
Abstract
This study aimed to evaluate time-of-day-specific functional impairments in children with obsessive–compulsive disorder (OCD) and identify related clinical and psychosocial factors. The registry data for a total of 136 children diagnosed with OCD was analyzed. Questionnaire - Children with Difficulties (QCD) was used to assess functional difficulties across daily lives and was reported by the parents. The QCD scores of the children with OCD were compared with community norms. Multiple regression analyses were used to examine the associations of the QCD domains with age, weekday sleep, anxiety, depression, behavioral problems, and siblings. The mean age of patients in the OCD group was 11.46 years (SD = 2.27), with 69 boys (51.1%) and 66 girls (48.9%). The children with OCD scored significantly lower across all QCD domains (all p < .01), with large effects for night (d = − 2.04), total QCD (d = − 2.10), school (d = − 1.90), and after-school (d = − 2.03) compared to the community sample. In the regression analyses, higher behavioral problem scores predicted better functioning in the morning and evening, whereas a greater number of siblings predicted poorer morning functioning. Higher anxiety scores were significantly associated with better night-time functioning. However, depressive symptoms were not significantly associated with overall functioning. Children and adolescents with OCD demonstrated marked domain-specific functional impairments, particularly during school, after school, and nighttime routines. Distinct psychosocial factors, including behavioral problems, sibling presence, and anxiety symptoms, were associated with time-specific functioning, underscoring the need for targeted, time-sensitive interventions.
Similar content being viewed by others

Introduction
Obsessive–compulsive disorder (OCD) is a serious neuropsychiatric condition that compromises children’s health and results in broad impairments across psychological and social functioning1,2,3,4. Several studies estimate the prevalence of OCD in children and adolescents to be between 1% and 3%, making it one of the more common childhood psychiatric disorders5,6. Some community-based studies report slightly lower rates (around 0.25%–1% in children aged 5–15 years). Other large epidemiological analyses and reviews found lifetime prevalence up to 4% in children and teenagers, with higher rates in boys (roughly a 3:2 ratio) likely due to earlier onset7. Specific regional studies, such as one from Bangladesh, found 2% prevalence among children, suggesting that rates can vary by population and cultural factors8. Although diagnoses are anchored in obsessions and compulsions, they are often quantified using symptom scales (e.g., CY-BOCS). A practical understanding of time-of-day-specific functional difficulties is essential for care. Such information helps target exposure, reduces family accommodation, supports school functioning, and improves health-related quality of life (QoL)1,2,3,9,10.
Mental disorders in childhood are closely linked to poor daily functioning with a lower QoL9,10,11,12. In pediatric OCD, QoL is reduced relative to the peers and may result in other psychiatric conditions. The decrement relates to symptom severity, comorbidity, and family accommodation, that may persist beyond acute symptom relief9,10,11,13,14. These findings highlight the need for multidimensional interventions that address not only obsessions/compulsions but also daily living skills, routines, and caregiver behaviors1,2,3,9,10,11,13,14.
School demands, homework, hygiene routines, bedtime transitions, and social/evaluative contexts can amplify rituals (e.g., checking, washing, and ordering) and reassurance seeking, thereby increasing distress and family conflicts1,2,3,10,15. Evidence-based care for pediatric OCD centers on cognitive‐behavioral therapy with exposure and response prevention (CBT-ERP). Meta-analyses of randomized trials report large effects on OCD severity (Hedges g = 1.21) and robust clinical benefits, with response and remission relative risks around 3.9 and 5.4 and a number-needed-to-treat of about 3 compared with comparison conditions. Large routine-care and specialty-clinic trials similarly find that roughly 60–75% of youth meet responder criteria and about 40–60% achieve remission after acute CBT-ERP, across individual, family-based, and group formats. Selective serotonin reuptake inhibitors (SSRIs) are also effective in pediatric OCD and are commonly combined with CBT-ERP in routine care15,16,17.
The Questionnaire–Children with Difficulties (QCD) is a brief, validated parent-report instrument designed to assess children’s daily functioning across specific time periods (morning, school, after-school, evening, and nighttime). It has demonstrated good reliability and validity in prior studies and has successfully delineated time-of-day profiles in depression, pervasive developmental disorders/autism, and ADHD, consistently showing lower total and subscale scores than community norms. This time-specific assessment approach is particularly valuable for identifying when OCD symptoms most interfere with daily routines, enabling targeted intervention planning. Prior QCD studies have highlighted the roles of sex, psychiatric symptoms, and time of day in shaping functional difficulties. For example, ADHD frequently shows evening-skewed problems and depression shows morning/school/evening dips, whereas autism-spectrum presentations display domain-specific decrements with sex differences18,19. These patterns suggest that OCD may also exhibit distinct time-of-day vulnerabilities (e.g., after-school and evening routines); however, the systematic characterization of QCD in pediatric OCD among boys and girls and across elementary and junior high schools has been limited.
