
Abstract
Direct oral anticoagulants (DOACs) are widely used in patients with atrial fibrillation (AF) to prevent stroke but increase the risk of upper gastrointestinal bleeding (UGIB). We aimed to quantify patient-perceived health-related quality-of-life (HRQoL) decrements associated with DOAC-related clinical events—stroke and UGIB—using a vignette-based approach. A survey was conducted with 391 AF patients on DOACs, embedded within a randomized trial evaluating proton pump inhibitor (PPI) co-therapy. Participants evaluated four hypothetical health states (stroke, post-stroke, UGIB, and post-UGIB) using EQ-5D-5L. The mean EQ-5D index for current health was 0.90 (SD 0.11). When imagining stroke, 89–95% of respondents perceived worsened HRQoL, particularly in self-care and usual activity domains. In contrast, 44–61% perceived worsened health in UGIB scenarios, primarily related to anxiety and depression. The estimated decrement in EQ-5D utility score was − 0.49 (SE 0.01) for stroke and − 0.16 (SE 0.01) for UGIB. Stroke was perceived to have a greater impact on the overall HRQoL domain, whereas UGIB was perceived to affect emotional well-being (anxiety/depression) disproportionately. These vignette-derived perceived utilities may inform patient-centered discussions and provide inputs for decision-analytic and cost-utility models evaluating anticoagulation strategies.
Trial registration number: KCT0006848.
Similar content being viewed by others
Introduction
Anticoagulant treatment, particularly the use of direct oral anticoagulant (DOAC), is pivotal in patients with atrial fibrillation (AF) to prevent stroke1,2,3. Although DOAC treatment is essential for stroke prevention in patients with AF, the use of DOACs can inevitably increase the risk of bleeding, most notably for upper gastrointestinal bleeding (UGIB)4,5. Stroke can cause severe neurological impairment, leading to reduced physical abilities, loss of independence, and the need for long-term care, which can drastically impair health-related quality of life (HRQoL)6,7. Otherwise, UGIB can diminish HRQoL due to hospitalizations, anxiety, and physical discomfort, and lead to interruptions in anticoagulation therapy, increasing the risk of stroke8,9,10. Balancing the benefits of DOAC use with the bleeding risks is essential for optimizing patient outcomes. However, no studies in patients taking DOACs have measured the HRQoL when stroke or UGIB occurred, which are mainly considered in cost-effectiveness modeling for DOAC11,12.
There is limited attention to the impact of DOAC-related clinical events on HRQoL, as perceived and reported by patients with AF. Patient-derived utility decrements for DOAC-related events are rarely available because these events are unpredictable and relatively infrequent, making prospective HRQoL measurement at the time of the event challenging. Nevertheless, it is crucial to assess the impact of stroke and UGIB on AF patients’ HRQoL to inform benefit–harm trade-offs.
To address this gap, we elicited patient-perceived utilities for hypothetical DOAC-related clinical events using vignettes with EQ-5D-5L. This substudy was embedded within the GUARD-OAC randomized trial to leverage a well-characterized cohort of DOAC-treated AF patients and standardized follow-up for gastrointestinal events with or without proton-pump inhibitor (PPI) co-therapy. It was designed to quantify perceived HRQoL decrements associated with these events rather than to infer the clinical effectiveness of PPI co-therapy. By comparing the perceived disutility of stroke (benefit of DOAC) with that of UGIB (harm of DOAC), we aimed to inform benefit–harm trade-offs and provide information for cost-effectiveness studies relevant to anticoagulation decisions. In addition, we explored factors associated with perceived HRQoL.
Methods
Vignette-based approach
Since cardiovascular events such as stroke are rare events, it is difficult to observe the HRQoL for that kind of health status. Considering AF patients, it can be particularly challenging to survey patients suffering from acute events such as stroke or UGIB due to the unpredictable occurrence. A vignette-based approach may be the only feasible method for eliciting health-state utility values for a cost-utility analysis13. This approach utilizes virtual scenarios representing the condition of interest. In the application of vignettes, respondents are assumed to rate vignette responses in the same way they rate their own HRQoL14. This study developed a vignette describing UGIB and stroke to measure the perceived HRQoL for these hypothetical health states. Then, the survey with the developed vignette was conducted on AF patients participating in a trial. This study was approved by the Seoul National University Hospital Institutional Review Board, Republic of Korea (H-2107-136-1236). Informed written consent was secured from all AF patients. All methods were performed in accordance with relevant guidelines and regulations.
Study population and survey
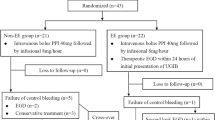
This was a vignette-based survey embedded in a randomized cotrolled trial, from which was titled ‘Gastrointestinal protection Using proton-pump inhibitor in pAtients who RequireD Oral AntiCoagulants (GUARD-OAC).’ The parent trial is a prospective, multicenter, open-label, randomized trial to investigate to evaluate the efficacy and safety of proton pump inhibitor (PPI) on patients taking DOAC for cardiovascular disease (Registration number at Clinical Research Information Service: KCT0006848; the registration date: December-02-2021). Patients required at least one year of DOAC (apixaban, edoxaban, rivaroxaban, and dabigatran) and HAS-BLED score ≥ 1 were randomly assigned in a 1:1 fashion to receive either DOAC alone or DOAC and PPI co-therapy. The primary endpoint is a composite of upper gastrointestinal clinical events – including bleeding, ulcer, or gastrointestinal symptoms – at one year after randomization. The study protocol with detailed inclusion and exclusion criteria is available at the Clinical Research Information Service15. Although HRQoL was planned to be collected in advance, it was not a measurement to evaluate the efficacy of an intervention in the trial.
