
Abstract
Identifying reliable prognostic markers is crucial for the effective management of chronic obstructive pulmonary disease (COPD). The platelet count has emerged as a potential inflammatory marker associated with clinical outcomes. The aim of this study was to investigate the relationships of the platelet count with all-cause mortality and readmission rates among patients with acute exacerbations of COPD (AECOPD). Patients who were diagnosed with AECOPD between January 2019 and December 2023 at our institution were included. The platelet count was recorded on admission. The primary outcome was all-cause mortality. The secondary outcomes included readmission for AECOPD and a composite endpoint of readmission and mortality. Multivariate Cox proportional hazards models were constructed to examine the associations between the study endpoints and platelet counts categorized as low, normal, and high (< 150, ≥ 150 to < 300, and ≥ 300 × 109/L, respectively). Additionally, restricted cubic spline (RCS) Cox regression was used to explore the dose‒response relationships of the platelet count with all-cause mortality and readmission. A total of 853 patients (mean age = 71.39 years; proportion of males = 58.7%) were ultimately included. After a follow-up of 48 (33–58) months, 163 deaths (19.1%) occurred among the cohort. The 5-year survival estimates were 67.5%, 81.2%, and 59.3% for the low, normal, and high platelet count groups, respectively (log-rank, P < 0.001). Similarly, the rate of readmission among patients with normal platelet counts was significantly lower than that in either the high or low platelet count groups (log-rank, P < 0.001). After adjusting for potential confounders, both low and high platelet counts in patients with AECOPD were found to be significantly associated with an increased risk of all-cause mortality and readmission. The RCS curves revealed U-shaped relationships of the platelet count with all-cause mortality and readmission in patients with AECOPD, with the lowest risk observed at a platelet count of approximately 200 × 10⁹/L for both outcomes. We observed U-shaped relationships of the platelet count with all-cause mortality and readmission in individuals with COPD. These findings may provide a simple approach for risk discrimination for adverse outcomes in patients with COPD.
Similar content being viewed by others

Introduction
Chronic obstructive pulmonary disease (COPD) is a pulmonary disease characterized by chronic airflow limitation. Globally, it affects approximately 212.3 million individuals, leading to 3.3 million deaths and resulting in 74.4 million disability-adjusted life years in 20191. COPD is projected to become the third leading cause of death by 2030, representing 8.6% of global deaths2. The chronic systemic inflammation associated with COPD has been closely linked to adverse clinical outcomes, including increased exacerbation frequency, reduced quality of life, and higher mortality rates3. This inflammation contributes to the pathophysiology of the disease, underscoring the importance of identifying reliable prognostic markers that can inform treatment strategies.
Given the systemic nature of the inflammatory response in COPD, identifying accessible blood-based biomarkers is crucial for clinical utility. Platelets have long been recognized for their critical roles in hemostasis and thrombosis; however, their involvement in inflammatory processes has gained increasing attention in the medical community4,5,6. This shift in focus underscores the complex and multifaceted functions of platelets beyond their traditional hemostatic activities. Platelet count is a standard parameter routinely assessed through complete blood count (CBC) analysis7. This metric serves as a vital indicator of a patient’s inflammatory status and overall health. Abnormalities in platelet levels—whether elevated (thrombocytosis) or decreased (thrombocytopenia)—have been linked to a wide range of adverse health outcomes across various patient populations. For instance, elevated platelet counts have been associated with poorer prognoses in conditions such as cancer, infections, sepsis, critical illness, and end-stage renal disease8,9,10,11. Furthermore, a U-shaped relationship between the platelet count and mortality has been observed in the general population, as well as among elderly and postmenopausal women12,13,14. In these contexts, high platelet counts may reflect underlying inflammatory processes or increased thrombotic risk, both of which can complicate patient management.
