
Abstract
Postoperative thirst affects 70% of surgical patients, causing discomfort and potential complications, especially in orthopedic patients. Current relief strategies remain suboptimal. This trial evaluated the efficacy and safety of mini-mint ice cubes (1 cm³, 20% mint) for early postoperative thirst relief. 282 patients were randomized to three groups: mini-mint ice cubes, room temperature water or absolute fasting. Primary outcome was thirst intensity at PACU discharge, measured by Numerical Rating Scale. Secondary outcomes included PACU stay, oropharyngeal discomfort, satisfaction, 24-hour postoperative quality of recovery (QoR-15), postoperative nausea and vomiting (PONV), delirium and adverse events. Mini-mint group had lower thirst (median [IQR]: 3 [1–5]) vs. water (4 [2–5], median difference: -1, 95% CI: -2 to 0; P = 0.004); vs. absolute fasting (7 [5–9], median difference: -4, 95% CI: -5 to -3; P < 0.001), shorter PACU stay (35 [30–43] min) vs. water (40 [33–45] min, P = 0.014); vs. absolute fasting (40 [35–55] min, P < 0.001), less oropharyngeal discomfort (12.9% vs. absolute fasting 27.2%, P = 0.015), higher satisfaction (4 [4–5]) vs. water (4 [4–5], P = 0.003) and absolute fasting (3 [2–4], P < 0.001), higher QoR-15 (124 [119–130]) vs. water (119 [114–125], P < 0.001) and absolute fasting (117 [111–123], P < 0.001). PONV, delirium, and hypoxemia showed no intergroup differences; cough occurred only in the water group (6.4%). Mini-mint ice cubes safely and effectively alleviate early postoperative thirst in orthopedic patients under general anesthesia, conferring clinically meaningful benefits compared to absolute fasting. Compared to room temperature water, the improvement is modest with uncertain clinical relevance.
Clinical trial registration number: ClinicalTrials.gov (ChiCTR2400089335, 6/9/2024).
Similar content being viewed by others

Introduction
Postoperative thirst remains one of the most prevalent yet frequently underestimated distressing symptoms following general anesthesia1. Reports indicate that up to 70% of surgical patients experience moderate to severe thirst during recovery in the post-anesthesia care unit (PACU)1,2. This symptom extends beyond mere discomfort and often induces anxiety, agitation, and may precipitate delirium, potentially leading to prolonged hospitalization3,4,5,6,7. Factors contributing to postoperative thirst include preoperative fasting, prolonged oral opening due to mechanical ventilation, and the perioperative administration of anticholinergic medications8,9,10.
Although Enhanced Recovery After Surgery (ERAS) guidelines advocate for early postoperative oral hydration11, clinical implementation remains suboptimal, particularly in orthopedic populations. This discrepancy may arise from legitimate concerns regarding aspiration risks in elderly patients, who often present with comorbidities such as dysphagia and cognitive impairment, as well as diminished protective airway reflexes12,13.
Contemporary strategies for alleviating thirst, such as early fluid intake, ice cubes, mentholated popsicles, aroma Gargling, chewing gum, and the application of wet gauze, have proven effective1,14,15,16,17,18,19. Notably, recent pilot studies have highlighted the significant efficacy of 1 cm³ mini-mint ice cubes with 20% concentration in alleviating thirst in critical care and palliative care settings20,21. The high-concentration mint component may provide additional benefits by activating transient receptor potential melastatin 8 (TRPM8) receptors and stimulating salivary flow22, while the small size of the ice cubes minimizes the risk of aspiration. Despite these promising findings, the application and assessment of these strategies in surgical populations remain inadequately explored in the literature. Orthopedic procedures, among the most prevalent surgical interventions worldwide, are likely to see an increase in postoperative thirst-related complications due to an aging population23. Furthermore, existing protocols in PACU often impose restrictions on oral intake without evidence-based justification, potentially extending patient discomfort. Therefore, optimizing components of enhanced recovery, such as identifying the optimal type, timing, and dosage of oral intake—holds considerable clinical importance.
To address this, we designed this triple-arm randomized controlled trial to investigate whether mini-mint ice cubes can safely and effectively alleviate thirst in orthopedic surgery patients during early PACU recovery. We hypothesized that mini-mint ice cubes would demonstrate superior thirst relief compared to room temperature water or absolute fasting.
