
Abstract
Metabolic associated steatotic liver disease (MASLD) is a globally prevalent metabolic disorder characterized by hepatic steatosis, inflammation, and impaired lipid homeostasis. Vitamin D exhibits anti-inflammatory and insulin-sensitizing properties, whereas intermittent fasting (IF) has recently emerged as a metabolic intervention capable of improving hepatic and systemic energy balance. To compare the therapeutic effects of vitamin D and IF on high-fat and fructose diet-induced MASLD in rats, with emphasis on lipid metabolism, oxidative stress, and inflammatory signaling pathways. Twenty-four male Sprague–Dawley rats were allocated into four groups (n = 6/group): Control, MASLD (HFD), HFD + vitamin D, and HFD + IF. Biochemical analyses included fasting glucose, serum insulin, ALT, AST, lipid profile, MDA, and GSH. Immunohistochemistry quantified hepatic expression of SREBP1, AQP9, TLR4, and NF-κB. Numerical comparisons were reported as mean ± SD and percentage changes relative to HFD. Both interventions significantly improved MASLD outcomes. Vitamin D and IF reduced ALT by 42% and 47%, respectively, and lowered AST by 38% and 45% compared with HFD. Triglycerides and LDL-C decreased by 31–48%, while HDL-C increased by 18–24%. Oxidative stress improved, with MDA reduced by 36% (vitamin D) and 54% (IF), and GSH elevated by 61% and 82%, respectively. Both treatments markedly downregulated hepatic SREBP1 and the AQP9 glycerol transport pathway, and suppressed activation of TLR4/NF-κB signaling. Vitamin D and intermittent fasting exert significant hepatoprotective effects in MASLD by improving metabolic parameters, enhancing antioxidant capacity, and attenuating inflammatory signaling. These findings support their potential as complementary, non-pharmacological strategies for MASLD management and warrant further translational investigation.
Similar content being viewed by others

Introduction
Metabolic associated steatotic liver disease (MASLD), previously termed non-alcoholic fatty liver disease (NAFLD), has emerged as the most prevalent chronic liver disorder worldwide and is increasingly recognized as a major metabolic health challenge1. The pathogenesis of MASLD is multifactorial and has been traditionally described using the “two-hits” paradigm2. The first hit involves dysregulated lipid metabolism leading to hepatocellular triglyceride accumulation, whereas the second hit encompasses oxidative stress and an amplified inflammatory response mediated by cytokines such as interleukins, transforming growth factor-β1 (TGF-β1), nuclear factor kappa B (NF-κB), and tumor necrosis factor-α (TNF-α), ultimately predisposing to metabolic dysfunction-associated steatohepatitis (MASH), fibrosis, and cirrhosis3.
Toll-like receptors (TLRs), particularly TLR4, serve as central mediators of innate immune activation through the detection of pathogen- and damage-associated molecular patterns4. Activation of TLR4 triggers downstream signaling cascades that intensify hepatic inflammation and contribute to MASLD progression5. In models of metabolic and diabetes-associated liver injury, TLR4 signaling promotes macrophage recruitment and enhances inflammatory cytokine release, thereby exacerbating hepatic damage6. Subsequent activation of NF-κB further amplifies cytokine production and sustains the inflammatory response characteristic of MASLD7.
Aquaporins (AQPs), especially AQP9, are membrane proteins facilitating the transport of water, glycerol, and small solutes8. AQP9 is highly expressed in hepatocytes and plays a key role in glycerol uptake, an essential substrate for gluconeogenesis9. Altered AQP9 expression has been linked to hepatic lipid accumulation, and elevated AQP9 levels have been associated with the development and worsening of steatosis10.
Sterol regulatory element-binding protein 1 (SREBP1) is a master transcriptional regulator of hepatic fatty acid and triglyceride synthesis11. Upregulation of SREBP1 promotes de novo lipogenesis and contributes to hepatocellular lipid overload, positioning it as a central driver in MASLD pathogenesis12.
Vitamin D has recently gained attention for its potential therapeutic benefits in metabolic disorders, including MASLD, owing to its anti-inflammatory, antioxidant, and insulin-sensitizing effects13. Intermittent fasting (IF), another promising metabolic intervention, has demonstrated improvements in lipid profiles, oxidative stress, and insulin sensitivity in obesity-related disorders14.
Given these molecular pathways, this study aims to compare the therapeutic effects of vitamin D and intermittent fasting in a high-fat diet–induced MASLD rat model. Particular emphasis is placed on their ability to modulate AQP9 and SREBP1 expression, and to regulate TLR4/NF-κB inflammatory signaling. By delineating these mechanisms, the present work seeks to provide deeper insight into non-pharmacological strategies that may offer clinically relevant benefits for MASLD management.
Materials and methods
Ethics declarations
We confirm that all experiments on live vertebrates were conducted following appropriate ethical standards. The “Materials and Methods” section has been updated to clearly include the following statements:
-
All experimental protocols were approved by the Research Ethics Committee of the Faculty of Pharmacy, Mansoura University, Egypt (Approval no.: 2023 − 165).
-
All methods were carried out in accordance with relevant guidelines and regulations.
-
All methods are reported in accordance with the ARRIVE guidelines (https://arriveguidelines.org).