Previous studies have shown that the presence of thrombocytosis, measured during acute exacerbations of COPD (AECOPD), is associated with an increased risk of both in-hospital and 1-year mortality15. This correlation underscores the potential role of platelets as markers of systemic inflammation and disease severity in COPD. In the context of AECOPD, elevated platelet counts may reflect underlying inflammatory processes that exacerbate respiratory distress and lead to worse outcomes. Conversely, thrombocytopenia—defined as a decreased platelet count—has also been linked to adverse outcomes in AECOPD patients. Research indicates that lower platelet counts are associated with in-hospital mortality, a heightened need for mechanical ventilation, admission to intensive care units, and extended hospital stays16. The presence of thrombocytopenia may indicate severe systemic illness, increased risk of bleeding complications, and potentially a poorer overall prognosis. In addition, Fawzy et al. suggested that in patients with stable COPD, the platelet count has a U-shaped association with an increased risk of 3-year all-cause mortality17. However, the precise platelet count thresholds above or below which mortality risk increases remain undefined. Furthermore, the relationship between the platelet count measured in COPD patients and readmission rates has not been previously explored.
Despite these insights, significant gaps remain in the literature. Specifically, the precise platelet count thresholds that correlate with increased mortality risk in COPD patients have not yet been clearly defined. Additionally, the relationship between platelet count and hospital readmission rates within this population remains unexplored. Therefore, this study aimed to elucidate the relationships between platelet count, all-cause mortality, and readmission rates in patients with AECOPD. Investigating these aspects could provide valuable information for clinicians seeking to enhance patient outcomes and optimize management strategies in COPD.
Materials and methods
Patient enrollment
This was a retrospective cohort study of consecutive patients admitted with AECOPD to Youyang Hospital, the First Affiliated Hospital of Chongqing Medical University, between January 2019 and December 2023. Patients were included in this study if they met the following criteria: a primary diagnosis of AECOPD and a diagnosis of COPD confirmed by spirometry during stable periods. The diagnosis of COPD was established by a pulmonary specialist based on the patient’s smoking history, clinical evaluation, and pulmonary function testing, which revealed airflow obstruction, even after bronchodilator administration (with a forced expiratory volume in 1 s (FEV1)-to-forced vital capacity (FVC) ratio of less than 0.70)18. AECOPD is defined as an acute worsening of respiratory symptoms, including dyspnea, cough, and changes in sputum volume or purulence, resulting in additional treatments18. In cases where a patient had been admitted to the hospital multiple times, only the first admission was recorded. The exclusion criteria were age < 40 years; airway disease primarily due to other causes (lung cancer, interstitial lung disease, asthma, bronchiectasis); and severe cardiovascular disease, including acute left heart failure, septic shock and diseases of the blood system.
This study conformed to the principles of the Declaration of Helsinki19. The study protocol was reviewed and approved by the Ethics Committee of Youyang Hospital, which is affiliated with the First Affiliated Hospital of Chongqing Medical University (Approval No.: 2024YYXRMYY11). Informed consent was waived due to the retrospective nature by the Ethics Committee of Youyang Hospital.
Data collection
We collected demographic and clinical data from electronic medical records, including sex, age, body mass index (BMI), smoking history (defined as continuous or cumulative smoking for more than six months), and comorbidities, and we collected samples for measuring blood counts and other inflammatory parameters at the time of admission (before administering antibiotics and steroids). Long-term inhalation drugs (defined as drugs inhaled for more than six months), including inhaled long-acting beta-agonists (LABAs) and inhaled corticosteroids (ICSs), can be used. Spirometry parameters, including the FEV1 and the FEV1/FVC ratio, were collected from the most recent stable period within the past two years.
Platelet count
Platelet counts were determined by conducting a complete blood count on blood samples via a Beckman Coulter automated blood analyzer in an MEC, expressed as × 109 cells/L. Only the baseline platelet count was used in this analysis to avoid survivorship bias and ensure that the platelet count was not affected by competing outcomes. On the basis of platelet count, the enrolled patients were further divided into three categories of low platelet count (< 150 × 109/L), normal platelet count (≥ 150 to < 300 × 109/L), and high platelet count (≥ 300 × 109/L). This classification follows the standard clinical definition of thrombocytopenia and the platelet count threshold identified in previous reports, which indicate an increased mortality risk in stable COPD patients and in the general population14,17.
Handling of missing values
In the dataset, there were missing values for prothrombin time (PT, n = 5), the international normalized ratio (INR, n = 5), D-dimer (n = 12), hemoglobin (Hb, n = 10), albumin (ALB, n = 9), brain natriuretic peptide (BNP, n = 22), total cholesterol (TC, n = 34), low-density lipoprotein cholesterol (LDL-c, n = 34), serum creatinine (SCr, n = 6), blood urea nitrogen (BUN, n = 6), high-sensitivity C-reactive protein (hs-CRP, n = 39), the partial pressure of carbon dioxide (PCO2, n = 40), and the left ventricular ejection fraction (LVEF, n = 52). We performed imputation of missing values via the R package RandomForest20.