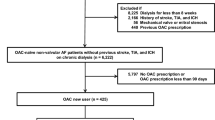
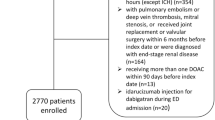
As part of a substudy within the GUARD-OAC trial, HRQoL data were collected from a subset of participants randomized between January 2022 and December 2022 at Seoul National University Hospital, a tertiary care academic hospital in the Republic of Korea. Although the parent trial was multicenter, this substudy was conducted at a single center. Participants were eligible for the substudy if they (1) met the trial eligibility criteria, (2) had non-valvular AF/AFL, (3) completed the baseline questionnaire, and (4) attended the 1-year follow-up assessment, at which time the HRQoL and vignette questionnaires were administered. At the 1-year visit, patients were invited to complete the EQ-5D-5L instrument for their current health state and for hypothetical vignettes describing DOAC-related clinical events (stroke and upper gastrointestinal bleeding). Patients who declined the vignette substudy were not asked to participate in the survey, even though they completed the 1-year follow-up (Supplementary Figure S1).
The parent trial (GUARD-OAC) is ongoing and continues recruitment and follow-up according to its prespecified protocol. Therefore, detailed exclusion and attrition counts for the overall multicenter trial population were not available at the time of this substudy analysis; however, participant flow and reasons for non-participation within the Seoul National University Hospital cohort are reported in Supplementary Figure S1.
A vignette-based survey was conducted to elicit perceived HRQoL associated with DOAC-related clinical events. At the 1-year visit, participants completed EQ-5D-5L for their current health state and then completed EQ-5D-5L after reading each vignette describing clinical event scenarios (stroke and UGIB). Although participants did not experience the events during the survey, they rated hypothetical health states described in standardized written vignettes. Vignettes were administered in a structured, interviewer-guided format by trained staff, with standardized explanations to ensure comprehension; participants were instructed to respond as if the described health state were their own.
Development of virtual scenarios for health status related to stroke and UGIB
The literature review was conducted to understand the symptoms of health status that AF patients taking DOACs may experience. Stroke was chosen since it is a primary outcome of DOAC treatment1,2,3. UGIB was considered as a health state because it is a frequent adverse event of the use of DOACs4,5. HRQoL is essential for cost-effectiveness studies, which generally estimate lifetime outcomes, so the possibility of recurrence and sequelae should be considered. Therefore, we defined four health statuses: (1) UGIB, (2) post-UGIB, (3) stroke, and (4) post-stroke.
The vignette texts were developed based on clinical definitions and reviewed by four cardiologists for clinical plausibility and clarity prior to administration. We developed vignettes that described the physical and psychosocial symptoms of four health states, as well as the AF patients’ restrictions on speaking and physical activities in daily life due to these symptoms. Four cardiologists (EKC, SRL, SK, and HJA) amended the descriptions of each health state to improve the accuracy and appropriateness of the vignettes, based on the clinical circumstances and experiences of those who had been treating AF patients taking DOAC for a long time, while considering patients’ health literacy. In addition, pilot testing was conducted with with lay adults without medical training (n = 3) to assess readability and comprehension (face validity). Feedback from the pilot was used to refine wording and improve interpretability prior to the main survey. The vignettes (descriptions of scenarios for four health states) are presented in Supplementary Table S1.
Assessment tool for the quality of life
Participants were asked to evaluate their current health and to imagine being in each vignette scenario. We adopted the certified Korean versions of EQ-5D-5L as the HRQoL measurements. The EQ-5D-5L is a widely-used, standardized tool for measuring HRQoL, especially in cost-effectiveness studies, and has demonstrated good validity, discriminatory ability, and reliability in patients and the general population16,17,18. It consists of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Across each of the five dimensions, respondents are asked to select the most appropriate status among 5 levels: no problems, slight problems, moderate problems, severe problems, and unable to/extreme problems. Based on responses in five domains, the EQ-5D index (utility) is calculated by following a tariff set from a standardized valuation study in South Korea19. The EQ-5D-5L utilities range from − 0.066 (worst case) to 1 (best case). The EuroQol Visual Analog Scale (EQ-VAS), included in the EQ-5D-5L instrument, was also measured. EQ-VAS asks patients to rate their health status between 0 (worst imaginable health status) and 100 (best imaginable health status).
EQ-5D index for current health that was measured at the time of randomization was used for analyzing factors associated with HRQoL; EQ-5D responses for four scenarios that were measured at the end of trial were used for analyzing patitnet’s perception on DOAC-related clinical events.
