
Abstract
Outdoor activity is known to protect against childhood myopia, particularly in school-aged children. However, limited evidence exists regarding how reduced outdoor exposure influences refractive development in younger children, especially those under 3 years old. We conducted a cross-sectional, population-based study of 70,490 children aged 0–6 years in Guangzhou, China, from 2018 to 2023. Annual refractive screenings were performed using a validated non-cycloplegic photoscreener (SW-800 refractive screener, Suoer Electronics, China). Children were stratified by age group and screening year. We analyzed trends in mean spherical equivalent (SE) and premyopia prevalence (SE between − 0.50 and + 0.75 diopters (D)), focusing on the effects of reduced outdoor activity in 2020 . Between 2018 and 2019, the equivalent spherical refractive error (SE) in children across all age groups remained stable, indicating a consistent hyperopic reserve. For the 1-year-old group, the SE was 0.66 ± 1.30 D in 2018 and 0.64 ± 1.19 D in 2019. For the 2-year-old group, the SE was 0.61 ± 1.06 D in 2018 and 0.63 ± 0.95 D in 2019. In the 3-6-year-old group, the mean SE ranged from 0.35 ± 0.83 D to 0.56 ± 0.88 D. During the same period, the prevalence of pre-myopia was between 50.96% and 77.99%. In 2020, during the home confinement period, all age groups showed a significant myopic shift, with the mean SE decreasing by 0.36–0.56 D compared to 2019. Specifically, for the 1-year-old group, the SE was 0.14 ± 0.75 D; for the 2-year-old group, it was 0.07 ± 0.42 D; for the 3-year-old group, it was 0.08 ± 0.50 D; for the 4-year-old group, it was 0.04 ± 0.56 D; for the 5-year-old group, it was 0.08 ± 0.53 D; and for the 6-year-old group, it was − 0.01 ± 0.46 D. The prevalence of pre-myopia reached its peak in all age groups in 2020 (80.26% in the 1-year-old group, and exceeding 94% in the 2-6-year-old groups), showing a significant increase compared to 2018–2019.The risk of pre-myopia in 2018 and 2019 was significantly lower than in 2020 (all OR < 0.30, P < 0.001). This study employed a cross-sectional design, with participants studied by year and age group independently. The trends observed reflect population-level refractive changes rather than individual longitudinal recovery trajectories. Reduced outdoor activity is associated with transient, age-dependent myopic shifts in children aged 0–6 years, particularly among those under 3 years. Findings support early integration of outdoor exposure in paediatric myopia prevention strategies.
Similar content being viewed by others

Background
Myopia, or nearsightedness, has emerged as a global public health challenge, with prevalence projected to exceed 740 million people by 20501,2. Early-onset myopia is particularly concerning due to its association with sight-threatening complications, including retinal detachment, maculopathy, and glaucoma3. Consequently, identifying strategies to prevent or delay the onset of myopia in childhood remains a critical public health priority.
Extensive evidence from longitudinal and interventional studies has demonstrated that increased outdoor activity reduces the risk of incident myopia and slows myopic progression in school-aged children4,5,6. This protective effect is thought to be mediated by light intensity, spectral composition, and the visual demand of distance viewing23,24,25,26,27. However, far less is known about how reduced outdoor exposure affects younger children, particularly those aged 0–3 years who are undergoing rapid ocular growth and emmetropization.
Lifestyle changes in recent years—including increased time spent indoors and reduced opportunities for outdoor play—have raised concerns regarding early refractive development7. In 2020, widespread home confinement during the COVID-19 pandemic further reduced children’s outdoor activity, a factor strongly associated with early myopic shifts8. During home confinement, individuals were required to reside in a separate room, wear masks, be prohibited from going out, and have visitors restricted. They were also required to take temperature and report daily, maintain a distance of approximately 1 m from family members, ventilate and disinfect indoor spaces regularly. If necessary, any outdoor activities must be conducted under closed-loop management, and nucleic acid testing (NAT) must be completed to ensure effective epidemic prevention and control. While previous studies have demonstrated an increase in myopia prevalence among school-aged children during the pandemic9,10,11,12, the impact on younger children, especially those under 3 years, has not been well characterized13. Given that this age group is in a particularly sensitive stage of visual development14, further investigation is needed.