Outcomes
In the present study, we hypothesized that the platelet level was an independent risk factor for all-cause mortality in AECOPD patients. Our primary outcome was all-cause mortality, whereas secondary outcomes included readmission for AECOPD and a composite outcome of readmission or all-cause mortality. The date of death was obtained with a detailed review of all available electronic medical records and telephone interviews with the patients’ next-of-kin reports.
Statistical analysis
Statistical analysis was performed via IBM SPSS version 25.0 (IBM SPSS Statistics, Armonk, NY, USA), R version 4.4.1 (Free Software Foundation Inc.), and GraphPad Prism 9.0. The results are presented as the means ± standard deviations for normally distributed continuous variables or as or median values plus interquartile ranges for skewed-distributed continuous data and absolute numbers with percentages for categorical variables. The baseline characteristics were compared via one-way analysis of variance or the Kruskal–Wallis test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. We used the Kaplan‒Meier method to assess the cumulative survival rate of AECOPD patients and the log-rank test to compare the differences in survival rates among the three groups21. Cox proportional hazards regression in a forward stepwise procedure was used to calculate the hazard ratios (HRs) and 95% confidence intervals (CIs) for all-cause mortality, readmission, and all-cause death or readmission. To visualize the associations between the platelet count and all-cause mortality as well as readmission in patients with AECOPD, restricted cubic splines (RCS) were constructed on the basis of the fully adjusted Cox model. On the basis of the results of RCS analysis, we subsequently determined the optimal threshold and conducted threshold analysis via two-piecewise Cox regression to explore the relationships between the platelet count and the endpoints22. A P value less than 0.05 was considered to indicate statistical significance.
Sample size and power analysis
As this was a retrospective cohort study, the sample size was determined by the number of eligible patients identified during the study period. Nevertheless, a post-hoc power analysis was conducted using PASS 2023. Based on the observed mortality difference between the normal platelet group and the high platelet group, the required sample size was estimated at approximately 65 patients per group under a conservative calculation method with continuity correction. Using the actual group sizes in our dataset (605 vs. 94 patients), the achieved statistical power was approximately 98%, indicating that the available sample size was sufficient to detect the observed effect size.
Results
Baseline characteristics of the enrolled participants
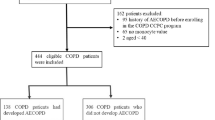
A total of 2340 patients with acute exacerbation of COPD at our hospital were included from January 2019 to December 2023. According to the inclusion and exclusion criteria, 1487 patients were excluded from this study, and 853 patients were ultimately included (Fig. 1). The demographic and clinical characteristics of the 853 patients according to platelet count are presented in Table 1. The average age was 71.39 ± 10.18 years, 501 were male (58.7%), and 293 had a history of smoking (34.3%). Among the 853 enrolled AECOPD patients, 154 had a low platelet count (18.0%), 605 had a normal platelet count (71.0%), and 94 had a high platelet count (11.0%). Patients with a low platelet count were more likely to be male and smokers, have atrial fibrillation, and have NYHA class III/IV symptoms than those with a high platelet count. Conversely, compared with those with a low platelet count, patients with a high platelet count were more likely to have hyperlipidemia and greater PT, prothrombin activity (PTA), TC levels, and LDL-C levels. The hs-CRP levels and white blood cell (WBC) counts were significantly greater in the high platelet count group. Moreover, compared with the other participants, those with a low platelet count had a greater INR, activated partial thromboplastin time (APTT), D-dimer level, aspartate transaminase (AST) level, BUN level, SCr level, and Hb level. No significant differences were found among the three groups regarding FEV1 or FEV1/FVC ratios.

Flow diagram for inclusion and analysis of exacerbation of chronic obstructive pulmonary disease (AECOPD) patients.