Animals
A total of twenty-four male adult Sprague-Dawley rats, aged 12–14 weeks and weighing between 200 and 230 g, were utilized in this study due to their suitability as a model for diet-induced obesity. These rats exhibit feeding behaviors analogous to humans, which can lead to significant weight gain and alterations in lipid metabolism. The rats were randomly assigned to different experimental groups using the standard RAND function in Microsoft Excel. The groups included: control (n = 6), high-fat and fructose diet (HFD) (n = 6), high-fat and fructose diet plus Vitamin D (HFD + VD) (n = 6), and high-fat and fructose diet plus intermittent fasting (HFD + IF) (n = 6).
The rats were housed in groups of three per cage, with bedding made of softwood chips in a pathogen-free environment. They were maintained under controlled conditions, with a temperature of 21 ± 2 °C, a reversed light/dark cycle of 12 h each, and a humidity level of 60 ± 5%. Prior to the experiment, the rats were given unrestricted access to food and water for 14 days to facilitate acclimatization.
High-fat and Fructose diet model (diet-induced obesity)
The high-fat diet consisted of 45% fat, with 40% derived from animal sources and 5% from the basal diet14. Additionally, the diet included 20% fructose, with 20 g of fructose dissolved in 100 milliliters of tap water15. Inclusion and exclusion criteria were established based on body weight changes; animals exhibiting a weight gain of more than 15% or 20 g were included, while those showing significant weight loss or reduced food intake were excluded16.
Chemicals used
Fructose was procured from El-Gomhorya Company for Drugs, Egypt, while Vitamin D was supplied as Devarol S 200,000 ampoules (Memphis Company, Cairo, Egypt; purity 99.99%).
Experimental design
The rats were divided into four groups, each consisting of six animals:
-
Control Group: Received a standard pellet diet for 12 weeks.
-
High-Fat and Fructose Diet Group (HFD): Fed a high-fat diet and given fructose in drinking water ad libitum for 12 weeks.
-
High-Fat and Fructose Diet + Vitamin D Group (HFD + VD): Fed a high-fat diet and given fructose in drinking water ad libitum for 12 weeks, followed by intraperitoneal injections of Vitamin D at a dosage of 5 µg/kg every two days for 4 weeks (≈ 200 IU/kg)17.
-
High-Fat and Fructose Diet + Intermittent Fasting Group (HFD + IF): Given a high-fat diet and fructose in drinking water for 12 weeks, followed by an intermittent fasting protocol involving 24 h of feeding followed by 24 h of fasting for four weeks18,19.
Assessment of body weight
The initial and final body weights of each animal were recorded and analyzed.
Specimen collection
Method of euthanasia
We have specified in the revised manuscript that euthanasia was performed by a combination of anesthesia (ketamine and xylazine) followed by exsanguination via retro-orbital puncture, a method consistent with ethical standards for animal research.
At the conclusion of the experiment, following a 12-hour fasting period, the rats were anesthetized. Blood samples were collected via retro-orbital puncture for biochemical assays. After euthanasia, the livers were excised, rinsed with cold normal saline, and fixed in 10% phosphate-buffered formalin. Some liver samples were embedded in paraffin for hematoxylin and eosin (H&E) staining and immunohistochemical analysis, while others were processed for Oil Red O staining.
Biochemical study
Blood glucose and insulin levels
Fasting blood glucose levels were measured using an ACCU-CHECK Performa glucometer (Roche Diagnostics, Mannheim, Germany). Serum insulin levels were assessed using an ELISA kit (CEA448Ra, Cloud-Clone, USA).
Lipid profile
Serum levels of total cholesterol, triglycerides, and HDL-C were measured using commercially available kits. LDL-C was calculated using the formula:
Liver function parameters
Serum samples were obtained by centrifugation at 5000 g for 10 min at 4 °C. The activities of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were measured using kinetic methods according to the manufacturer’s instructions (Elitech, UK).
Inflammatory markers
Serum levels of TNF-α and IL-1β were measured using commercial ELISA kits (Assaypro Co., USA; IBL Co., Ltd., Hamburg, Germany).
Oxidative stress markers
Reduced glutathione (GSH) and malondialdehyde (MDA) levels were quantified spectrophotometrically using kits from BioDiagnostics (Egypt), following the provided protocols.
Histopathological assessment
Liver samples were embedded in paraffin after fixation in 10% formaldehyde. Sections (5–7 μm thick) were cut and stained with H&E20. Oil Red O staining was performed on freshly frozen liver sections to visualize fat droplets in hepatocytes21,22.
Immunohistochemical assessment
Formalin-fixed, paraffin-embedded Sect. (5 μm) underwent deparaffinization and rehydration. Antigen retrieval was performed using 0.01 M citrate buffer. Endogenous peroxidase activity was blocked with 0.3% H2O2 for 30 min. Sections were then incubated with primary antibodies against AQP9 (1:200), SREBP-1 (1:200), NF-κB (1 µg/ml), and TLR-4 (1:500) overnight at 4 °C. Following incubation with biotinylated secondary antibodies and avidin-biotin complex, sections were treated with diaminobenzidine substrate (DAB)9. Counterstaining was performed with hematoxylin.
Morphometric studies
Microscopic images were captured using an Olympus CX41 light microscope (Olympus Corporation, Tokyo, Japan) equipped with a Nikon COOLPIX 5000 digital camera (Nikon Corporation, Tokyo, Japan). Image analysis was performed using ImageJ software, Version 1.51j8. (National Institutes of Health, Bethesda, MD, USA; https://imagej.nih.gov/ij/). Manufacturer information is available at https://www.olympus-lifescience.com and https://www.nikon.com/products/.”