Premyopia, characterized by a slight negative shift in spherical equivalent (SE) refractive error defined as the SE refractive error > − 0.5 D and ≤ + 0.75 D15, is increasingly recognized as a key predictor of future myopia risk. Understanding how pandemic-related lifestyle changes influenced premyopia prevalence in young children is essential for informing prevention strategies. This study aims to address this gap by analyzing six years of refractive data (2018–2023) from a large sample of children aged 0–6 years. By examining trends in SE and premyopia before, during, and after the 2020 home confinement, this study highlights the importance of early-life interventions in mitigating the long-term visual health impacts of environmental disruptions.
Methods
This annual cross-sectional study was conducted from 2018 to 2023, focusing on children aged 0–6 years in the Baiyun community, Guangzhou, Guangdong Province, China. Centralized refractive screening was conducted annually for children aged 3–6 years in kindergartens across Baiyun District every October-November, with notifications issued one week in advance. For children aged 0–3 years, annual refractive screening was completed simultaneously with physical examinations and vaccination at community hospitals. In 2020, due to COVID-19, all kindergartens in the city were closed from January 23 to May 31, and children were placed under home confinement. Kindergartens reopened in batches on June 1, and after reopening, the quarantine requirements of “14-day health monitoring + scheduled drop-off and pick-up by time slots + parents not allowed to enter the kindergarten premises” were implemented. For children aged 0–3 years, screening in 2020 was postponed to July-December, while screening for children aged 3–6 years was still completed in October-November. The annual screening rate of this study covered over 85% of children in the district, and age was calculated as of the screening date. Data were locked for analysis in July 2024. This cross-sectional study followed the STROBE Statement for cross-sectional studies and was approved by the Ethics Committees of Guangdong Provincial People’s Hospital (Approval number: S2022-019-01) and Baiyun Branch of the Third Affiliated Hospital of Guangzhou Medical University(Guangzhou Baiyun Maternal and Child Health Hospital) (Approval number: 20230701). Written informed consent was obtained from the parents in accordance with the Declaration of Helsinki.
Screening procedures
This study conducted screening using the SW-800 refractive screener (Suoer Electronics, China). The refractive screener employs an optical reflection photography method for the identification and screening of refractive errors. It can measure spherical power within the range of −7.50D to + 7.50D, cylindrical power from 0.00D to 3.00D, axis angle between 0° and 180°, pupil diameter from 4 mm to 9 mm, and interpupillary distance (IPD) from 35 mm to 80 mm. The SW-800 refractive screener has been validated to demonstrate consistency with the results of cycloplegic refraction and the Spot vision screener16,17,18.
Screening was performed by professionally trained examiners who held the screener at a distance of approximately 1 m from the subject. They gradually adjusted the position according to on-screen prompts until the instrument automatically recorded data including binocular spherical power, cylindrical power, axis position, pupil diameter, IPD, and eye position. The screener automatically calculates the spherical equivalent (SE) based on spherical power, cylindrical power, and axis. Its measurement range is ± 7.50D with an incremental step of 0.25D. If the refractive status exceeds ± 7.50D, the screener triggers an automatic early warning, and the examiner advises the subject to refer to an ophthalmology clinic for further examination. The screener’s software also issues an automatic alert if significant refractive errors, anisometropia, or strabismus are detected during screening. The astigmatism assessment criteria for the Suowei SW-800 refractive screener are as follows: >2.25D of cylindrical power for children < 1 year old; >2.00D of cylindrical power for children aged 1–3 years; and > 1.75D of cylindrical power for children aged 3–6 years. In 2020, COVID-19 protocols were observed, with examiners maintaining a 1-meter distance from children and wearing masks. Myopia was defined as SE < −0.50 D, premyopia was defined as SE refractive error ≥ − 0.5 D and ≤ + 0.75 D15. Exclusion criteria were wearing contact lenses on the day of screening, use of eye drops for any ocular condition, history of ocular surgery, and use of low-dose atropine for myopia control. Examiners screened each child for these criteria before testing; children meeting any exclusion criteria were excluded from analysis.