Platelet count and clinical outcomes
Kaplan–Meier survival curves were generated to analyze the incidence of outcomes among the groups (Fig. 2). After a follow-up of 48 (33–58) months, 163 deaths (19.1%) occurred among the cohort (Supplementary Table 1). The 5-year survival estimates were 81.2% for patients with normal platelet counts, 67.5% for those with low platelet counts, and 59.3% for those with high platelet counts. Compared with those with a normal platelet count, patients with a low or high platelet count showed a decreased survival probability (P < 0.001 in the log-rank test) (Fig. 2A). Readmission for AECOPD among patients with normal platelet counts was also significantly lower than that for those with high or low platelet counts (P < 0.001; Fig. 2B). Similarly, the composite outcome of readmission or all-cause mortality was lowest in the normal platelet count group (p < 0.001; Fig. 2C).

Kaplan-Meier graphs for primary and secondary outcomes. (A). Kaplan-Meier graph of mortality; (B). Kaplan-Meier graph of all-cause readmission, (C). Kaplan-Meier graph of death or readmission.
The HRs for all outcomes calculated via Cox multivariate analysis are presented in Table 2. After adjusting for potential confounders including age, hypertension, AF, NYHA class III/IV symptoms, malignant tumors, antiplatelet agents, lipid-lowering drugs, anticoagulation agents, antibiotics, fibrinogen (FBG), the INR, and fibrin degradation products (FDP), both low and high platelet counts were strongly associated with an increased risk of adverse events. Compared with the normal platelet count subgroup, the adjusted HRs of all-cause mortality were 1.82 (95% CI 1.25 to 2.64, P = 0.002) in the low platelet count subgroup and 2.36 (95% CI 1.57 to 3.55, P < 0.001) in the high platelet count subgroup. Similarly, the adjusted HRs for readmission were 1.40 (95% CI 1.07 to 1.83, P = 0.016) for low platelet counts and 1.83 (95% CI 1.36 to 2.47, P < 0.001) for high platelet counts. This U-shaped relationship remained consistent for the composite outcome of readmission or all-cause mortality (Low platelet group: HR 1.53, 95% CI 1.10 to 2.13, P = 0.013; High platelet group: HR 1.92, 95% CI 1.48 to 2.49, P < 0.001) (Supplementary Table 2, Supplementary Figs. 1–3).
Association of platelet count with mortality
After adjusting for age, sex, BMI, laboratory test results, and the presence of comorbidities, the RCS curves revealed a U-shaped association between the platelet count and outcomes, with thresholds of 198.449 × 109/L and 200.295 × 109/L (both P values for nonlinear < 0.001; Fig. 3A-B). These findings indicate that before and after the cutoff point, the platelet count is distinctly associated with the outcomes. Furthermore, the two-piecewise linear regression revealed that the risk of all-cause mortality decreased to a minimum at a platelet count of 198.449 × 109/L and then increased with increasing platelet counts [HR (95% CI): 0.87 (0.82–0.97), 1.06 (1.03–1.08) per 10 × 109/L increase in platelet count to less or more than 198.449 × 109/L, respectively]. Similarly, the risk of all-cause readmission decreased with increasing platelet count to 200.295 × 109/L and then increased with increasing platelet count [HR (95% CI): 0.86 (0.82–0.91), 1.06 (1.03–1.08) per 10 × 109/L increase in platelet count to less or more than 200.295 × 109/L, respectively] (Table 2). Therefore, U-shaped associations of the platelet count with all-cause mortality and readmission were detected, with the nadir for mortality occurring at a platelet count of 198.449 × 109/L and that for readmission at 200.295 × 109/L, suggesting an optimal range around 200 × 10⁹/L.

The U-shaped associations of the platelet count with all-cause mortality and readmission.
Discussion
In the present study, we demonstrated a U-shaped association between platelet count and the risk of all-cause mortality and readmission in patients with AECOPD. Both low and high platelet counts were independent predictors of adverse outcomes, with the nadir of risk observed at a platelet count of approximately 200 × 10⁹/L. These findings highlight the platelet count as a simple, readily available prognostic marker in this patient population.