Materials and methods
Study design
This study was a single-center, triple-arm, assessor-blinded randomized controlled trial, conducted and reported in accordance with CONSORT guidelines24. The protocol was approved by the Institutional Review Board of Jianyang People’s Hospital (reference number JYL2024003Z) on March 22, 2024 and registered with the Chinese Clinical Trial Registry (reference ID ChiCTR2400089335) on September 6, 2024, prior to initiating patient enrollment. The study was conducted in accordance with the Declaration of Helsinki, and all participants provided written informed consent prior to enrollment.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) aged ≥ 18 years; (2) American Society of Anesthesiologists (ASA) physical status classification I–III; (3) scheduled for elective non-spinal orthopedic surgery under general anesthesia. Exclusion criteria included: (1) known allergy to ice or mint; (2) inability to communicate due to mental illness, dementia, or hearing impairment; (3) presence of gastrointestinal obstruction or dysphagia symptoms. Withdrawal criteria included surgical cancellation or postoperative transfer to the intensive care unit (ICU) for safety reasons. All included patients were assessed for frailty using the FRAIL scale, which assesses five domains: fatigue, resistance, ambulation, illness, and weight loss. Each item is scored 1 if present and 0 if absent. Total scores range from 0 to 5: 0 indicates robustness; 1–2, pre-frailty; and 3–5, frailty25.
Randomization, blinding, and intervention
Patients were randomly assigned to three parallel groups: the mini-mint ice cubes group, the room temperature water group, and the absolute fasting group, at a 1:1:1 allocation ratio. Both the room temperature water and absolute fasting groups were controls. Two prespecified co-primary comparisons were: (1) mini-mint ice cubes group vs. room temperature water group; (2) mini-mint ice cubes group vs. absolute fasting group. An independent researcher generated the randomization sequence using Stata (version 15.0, Stata Corp LLC) with block randomization (block size = 6). Group assignments were sealed in sequentially numbered opaque envelopes. Enrollment was performed the day before surgery by a dedicated researcher who was masked to group assignments and not involved in any other trial procedures.
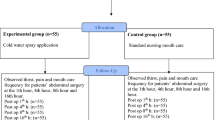
In the mini-mint ice cubes group, patients initially sucked three mini-mint ice cubes, with additional sets (each containing 3 cubes) provided based on individual preference, no upper limit on the total dosage. Preparation method20: Water was mixed with concentrated mint syrup to achieve a 20% mint concentration, then frozen in 1 cm³ (1 mL volume) silicone trays to form mini-mint ice cubes. In the room temperature water group: 10 mL of room temperature water (from the hospital water dispenser) was administered via a 10 mL syringe initially, with additional amounts provided based on patient preference (maximum 0.5 mL/kg)26.
All thirst-relief interventions were implemented only after evaluation and approval by the attending anesthesiologist in the PACU. The following requirements had to be met: full consciousness after extubation, stable vital signs, adequate recovery of cough and swallowing reflexes, and absence of nausea or vomiting. To minimise bias, envelopes containing the intervention assignment were opened only after the initial thirst assessment. Trained PACU nurses administered the interventions. Patients were positioned with the head elevated at 15°–30°. Additional interventions were permitted if no discomfort occurred after the initial administration. Interventions were paused for 10 min if coughing, nausea, or vomiting developed, followed by re-evaluation. No fluids were administered within 10 min prior to PACU discharge to prevent transport-related vomiting. Nurses truthfully recorded pre-intervention thirst intensity, intervention time, the volume of water/number of ice cubes used, and adverse events including the incidence of coughing and hypoxemia (SpO2 < 92%) during the intervention period. Any adverse event that occurred was immediately reported to the attending anesthesiologist, who managed it in accordance with clinical standards. PACU-related outcome measures were assessed by experienced, fully blinded researchers at the time of PACU discharge. Intervention-administering nurses and the participants could not be blinded due to the distinct nature of the interventions.