Statistical analysis
For baseline characteristics, continuous variables were summarized using means and standard deviations (SD), and categorical variables were represented as counts and percentages. The deterioration of response was defined as a case in which a response of a dimension for health status of interest was worse than the current health or event case. Improvement of response was defined as a case where the response was better than the current health or event case. Boxplot and Sankey’s diagrams visualized the distribution of utilities (Supplementary Figure S2) and the flow of the EQ-5D responses between current status and scenarios in each dimension (Supplementary Figure S3), respectively.
We used a linear mixed random-intercept model, adjusting for covariates, to examine the disutility associated with the health scenarios, defined as the differences in utility values between the current and scenario health states. For comparison, the mean and standard error (SE) of the least-squares estimates were estimated. The difference represents the decrease in utility due to the condition described in the scenarios. That is, the difference can be interpreted as disutility. For the linear mixed-effects models, we assessed key assumptions by examining the distribution of random effects and residuals. Normality and homoscedasticity of residuals were evaluated using residual and Q–Q plots, and no major deviations were observed. The random-intercept specification was also examined for model stability and convergence. Random intercepts were fitted only at the individual (patient) level. This specification was chosen to account for between-patient heterogeneity in baseline utility while assuming that the effects of covariates are constant within patients over scenarios. No additional higher-level random effects were included.
Based on previous studies,20,21,22,23,24,25,26 covariates were collected. Demographic characteristics, including age, body mass index (BMI), and sex, were collected at baseline. Two risk scores were employed for AF: the CHA2DS2-VASc score, which assesses stroke risk, and the HAS-BLED score, which measures bleeding risk27. The risk score for cognitive dysfunction, KDSQ-C/H/D scores,28 were included as a factor in the analysis, considering the significant influence of cognitive dysfunction on HRQoL as indicated by Pan et al.29 Furthermore, the type, duration, and class of AF [a European Heart Rhythm Association (EHRA) symptom classification] were collected. The study also investigated factors related to stroke or UGIB, including the type of DOAC, history of smoking, history of drinking, comorbidities, and family history of gastrointestinal bleeding and cardiovascular disease. The comorbidities included hypertension, diabetes, previous acute coronary syndrome, previous percutaneous coronary intervention, peripheral artery disease, congestive heart failure, chronic kidney disease, chronic liver disease, a history of prior stroke, transient ischemic attack, systemic thromboembolism, and UGIB.
To assess factors impacting HRQoL, a gamma generalized linear model (GLM) with a log link function was utilized. The inverse utility was considered as a dependent variable for the gamma distribution. This allows for a skewed distribution of utility values and prevents the prediction of utilities > 1. We verified the appropriateness of the gamma distribution and link function by inspecting the distribution of the transformed outcome (inverse utility) and by evaluating deviance residuals and fitted-versus-observed plots. These diagnostics indicated adequate model fit and no evidence of systematic misspecification. In addition, we assessed influential observations and multicollinearity across models; no influential outliers or problematic collinearity were identified. Based on these diagnostic checks, the assumptions underlying both modeling frameworks were deemed reasonable. Through the model, the effect size and 95% confidence interval (CI) were estimated. For interpretability, we report the inverse of exponentiated coefficients as ratios corresponding to the direction of the EQ-5D index (higher values indicate higher utility). For example, if the estimated ratio of factor X is 0.8, it means that factor X reduces utility by 20%.
Because utility values are bounded and commonly exhibit a ceiling effect, we additionally fitted a Tobit regression model as a sensitivity analysis to examine factors associated with utility. In the Tobit model, the same set of covariates used in the primary GLM was included. Results from the Tobit model are reported as regression coefficients (β) with 95% confidence intervals and were compared with the exponentiated coefficients (exp[β]) from the gamma GLM to assess robustness of the identified associations.
All analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, North Carolina, USA). R version 4.2.2 (The R Foundation for Statistical Computing, Vienna, Austria) was used for Sankey diagrams. There were no missing values for the primary outcome variables, including EQ-5D and EQ-VAS scores. All analyses were based on complete data.
Result
HRQoL data related to clinical events were obtained from 391 patients (PPI group n = 199, Non-PPI group n = 192) who assessed hypothetical health conditions through vignettes (Supplementary Figure S1). The baseline characteristics of respondents are shown in Table 1. At the baseline, the mean age was 73.2 (SD 6.4) years old, with 56.3% falling in the 70–79 age group. There were more male patients (64.7%) than females (35.3%). Persistent AF was the most observed (62.4%), and the most common comorbidity was hypertension (70.3%), following diabetes (29.7%). Of the total, 6.6% and 2.1% had a history of stroke and UGIB, respectively. The characteristics between two groups were similar. At the baseline, the mean utility measured by EQ-5D was 0.90 (SD 0.11) while the mean utility was 0.90 (SD 0.11) at 1 year after.