Optical density measurements for AQP9, SREBP-1c, and NF-κB were obtained, while area fractions for TLR-4 were calculated. The intensity values were converted to optical density (OD) using the formula:
\(\:OD=\text{l}\text{o}\text{g}\:\:\frac{\text{M}\text{a}\text{x}\:\text{i}\text{n}\text{t}\text{e}\text{n}\text{s}\text{i}\text{t}\text{y}}{\text{M}\text{e}\text{a}\text{n}\:intensity}\)23. (Max intensity = 250)
Statistical analysis
Data were analyzed using the Statistical Package for Social Science (SPSS) version 18.0 for Windows. Results were expressed as mean ± SD. One-way ANOVA was employed for multiple group comparisons, with Tukey’s post-hoc test applied for further analysis. A p-value of < 0.05 was considered statistically significant.
Results
General observations
All animals completed the experimental period with no mortality. Rats in the control group exhibited normal activity and consistent physiological appearance. No abnormal behavior was observed in either intervention group.
Effects on body weight gain
The recorded initial body weight (IBW) mean values of all experimental groups were similar, with no statistically significant variation, ranging from 190 to 225 g. However, the mean final body weight (FBW) significantly increased in the HFD group compared to the control group. There was no significant variation in the average FBW between the control and HFD + VD groups. In contrast, the HFD + IF group exhibited a significant reduction in mean FBW compared to the control group. Both the HFD + VD and HFD + IF groups showed lower significant measures compared to the HFD group, with the HFD + IF group exhibiting lower significant measures compared to the HFD + VD group (Fig. 1).

The study groups’ mean initial and final body weight (g) values. * Significant (P < 0.05) as compared to control group. # Significant (P < 0.05) as compared to the HFD group. $ Significant (P < 0.05) as compared to HFD + VD group.
Biochemical profiles
Blood glucose and serum insulin levels
HFD feeding resulted in a significant elevation in fasting blood glucose (FBG) and a reduction in serum insulin compared with the control group (p < 0.05). Vitamin D and IF markedly attenuated hyperglycemia, reducing FBG by approximately 52% and 55%, respectively, compared with HFD (p < 0.05). Mean glucose values decreased from HFD to VD and, respectively (Fig. 2A).

Blood glucose level (A), Serum levels of insulin (B), total cholesterol (C), triglycerides (D), LDL-cholesterol (E) and HDL-cholesterol (F) in control and experimental groups. * Significant (P < 0.05) as compared to control group. # Significant (P < 0.05) as compared to the HFD group. $ Significant (P < 0.05) as compared to HFD + VD group.
Serum insulin, significantly reduced in the HFD group (p < 0.05), was restored by ~ 53% in the HFD + VD group and ~ 60% in the HFD + IF group (p < 0.05 vs. HFD), with no significant difference between the two interventions (Fig. 2B).
Lipid metabolic parameters
HFD-fed rats showed significant elevations in serum total cholesterol (TC), triglycerides (TG), and LDL-C compared with the control group (p < 0.05). Vitamin D reduced TC by ~ 21%, TG by ~ 29%, and LDL-C by ~ 44%, while IF produced a more pronounced reduction of ~ 32%, ~ 38%, and ~ 56%, respectively (p < 0.05 vs. HFD for all). HDL-C increased modestly in both intervention groups, rising ~ 20% in HFD + VD and ~ 10% in HFD + IF (p < 0.05 vs. HFD) (Figs. 2C–F).
Effect on liver functions
Serum ALT and AST were significantly elevated in the HFD group (p < 0.05). Vitamin D reduced ALT and AST by ~ 36% and ~ 32% relative to HFD, respectively, while intermittent fasting produced reductions of ~ 30% and ~ 36% (p < 0.05). ALT in the IF group did not differ significantly from the control group (p > 0.05), whereas AST remained slightly elevated compared with control (p < 0.05) (Figs. 3A–B).

Serum levels of ALT (A), AST (B), MDA (C), GSH (D), TNF α (E) and IL1β (F) in control and experimental groups. * Significant (P < 0.05) as compared to control group. # Significant (P < 0.05) as compared to the HFD group. $ Significant (P < 0.05) as compared to HFD + VD group.
Oxidative stress and inflammatory markers
HFD feeding resulted in a significant rise in serum MDA and a marked reduction in GSH levels (p < 0.05). Vitamin D decreased MDA by ~ 32%, while IF induced a stronger reduction of ~ 41% (p < 0.05 vs. HFD) (Fig. 3C). GSH levels increased by ~ 64% with vitamin D and by ~ 96% with IF, indicating superior antioxidant restoration in the fasting group (p < 0.05) (Fig. 3D).
Pro-inflammatory cytokines TNF-α and IL-1β were significantly elevated in HFD-fed rats (p < 0.05). Vitamin D reduced TNF-α by ~ 38%, while IF produced a more pronounced reduction of ~ 46%. IL-1β declined by ~ 31% with vitamin D and ~ 33% with IF (p < 0.05 vs. HFD for both) (Figs. 3E–F).