Beyond the clinical presentation, family context is central to pediatric OCD. Siblings may be buffers or stressors—helping with routines or, conversely, being drawn into rituals or reassurance cycles—and their presence can shape the highest burden periods (typically the evening)9,14. Family based therapy frameworks emphasizes family as an active change agent to reduce accommodation—modifications family members make to facilitate the child’s OCD rituals or reduce distress—and practice ERP in real time9,14,15. Comorbidities such as anxiety, depression, oppositional behaviors, ADHD, and tic disorders are common and may result in functional impairment or a complicated CBT response. However, their independent contribution to day-to-day functioning after accounting for OCD itself remains debated. Pandemic-related disruptions appear to heighten service demand and family burden for various mental health conditions in children. Whether post-pandemic functioning in pediatric OCD has normalized equally across time-of-day contexts is an open question that warrants empirical investigation20,21,22,23. Notably, OCD in both children and adults is characterized by high levels of family accommodation in which relatives become involved in the patient’s rituals or avoidance behaviors. This phenomenon creates a unique intrafamilial dynamic and represents a substantial source of caregiver burden, highlighting pediatric OCD as a condition associated with substantial family burden, including high levels of family accommodation and caregiver distress.
In this study, we evaluated daily functional difficulties among children with OCD in elementary and junior high school cohorts using QCD. We compared the total QCD and all time-of-day subscales with age-appropriate community norms, and examined associations with clinical (anxiety, depressive, oppositional, and ADHD symptoms) and family factors (sibling presence). Given the salience of late day routines in pediatric OCD, we also inspected whether decrements clustered in the after-school and evening periods.
Our study had four hypotheses. (1) Children with OCD (elementary and junior high) would score significantly lower than community controls on the QCD total and all subscales; (2) worse QCD would correlate with higher anxiety, depression, oppositional, and ADHD symptom burden; (3) sibling presence would be associated with time-of-day-specific functioning differences (e.g., evening routines), consistent with the literature on family accommodation; and (4) markers of higher clinical complexity (e.g., comorbidity or prior hospitalization when available) would align with more severe daily functional impairment.
Methods
Study design and setting
This retrospective case-control study evaluated the daily functioning of children with OCD by administering the QCD. Participants were categorized into clinical (children with OCD) and community-based control groups, which comprised junior high school students from Ichikawa City, western Chiba Prefecture. Ichikawa is a residential and educational hub approximately 20 km from Tokyo, with a population of 501,209 as of April 2024, and ranks as the fourth largest city in the prefecture.
The study was conducted as per the ethical principles outlined in the Declaration of Helsinki. The informed consent process followed the Ethical Guidelines for Clinical Epidemiology Research established by the Ministry of Health, Labour, and Welfare of Japan. Direct consent was not always required for observational studies that use anonymized clinical records without human tissue samples. However, researchers must publicly disclose the purpose and implementation of the study. This disclosure was posted in the outpatient clinic of the participating hospital. All personal identifiers (e.g., names and dates of birth) were excluded.
This study was approved by the Ethics Committee of the National Center for Global Health and Medicine (NCGM-G-003042–10, NCGM-S-004487–03; Tokyo, Japan).
Recruitment and participants
Data were obtained from the clinical registry maintained by the Department of Child and Adolescent Psychiatry at the National Kohnodai Medical Center of the Japan Institute for Health Security. This registry has been collecting information on first-time outpatient visits since January 2016, which enables comparisons with community samples.
We used registry data to examine the experiences of parents of children with OCD who visited outpatient clinics. The inclusion criteria were children and adolescents in ninth grade or younger, corresponding to an age range of 6–15 years, who were first-time patients using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria.
Since January 2016, our outpatient clinic has used a standardized intake protocol in which parents complete the QCD and Oppositional Defiant Behavior Inventory (ODBI) and children complete the Depression Self-Rating Scale (DSRS) before the first consultation. For the present retrospective case–control study, we extracted data from these routinely collected intake assessments and the corresponding clinical diagnoses recorded in the electronic medical records.
Of the 4,368 registrants, 136 elementary and junior high school students were diagnosed with OCD. Preschool cases were excluded. Finally, the data from 136 children were analyzed. Clinical data included responses from the QCD, DSRS, and ODBI as well as medical record information on suicidal ideation and school non-attendance. Patients with incomplete questionnaires or clinical data were excluded. All participants were treatment-naive for CBT specialized for children at the time of assessment.