Baseline demographic and clinical characteristics stratified by completion of the 1-year follow-up in the parent trial cohort and by randomization group are provided in Supplementary Tables S2–S3 to assess potential selection bias. Compared with participants who declined the vignette survey, completers were slightly younger (73.2 vs. 74.8 years, p < 0.001) and had marginally lower CHA₂DS₂-VASc scores (3.0 vs. 3.2, p = 0.003). The distribution of DOAC type also differed (p = 0.007), and lifestyle factors (smoking and alcohol use) varied between groups. Other baseline clinical characteristics, including HAS-BLED score and major comorbidities, were broadly comparable. Importantly, randomization group allocation (PPI vs. non-PPI) did not differ by vignette survey completion status (p = 0.648) (Supplementary Table S2). As presented in Supplementary Table S3, no statistically significant differences were observed between the PPI group (n = 199) and the non-PPI group (n = 192) across demographic variables, comorbidities, risk scores, or medication use.
Table 2 presents the HRQOL for five health states — current, stroke, post-stroke, UGIB, and post-UGIB — measured using the EQ-5D based on the scenario. The mean utility was the lowest when patients imagined having a stroke episode (0.41, SD 0.26) and went up to 0.73 (SD 0.17) in the post-stroke status. When imagining the occurrence of UGIB, the mean utility was 0.73 (SD 0.22), but this increased to 0.90 (SD 0.12) in the post-UGIB status, which is comparable with that in the current health (0.90, SD 0.11). When adjusting factors affecting the EQ-5D index, the utilities in all the health statuses except the post-UGIB state was significantly different from the utility of the current health. The decrement of EQ-5D was the biggest for stroke (adjusted disutility 0.49, SE 0.01), followed by UGIB (adjusted disutility 0.16, SE 0.01). Supplementary Table S4 presents EQ-VAS and EQ-5D index for current and four hypothetical health states by parent trial group. No statistically significant differences were observed between the PPI (n = 199) and non-PPI (n = 192) groups for any health state, either in current health status or in perceived utility for hypothetical scenarios (UGIB, post-UGIB, stroke, and post-stroke).
The change of AF patients’ perception to hypothetical health statuses is shown in Table 3 based on individual levels of responses across five domains. The changes were notable in the case of stroke, and they were not reverted in the post-stroke state as much as in the post-UGIB state. 70.08% of respondents shows that their EQ-5D with the UGIB would be lower than their utility with only AF, while 95.65% did with the stroke. Across five dimensions, 44–61% of AF patients responded that UGIB would result in worse health outcomes compared to their current health status, and 71.1% of respondents perceived their health status would be improved in case of post-UGIB. The greatest proportion of worsening due to UGIB was the anxiety/depression (60.87%) among five dimensions (Fig. 1). Regarding stroke, 89–95% of AF patients responded that their health would become worse than its current state across five dimensions. The greatest proportion of worsening due to stroke were self-care and usual activity (94.63% in both, Fig. 2 shows usual activity). 84% of AF patients responded improvement in mobility, self-care, and usual activities following a stroke (post-stroke vs. stroke). The detailed responses are visualized using the Sankey diagrams in the Supplementary Figure S3.

Sankey diagram of transitions in EQ-5D anxiety/depression levels across the UGIB scenarios Arrangement – a left bar: current, a middle bar: event occurred, a right bar: post-event; Color - blue-green is level 1, yello is level 3, and red is level 5. Level 1 = I have no problems; Level 2 = I have slight problems; Level 3 = I have moderate problems; Level 4 = I have severe problems; Level 5 = I am unable. UGIB, upper gastrointestinal bleeding.

Sankey diagram of transitions in EQ-5D usual activities levels across the stroke scenarios. Arrangement – a left bar: current, a middle bar: event occurred, a right bar: post-event; Color - blue-green is level 1, yello is level 3, and red is level 5. Level 1 = I have no problems; Level 2 = I have slight problems; Level 3 = I have moderate problems; Level 4 = I have severe problems; Level 5 = I am unable. UGIB, upper gastrointestinal bleeding.
Additionally, factors associated with utility of AF patients were identified through the gamma GLM (Table 4). Age (ratio 0.996, 95% CI 0.994–0.998) and BMI (0.995, 0.991–0.998) show a negative association with utility. AF patients with an EHRA symptom classification of 1 have higher utilitythan AF patients with an EHRA symptom classification of 2b (1.054, 1.002–1.110). Male also reported a higher utility than female (1.030, 1.001–1.059). The KDSQ scores and HAS-BLED scores are also associated with the lower one.
Discussion
This study evaluated the utility values of AF patients and perceived HRQoL across four potential DOAC-related clinical events (stroke, post-stroke, UGIB, post-UGIB) with the EQ-5D instrument given the vignette with hypothetical scenarios. This study highlights the differential impact of stroke and UGIB on HRQoL in patients taking DOAC. Stroke was perceived to be the greatest decline in utility (-0.49), primarily due to impairments in self-care and daily activities. In contrast, UGIB had a smaller impact (-0.16) but was strongly associated with increased anxiety and depression. To the best of our knowledge, no previous study has comprehensively assessed patient-reported HRQoL in AF with specific attention to both stroke and UGIB. The utility decrements reported in this study offer a more nuanced understanding of the lived burden of these adverse events. These findings suggest that while stroke prevention should remain the primary goal of DOAC therapy, UGIB prevention is also important for maintaining quality of life.