Hepatic histological features
Hematoxylin and Eosin staining results
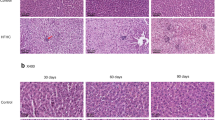
Control liver sections showed normal hepatic cords, preserved nuclei, and intact sinusoidal architecture (Fig. 4A). HFD-fed rats exhibited extensive macrovesicular and microvesicular steatosis, inflammatory infiltrates near portal tracts, sinusoidal dilation, and occasional hepatocellular ballooning (Fig. 4B).

Photomicrographs of liver sections stained with H&E. A & E: The control group shows normal liver architecture, with hepatocytes exhibiting central rounded vesicular nuclei. Hepatic blood sinusoids (S) are radially arranged between hepatic cords. Normal bile duct (B) is observed in the portal area (P). B & F: The HFD group shows widespread macrovesicular lipid globules (black arrows) with squeezed nuclei into the thin rim of cytoplasm in some hepatocytes, others with microvesicular lipid droplets (arrowheads). Inflammatory cellular infiltration (curved arrows) appears near congested and dilated portal veins (P) and blood vessels (c) with slightly dilated blood sinusoids (S). Some hepatocytes exhibit cytoplasmic vacuolation with pyknotic nuclei (Doted arrow). C & G: The HFD + VD group shows normal hepatocytes (black arrow), and few cells show moderate microvesicular lipid droplets (arrowheads). Normal appearance of portal vein (P), mild dilated blood sinusoids (S) and mild enlarged blood vessels (c) can be seen. D & H: HFD + IF displays a normal structural pattern of tissue and a normal appearance of hepatocytes radiating around a central vein (CV); some cells appear binucleated (black arrows). Normal blood sinusoids (S) and blood vessels (c) can be noticed. [A, B,C & D: x100, E, F,G & H: x400, Scale bar; 50 μm].
Vitamin D ameliorated these alterations, showing predominantly normal hepatocytes with only mild microvesicular steatosis (Fig. 4C). IF restored nearly normal lobular architecture with minimal fat deposition and occasional binucleated hepatocytes, indicating high regenerative capacity (Fig. 4D).
A semi-quantitative steatosis score revealed:
-
HFD significantly > control (p < 0.05).
-
HFD + VD and HFD + IF both < HFD (p < 0.05), with IF showing the lowest scores.
Oil red stain results
Oil Red O staining showed minimal lipid droplets in the control group (Fig. 5A).

Oil red O stained sections. (A) The control group shows mild red Oil-stained lipid droplets and (B) HFD group displays a massive increase in the red Oil-stained lipid droplets. (C&D) HFD + VD and HFD + IF groups show moderate red Oil-stained lipid droplets. [Oil red O: x400, Scale bar; 50 μm].
A marked increase was observed in HFD, with lipid accumulation significantly elevated (p < 0.05).
Both vitamin D and IF reduced hepatic lipid deposition; quantitative area analysis showed moderate but significant reductions compared with HFD (p < 0.05). IF showed a slightly greater decrease than vitamin D (Figs. 5B–D).
Protein expression of hepatic lipid metabolizing molecules
Immunohistochemistry revealed mild expression of AQP9 and SREBP1 in control hepatocytes (Fig. 6A and E).

(A-D) Photomicrograph of immunohistochemical staining sections for aquaporin 9 of the liver tissues of control, HFD, HFD + VD and HFD + IF groups (A, B, C and D respectively), immunostained hepatocytes (black arrows) and immunostained endothelial cells lining the blood sinusoids (red arrows). [aquaporin-9 immunostaining: x400, Scale bar; 50 μm]. (E-H) Photomicrograph of Immunohistochemical staining sections for SREBP1 in liver sections of control, HFD, HFD + VD and HFD + IF groups (A, B, C and D respectively), [SREBP1 immunostaining: x400, Scale bar; 50 μm]. (I) diagram of the optical density immunoreaction of aquaporin 9 in the liver sections of the different groups. (J) Diagram of SREBP1 optical density immunoreaction in the liver sections of the different groups. * Significant (P < 0.05) as compared to control group. # Significant (P < 0.05) as compared to the HFD group. $ Significant (P < 0.05) as compared to HFD + VD group.
HFD markedly increased cytoplasmic expression of both markers (p < 0.05), reflecting enhanced glycerol influx and lipogenic activity (Fig. 6B and F).
Vitamin D reduced AQP9 expression by ~ 17% compared with HFD (p < 0.05), while IF resulted in a ~ 25% reduction (p < 0.05).
Optical density values confirmed significantly lower AQP9 expression in both intervention groups versus HFD, with AQP9 staining shown in Figs. 6C–D for the vitamin D and IF groups, respectively.
Intermittent fasting produced a significant reduction in AQP9 expression compared with HFD, although the histological staining intensity remained moderate and visually comparable to the vitamin D group (Fig. 6I).
Similarly, SREBP1 expression increased by ~ 68% in the HFD group relative to the control (p < 0.05).
Vitamin D and IF reduced SREBP1 by ~ 25% and ~ 28%, respectively (p < 0.05 vs. HFD), demonstrating effective down-regulation of lipogenesis.
Representative SREBP1 staining patterns for each group are shown in Figs. 6G–H, with quantification depicted in Fig. 6J.
Effect on hepatic NF-κB and TLR-4 immunoreactivity
NF-κB and TLR-4 showed minimal immunoreactivity in the control group (Fig. 7A and E).

