oncology patient quality-of-life, fatigue, and pain assessment into clinical practice. JOP. 10(4), 248–253. https://doi.org/10.1200/JOP.2013.001276 (2014).
Nagy, G. et al. EULAR points to consider for the management of difficult-to-treat rheumatoid arthritis. Ann. Rheum. Dis. 81(1), 20–33. https://doi.org/10.1136/annrheumdis-2021-220973 (2022).
Heidenreich, P. A. et al. AHA/ACC/HFSA guideline for the management of heart failure: A report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation https://doi.org/10.1161/CIR.0000000000001063 (2022).
National Institute for Health and Care Excellence. Rheumatoid Arthritis in Adults: Management. 2018. https://www.nice.org.uk/guidance/ng100
UNICEF East Asia and Pacific Regional Office. Digital Literacy in Education Systems Across ASEAN.; 2021. https://www.unicef.org/eap/media/7766/file/Digital%20Literacy%20in%20Education%20Systems%20Across%20ASEAN%20Cover.pdf
Yu, F. et al. The influence of anticipated HIV stigma on health-related behaviors, self-rated health, and treatment preferences among people living with HIV in East Asia. AIDS Behav. 27(4), 1287–1303. https://doi.org/10.1007/s10461-022-03865-5 (2023).
Lauber, C. & Rössler, W. Stigma towards people with mental illness in developing countries in Asia. Int. Rev. Psychiatry 19(2), 157–178. https://doi.org/10.1080/09540260701278903 (2007).
Lim, Y. J., Chan, S. Y. & Ko, Y. Stigma and health-related quality of life in Asian adults with epilepsy. Epilepsy Res. 87(2), 107–119. https://doi.org/10.1016/j.eplepsyres.2009.08.014 (2009).
Lee, P. Y. et al. Barriers of and strategies for shared decision-making implementation in the care of metastatic breast cancer: A qualitative study among patients and healthcare professionals in an Asian country. Health Expect. 25(6), 2837–2850. https://doi.org/10.1111/hex.13590 (2022).
Lin, C. P. et al. What influences patients’ decisions regarding palliative care in advance care planning discussions? Perspectives from a qualitative study conducted with advanced cancer patients, families and healthcare professionals. Palliat. Med. 33(10), 1299–1309. https://doi.org/10.1177/0269216319866641 (2019).
Cofie, N., Braund, H. & Dalgarno, N. Eight ways to get a grip on intercoder reliability using qualitative-based measures. Can. Med. Ed. J. https://doi.org/10.36834/cmej.72504 (2022).
Acknowledgements
The authors thank all participants for their time and contribution to the study.
Funding
This study received grant funding from SingHealth Duke-NUS Academic Medical Centre through grants Pitch-For-Funds 03/FY2024/P2/26-A148, AM-HEARTS AM/HRT048/2025 (SRDUKAMR25H8) and R2S 2025/R2S/000001, and from the National Medical Research Council of Singapore through grant PHRGNIG24jul-0002 to Dr Kwan Yu Heng. The study received grant funding from the National University Health System through grant NUHSRO/2023/075/RO5+6/HPHSR-Sep23/04 to Dr Ellie Choi. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
KYH and CYS contributed to the conceptualization, supervision, data analysis and interpretation, drafting, and editing of the full manuscript. KYH and EC provided funding for the study. CYS, DJY, QL, EC, TP, BC, and CXR contributed to the data collection. CYS, DJY, QL, EC, TP, BC, WTH, KYH, and CXR contributed to the qualitative interview coding. TO, HRA, CG, JB, LLL, TSY, OPS, WF, LYY, YS, SC, JT contributed to the data analysis. KYH, CYS, DJY, QL, EC and CXR contributed to the drafting of the manuscript. All authors contributed to full manuscript editing, read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kwan, Y.H., Cheung, Y.S., Chew, X.R. et al. Barriers and facilitators of implementing patient-reported outcome measures in clinical care using the CFIR-ERIC framework. Sci Rep 16, 5494 (2026). https://doi.org/10.1038/s41598-026-35154-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-35154-9