UGIB, which could occur during the DOAC treatment of AF patients, lowers the patients’ HRQoL (disutility 0.16 in this study). Campbell et al.10 reported a mean utility of 0.68–0.74 in patients admitted to hospitals with acute UGIB in the UK while the mean for the UK general population was 0.86. It was not compared with utility of AF patients without UGIB or stroke but shows the UGIB attributed to the lower HRQoL. In this study, patients perceived UGIB as a temporary condition, with HRQOL nearly returning to baseline post-UGIB (utility: 0.90), whereas post-stroke valued lower (0.73). This suggests that UGIB was perceived as largely transient, with HRQoL expected to return close to baseline after resolution. In contrast, stroke has the potential to significantly and irreversibly reduce the patient’s HRQoL. This pattern was consistent across both the disutility estimates and the distribution of individual vignette valuations. As shown in Supplementary Figure S2 and Supplementary Figure S3, this trend was consistent across all dimensions of the EQ-5D. This suggests that UGIB, though distressing, is not as debilitating in the long term as stroke.
The study by Sadlonova et al.30 analyzed HRQoL, anxiety, and depressive symptoms in AF patients after stroke. The utility measured with EQ-5D increases relative to baseline at 3 months (0.37), 6 months (0.43), and 12 months follow-up (0.44). The study concludes that stroke survivors generally show improvements in HRQoL, and reductions in anxiety. Joundi et al.31 conducted a systematic review and meta-analysis on utility in patients with stroke. Although this study not considered AF patients, pooled utility was the lowest during hospitalization (0.39), followed by at rehabilitation (0.57), at 3 months (0.65), and at 5 years after stroke (0.70). Although we did not specify a post-stroke time point, and patients assessed HRQoL based on hypothetical health conditions rather than experienced stroke, the difference between the stroke and the post-stroke was similar to those reported in the previous studies30,31 (0.37 to 0.44 in Sadlonova et al.30; 0.26 to 0.31 in Joundi et al.31; 0.31 in our study). In AF patients, anxiety was inversely related with stroke30,32. Our results also shows that stroke affected not only activity-related domains but also anxiety/depression domains.
In our vignette-based valuations, UGIB was perceived to affect the anxiety/depression dimension especially. Beyond bleeding itself, fear of bleeding is a common concern for patients with AF.33,34 In addition to managing the bleeding episode itself, clinicians may need to address patients’ psychological burden and uncertainty related to anticoagulation after a bleeding event34. Practical approaches could include clear communication regarding plans for temporary interruption and resumption of anticoagulation when clinically appropriate, given the competing risks of bleeding and thromboembolism35. This concern may be particularly salient in frail and clinically complex AF populations, where anticoagulation decisions are frequently individualized to balance competing thromboembolic and bleeding risks36. Recent observational data have shown that stopping DOACs is associated with poorer clinical outcomes, such as increased risks of all-cause death and major adverse cardiovascular events37. This highlights the potential dangers of extended discontinuation interruption. Existing decision aids and DOAC decision-support tools for AF emphasize individualized benefit–risk communication38. These perceived utilities may also support shared decision-making by making patient-valued trade-offs more explicit when discussing DOAC. Incorporating patient-perceived disutility estimates for stroke and UGIB may help clinicians better understand how patients perceive these conditions. Our exploratory finding that PPI co-therapy does not significantly change the perceived disutility of UGIB indicates that the psychological burden of bleeding events stays high regardless of preventive medication, highlighting the importance of patient education.
We also analyzed the factors related to the utility. A lot of studies20,21,23,25,39,40,41,42,43,44 have reported impaired HRQoL in patients with AF and analyzed associated factors; age, female, and symptomatic AF influence HRQoL,25 focusing on EQ-5D, age, gender, AF type and symptom were established as factors23. Our study revisited the fact that age, sex, symptoms (EHRA symptom classification) and BMI were associated with utility. Our findings are consistent with a trend of utility in the Korean population and previous studies that state that older age is associated with decreased utility21,22,23,25. Regarding gender, men were more likely to report higher HRQoL. It was consistent with numerous previous studies40,41,42. Interestingly, Freeman et al.45 reported the effect of comorbidity, but in our study, it was foundd to be insignificant. It seems to be due to the difference in adjusting comorbidity. Freeman et al.45 reported HRQoL without adjusting other factors, while our study presented the estimates after adjusting all included factors.
Beyond previous studies, we considered patients’ cognitive function as a candidate for the factor affecting HRQoL in patients with AF because OAC is known to increase the risk of cognitive decline, mild cognitive impairment, and dementia in patients with AF. We found an association between cognitive dysfunction (indexed as the KDSQ-C/H/D scores) and HRQoL in patients with AF. Pan et al.29 reported that the EQ-5D index and VAS scores were significantly lower for older Chinese with cognitive dysfunction than their counterparts using 5,557 individuals of community-based cross-sectional data. After adjusting covariates, the difference in the EQ-5D index was − 0.016 (95% CI: −0.024 to − 0.008); Srinoprasert et al.21 reported that dementia is associated with low HRQoL in older AF patients. Both studies consistently showed a lower utility.