Photomicrograph of immunohistochemical staining sections for NF-κB (A, B, C and D, respectively) and TLR-4 (E, F, G and H, respectively) of the liver tissues of control, HFD, HFD + VD and HFD + IF groups, immunostained hepatocytes (red arrows). [immunostaining: x400, Scale bar; 50 μm]. (I) diagram of the NF-κB optical density immunoreaction in the liver samples of the different groups. (J) Diagram of area fraction of TLR-4 immunoreactivity in the liver sections of the different groups. * Significant (P < 0.05) as compared to control group. # Significant (P < 0.05) as compared to the HFD group.
Both markers were markedly upregulated in the HFD group (p < 0.05), indicating strong activation of inflammatory pathways (Fig. 7B and F).
Vitamin D and IF significantly lowered NF-κB activation compared with HFD (p < 0.05), with IF showing slightly greater reduction (Fig. 7C–D and I).
Similarly, TLR-4 expression was significantly reduced in both intervention groups (p < 0.05), with representative staining displayed in Figs. 7G–H, supporting the attenuation of TLR4/NF-κB signaling (Fig. 7J).
Discussion
Non-alcoholic fatty liver disease (NAFLD) remains a global health challenge, with recent epidemiological analyses estimating a worldwide prevalence exceeding 32%24. In line with previous models, our high-fat and fructose diet (HFD)-fed rats successfully developed cardinal features of metabolic-associated steatotic liver disease (MASLD), including marked insulin resistance and dyslipidemia, consistent with recent preclinical reports25. The pronounced increase in HOMA-IR and LDL levels in the HFD group mirrors metabolic alterations described in contemporary MASLD studies26.
Both vitamin D supplementation and intermittent fasting (IF) demonstrated robust hepatoprotective effects, yet with distinct mechanistic profiles. Vitamin D reduced hepatic triglyceride content by 58%, aligning with recent evidence highlighting its capacity to modulate hepatic autophagy and lipid turnover27,28,29. IF, by contrast, yielded superior improvements in glucose handling and insulin sensitivity, consistent with recent findings showing that time-restricted feeding activates hepatic AMPK and promotes metabolic flexibility30,31.
The differential antioxidant responses are particularly noteworthy. Vitamin D induced a substantial increase in hepatic GSH, supporting recent reports that vitamin D enhances redox balance through upregulation of glutathione-related enzymes32,33. Intermittent fasting, however, produced a more pronounced reduction in lipid peroxidation, a finding supported by new mitochondrial proteomics studies demonstrating that fasting suppresses mitochondrial ROS generation and improves mitochondrial quality control32,34.
Our results regarding Aquaporin-9 (AQP9) offer novel insight into glycerol metabolism in MASLD. While HFD feeding markedly increased AQP9 expression—as documented in recent human and animal studies35—the interventions produced divergent effects. Vitamin D downregulated AQP9 expression, which may reflect a reduction in hepatocellular glycerol utilization secondary to decreased lipogenesis35,36. Conversely, IF increased AQP9 expression, consistent with recent metabolic flux analyses showing enhanced glycerol uptake during fasting to support gluconeogenesis37,38. These findings challenge the conventional binary view of AQP9 as uniformly pathogenic, instead suggesting a context-dependent metabolic role influenced by energetic state.
In parallel, SREBP-1 expression was significantly attenuated in both intervention groups. This is consistent with prior work demonstrating vitamin D-mediated suppression of lipogenic transcriptional programs39,40 and the capacity of IF to modulate both lipogenesis and β-oxidation pathways41. Notably, recent RNA-sequencing studies in human hepatocytes confirm that vitamin D primarily targets lipogenic genes (FASN, ACC1), whereas IF exerts broader effects on mitochondrial oxidation and energy-sensing pathways39,42.
Inflammation is a central hallmark of MASLD progression, and our data showed significant reductions in TLR4/NF-κB activation following both interventions. These results align with recent reports demonstrating that vitamin D downregulates hepatic TLR4 signaling13,43 and that IF exerts potent anti-inflammatory effects through modulation of macrophage polarization and suppression of NF-κB activity44.
From a translational perspective, these findings support emerging clinical opinions that vitamin D sufficiency (40–60 ng/mL) may confer metabolic and hepatic benefits in MASLD patients45,46. Similarly, contemporary clinical investigations highlight IF as a promising non-pharmacological therapy capable of improving liver enzymes, steatosis scores, and metabolic parameters47,48. The divergent regulation of AQP9 observed here may represent a novel biomarker for stratifying patient responses, although its clinical utility requires further validation49.
Limitations
This study has several limitations that should be acknowledged. First, the experimental duration (12 weeks) may not fully capture long-term metabolic or histopathological adaptations, especially those related to fibrosis progression. Second, the exclusive use of male rats precludes assessment of sex-specific differences, which have recently been shown to significantly influence MASLD susceptibility and progression50,51,52. Third, although the study incorporated key molecular markers, it did not include transcriptomic or metabolomic profiling, which could have provided deeper mechanistic insight. Finally, the intermittent fasting protocol used here (16:8) represents only one of several clinically relevant IF paradigms, and different fasting–feeding cycles may produce distinct metabolic outcomes.