Community control group
The Ichikawa City Education Committee approved the survey for public elementary and junior high school students. Teachers distributed consent and assent forms along with four questionnaires (including the QCD) to the parents of 10,000 randomly selected children from September 20 to 30, 2008. We used the QCD scores of the children from this community sample, as reported in a previous study24.
Measures
Questionnaire-children with difficulties
The QCD is a brief parent-rated tool that captures daily functioning in specific time periods—morning, school, after-school, evening, night, and overall behavior, with higher scores indicating better functioning18,19,25. The QCD comprised 20 parent-rated items that assess children’s functioning at specific times of the day: early morning/before school (items 1–4), during school (5–7), after school (8–10), evening (11–14), night (15–18), and overall behavior (19–20). Each item is rated on a 4-point Likert scale ranging from 0 (completely disagree) to 3 (completely agree). Higher scores reflect better functioning and fewer daily difficulties26. The QCD includes practical, easy-to-understand items such as washing one’s face, brushing teeth, and dressing. Previous studies established its internal consistency and validity26. We calculated both the total and subscale scores for each time domain.
Depression self-rating scale
This 18-item scale measures depressive symptoms in children. It included items with either positive or negative associations with depression, each rated as “always” (2 points), “sometimes” (1 point), or “never” (0 points); half the items were reverse scored. The total scores range from 0 to 27 points, with higher scores indicating more severe depressive symptoms. A score of ≥ 16 points was used as the clinical cut-off in Japan27.
Spence children’s anxiety scale
The Spence Children’s Anxiety Scale (SCAS) is a 38-item scale that assesses anxiety symptoms across several domains, including social phobia, obsessive-compulsive disorder, and panic disorder28. It was completed by either the child or caregiver. Each item is rated from 0 to 3 points, with higher total scores indicating greater anxiety severity. Although no universally accepted cutoff exists, a score of 42 points has been suggested as the threshold for clinically significant anxiety.
Oppositional defiant behavior inventory
The ODBI includes 41 items that measure behaviors associated with ADHD, ODD, and conduct disorders. Responses were rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (very much). Scores of > 20 points indicated a high likelihood of ODD. The ODBI demonstrates good internal consistency, test-retest reliability, and concurrent and divergent validity29.
All the psychological questionnaires (DSRS, SCAS, and ODBI) were completed by the primary caregiver during the child’s first psychiatric consultation. Data were obtained during routine clinical assessments and a retrospective analysis was performed.
Sleep duration and history of inpatient treatment
A self-administered questionnaire on sleep time on weekdays and holidays was administered during the child’s first visit and accumulated in the medical records as clinical data. The data stored as registry data were used in this study. Regarding the history of inpatient treatment, the history of hospitalization during treatment after the initial consultation was recorded and extracted.
Statistical analysis
Before parametric analyses, such as t-tests and Pearson’s correlations, we assessed the normality of the continuous variables using the Shapiro–Wilk test. Most variables followed a normal distribution. For variables that deviated from normality, we performed nonparametric analyses using the Mann–Whitney U test and Spearman’s rank correlation. These analyses yielded results comparable to those of the parametric tests. Therefore, this study only presents the parametric test results.
All statistical analyses were conducted using R. Independent sample t-tests were used to compare between-group QCD subscale scores. Effect sizes were calculated using Cohen’s d. Pearson’s correlation coefficients were used to examine the associations between the QCD scores and clinical measures (DSRS, SCAS, and ODBI). For between-group comparisons of QCD domain scores, a Bonferroni-adjusted significance threshold of p < .01 was used to account for multiple comparisons across six domains (α = 0.05/6 = 0.008, rounded to p < .01 for conservativeness). For regression analyses, statistical significance was set at p < .05.
Multivariate regression analysis
To examine the independent associations between clinical and psychosocial variables and daily functioning, multiple linear regression analyses were conducted with the QCD total and subscale scores as dependent variables. Covariates included age, weekday sleep duration, and history of inpatient treatment (coded 1 = yes, 0 = no).
These variables were selected a priori based on their clinical relevance and previous studies. A separate regression model was performed for each QCD domain (morning, school, after-school, evening, night, and overall behavior). Standardized beta coefficients, 95% confidence intervals, and p-values are presented. All analyses were conducted using R software.
Results
Descriptive and clinical data for the OCD group
The clinical sample comprised 136 children and adolescents (age range, 6–15 years) diagnosed with OCD according to the DSM-5 criteria by board-certified child and adolescent psychiatrists. The mean age was 11.46 years (SD = 2.27). The sample was almost evenly divided according to sex: 69 boys (51.1%) and 66 girls (48.9%). In terms of educational level, 79 participants (58.5%) were enrolled in elementary school and 56 (41.5%) in junior high school. The mean number of siblings was 0.96 (SD = 0.86), with a range from zero to three.