Our study has several limitations. First, our approach utilized a scenario survey based on assumptions rather than patients’ experiences, which might render the results less accurate. A limitation is that vignette validity was supported primarily by expert review and standardized administration; only a small lay pilot was conducted, and formal patient cognitive debriefing and readability testing were not performed. Future work could strengthen face validity through patient-led pilot testing. However, the utility valuse we elicited were similar to previous reviews and studies. Second, although all patients were enrolled from a randomized controlled trial, this substudy was conducted at a single tertiary hospital. It included only patients who completed both baseline and 1-year follow-up assessments. This may have introduced selection bias and limits the generalizability of the findings to broader or more diverse populations. However, compared with non-completers, completers were modestly younger with slightly lower CHA₂DS₂-VASc scores, while most other baseline clinical characteristics were broadly similar (Supplementary Table S2). Bleeding risk (HAS-BLED) and major comorbidities were comparable, partially mitigating concerns regarding systematic bias. Third, considering that the average age of the patients was 74 years, with more than 50% falling in their 70s, caution is advised when generalizing these findings to patients in different age groups. Fourth, no formal sample size calculation was performed for this substudy, and while the final sample (n = 391) was sufficient for utility estimation, the precision of subgroup analyses may be limited.
Despite the several limitations, this study is the first to assess the utility of stroke and UGIB simultaneously in patients with AF. This addresses an important and often overlooked aspect of anticoagulant therapy, patients’ perception of the burden associated with thromboembolic and bleeding events. By quantifying the HRQoL impact of hypothetical stroke and UGIB scenarios, we sought to provide evidence directly applicable to clinical decision-making, policy modeling, and patient counseling. In addition, these vignette-derived perceived utilities/disutilities may serve as pragmatic inputs for cost-utility analyses when event-based HRQoL data are difficult to obtain. Due to the strong association between UGIB and psychological distress, adequate mental health support should be provided to affected patients.
Conclusion
Our study employed a vignette to quantify the HRQoL related to events that AF patients might encounter during the DOAC therapy, such as stroke and UGIB. Participants valued the hypothetical stroke as having a larger disutility than the hypothetical UGIB. Although stroke had a greater overall impact on HRQoL, UGIB—despite its smaller disutility—was perceived as emotionally distressing and more reversible. These perceived utilities may support patient-centered communication and can be incorporated into cost-utility analyses evaluating anticoagulation strategies. This study provides valuable utility values that can be applied in cost-utility studies and health policy evaluations in anticoagulation care.
Data availability
De-identified individual participant data, including the data dictionary and statistical code, will not be shared due to legal and ethical restrictions imposed by the Institutional Review Board and national data protection regulations.
References
Chan, N., Sobieraj-Teague, M. & Eikelboom, J. W. Direct oral anticoagulants: evidence and unresolved issues. Lancet 396, 1767–1776. https://doi.org/10.1016/S0140-6736(20)32439-9 (2020).
Gabet, A. et al. Stroke incidence and death in atrial fibrillation patients newly treated with direct oral anticoagulants. Clin. Epidemiol. 13, 131–140. https://doi.org/10.2147/CLEP.S290707 (2021).
Hindricks, G. et al. ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC (vol 42, pg 373, 2021). European Heart Journal 42, 4194–4194, (2020). https://doi.org/10.1093/eurheartj/ehab648 (2021).
Ray, W. A. et al. Association of oral anticoagulants and proton pump inhibitor cotherapy with hospitalization for upper Gastrointestinal tract bleeding. JAMA 320, 2221–2230. https://doi.org/10.1001/jama.2018.17242 (2018).
Komen, J. et al. Non-vitamin K antagonist oral anticoagulants, proton pump inhibitors and Gastrointestinal bleeds. Heart 108, 613–618. https://doi.org/10.1136/heartjnl-2021-319332 (2022).
Kariyawasam, P. N., Pathirana, K. D. & Hewage, D. C. Factors associated with health related quality of life of patients with stroke in Sri Lankan context. Health Qual. Life Outcomes. 18, 129. https://doi.org/10.1186/s12955-020-01388-y (2020).
Baumann, M., Le Bihan, E., Chau, K. & Chau, N. Associations between quality of life and socioeconomic factors, functional impairments and dissatisfaction with received information and home-care services among survivors living at home two years after stroke onset. BMC Neurol. 14, 1–12 (2014).
Son, Y. J., Baek, K. H., Lee, S. J. & Seo, E. J. Health-Related quality of life and associated factors in patients with atrial fibrillation: an integrative literature review. Int. J. Environ. Res. Public. Health. 16 https://doi.org/10.3390/ijerph16173042 (2019).
Zappulla, P. & Calvi, V. Gastrointestinal bleeding and direct oral anticoagulants among patients with atrial fibrillation: Risk, Prevention, Management, and quality of life. TH. Open. 5, e200–e210. https://doi.org/10.1055/s-0041-1730035 (2021).