COPD plays a significant role in global morbidity and mortality rates, typified by progressive airflow restriction and persistent respiratory symptoms, imposing a heavy economic burden on patients, families and society1,23. Therefore, identifying easily accessible and technically undemanding markers that are associated with mortality in COPD patients becomes essential for reducing disease burden and mortality rates. Blood-based biomarkers are advantageous because they are less invasive and they are reproducible. Inflammatory biomarkers, such as CRP, FBG, IL-6, IL-8, and WBCs, reflect systemic inflammation and are linked to COPD severity and exacerbation risk24. Consequently, there remains considerable interest in the use of routine biomarkers to identify COPD patients at risk for mortality.
The lung is an important site for platelet biogenesis by extramedullary megakaryocytes25. The contribution of the lungs to platelet biogenesis is substantial, accounting for approximately 50% of total platelet production, which equates to approximately 10 million platelets per hour26. A meta-analysis combining both the SPIROMICS and COPDGene studies suggested that thrombocytosis was associated with increased odds of having AECOPD or severe AECOPD during the prior year, increased dyspnea, poorer health status, and worse respiratory-specific quality of life27. In a study involving patients with stable COPD, platelet counts were significantly greater than those of healthy controls and were not influenced by smoking habits28. Although our study concentrated on hospitalized AECOPD patients, the observed U-shaped relationship between platelet count and mortality is consistent with findings in stable COPD populations17. Notably, our cohort exhibited a lower smoking prevalence compared to commonly reported COPD populations, which may reflect regional epidemiological differences. None of the female participants (41.3% of the cohort) reported smoking, which is consistent with historically low smoking rates among older women in rural China29. This observation aligns with growing evidence that non-smoking-related COPD accounts for a significant proportion of cases in regions with high exposure to biomass fuel combustion and environmental pollutants30. In rural Southwest China, where the household use of biomass fuels (e.g., wood, crop residues) for cooking and heating is widespread, prolonged exposure to indoor air pollution likely contributes to the development of COPD independent of smoking status31. The consistency of this U-shaped relationship underscores the potential universality of platelet count as a prognostic marker in COPD, regardless of exacerbation status. Nevertheless, future research should validate these associations in larger COPD cohorts, encompassing both stable and exacerbated patients.
Platelets serve as the primary cellular mediators of hemostasis and thrombosis32. Recent studies have also suggested that platelets play significant roles as immune and inflammatory cells33. First, platelet granules store and secrete various bioactive substances, including adhesion proteins, growth factors, chemokines, cytokine-like factors, and coagulation factors, which promote the recruitment of more platelets and leukocytes6,34. Furthermore, platelets contribute to the development of inflammation by interacting with leukocytes, endothelial cells, and the subendothelial matrix5,6. Consequently, an elevated platelet count at baseline may exacerbate the inflammatory state, which is believed to lead to poorer clinical outcomes35. Under pathological conditions, platelets can become positively primed, attaining a preactivated state. In the inflamed vessel wall, platelets interact with leukocytes and the coagulation system, facilitating interactions that mediate thromboinflammation. The levels of CD47 and P-selectin, which serve as markers of platelet activation, increase significantly during AECOPD. This observation suggests that platelet activation occurs in AECOPD and indicates that platelets, as a type of inflammatory cell, play a role in the pathophysiology of the disease36. Elevated platelet levels have been shown to be associated with significantly elevated CRP, implying that systemic inflammation may play a role in the pathway between platelet elevation and COPD morbidity27. However, it remains unclear whether COPD triggers reactive thrombocytosis, leading to inflammation, or if systemic inflammation precedes reactive thrombocytosis and COPD.
Platelets are not only associated with inflammation related to COPD but also play a crucial role in mediating the development of pulmonary vascular microthrombosis. Spherization of red blood cells has been observed in COPD patients, which induces an increase in the mean square displacement of platelets, thereby promoting their adhesion, aggregation, and activation at the vessel wall37. Studies have demonstrated endothelial dysfunction, intimal thickening, and reduced and narrowed vasculature in COPD patients, all of which contribute to platelet rolling and aggregation38,39. COPD is often accompanied by hypoxemia. Notably, platelets obtained from patients with COPD presented significantly higher levels of HIF-2α and PAI-1 than those obtained from healthy individuals. These findings offer a molecular basis for the thrombogenic phenotype observed in COPD. Additionally, platelets play a role in angiogenesis, maintaining vascular integrity, and releasing vasoactive substances40.