Statistical analysis
Repeated measurements are present at the individual level, but independence is assumed at the analytical cell (year×age group) level. Annual refractive data were summarized as SE measurements. Statistical analyses were performed using Stata version 14.0. Figure 1 was created using Figdraw; Fig. 2 were created using GraphPad Prism version 8. The z-test, χ² test, and one-way ANOVA were used where appropriate. A two-sided P value of < 0.05 was considered statistically significant for primary outcomes. Using 2020 as the reference year, Bonferroni correction was applied for the adjustment of multiple comparisons of spherical equivalent (SE) and the prevalence of pre-myopia.

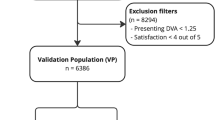
Flowchart of Participant Selection for the Study.

Trends in Myopia, Premyopia, and No Myopia Prevalence by Age (2018–2023). Annual prevalence of myopia, premyopia, and no myopia among children aged 0–6 years from 2018 to 2023, stratified by age group. Each stacked bar represents the percentage of children classified as having no myopia (light blue), premyopia (teal), or myopia (dark blue) for a given year. The prevalence of premyopia increased markedly in 2020 across all age groups.
Results
A total of 96,918 children aged 0–6 years participated in refractive screenings between 2018 and 2023. After applying exclusion criteria, 70,490 valid records were included in the final analysis (Fig. 1). The excluded data were due to disqualifying age (n = 7,812), ineligible screening times (n = 10,722), missing refraction data (n = 367), incompatible refraction data (n = 33), and repeated examinations (n = 7,494). Of the final dataset, 43,061 records were from preschoolers (37–72 months) screened in kindergartens, while 27,429 records were from infants and toddlers (0–36 months) screened during childcare check-ups. This study is a cross-sectional study, where participants in different age groups across years are mutually independent with no duplicate inclusion. A total of 17,452 children underwent multiple examinations across different years, including 8683 (2 years), 5352 (3 years), 2394 (4 years), 815 (5 years), and 208 (6 years). In this study, age is defined based on completed years. Children aged 0–12 months are categorized as age 1, those aged 13–24 months as age 2, and so on, with each subsequent age group representing a one-year increment in age based on completed months at the time of measurement. The specific numbers of boys and girls in each age group who participated in the screening from 2018 to 2023 are provided in Supplementary Materials.
The mean spherical equivalent (SE) values and standard deviations (SD) of children in each age group across different years are presented in Table 1. The results showed that the mean SE values of all age groups in 2020 were significantly lower than those in other years: 0.14 ± 0.75 D for the 1-year-old group, 0.07 ± 0.42 D for the 2-year-old group, 0.08 ± 0.50 D for the 3-year-old group, 0.04 ± 0.56 D for the 4-year-old group, 0.08 ± 0.53 D for the 5-year-old group, and − 0.01 ± 0.46 D for the 6-year-old group. The changes in SE (Δ) and 95% confidence intervals (95% CI) of each age group in different years relative to 2020 are shown in Table 2. From 2018 to 2019, the SE values of all age groups were higher than those in 2020, with the range of SE changes being 0.36–0.56 D. Among these, the 2-year-old group in 2019 had the largest SE change (0.56 D, 95% CI: 0.48–0.63 D).
The annual distribution of the prevalence of pre-myopia in children of each age group is illustrated in Fig. 2. In 2020, the prevalence of pre-myopia in all age groups reached a peak. Specifically, the prevalence in the 2–6-year-old groups all exceeded 94% (94.24% for the 2-year-old group, 95.41% for the 3-year-old group, 94.12% for the 4-year-old group, 94.33% for the 5-year-old group, and 94.62% for the 6-year-old group), while the prevalence in the 1-year-old group was also as high as 80.26%. Using 2020 as the reference, the odds ratios (OR) and 95% confidence intervals (95% CI) for the risk of pre-myopia in each year compared with 2020 are presented in Table 3. The results indicated that the risk of pre-myopia in all age groups in 2018 and 2019 was significantly lower than that in 2020 (all OR < 0.30, P < 0.001). Among these, the 2-year-old group in 2018 had the lowest OR (0.10, 95% CI: 0.07–0.14).