Anesthesia management
All patients received standard anesthesia management. No pre-anesthetic medications were administered. Patients consumed 200 mL of oral nutritional liquid 2–4 h before surgery. Ultrasound-guided nerve block and, when necessary, radial artery cannulation were performed in the pre-anesthesia holding area by the same attending anesthesiologist. Upon entering the operating room, standard monitoring was initiated, including electrocardiogram (ECG), non-invasive or invasive blood pressure, pulse oxygen saturation (SpO2), and heart rate (HR). General anesthesia was induced with etomidate (0.2–0.4 mg/kg), sufentanil (0.2–0.4 µg/kg), and cisatracurium (0.2–0.3 mg/kg). Following endotracheal intubation or laryngeal mask insertion, anesthesia was maintained with sevoflurane (1–2%) and remifentanil (0.05–0.2 µg/kg/min), targeting a bispectral index (BIS) of 40–60. All anesthetic agents were discontinued at the end of the procedure. During the operation, mean arterial pressure (MAP) was maintained within ± 20% of baseline; forced-air warming blankets and additional muscle relaxants were used as needed. Bradycardia (defined as HR < 50 beats per minute) was treated with atropine (0.3–0.5 mg). All patients received intravenous dexamethasone (10 mg) and ramosetron (0.3 mg) for antiemesis. Following surgery, patients were transferred to the PACU for extubation, with a sufentanil-based patient-controlled intravenous analgesia (PCIA) pump: background infusion 0.04 µg/kg/h, bolus dose 0.01 µg/kg; lockout time 20 min.
Extubation timing was determined by the attending anesthesiologist in the PACU. Residual neuromuscular blockade was routinely antagonized with neostigmine (30 µg/kg) and atropine (10 µg/kg) in the absence of contraindications. Extubation was performed carefully after confirming a train-of-four (TOF) ratio > 0.9, adequate spontaneous ventilation, and patient compliance. PACU discharge required an Aldrete score ≥ 9. After transfer to the ward, patients initiated oral intake as tolerated under physician guidance and received oral celecoxib (100–200 mg) every 12 h for enhanced analgesia.
Outcomes
The primary outcome was thirst intensity at PACU discharge, measured using a numerical rating scale (NRS; 0 = no thirst, 10 = worst imaginable thirst). This validated tool had been widely used for evaluating the intensity of subjective symptoms such as pain and thirst in clinical research27. Secondary outcomes included: (1) length of PACU stay; (2) incidence of oropharyngeal discomfort at PACU discharge; (3) incidence of postoperative nausea and vomiting (PONV) during PACU stay; (4) patient satisfaction score at PACU discharge (5-point Likert scale28: 1 = definitely dissatisfied, 2 = somewhat dissatisfied, 3 = neutral, 4 = satisfied, 5 = very satisfied). (5) incidence of PONV within 24 h after surgery, assessed within 24 ± 2 h postoperatively; (6) postoperative quality of recovery at 24 h, assessed using the 15-item Quality of Recovery Questionnaire (QoR-15) at the same assessment time as (5). This instrument is validated with excellent reliability, high responsiveness, and clinical feasibility in surgical populations29; (7) time of bowel function recovery (flatus or stools); (8) incidence of delirium during the postoperative days 1–3 or until discharge, assessed daily between 5 pm and 7 pm using the 3-minute Diagnostic Confusion Assessment Method (3D-CAM)30; (9) postoperative hospital length of stay. All follow-up and assessments were conducted by trained staff who were masked to group assignments.
Sample size calculation
The primary endpoint of this study was to compare the thirst scores at PACU discharge between: (1) mini-mint ice cubes group vs. room temperature water group, and (2) mini-mint ice cubes group vs. absolute fasting group. Based on a pilot trial, the absolute fasting group was expected to have a mean thirst score of 6, with standard deviation (SD) = 2.5. Assuming a 30% reduction in the mini-mint ice cubes group vs. absolute fasting and 20% reduction vs. room temperature water group, 94 patients per group were required to achieve 80% power (two-sided, α = 0.025) with a 10% dropout rate, calculated using PASS software (version 15.0, NCSS, USA).
Statistical analyses
Continuous variables were presented as mean (SD) or median (interquartile range [IQR]) based on the Shapiro-Wilk test. Comparisons among the three groups were performed using one-way analysis of variance (ANOVA) or Kruskal-Wallis test. Categorical variables were presented as n (%) and compared using the Chi-square test or Fisher’s exact test. Median difference (MD) for the primary outcome was estimated using the Hodges–Lehmann method based on the Mann-Whitney U test. The analysis was conducted by intention-to-treat (ITT) principle, and a per-protocol (PP) analysis was also performed.