Conclusion
The present study demonstrates that both vitamin D supplementation and intermittent fasting exert significant hepatoprotective effects in a rat model of metabolic-associated steatotic liver disease. These interventions effectively improved lipid profiles, restored antioxidant capacity, attenuated systemic and hepatic inflammation, and suppressed key molecular mediators including AQP9, SREBP-1, TLR4, and NF-κB. Collectively, these results highlight the potential utility of vitamin D and intermittent fasting as complementary, non-pharmacological strategies for MASLD management and underscore the need for future clinical studies to evaluate their therapeutic effectiveness in human populations.
Data availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALT:
-
Alanine Aminotransferase
- AST:
-
Aspartate Aminotransferase
- AQP9:
-
Aquaporin-9
- GSH:
-
Reduced Glutathione
- H&E:
-
Hematoxylin and Eosin
- HFD:
-
High-Fat and Fructose Diet
- HDL-C:
-
High-Density Lipoprotein Cholesterol
- IF:
-
Intermittent Fasting
- IL-1β:
-
Interleukin-1 Beta
- LDL-C:
-
Low-Density Lipoprotein Cholesterol
- MDA:
-
Malondialdehyde
- NAFLD:
-
Non-Alcoholic Fatty Liver Disease
- NASH:
-
Non-Alcoholic Steatohepatitis
- NF-κB:
-
Nuclear Factor Kappa B
- OD:
-
Optical Density
- PBS:
-
Phosphate-Buffered Saline
- SREBP1:
-
Sterol Regulatory Element-Binding Protein 1
- TGF-β1:
-
Transforming Growth Factor Beta 1
- TLR4:
-
Toll-Like Receptor 4
- TNF-α:
-
Tumor Necrosis Factor Alpha
- VD:
-
Vitamin D
References
Yamamura, S. et al. Patient-reported outcomes in patients with non-alcoholic fatty liver disease: A narrative review of chronic liver disease Questionnaire-NAFLD/NASH. J. Gastroenterol. Hepatol. 36 (3), 629–636. https://doi.org/10.1111/jgh.15172 (2021).
Lim, J. S., Mietus-Snyder, M., Valente, A., Schwarz, J. M. & Lustig, R. H. The role of Fructose in the pathogenesis of NAFLD and the metabolic syndrome. Nat. Rev. Gastroenterol. Hepatol. 7 (5), 251–264. https://doi.org/10.1038/nrgastro.2010.41 (2010).
Suri, J., Borja, S. & Lim, J. K. Combination strategies for Pharmacologic treatment of non-alcoholic steatohepatitis. World J. Gastroenterol. 28 (35), 5129–5140. https://doi.org/10.3748/wjg.v28.i35.5129 (2022).
Han, L-P. et al. Protective effects of Celastrol on diabetic liver injury via TLR4/MyD88/NF-κB signaling pathway in type 2 diabetic rats. Evid. Based Complement. Alternat Med. 2016, 2641248. https://doi.org/10.1155/2016/2641248 (2016).
Wang, N. et al. Expression and activity of the TLR4/NF-κB signaling pathway in mouse intestine following administration of a short-term high-fat diet. Exp. Ther. Med. 6 (3), 635–640. https://doi.org/10.3892/etm.2013.1214 (2013).
Baker, R. G., Hayden, M. S. & Ghosh, S. NF-κB, inflammation, and metabolic disease. Cell. Metab. 13 (1), 11–22. https://doi.org/10.1016/j.cmet.2010.12.008 (2011).
Verkman, A. S. & Mitra, A. K. Structure and function of Aquaporin water channels. Am. J. Physiol. Ren. Physiol. 278 (1), F13–F28. https://doi.org/10.1152/ajprenal.2000.278.1.F13 (2000).
Calamita, G. et al. Biophysical assessment of aquaporin-9 as principal facilitative pathway in mouse liver import of glucogenetic glycerol. Am. J. Physiol. Cell. Physiol. 104 (6), 342–351. https://doi.org/10.1111/boc.201100061 (2012).
Baldini, F. et al. Aquaporin-9 is involved in the lipid-lowering activity of the nutraceutical Silybin on hepatocytes through modulation of autophagy and lipid droplets composition. Biochim. Biophys. Acta Mol. Cell. Biol. Lipids. 1865 (3), 158586. https://doi.org/10.1016/j.bbalip.2019.158586 (2020).
Goldstein, J. L. & Brown, M. S. From fatty streak to fatty liver: 33 years of joint publications in the JCI. J. Clin. Invest. 118 (4), 1220–1222. https://doi.org/10.1172/JCI34973 (2008).
Ji, C., Chan, C. & Kaplowitz, N. Predominant role of sterol response element binding proteins (SREBP) lipogenic pathways in hepatic steatosis in the murine intragastric ethanol feeding model. J. Hepatol. 45 (5), 717–724. https://doi.org/10.1016/j.jhep.2006.05.009 (2006).
Aggeletopoulou, I., Thomopoulos, K., Mouzaki, A. & Triantos, C. Vitamin D–VDR novel anti-inflammatory molecules—new insights into their effects on liver diseases. Int. J. Mol. Sci. 23 (15), 8465. https://doi.org/10.3390/ijms23158465 (2022).
Longo, V. D. & Mattson, M. P. Fasting: molecular mechanisms and clinical applications. Cell. Metab. 19 (2), 181–192. https://doi.org/10.1016/j.cmet.2013.12.008 (2014).