Limitations
Our study has several limitations. First, the all-cause mortality rate of 19.1% during a median follow-up of 48 months is lower than rates reported in some prior studies41. This may relate to our retrospective, single-center design, though we screened a large number of medical records. Second, a major limitation is the unavailability of data on cause-specific deaths. Third, although we have clearly demonstrated that platelet counts exhibit a U-shaped association with mortality and readmission, the mechanisms underlying this relationship remain unclear. The identified optimal cutoff points from RCS were statistically derived and not intended as a single dichotomous threshold for clinical decision-making. Future prospective studies should validate these cutoff points and assess their clinical utility in risk prediction models, as they may vary across different patient cohorts. Therefore, the relationship between the platelet count and COPD outcomes should be considered exploratory rather than causal. Finally, it is yet to be determined whether the treatment of thrombocytopenia or thrombocytosis has any effect on patient outcomes.
Conclusion
A U-shaped relationship of the platelet count with all-cause mortality and readmission was detected in patients with COPD. These findings suggest that the platelet count, a routinely measured clinical assay, may serve as an important biomarker associated with COPD outcomes, potentially aiding in the classification of disease severity and the determination of treatment intensity.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- AECOPD:
-
Acute exacerbation of chronic obstructive pulmonary disease
- RCS:
-
Restricted cubic splines
- BMI:
-
Body mass index
- LABA:
-
Long-acting beta-agonist
- ICS:
-
Inhaled corticosteroid
- FEV1:
-
Forced expiratory volume in the first second
- FEV1/FVC:
-
The ratio of FEV1 to forced vital capacity
- PT:
-
Prothrombin time
- INR:
-
International normalized ratio
- D-D:
-
D-dimer
- Hb:
-
Hemoglobin
- ALB:
-
Albumin
- BNP:
-
Brain natriuretic peptide
- TC:
-
Total cholesterol
- LDL-c:
-
Low-density lipoprotein cholesterol
- Scr:
-
Serum creatinine
- BUN:
-
Blood urea nitrogen
- hs-CRP:
-
High-sensitivity C-reactive protein
- PCO2:
-
Partial pressure of carbon dioxide
- LVEF:
-
Left ventricular ejection fraction
- HRs:
-
Hazard ratios
- CI:
-
Confidence interval
- PTA:
-
Prothrombin activity
- WBC:
-
White blood cell
- APTT:
-
Activated partial thromboplastin time
- AST:
-
Aspartate transaminase
- AF:
-
Atrial fibrillation
- FBG:
-
Fibrinogen
- FDP:
-
Fibrinogen degradation products
References
Safiri, S. et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the global burden of disease study 2019. BMJ (Clinical Res. ed). 378, e069679. https://doi.org/10.1136/bmj-2021-069679 (2022).
Prevalence and attributable health burden of chronic respiratory diseases. 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 8 (6), 585–596. https://doi.org/10.1016/S2213-2600(20)30105-3 (2020).
Agustí, A. et al. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. 7 (5), e37483. https://doi.org/10.1371/journal.pone.0037483 (2012).
Furie, B. & Furie, B. C. Thrombus formation in vivo. J. Clin. Invest. 115 (12), 3355–3362 (2005).
Tabuchi, A. & Kuebler, W. M. Endothelium-platelet interactions in inflammatory lung disease. Vascul Pharmacol. 49 (4–6), 141–150. https://doi.org/10.1016/j.vph.2008.06.004 (2008).
Gawaz, M., Langer, H. & May, A. E. Platelets in inflammation and atherogenesis. J. Clin. Invest. 115 (12), 3378–3384 (2005).
Bessman, J. D. Evaluation of automated whole-blood platelet counts and particle sizing. Am. J. Clin. Pathol. 74 (2), 157–162 (1980).
Mirsaeidi, M. et al. Thrombocytopenia and thrombocytosis at time of hospitalization predict mortality in patients with community-acquired pneumonia. Chest 137 (2), 416–420. https://doi.org/10.1378/chest.09-0998 (2010).
Suppiah, R. et al. Thrombocytosis as a prognostic factor for survival in patients with metastatic renal cell carcinoma. Cancer 107 (8), 1793–1800 (2006).