In sensitivity analyses, post-hoc adjusted analyses for the primary outcome were conducted using a generalized linear model (GLM) to estimate regression coefficient (β) with 95% confidence interval (CI). The model was specified with a Gaussian family and identity link function. Baseline thirst intensity was included as a covariate, and additional potential confounders were incorporated into the model if they yielded a P-value < 0.2 in univariable analyses. Subgroup analyses were further conducted using the GLM, stratified by age (< 65 vs. ≥ 65 years), gender, ASA Classification, type of surgery (limb fractures vs. other surgeries), and intubation approach (laryngeal mask airway vs. endotracheal intubation). Post-hoc analyses were not alpha-adjusted and were treated as exploratory. A two-tailed P < 0.05 was considered statistically significant. All analyses were performed using SPSS (version 24; IBM Corp., Armonk, NY, USA) and GraphPad Prism (version 10.2.3; GraphPad Software, Boston, MA).
Results
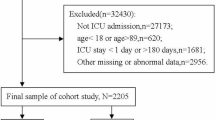
Between October 8, 2024 and December 20, 2024, 338 patients were screened for eligibility. 56 patients were excluded (22 refused participation, 18 had hearing impairment, 11 had dementia, 5 had ice allergy). A total of 282 patients were enrolled, with 279 included in the final analysis (93 in the mini-mint ice cubes group, 94 in the room temperature water group and 92 in the absolute fasting group). Three patients dropped out after group allocation for the following reasons: one in the mini-mint ice cubes group and one in the absolute fasting group were transferred to the ICU after surgery, and one in the absolute fasting group had surgery cancelled due to hypertension (Fig. 1).

CONSORT Flowchart of patient enrollment and inclusion in analysis. ITT: intention-to-treat; PP: per-protocol.
Clinical characteristics
Patient characteristics, intraoperative and recovery period data are presented in Table 1. In this cohort, the mean thirst intensity in the PACU before intervention was 6.0 ± 2.6, with 82.1% (229 cases) experiencing moderate to severe thirst (NRS ≥ 4). The mean time to intervention after extubation was 12.2 ± 4.3 min.
Primary outcome
Thirst intensity at PACU discharge in the mini-mint ice cubes group (3 [1–5]) was significantly lower than in the room temperature water group (4 [2–5]; MD, −1; 95% [CI], −2 to 0; P = 0.004) and the absolute fasting group (7 [5–9]; MD, −4; 95% [CI], −5 to −3; P < 0.001) (Table 2). Results of the per-protocol analysis were consistent with the primary analysis (see supplement table S1 and table S2).
Changes in thirst intensity before and after the intervention are illustrated in Fig. 2. The mean reduction in thirst intensity was 3.4 ± 1.9 in the mini-mint ice cubes group, 2.2 ± 2.0 in the room temperature water group. In contrast, the absolute fasting group exhibited a mean increase in thirst intensity of 1.0 ± 1.7. The difference between the mini-mint ice cubes group and the room temperature water group was significant (P < 0.001), as was the difference between the mini-mint ice cubes group and the absolute fasting group (P < 0.001).

Thirst intensity assessed at two time points. T0: Thirst intensity before intervention; T1: Thirst intensity at PACU discharge. PACU: post-anesthesia care unit.
Secondary outcome
Secondary outcomes are presented in Table 2. The length of PACU stay in the mini-mint ice cubes group (35 [30–43]) was significantly shorter than that in the room temperature water group (40 [33–45]; MD, −5; 95% [CI], −5 to 0; P = 0.014) and the absolute fasting group (40 [35–55]; MD, −5; 95% [CI], −10 to −5; P < 0.001). Regarding the incidence of oropharyngeal discomfort at PACU discharge, the mini-mint ice cubes group had a significantly lower rate than the absolute fasting group (12 [12.9%] vs. 25 [27.2%]; relative risk (RR), 0.40; 95%[CI], 0.19 to 0.85; P = 0.015), but exhibited no significant difference compared with the room temperature water group (12 [12.9%] vs. 14 [14.9%]; RR, 1.09; 95%[CI], 0.70 to 1.70; P = 0.694). Patient satisfaction scores at PACU discharge were significantly higher in the mini-mint ice cubes group (4 [4–5]) compared with the room temperature water group (4 [4–5]; MD: 0; 95% CI: 0 to 1; P = 0.003) and the absolute fasting group (3 [2–4]; MD: 1; 95% CI: 1 to 1; P < 0.001). Additionally, QoR-15 score at 24 h after surgery was higher in the mini-mint ice cubes group (124 [119–130]) than in the room temperature water group (119 [114–125]; MD: 4; 95% CI: 2 to 7; P < 0.001) and the absolute fasting group (117 [111–123]; MD: 7; 95% CI: 4 to 9; P < 0.001). No significant differences were observed in other secondary outcomes among the three groups.