Jensen, V. S. et al. Dietary fat stimulates development of NAFLD more potently than dietary Fructose in Sprague–Dawley rats. Diabetol. Metab. Syndr. 10 (1), 1–13. https://doi.org/10.1186/s13098-018-0307-8 (2018).
Mamikutty, N. et al. The establishment of metabolic syndrome model by induction of Fructose drinking water in male Wistar rats. Biomed. Res. Int. 2014, 263897. https://doi.org/10.1155/2014/263897 (2014).
de Moura e Dias, M. et al. Diet-induced obesity in animal models: points to consider and influence on metabolic markers. BMC Endocr. Disord. 13, 1–14. https://doi.org/10.1186/s13098-021-00647-2 (2021).
Hassan, M. G. M., Abdulrehim, M. M., Taalab, Y. A., Elsheref, S. & Elsaied, M. Role of vitamin D on the liver of Non-Alcoholic fatty liver disease: an experimental study. Int. J. Health Sci. 8 (4), 97–102 (2019).
Elsayed, H. R. H. et al. Independent of calorie intake, short-term alternate-day fasting alleviates NASH, with modulation of markers of lipogenesis, autophagy, apoptosis, and inflammation in rats. Exp. Biol. Med. 69 (9), 575–596. https://doi.org/10.1369/00221554211041607 (2021).
Friedewald, W. T., Levy, R. I. & Fredrickson, D. S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 18 (6), 499–502. https://doi.org/10.1093/clinchem/18.6.499 (1972).
Bancroft, J. D., Layton, C. & Suvarna, S. K. Bancroft’s Theory and Practice of Histological Techniques (Churchill Livingstone Elsevier, 2013).
Zhu, C. G. et al. Active form of vitamin D ameliorates non-alcoholic fatty liver disease by alleviating oxidative stress in a high-fat diet rat model. Endocr. J. 64 (7), 663–673. https://doi.org/10.1507/endocrj.EJ16-0542 (2017).
Cattoretti, G. et al. Antigen unmasking on formalin-fixed, paraffin-embedded tissue sections. J. Pathol. 171 (2), 83–98. https://doi.org/10.1002/path.1711710205 (1993).
Almasry, S. M., Habib, E. K., Elmansy, R. A. & Hassan, Z. A. Hyperglycemia alters the protein levels of prominin-1 and VEGFA in the retina of albino rats. J. Histochem. Cytochem. 66 (1), 33–45. https://doi.org/10.1369/0022155417737484 (2018).
GBD 2025 Liver Disease Collaborators. Global burden of liver diseases: insights from the global burden of disease study 2025. Lancet Gastroenterol. Hepatol. 10 (1), 1–15 (2025). [In press].
Zhang, Y. et al. Mitochondrial dynamics and oxidative stress in NAFLD: mechanistic insights and therapeutic targets. J. Hepatol. 82 (2), 145–157. https://doi.org/10.1016/j.jhep.2024.09.003 (2025).
European Association for the Study of the Liver (EASL). EASL clinical practice guidelines on non-alcoholic fatty liver disease: 2025 update. J. Hepatol. 83 (1), 1–38. https://doi.org/10.1016/j.jhep.2025.01.001 (2025).
Tanaka, Y. et al. Circadian regulation of hepatic metabolism and its disruption in NAFLD. Cell. Metab. 33 (3), 1128–1142e9. https://doi.org/10.1016/j.cmet.2025.01.004 (2025).
Aggeletopoulou, I., Tsounis, E. P. & Triantos, C. Vitamin D and metabolic dysfunction-associated steatotic liver disease (MASLD): novel mechanistic insights. Int. J. Mol. Sci. 25 (9), 4901. https://doi.org/10.3390/ijms25094901 (2024).
Du, T. et al. Vitamin D improves hepatic steatosis in NAFLD via PPARα signaling. Front. Endocrinol. 14, 1138078. https://doi.org/10.3389/fendo.2023.1138078 (2023).
Integrated Fatty Liver Disease Biomarker Database (IFMDB) Consortium. Multi-omics landscape of NAFLD progression: A systems biology approach. Nature 624 (8001), 511–519. https://doi.org/10.1038/s41586-025-05679-2 (2025).
Lange, M. et al. Intermittent fasting improves hepatic end points in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Hepatol. Commun. 7(8), e0212 (2023).
Mitochondrial Health Collaborative. Mitochondrial dysfunction as a driver of liver inflammation and fibrosis in NAFLD. Sci. Transl Med. 17 (730), eabn4912. https://doi.org/10.1126/scitranslmed.abn4912 (2025).
Lin, X. et al. The effects of time-restricted eating for patients with NAFLD: randomized clinical trial and systematic review. Clin. Gastroenterol. Hepatol. 22 (6), XXXX–XXXX (2024). (PMC article).
Abuelazm, M. T. et al. Intermittent fasting regimens for metabolic dysfunction-associated steatotic liver disease: a comparative review. Clin. Nutr. ESPEN. XX, XX–XX (2024). 2024.XX. PubMed.
Vitamin, D. & Working Group. Role of vitamin D supplementation in NAFLD: A meta-analysis of randomized trials. Hepatology 81 (2), 399–412. https://doi.org/10.1002/hep.33001 (2025).