Campbell, H. E. et al. Costs and quality of life associated with acute upper Gastrointestinal bleeding in the UK: cohort analysis of patients in a cluster randomised trial. BMJ Open. 5, e007230. https://doi.org/10.1136/bmjopen-2014-007230 (2015).
Harrington, A. R., Armstrong, E. P., Nolan, P. E. Jr. & Malone, D. C. Cost-effectiveness of apixaban, dabigatran, rivaroxaban, and warfarin for stroke prevention in atrial fibrillation. Stroke 44, 1676–1681. https://doi.org/10.1161/STROKEAHA.111.000402 (2013).
Thom, H. H. Z. et al. Directly acting oral anticoagulants for the prevention of stroke in atrial fibrillation in England and wales: Cost-Effectiveness model and value of information analysis. MDM Policy Pract. 4, 2381468319866828. https://doi.org/10.1177/2381468319866828 (2019).
Matza, L. S., Stewart, K. D., Lloyd, A. J., Rowen, D. & Brazier, J. E. Vignette-Based utilities: Usefulness, Limitations, and methodological recommendations. Value Health. 24, 812–821. https://doi.org/10.1016/j.jval.2020.12.017 (2021).
King, G., Murray, C. J. L., Salomon, J. A. & Tandon, A. Enhancing the validity and Cross-Cultural comparability of measurement in survey research. Am. Polit Sci. Rev. 98, 191–207. https://doi.org/10.1017/s000305540400108x (2004).
Gastrointestinal protection Using proton-pump inhibitor in pAtients who RequireD Oral AntiCoagulatns - randomized clinical trial: Study details, (2021). https://cris.nih.go.kr/cris/search/detailSearch.do?seq=20648&search_page=L
Herdman, M. et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20, 1727–1736. https://doi.org/10.1007/s11136-011-9903-x (2011).
Janssen, M. F. et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual. Life Res. 22, 1717–1727. https://doi.org/10.1007/s11136-012-0322-4 (2013).
Devlin, N. J. & Brooks, R. EQ-5D and the EuroQol group: Past, present and future. Appl. Health Econ. Health Policy. 15, 127–137. https://doi.org/10.1007/s40258-017-0310-5 (2017).
Kim, S. H. et al. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 25, 1845–1852. https://doi.org/10.1007/s11136-015-1205-2 (2016).
Witassek, F. et al. Health-related quality of life in patients with atrial fibrillation: the role of symptoms, comorbidities, and the type of atrial fibrillation. PLoS One. 14, e0226730. https://doi.org/10.1371/journal.pone.0226730 (2019).
Srinonprasert, V. et al. Factors associated with low health-related quality of life among younger and older Thai patients with non-valvular atrial fibrillation. Qual. Life Res. 28, 2091–2098. https://doi.org/10.1007/s11136-019-02171-3 (2019).
Randolph, T. C. et al. Patient factors associated with quality of life in atrial fibrillation. Am. Heart J. 182, 135–143. https://doi.org/10.1016/j.ahj.2016.08.003 (2016).
Berg, J., Lindgren, P., Nieuwlaat, R., Bouin, O. & Crijns, H. Factors determining utility measured with the EQ-5D in patients with atrial fibrillation. Qual. Life Res. 19, 381–390. https://doi.org/10.1007/s11136-010-9591-y (2010).
Hagens, V. E. et al. Effect of rate or rhythm control on quality of life in persistent atrial fibrillation. Results from the rate control versus electrical cardioversion (RACE) study. J. Am. Coll. Cardiol. 43, 241–247. https://doi.org/10.1016/j.jacc.2003.08.037 (2004).
Zhang, L., Gallagher, R. & Neubeck, L. Health-related quality of life in atrial fibrillation patients over 65 years: A review. Eur. J. Prev. Cardiol. 22, 987–1002. https://doi.org/10.1177/2047487314538855 (2015).
Koutoukidis, D. A., Jones, N. R., Taylor, C. J., Casadei, B. & Aveyard, P. Obesity, self-reported symptom severity, and quality of life in people with atrial fibrillation: A community-based cross-sectional survey. Nutr. Metab. Cardiovasc. Dis. 30, 2221–2229. https://doi.org/10.1016/j.numecd.2020.07.009 (2020).
Pisters, R. et al. A novel User-Friendly score (HAS-BLED) to assess 1-Year risk of major bleeding in patients with atrial fibrillation. Chest 138, 1093–1100. https://doi.org/10.1378/chest.10-0134 (2010).
Yang, D.-W., Cho, B.-l., Chey, J.-Y., Kim, S.-Y. & Kim, B.-S. The development and validation of Korean dementia screening questionnaire (KDSQ). J. Korean Neurol. Assoc. 20, 135–141 (2002).
Pan, C. W. et al. Cognitive dysfunction and health-related quality of life among older Chinese. Sci. Rep. 5, 17301. https://doi.org/10.1038/srep17301 (2015).
Sadlonova, M. et al. Health-related quality of life, anxiety and depression up to 12 months post-stroke: influence of sex, age, stroke severity and atrial fibrillation–A longitudinal subanalysis of the Find-AFRANDOMISED trial. J. Psychosom. Res. 142, 110353 (2021).