Adverse events
Adverse events related to interventions are also shown in Table 2. No hypoxemia was observed in any group, while coughing occurred only in the room temperature water group (6 [6.4%]).
Other outcomes
Table 3 shows the estimated changes in thirst intensity derived from the adjusted GLM. Consistent with our hypotheses, the mini-mint ice cubes group exhibited a significantly greater reduction in NRS thirst scores during subsequent PACU assessments compared with both the room temperature water group and the absolute fasting group (P < 0.05). The model was adjusted for confounding factors including gender, hemoglobin level, coronary artery disease, atropine use, PCIA use, intervention time, and pre-intervention thirst intensity. In all subgroups except for ASA Classification III subgroup and the ‘other surgeries’ subgroup, the mini-mint ice cubes group still demonstrated a significant reduction in NRS thirst scores relative to the room temperature water group and the absolute fasting group (P < 0.05) (see Supplementary Table S3).
Consumption of mini-mint ice cubes and room temperature water
As shown in Fig. 3, the consumption of mini-mint ice cubes was 3 [3–6] [mean (SD): 4.4 (1.9)], while water intake in the room temperature water group was 10 [10–20] mL [mean (SD): 16.3 (9.2) mL].

Distribution of mini-mint ice cubes consumption and room temperature water intake in intervention groups.
Discussion
In this study, we explored the application of 1 cm³ mini-mint ice cubes for the first time to alleviate postoperative thirst in patients undergoing orthopedic surgery. Our findings demonstrate that mini-mint ice cubes represent a safe and highly effective non-pharmacological intervention, as they significantly reduced postoperative thirst compared with both room temperature water and no intervention in patients who received general anesthesia for orthopedic procedures.
The innovation of this study lies in the utilization of unique 1 cm³ mini-mint ice cubes with a 20% mint concentration, which substantially reduces the actual required dosage (a mean of 4.4 ice cubes per patient). This dosage is lower than both the 10–20 mL of 0.05% mint concentration ice lollies employed in previous studies17,18 and the mean volume required by patients in the room temperature water group of the present study (16.3 mL per patient). Furthermore, benefiting from the miniature cube design, the risk of coughing was significantly lower in the mini-mint ice cubes group compared with the room temperature water group (0 vs. 6 cases). Although we did not directly measure nursing workload in this study, these outcomes theoretically reduce the nursing burden associated with feeding assistance and patient monitoring. Second, the intervention protocol featured high flexibility, allowing patients to adjust intake according to individual needs without strict restrictions on volume or frequency. This approach was more in line with actual clinical needs than previous studies17,18,19. Furthermore, we report for the first time that the earliest safe intervention time in this cohort was 12 min, with a mean water intake of 16.3 mL (0.26 mL/kg) in the room temperature water group—much lower than the reference value in our study design26. This discrepancy may be related to the physiological characteristics of older adults, who typically consume less fluid than younger individuals despite similar thirst intensity and plasma osmolality, suggesting more rapid achievement of fluid satiety. Our data also indicate that despite severe preoperative thirst, patients preferred repeated small-volume intake over a single large-volume administration.
A recent study exploring aromatic gargle solutions in spinal surgery patients demonstrated that 60 mL doses effectively alleviated postoperative symptoms including thirst, halitosis, and sore throat19. While our current research focuses on a different population of orthopedic surgical patients, the findings align with these conclusions. Moreover, our mini-mint ice cubes intervention offers potential advantages in dosage precision, patient compliance, and overall comfort.