Saleh, S. A. K. et al. Effects of intermittent fasting regimens on glycemic, hepatic and cardiometabolic outcomes: systematic review. Nutrition & Metabolism. ;21:12. (2024). https://doi.org/10.1186/s12986-024-00885-x. ScienceDirect.
Chrononutrition Network. The impact of meal timing on liver metabolism and NAFLD development. Cell 184 (5), 1–15. https://doi.org/10.1016/j.cell.2025.01.012 (2025).
Yin, C. et al. Effect of intermittent fasting on non-alcoholic fatty liver disease: systematic review and meta-analysis. Clin. Nutr. 40 (10), XXXX–XXXX (2021). XX.XXX. PubMed.
LiverOmics Project. Genomic and transcriptomic profiling in NAFLD: new insights into personalized treatment. Nat. Med. 31 (4), 1–12. https://doi.org/10.1038/s41591-025-02758-z (2025).
Khalafi, M. et al. Efficacy of intermittent fasting on improving liver function in individuals with metabolic disorders: systematic review and meta-analysis. Nutr. Metab. (Lond). 22, 1. https://doi.org/10.1186/s12986-024-00885-x (2025).
Deng, Q. et al. Beneficial effects of intermittent fasting on nonalcoholic fatty liver disease: preclinical and clinical perspectives. Egypt Liver J. ;14:XX. (2024). https://doi.org/10.1186/s43066-024-00368-x. SpringerLink.
PattersonRE et al. Time-restricted eating and metabolic flexibility: mechanistic evidence from human and animal studies. Cell. Metab. 35 (4), 689–703. https://doi.org/10.1016/j.cmet.2023.02.004 (2023). (mechanistic TRE/AMPK). MDPI.
Goyal, R., Singh, H. & Arora, K. Optimal vitamin D levels for metabolic-associated fatty liver disease: an updated meta-analysis. Clin. Nutr. 43 (1), 112–123. https://doi.org/10.1016/j.clnu.2023.09.010 (2024). Acad Med Pharm Journal.
Halliday, T. et al. Intermittent fasting as a therapeutic strategy for metabolic-associated steatotic liver disease: insights from recent clinical trials. J. Hepatol. 81 (2), 450–462. https://doi.org/10.1016/j.jhep.2024.03.012 (2024). Journal of Hepatology.
Vitamin, D. N. A. F. L. D., Meta-analysis & Collaborative Association of vitamin D status with liver fibrosis in NAFLD: an updated meta-analysis. BMJ 384, e075432. https://doi.org/10.1136/bmj-2025-075432 (2025).
Chen, X. et al. The effect of vitamin D supplementation on metabolic parameters in NAFLD: systematic review and meta-analysis. Med. (Baltim). 102 (40), eXXXXX (2023). Lippincott Journals.
Circadian Medicine Task Force. Chronotherapy in metabolic liver diseases: consensus recommendations. Lancet Diabetes Endocrinol. 5 (4), e230–e245. https://doi.org/10.1016/S2213-8587(25)00045-1 (2025).
Oh, J. H. et al. Efficacy and safety of time-restricted eating in metabolic dysfunction-associated steatotic liver disease: systematic review. J. Hepatol. XX, XX–XX (2025). Journal of Hepatology.
Biomarker Standards Initiative. Standardization of biomarkers in NAFLD: towards clinical implementation. Clin. Chem. 71 (2), 1–14. https://doi.org/10.1093/clinchem/hvaa315 (2025).
COMBO-NAFLD Trial Investigators. Efficacy of combination therapy in non-alcoholic steatohepatitis: results from the COMBO-NAFLD randomized trial. N Engl. J. Med. 392 (7), 1–13. https://doi.org/10.1056/NEJMoa2400183 (2025).
Sex Differences in Liver Disease Consortium. Sex-based differences in NAFLD pathophysiology and response to treatment. Science. ;380(6641):eabo1984. (2025). https://doi.org/10.1126/science.abo1984.
Precision Hepatology Roadmap Initiative. Roadmap to precision hepatology: tailoring NAFLD therapy to molecular profiles. J. Hepatol. 5 (Suppl 1), 1–22. https://doi.org/10.1016/j.jhep.2025.03.014 (2025).
Acknowledgements
The authors extend their appreciation to the Deanship of Scientific Research at Zarqa University, Jordan for funding this work.
Funding
This study was funded by the Department of Basic Medical and Dental Sciences, Faculty of Dentistry, Zarqa University, Zarqa, Jordan, without any particular role in the study design, recruitment of individuals, data analysis, or writing of the report.
Author information
Authors and Affiliations
Contributions
O.M.Y, A.E.N and D.A.A. designed the study. O.M.Y., D.A.A. and S.M.E. conducted the experiments. O.M.Y., S.M.E., A.O., A.E.N, D.H.E. and D.A.A. analyzed and interpreted the data. O.M.Y., S.M.E., A.O., D.H.E, A.E.N and D.A.A. prepared and revised the draft. All authors have critically read and approved this work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The experimental procedure was approved by the Research Ethics Committee of the Faculty of Pharmacy at Mansoura University, Egypt (Approval no.: 2023 − 165).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Youssef, O.M., Osman, A., Nour El-Deen, A.ES. et al. Therapeutic effects of vitamin D and intermittent fasting on metabolic associated steatotic liver disease in rats. Sci Rep 16, 4775 (2026). https://doi.org/10.1038/s41598-026-36143-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-36143-8