In conclusion, home confinement during the COVID-19 pandemic in 2020 significantly reduced the hyperopic reserve of children aged 0–6 years, while the prevalence of pre-myopia increased sharply.
Discussion
This study comprehensively analyzed the refractive development of 70,490 preschool children aged 0–6 years over six years, providing critical insights into how environmental changes—particularly reduced outdoor activity—affect early refractive development. Our findings revealed a significant myopic shift in SE during the 2020 home confinement, with an increased prevalence of premyopia observed across all age groups. Notably, this effect was most pronounced in children aged younger than 36 months, emphasizing the heightened sensitivity of early refractive development to environmental factors. These findings reveal the potential influence of early-life environmental factors on refractive development14,19,20,21 and support the need for early interventions to slow down the risk of myopia onset.
The observed myopic shift coincided with a period of markedly reduced outdoor activity, a well-established protective factor against myopia7,22. Even among infants under 1 year old, who have limited exposure to near work, the significant SE decline suggests that subtle changes in visual stimuli and lighting conditions during confinement may disrupt normal refractive development14,23. Additionally, confined spaces may increase peripheral hyperopic defocus, further promoting myopic shifts24. Previous studies have shown that natural, full-spectrum light inhibits excessive axial elongation25,26, while low-intensity indoor lighting accelerates it27, potentially contributing to the observed refractive changes. Preschool children typically maintain a high hyperopia reserve, resulting in low myopia prevalence13,28,29,30.
Our findings complement previous studies documenting increased myopia prevalence in school-aged children during periods of behavioral restriction10,11,31,32,33. While most studies have focused on children aged 6–12 years, our data highlight that preschool-aged children are also highly susceptible to environmental changes. These findings extend the known period of refractive sensitivity to infancy, demonstrating that visual environments significantly influence early refractive development even in the absence of structured near-work behaviors. Public health strategies should prioritize access to outdoor environments and minimize adverse visual conditions during periods of confinement or restricted activity to protect early refractive development and mitigate the long-term burden of myopia. Specific Measures are as Follows: (1) The urban planning level: It is recommended that in the planning of new communities and kindergartens, priority be given to ensuring the supply of outdoor activity spaces (e.g., adding children-specific green spaces and activity venues); in the renovation of old communities, optimize the layout of public spaces, increase activity areas with high light transmittance and wide visibility, and provide a safe and convenient outdoor exposure environment for young children. (2) The child care policy level:① During special periods (home confinement scenarios such as epidemics and disasters): Formulate the Guidelines for Children’s Home Visual Health, which clearly requires arranging outdoor activities in segments every day (e.g., looking far away from balconies, short walks in communities) with a cumulative outdoor duration of no less than 2 h; at the same time, standardize the indoor eye-use environment (e.g., recommending an indoor light intensity of ≥ 500 lx and avoiding close-range eye use for more than 20 min at a time);② During regular periods: Incorporate “daily outdoor activities of ≥ 2 hours” into the compulsory content of kindergartens’ daily routines, and establish a monitoring mechanism for the duration of outdoor activities in kindergartens to ensure policy implementation.
The large sample size and longitudinal design of this study enabled detailed tracking of refractive trends across multiple years and age groups. Including infants and young children provided valuable insights into refractive sensitivity during early development, a population often underrepresented in prior research. However, several limitations should be noted. First, refractive measurements were conducted without cycloplegia, which may introduce a slight myopic bias, particularly in younger children, despite the validation of the SW-800 screener. Second, this study lacked direct measures of outdoor exposure, screen time, or near-work duration. Therefore, the observed refractive changes during 2020 cannot be causally attributed to reduced outdoor activity alone. Lifestyle changes during COVID-19 represent a complex set of confounding factors, including increased near-work and altered lighting conditions. The absence of direct measures of outdoor exposure—such as wearable light sensors or validated parent-reported questionnaires—limits our ability to quantitatively assess the relationship between reduced outdoor time and refractive changes. Future studies should incorporate both objective and subjective measures of environmental exposure to better characterize these associations. Third, the single geographic setting may limit generalizability to populations with differing environmental conditions. Additionally, the lack of axial length and corneal curvature measurements restricts analysis of the underlying biological mechanisms. Given that AL is a key determinant of myopia development, future studies should integrate AL and corneal measurements to clarify the biological basis of refractive changes in early childhood. Finally, longer-term follow-up is needed to assess whether these refractive changes persist or resolve over time.