Hui, P., Cook, D. J., Lim, W., Fraser, G. A. & Arnold, D. M. The frequency and clinical significance of thrombocytopenia complicating critical illness: a systematic review. Chest 139 (2), 271–278. https://doi.org/10.1378/chest.10-2243 (2011).
Xu, Y., Jin, X., Shao, X., Zheng, F. & Zhou, H. Valuable prognostic indicators for severe burn sepsis with inhalation lesion: age, platelet count, and procalcitonin. Burns Trauma. 6, 29. https://doi.org/10.1186/s41038-018-0132-1 (2018).
Tsai, M-T., Chen, Y-T., Lin, C-H., Huang, T-P. & Tarng, D-C. U-shaped mortality curve associated with platelet count among older people: a community-based cohort study. Blood 126 (13), 1633–1635. https://doi.org/10.1182/blood-2015-06-654764 (2015).
Kabat, G. C. et al. Platelet count and total and cause-specific mortality in the women’s health initiative. Ann. Epidemiol. 27 (4), 274–280. https://doi.org/10.1016/j.annepidem.2017.02.001 (2017).
Vinholt, P. J. et al. Platelet count is associated with cardiovascular disease, cancer and mortality: A population-based cohort study. Thromb. Res. 148, 136–142. https://doi.org/10.1016/j.thromres.2016.08.012 (2016).
Harrison, M. T. et al. Thrombocytosis is associated with increased short and long term mortality after exacerbation of chronic obstructive pulmonary disease: a role for antiplatelet therapy? Thorax 69 (7), 609–615. https://doi.org/10.1136/thoraxjnl-2013-203996 (2014).
Rahimi-Rad, M. H., Soltani, S., Rabieepour, M. & Rahimirad, S. Thrombocytopenia as a marker of outcome in patients with acute exacerbation of chronic obstructive pulmonary disease. Pneumonol Alergol Pol. 83 (5), 348–351. https://doi.org/10.5603/PiAP.2015.0056 (2015).
Fawzy, A. et al. Association of platelet count with all-cause mortality and risk of cardiovascular and respiratory morbidity in stable COPD. Respir Res. 20 (1), 86. https://doi.org/10.1186/s12931-019-1059-1 (2019).
Global Initiative for Chronic Obstructive Lung. Global strategy for diagnosis, management, and prevention of COPD;. Accessed January 1. (2022). https://goldcopd.org/
World Medical Association. Declaration of helsinki: ethical principles for medical research involving human subjects. JAMA 310 (20), 2191–2194. https://doi.org/10.1001/jama.2013.281053 (2013).
Kess, T. et al. A migration-associated supergene reveals loss of biocomplexity in Atlantic Cod. Sci. Adv. 5 (6), eaav2461. https://doi.org/10.1126/sciadv.aav2461 (2019).
Jager, K. J., van Dijk, P. C., Zoccali, C. & Dekker, F. W. The analysis of survival data: the Kaplan-Meier method. Kidney Int. 74 (5), 560–565. https://doi.org/10.1038/ki.2008.217 (2008).
Yu, X., Cao, L. & Yu, X. Elevated cord serum manganese level is associated with a neonatal high ponderal index. Environ. Res. 121, 79–83. https://doi.org/10.1016/j.envres.2012.11.002 (2013).
Kim, J. et al. Association between chronic obstructive pulmonary disease and gastroesophageal reflux disease: a National cross-sectional cohort study. BMC Pulm Med. 13, 51. https://doi.org/10.1186/1471-2466-13-51 (2013).
Su, B. et al. Inflammatory markers and the risk of chronic obstructive pulmonary disease: A systematic review and Meta-Analysis. PLoS One. 11 (4), e0150586. https://doi.org/10.1371/journal.pone.0150586 (2016).
Johnston, I., Hayes, V. & Poncz, M. Threading an elephant through the eye of a needle: where are platelets made? Cell. Res. 27 (9), 1079–1080. https://doi.org/10.1038/cr.2017.65 (2017).
Lefrançais, E. et al. The lung is a site of platelet biogenesis and a reservoir for Haematopoietic progenitors. Nature 544 (7648), 105–109. https://doi.org/10.1038/nature21706 (2017).
Fawzy, A. et al. Association of thrombocytosis with COPD morbidity: the SPIROMICS and COPDGene cohorts. Respir Res. 19 (1), 20. https://doi.org/10.1186/s12931-018-0717-z (2018).