The meta-analysis revealed that while both mint and ice demonstrated intrinsic thirst-relieving properties14,31, the synergistic effects observed in mini-mint ice cubes surpass those of ice alone, even in elderly populations where pure ice interventions show diminished efficacy32. Although a statistically significant difference was observed between the mini-mint ice cubes group and room temperature water groups, the clinical significance of the difference remains debatable. While it did not meet the minimum clinically important difference of 1.7 points on the NRS established in pain research33, the absolute reduction to a median NRS score of 3 (borderline mild to moderate severity) may still hold meaningful clinical relevance. This threshold reduction may translate to fewer nursing interventions and improved patient cooperation during critical recovery phases.
Additionally, the intervention’s multimodal benefits extended beyond thirst relief, significantly alleviating post-intubation sore throat, improving patient satisfaction and reducing PACU length of stay. This is of particular clinical significance in high volume surgical centers. The effect may be attributed to the combined actions of high-concentration mint and ice, including: rapid thirst relief via activation of oropharyngeal thermoreceptors; cooling and analgesic effects of menthol; physiological responses to cold stimulation; and psychological enhancement of subjective comfort22,34. Furthermore, the application of mini-mint ice cubes improved the 24-hour postoperative QoR-15 score. The potential mechanism may be linked to the very early application of mini-mint ice cubes and subsequently the positive sustained effects of high-concentration menthol: sucking the mini-mint ice cubes may exert effects by slowly releasing menthol, which alleviates postoperative oropharyngeal discomfort and anxiety, mitigates sleep fragmentation induced by these symptoms, and improves sleep quality through a mild sedative effect—ultimately accelerating overall physical recovery22,35,36,37.
There are several limitations to our study. First, the external validity of the trial is slightly weakened by the inclusion population and single-center design. Given that the study scope was limited to patients undergoing non-spinal orthopedic surgery, caution is advised when extrapolating the results to other surgical populations, particularly elderly patients with impaired swallowing function. However, considering the anxiolytic and sleep-improving properties of mint, this intervention may offer potential advantages in populations at high risk of cognitive impairment. Second, we only administered the intervention short-term in the PACU, future studies could extend its application to the general ward and investigate its impacts on long-term postoperative recovery. Third, participant blinding was impractical, as patients could readily distinguish between mint ice cubes and water, introducing potential bias. To mitigate this, researchers and nursing staff received rigorous training to ensure equal treatment for all groups. Fourth, atropine is a well-recognized additional risk factor for postoperative thirst. A primary reason for its relatively frequent administration in the present study was the unavailability of sugammadex at our institution, which necessitated the routine co-administration of neostigmine with atropine for neuromuscular blockade reversal. This may partially explain why the incidence of severe thirst reached 82.1% in our study population. On the other hand, strict clinical criteria for intraoperative atropine administration for bradycardia were predefined in the study protocol. Consequently, the three intervention groups were well-balanced with respect to overall atropine exposure. To account for its potential confounding effect on the primary outcome, we additionally performed a supplementary analysis using the GLM. In clinical practice, it is necessary to reduce the use of medications that induce postoperative thirst.
In conclusion, mini-mint ice cubes provide a simple, safe, and efficient intervention for orthopedic surgery patients undergoing general anesthesia. Although a statistically significant difference was observed compared with room temperature water, the improvement is modest and of uncertain clinical relevance. In contrast, relative to absolute fasting, mini-mint ice cubes exert a significant thirst-relieving effect with clinically relevant benefits.
Data availability
The data analysed in the current study are available from the corresponding author for reasonable request.
References
Lee, C. W. et al. Prevalence, risk factors, and optimized management of moderate-to-severe thirst in the post-anesthesia care unit. Sci. Rep. 10 (1), 16183 (2020).
Walker, E. M. K. et al. Patient reported outcome of adult perioperative anaesthesia in the united kingdom: a cross-sectional observational study. Br. J. Anaesth. 117 (6), 758–766 (2016).
Alves, de Nascimento, L., Oliveira, Lopes, M. V. & Fahl, Fonseca, L. Development and validation of a new nursing diagnosis: perioperative thirst. Int. J. Nurs. Knowl. 32 (4), 253–261 (2021).