Future research should explore the long-term refractive outcomes of children affected by pandemic-related lifestyle changes, with a focus on those with early-onset premyopia. Investigations into specific environmental factors, such as screen time and outdoor exposure, and interventional studies testing preventive strategies like outdoor activity programs and screen-time guidelines, are needed to inform best practices for early myopia prevention.
This study demonstrates a clear association between reduced outdoor activity and increased premyopia prevalence in young children, with the greatest impact on those under 3 years of age. These findings reveal the importance of early myopia prevention strategies and monitoring refractive development from infancy. As societies recover from the pandemic, prioritizing visual health in young children will be critical in addressing the global burden of myopia.
Data availability
Prof Zeng and Tian has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Data will be available without any restriction for 10 years after publication from the corresponding author, Prof Tian (email: tianzhenbaiyun@163.com) upon request.
References
Holden, B. A. et al. Global prevalence of myopia and high myopia and Temporal trends from 2000 through 2050. Ophthalmology 123, 1036–1042 (2016).
Liang, J. et al. Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br. J. Ophthalmol. 0, 1–10 (2024).
Ohno-Matsui, K., Lai, T. Y. Y., Lai, C. C. & Cheung, C. M. G. Updates of pathologic myopia. Prog Retin Eye Res. 52, 156–187 (2016).
Low, W. et al. Family history, near work, outdoor activity, and myopia in Singapore Chinese preschool children. Br. J. Ophthalmol. 94, 1012–1016 (2010).
Rose, K. A. et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 115, 1279–1285 (2008).
Wu, P. C., Tsai, C. L., Wu, H. L., Yang, Y. H. & Kuo, H. K. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology 120, 1080–1085 (2013).
Xiang, M., Zhang, Z. & Kuwahara, K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog Cardiovasc. Dis. 63, 531–532 (2020).
Wong, C. W. et al. Digital screen time during the COVID-19 pandemic: risk for a further myopia boom? Am. J. Ophthalmol. 223, 333–337 (2021).
Chang, P. et al. Comparison of myopic progression before, during, and after COVID-19 lockdown. Ophthalmology 128, 1655–1657 (2021).
Wang, J. et al. Progression of myopia in school-aged children after COVID-19 home confinement. JAMA Ophthalmol. 139, 293–300 (2021).
Zhang, X. J. et al. Prevalence of myopia in children before, during, and after COVID-19 restrictions in Hong Kong. JAMA Netw. Open. 6, 3:e234080 (2023).
Wang, J. X. et al. Evaluation and follow-up of myopia prevalence among school-aged children subsequent to the COVID-19 home confinement in Feicheng, China. JAMA Ophthalmol. 141, 4:333–340 (2023).
Yang, Y. C., Hsu, N. W., Wang, C. Y., Shyong, M. P. & Tsai, D. C. Prevalence trend of myopia after promoting eye care in preschoolers: a serial survey in Taiwan before and during the coronavirus disease 2019 pandemic. Ophthalmology 129 (2), 181–190 (2022).
Mutti, D. O. et al. Ocular component development during infancy and early childhood. Optom. Vis. Sci. 95, 11:976–985 (2018).
Flitcroft, D. I. et al. IMI-defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest. Ophthalmol. Vis. Sci. 60, 3:M20–M30 (2019).
You, Y. X. et al. Prevalence of refractive error among Chinese preschool children: the Changsha children eye study. Front. Public. Health. 10, 1019816 (2022).
You, Y. X., Xu, M., Song, Y. L., Zhou, H. F. & Wei, S. H. Longitudinal changes in refractive error among preschool children aged 1–6 years: the Changsha children eye study. Front. Med. 9, 831177 (2022).
Qian, X. et al. Compared performance of spot and sw800 photoscreeners on Chinese children. Br. J. Ophthalmol. 0, 1–6 (2018).