Biljak, V. R. et al. Platelet count, mean platelet volume and smoking status in stable chronic obstructive pulmonary disease. Platelets 22 (6), 466–470. https://doi.org/10.3109/09537104.2011.573887 (2011).
Chen, Z. et al. China kadoorie biobank of 0.5 million people: survey methods, baseline characteristics and long-term follow-up. Int. J. Epidemiol. 40 (6), 1652–1666. https://doi.org/10.1093/ije/dyr120 (2011).
Smith, M. et al. Prevalence and correlates of airflow obstruction in ∼317,000 never-smokers in China. Eur. Respir J. 44 (1), 66–77. https://doi.org/10.1183/09031936.00152413 (2014).
Liu, S. et al. Biomass fuels are the probable risk factor for chronic obstructive pulmonary disease in rural South China. Thorax 62 (10), 889–897 (2007).
Hvas, A-M. Platelet function in thrombosis and hemostasis. Semin Thromb. Hemost. 42 (3), 183–184. https://doi.org/10.1055/s-0036-1572329 (2016).
Morrell, C. N., Aggrey, A. A., Chapman, L. M. & Modjeski, K. L. Emerging roles for platelets as immune and inflammatory cells. Blood 123 (18), 2759–2767. https://doi.org/10.1182/blood-2013-11-462432 (2014).
Breitenstein, A., Tanner, F. C. & Lüscher, T. F. Tissue factor and cardiovascular disease: quo vadis? Circ. J. 74 (1), 3–12. https://doi.org/10.1253/circj.cj-09-0818 (2010).
Nikolsky, E. et al. Impact of baseline platelet count in patients undergoing primary percutaneous coronary intervention in acute myocardial infarction (from the CADILLAC trial). Am. J. Cardiol. 99 (8), 1055–1061 (2007).
Pan, L., Yang, Y. & Dong, D. [Integrin-associated proteins in blood plasma of patients with acute exacerbation of chronic obstructive pulmonary disease]. Zhonghua Jie He He Hu Xi Za Zhi. 33 (4), 265–267 (2010).
Zouaoui Boudjeltia, K. et al. Spherization of red blood cells and platelet margination in COPD patients. Ann. N Y Acad. Sci. 1485 (1), 71–82. https://doi.org/10.1111/nyas.14489 (2021).
Peinado, V. I. et al. Endothelial dysfunction in pulmonary arteries of patients with mild COPD. Am. J. Physiol. 274 (6), L908–L913. https://doi.org/10.1152/ajplung.1998.274.6.L908 (1998).
Barberà, J. A. et al. Pulmonary vascular abnormalities and ventilation-perfusion relationships in mild chronic obstructive pulmonary disease. Am. J. Respir Crit. Care Med. 149 (2 Pt 1), 423–429 (1994).
Chaurasia, S. N. et al. Platelet HIF-2α promotes thrombogenicity through PAI-1 synthesis and extracellular vesicle release. Haematologica 104 (12), 2482–2492. https://doi.org/10.3324/haematol.2019.217463 (2019).
Naeem, S. et al. Mapping the global distribution, risk factors, and Temporal trends of COPD incidence and mortality (1990–2021): ecological analysis. BMC Med. 23 (1), 210. https://doi.org/10.1186/s12916-025-04014-0 (2025).
Funding
This study was supported by the Youyang Hospital of The First Affiliated Hospital of Chongqing Medical University (no. 2024YY760005).
Author information
Authors and Affiliations
Contributions
SW and LJ gave substantial contributions to the study design and manuscript revisions. JR and YR were responsible for the data analyses and manuscript draft. YZ, LP, BY, XR, and HD contributed to the data collection and follow-up. All the authors have read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study protocol was reviewed and approved by the Ethics Committee of Youyang Hospital, a Branch of The First Affiliated Hospital of Chongqing Medical University (Approval No.: 2024YYXRMYY11). Informed consent was waived due to the retrospective nature by the Ethics Committee of Youyang Hospital.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ran, J., Ran, Y., Ran, Y. et al. Platelet count has a U-shaped association with all-cause mortality in COPD patients. Sci Rep 16, 5341 (2026). https://doi.org/10.1038/s41598-026-36268-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-36268-w