Kjeldsen, C. L. et al. Patients’ experience of thirst while being conscious and mechanically ventilated in the intensive care unit. Nurs. Crit. Care. 23 (2), 75–81 (2018).
Sato, K., Okajima, M. & Taniguchi, T. Association of persistent intense thirst with delirium among critically ill patients: A Cross-sectional study. J. Pain Symptom Manage. 57 (6), 1114–1120 (2019).
Nascimento, L. A. D. et al. Advances in the management of perioperative patients’ thirst. AORN J. 111 (2), 165–179 (2020).
Lin, R., Li, H., Chen, L. & He, J. Prevalence of and risk factors for thirst in the intensive care unit: an observational study. J. Clin. Nurs. 32 (3–4), 465–476 (2023).
Arai, S., Stotts, N. & Puntillo, K. Thirst in critically ill patients: from physiology to sensation. Am. J. Crit. Care. 22 (4), 328–335 (2013).
Conchon, M. F., Nascimento, L. A., Fonseca, L. F. & Aroni, P. Perioperative thirst: an analysis from the perspective of the symptom management theory. Rev. Esc Enferm USP. 49 (1), 122–128 (2015).
Arany, S., Kopycka-Kedzierawski, D. T., Caprio, T. V. & Watson, G. E. Anticholinergic medication: related dry mouth and effects on the salivary glands. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 132 (6), 662–670 (2021).
Ljungqvist, O., Scott, M. & Fearon, K. C. Enhanced recovery after surgery: A review. JAMA Surg. 152 (3), 292–298 (2017).
Zhang, W. et al. Comparison of the innovative endoscopic oropharyngeal airway and the conventional mouthpiece in elderly outpatients undergoing Esophagogastroduodenoscopy under sedation: a prospective and randomized study. BMC Gastroenterol. 22 (1), 8 (2022).
Omori, M. et al. A simple assessment of the eating and swallowing functions in elderly patients with pneumonia. J. UOEH. 41 (3), 283–294 (2019).
Tsai, H. Y., Chao, A. & Hsiao, W. L. The effectiveness of cold oral stimuli in quenching postoperative thirst: A systematic review and meta-analysis. Intensive Crit. Care Nurs. 75, 103359 (2023).
Peyrot et al. Oral cooling and carbonation increase the perception of drinking and thirst quenching in thirsty adults. PLoS One. 11 (9), e0162261 (2016).
Postma, B. L., Boesveldt, E. M. & van, How to quench your thirst. The effect of water-based products varying in temperature and texture, flavour, and sugar content on thirst. Physiol. Behav. 180, 45–52 (2017).
Serato, V. M. et al. Package of menthol measures for thirst relief: a randomized clinical study. Rev. Bras. Enferm. 72 (3), 600–608 (2019).
Conchon, M. F., Fonseca, L. F. & Galvão, C. M. Use of mentholated popsicle in the management of the elderly patient’s thirst in the immediate postoperative period: A randomized controlled trial. J. Perianesth Nurs. 36 (3), 262–267 (2021).
Oh, K. E., Song, A. R. & Sok, S. R. Effects of aroma Gargling, cold water Gargling, and wet gauze application on Thirst, Halitosis, and sore throat of patients after spine surgery. Holist. Nurs. Pract. 31 (4), 253–259 (2017).
Lemyze, M., Lavoisier, J., Temime, J., Granier, M. & Mallat, J. To relieve the patient’s Thirst, refresh the mouth first: A pilot study using mini mint ice cubes in severely dehydrated patients. J. Pain Symptom Manage. 60 (1), e82–e88 (2020).
Phelan, C., Hammond, L., Thorpe, C., Allcroft, P. & O’Loughlin, M. A. Novel approach to managing thirst and dry mouth in palliative care: A prospective randomized Cross-Over trial. J. Pain Symptom Manage. 66 (5), 587–594e2 (2023).
Patel, T., Ishiuji, Y. & Yosipovitch, G. Menthol: a refreshing look at this ancient compound. J. Am. Acad. Dermatol. 57 (5), 873–878 (2007).
Gade, I. L. et al. Venous thromboembolism after lower extremity orthopedic surgery: A population-based nationwide cohort study. Res. Pract. Thromb. Haemost. 5 (1), 148–158 (2020).