Brown, N. P., Koretz, J. F. & Bron, A. The development and maintenance of emmetropia. Eye 13, 83–92 (1999).
Mutti, D. O. et al. Axial growth and changes in lenticular and corneal power during emmetropization in infants. Invest. Ophthalmol. Vis. Sci. 46, 9:3074–3080 (2005).
Rozema, J., Dankert, S. & Iribarren, R. Emmetropization and non-myopic eye growth. Surv. Ophthalmol. 68, 759–783 (2023).
Wang, G. H., Zhang, Y. T., Zhao, J., Zhang, J. & Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 395, 945–947 (2020).
Morgan, I. G., Rose, K. A., Ellwein, L. B. & the Refractive Error Study in Children Survey Group. Is emmetropia the natural endpoint for human refractive development: an analysis of population-based data from the refractive error study in children. Acta Ophthalmol. 88, 877–884 (2010).
Sng, C. C. A. et al. Change in peripheral refraction over time in Singapore Chinese children. Invest. Ophthalmol. Vis. Sci. 52, 7880–7887 (2011).
He, M. G. et al. Effect of time spent outdoors at school on the development of myopia among children in china: a randomized clinical trial. JAMA 314, 1142–1148 (2015).
Zong, Z. Q., Zhang, Y. X., Qiao, J. C., Tian, Y. & Xu, S. J. The association between screen time exposure and myopia in children and adolescents: a meta-analysis. BMC Public. Health. 24, 1625 (2024).
Muralidharan, A. R. et al. Light and myopia: from epidemiological studies to Neurobiological mechanisms. Ther. Adv. Ophthalmol. 13, 1–45 (2021).
Guo, X. X. et al. Significant axial elongation with minimal change in refraction in 3- to 6-year-old Chinese preschoolers: the Shenzhen kindergarten eye study. Ophthalmology 124, 1–13 (2017).
Wang, C. Y. et al. Premyopia at preschool age: population-based evidence of prevalence and risk factors from a serial survey in Taiwan. Ophthalmology 129, 1–10 (2022).
Wen, G. et al. Prevalence of myopia, hyperopia, and astigmatism in Non-hispanic white and Asian children: multi-ethnic pediatric eye disease study. Ophthalmology 120, 2109–2116 (2013).
Abounoori, M. et al. Paediatric myopia shift during the COVID-19 pandemic home confinement: a systematic review and meta-analysis. BMJ Paediatr. Open. 6, e001755 (2022).
Pan, W. & Lan, W. Z. The current and future landscape of the childhood myopia epidemic in China—a review. Ophthalmol. Ther. 13, 883–894 (2024).
Laan, D., Tan, E. T. C., Jellema, P. I. & Jenniskens, H. M. Myopia progression in children during home confinement in the COVID-19 pandemic: a systematic review and meta-analysis. J. Optom. 17, 100493 (2024).
Funding
This research was funded by the Guangdong Medical Research Fund Project (No. A2023391); Guangdong Basic and Applied Basic Research Fund Project (No.2021A1515011822); Guangdong Science and Technology Project (No.2017B010110013); Guangdong Provincial People’s Hospital Self-funded Project (No.8207031022); Guangzhou Municipal Science and Technology Program (No.2025B03J0135).
Author information
Authors and Affiliations
Contributions
Prof Zeng and Tian had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Xu, Zhang and Yang contributed equally to this work as co–first authors. Prof Zeng and Tian contributed equally to this work as co–corresponding authors.Concept and design: Xu, Zhang, Yang, Zeng and Tian.Acquisition, analysis, or interpretation of data: All authors.Drafting of the manuscript: Xu, Zhang, Yang.Critical review of the manuscript for important intellectual content: All authors.Statistical analysis: Xu, Zhang, Yang.Administrative, technical, or material support: Lan, Li, Luo, Guo.Supervision: Zeng and Tian.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xu, L., Zhang, Y., Yang, C. et al. Age-dependent and reversible refractive changes in 0–6 years old children associated with reduced outdoor activity: a six-year community-based study. Sci Rep 16, 5719 (2026). https://doi.org/10.1038/s41598-026-36515-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-36515-0