Joundi, R. A. et al. Health state utility values in people with stroke: A systematic review and Meta-Analysis. J. Am. Heart Assoc. 11, e024296. https://doi.org/10.1161/JAHA.121.024296 (2022).
Schnabel, R. B. et al. Symptom burden of atrial fibrillation and its relation to interventions and outcome in Europe. J. Am. Heart Assoc. 7, e007559. https://doi.org/10.1161/JAHA.117.007559 (2018).
Yao, C., Jones, A. E., Slager, S., Fagerlin, A. & Witt, D. M. Exploring clinician perspectives on patients with atrial fibrillation who are not prescribed anticoagulation therapy. PEC Innov. 1, 100062. https://doi.org/10.1016/j.pecinn.2022.100062 (2022).
Ueda, I. et al. Patient concern regarding bleeding side effects from oral anticoagulation therapy for atrial fibrillation: an analysis from the multicentre KiCS-AF registry. Eur. J. Cardiovasc. Nurs. 23, 358–366. https://doi.org/10.1093/eurjcn/zvad094 (2023).
Tomaselli, G. F. et al. 2020 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: a report of the American college of cardiology solution set oversight committee. J. Am. Coll. Cardiol. 76, 594–622 (2020).
Romiti, G. F. & Lip, G. Y. Switching Anticoagulants and Managing Complexity in Frail Patients With Atrial Fibrillation: An Integrated Approach. J. Am. Coll. Cardiol. 86, 440–443 (2025).
Bucci, T. et al. Adverse events in clinically complex elderly patients with atrial fibrillation according to oral anticoagulation status. EClinicalMedicine 78, 102974. https://doi.org/10.1016/j.eclinm.2024.102974 (2024).
Joglar, J. A. et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Col. Cardiol. 83, 109–279. https://doi.org/10.1016/j.jacc.2023.08.017 (2024).
Dorian, P. et al. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: implications for the assessment of investigational therapy. J. Am. Coll. Cardiol. 36, 1303–1309. https://doi.org/10.1016/s0735-1097(00)00886-x (2000).
Freeman, J. V. et al. Association between atrial fibrillation Symptoms, quality of Life, and patient outcomes: results from the outcomes registry for better informed treatment of atrial fibrillation (ORBIT-AF). Circ. Cardiovasc. Qual. Outcomes. 8, 393–402. https://doi.org/10.1161/CIRCOUTCOMES.114.001303 (2015).
Piccini, J. P. et al. Differences in clinical and functional outcomes of atrial fibrillation in women and men. JAMA Cardiol. 1, 282–291. https://doi.org/10.1001/jamacardio.2016.0529 (2016).
Blum, S. et al. Prospective assessment of Sex-Related differences in symptom status and health perception among patients with atrial fibrillation. J. Am. Heart Assoc. 6 https://doi.org/10.1161/JAHA.116.005401 (2017).
Potpara, T. S. et al. Self-reported treatment burden in patients with atrial fibrillation: quantification, major determinants, and implications for integrated holistic management of the arrhythmia. Europace 22, 1788–1797. https://doi.org/10.1093/europace/euaa210 (2020).
Almeida Gde, Q., Noblat Lde, A. & Passos, L. C. Do Nascimento, H. F. Quality of life analysis of patients in chronic use of oral anticoagulant: an observational study. Health Qual. Life Outcomes. 9, 91. https://doi.org/10.1186/1477-7525-9-91 (2011).
Freeman, J. V. et al. Association between atrial fibrillation symptoms, quality of life, and patient outcomes: results from the outcomes registry for better informed treatment of atrial fibrillation (ORBIT-AF). Circulation: Cardiovasc. Qual. Outcomes. 8, 393–402 (2015).
Funding
This work was supported by a grant from the Patient-Centered Clinical Research Coordinating Center (PACEN) funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2021-KH119931). The funder had no role in study design, data collection, analysis, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
Conceptualization: Kwon SH, Lee EK, Lee SR, Choi EK; Data curation: Ahn HJ, Lee SR, Choi EK; Data analysis: Kwon SH, Nam JH; Methodology: Kwon SH, Nam JH, Lee EK, Ahn HJ, Kwon S, Lee SR, Choi EK; Writing - original draft: Kwon SH, Nam JH, Lee EK; Writing - review & editing: All authors.
Corresponding authors
Ethics declarations
Competing interests
Eue-Keun Choi reported research grants or speaking fees from Bayer, BMS/Pfizer, Biosense Webster, Chong Kun Dang, Daiichi-Sankyo, Dreamtech Co., Ltd., Medtronic, Samjinpharm, Sanofi-Aventis, Seers Technology, Skylabs, and Yuhan. The other authors have no financial conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kwon, SH., Ahn, HJ., Nam, J.H. et al. Patient-reported health utility of stroke and gastrointestinal bleeding related to DOACs in atrial fibrillation: a vignette-based substudy of a randomized controlled trial. Sci Rep 16, 5328 (2026). https://doi.org/10.1038/s41598-026-35628-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-35628-w