Schulz, K. F., Altman, D. G., Moher, D. & Group, C. O. N. S. O. R. T. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 340, c332 (2010).
Gong, S. et al. Association between the FRAIL scale and postoperative complications in older surgical patients: A systematic review and Meta-Analysis. Anesth. Analg. 136 (2), 251–261 (2023).
Yin. Early versus delayed postoperative oral hydration after general anesthesia: a prospective randomized trial. Int. J. Clin. Exp. Med. 7 (10), 3491–3496 (2014).
Puntillo, K., Arai, S. R., Cooper, B. A., Stotts, N. A. & Nelson, J. E. A randomized clinical trial of an intervention to relieve thirst and dry mouth in intensive care unit patients. Intensive Care Med. 40 (9), 1295–1302 (2014).
Barnett, S. F. et al. Patient-satisfaction measures in anesthesia: qualitative systematic review. Anesthesiology 119 (2), 452–478 (2013).
Yoon, S. et al. Validation and clinical utility of the Korean version of the quality of Recovery-15 with enhanced recovery after surgery: a prospective observational cohort study. Br. J. Anaesth. 125 (4), 614–621 (2020).
Olbert, M., Eckert, S., Mörgeli, R., Kruppa, J. & Spies, C. D. Validation of 3-minute diagnostic interview for CAM-defined delirium to detect postoperative delirium in the recovery room: A prospective diagnostic study. Eur. J. Anaesthesiol. 36 (9), 683–687 (2019).
Wang, R., Wang, L., Liu, T. & Peng, C. Effects of menthol on thirst during surgery patients fasting: A systematic review and meta-analysis of randomized controlled studies. Int. J. Nurs. Pract. 30 (3), e13191 (2024).
Waldock, K. A. M., Hayes, M., Watt, P. W. & Maxwell, N. S. The elderly’s physiological and perceptual responses to cooling during simulated activities of daily living in UK summer Climatic conditions. Public. Health. 193, 1–9 (2021).
Todd, K. H. Clinical versus statistical significance in the assessment of pain relief. Ann. Emerg. Med. 27 (4), 439–441 (1996).
Eccles, R. Role of cold receptors and menthol in thirst, the drive to breathe and arousal. Appetite 34 (1), 29–35 (2000).
Ni, Y. B., Yu, M. & Liu, C. M. Sleep disturbance and cognition in the elderly: a narrative review. Anesthesiol Perioper Sci. 2 (3), 26 (2024).
Kazemi, A., Iraji, A., Esmaealzadeh, N., Salehi, M. & Hashempur, M. H. Peppermint and menthol: a review on their biochemistry, Pharmacological activities, clinical applications, and safety considerations. Crit. Rev. Food Sci. Nutr. 65 (8), 1553–1578 (2025).
Motlagh, M. A., Tirgari, B., Rashtabadi, O. R., Ahmadinejad, M. & Jahani, Y. The effects of aromatherapy massage with mint and sweet almond oils on the sleep quality of patients with traumatic brain injury admitted to intensive care unit: a randomized clinical trial. Sleep. Breath. 29 (1), 126 (2025).
Acknowledgements
The authors greatly thank the orthopedic team of Jianyang People’s Hospital for their support.
Author information
Authors and Affiliations
Contributions
Wenjie Mao: Conceptualization, formal analysis, writing – original draft. Yang Zhou: Data curation, investigation. Hua Zhang: Investigation, methodology. Ping Yin: Investigation. Zeyu Li: Investigation. Dan Yin: Investigation. Yan Weng: Formal analysis, methodology. Suying Li: Data curation, project administration. Huide Wang: Supervision, project administration. Qing Zhong: Supervision, writing – review & editing. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval was granted by the Institutional Review Board of Jianyang People’s Hospital (March 22, 2024, approval number: JYL2024003Z) and registered on the Chinese Clinical Trial Registry (September 6, 2024, registration ID: ChiCTR2400089335).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Our manuscript does not involve any individual person’s data in any form (including any individual details, images or videos). All data and materials are available.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mao, W., Zhou, Y., Zhang, H. et al. Mini-mint ice cubes for early postoperative thirst relief in orthopedic patients undergoing general anesthesia: a randomized controlled trial. Sci Rep 16, 5580 (2026). https://doi.org/10.1038/s41598-026-36593-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-36593-0