Clinical background data revealed that 46.7% of the sample had not attended school for more than three months, consistent with the national definition of school refusal. In addition, 11.1% of the sample had experienced domestic violence, and 11.1% reported suicidal ideation. The descriptive statistics (Table 1) characterized the study population as a clinically complex group with a notable psychosocial burden.
QCD score distributions and comparison with community reference
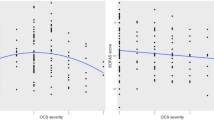
Table 2 presents the distributions of the QCD scores in the OCD and community reference groups. Across all six time-of-day domains and the total score, children with OCD showed significantly lower scores than the community sample (all p < .01).
In the morning domain, the OCD group had a mean score of 5.95 (SD = 3.34), whereas the community group scored 8.27 (SD = 2.69), with a large effect size (d = − 0.78). For the school domain, the OCD group scored 3.84 (SD = 2.64) compared to 7.83 (SD = 1.58) in the community group (d = − 1.90). After-school functioning showed similar differences, with scores of 3.57 (SD = 2.53) in the OCD group versus 7.70 (SD = 1.58) in the community group (d = − 2.03). Evening functioning scores were also lower in the OCD group (M = 5.46, SD = 3.31) than in the community group (M = 9.87, SD = 1.70), with d = − 1.75. Nighttime functioning showed a marked difference, with OCD participants scoring 3.56 (SD = 2.76) compared to 8.08 (SD = 1.70) in the community sample (d = − 2.04). For overall behavior, mean scores were 3.16 (SD = 2.05) in the OCD group and 4.86 (SD = 1.26) in the community group (d = − 1.03). Finally, the total QCD score was substantially lower in the OCD group (M = 25.53, SD = 12.59) than in the community sample (M = 47.20, SD = 8.28), with a large effect size (d = − 2.10).
Regression analyses of QCD domains
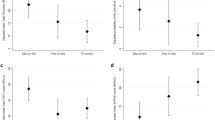
Table 3 shows the results of the multiple regression analyses examining the associations between clinical and psychosocial variables and QCD subscale scores.
In the morning domain, higher ODBI scores were significantly associated with better functioning (β = 0.281, 95% CI [0.10–0.46], p = .005). Conversely, a greater number of siblings was significantly associated with poorer morning functioning (β = − 0.189, 95% CI [–0.38 to − 0.00], p = .049). Other variables, including age, sleep duration, and anxiety and depression scores, were not significant. No predictors were statistically significant for school or after-school domains. In the evening domain, higher ODBI scores predicted better functioning (β = 0.281, 95% CI [0.09–0.46], p = .005). None of the other predictors were statistically significant. In the night domain, higher SCAS total scores were significantly associated with better functioning (β = 0.07, 95% CI [0.01–0.13], p = .02). None of the examined variables showed significant associations with overall behavior.
Discussion
Characteristics of daily functional impairments among children with OCD
This study provides a comprehensive description of daily functional impairments in children and adolescents with OCD. Difficulties were observed across all time-of-day domains assessed by the QCD, with particularly marked impairments during school hours, after school, and at night3. These patterns suggest that the disorder exerts its most profound impact during periods that require sustained attention, compliance with structured activities, and transitions between contexts, situations that are often disrupted by intrusive thoughts and compulsive behaviors.
The functional profile identified here is consistent with previous research, indicating that pediatric OCD is associated with a broad reduction in quality of life, often exceeding that observed in other child psychiatric conditions4,30,31,32,33. Our findings extend the literature by delineating time-specific vulnerabilities and emphasizing that impairment is not uniform throughout the day. School time difficulties may reflect the combined demands of academic performance, social interactions, and adherence to institutional rules, all of which can be compromised by OCD-related rituals and avoidance behaviors. After-school challenges may arise as accumulated fatigue interacts with symptom exacerbation in less-structured settings. Night-time impairments likely stem from bedtime rituals, prolonged checking, or heightened anxiety before sleep, which can disrupt rest and contribute to daytime fatigue and functional decline.
These temporal patterns also align with clinical observations that symptom expression in OCD varies according to daily routines, environmental demands, and family interactions9,10,14. By mapping these patterns, the present study highlighted the value of time-of-day-specific assessment tools such as QCD in guiding targeted interventions.
Impact of physical and psychosocial factors on daily functioning
Multivariate analyses revealed that factors associated with functional impairment varied by time domain, emphasizing the importance of a nuanced, context-sensitive approach to treatment planning.
Behavioral problems, as measured using the ODBI, were linked to better functioning in the morning and evening3,10. Counterintuitively, this may indicate that children with more overt externalizing behaviors receive greater parental supervision and prompts during these periods, which in turn supports their daily routines. However, increased involvement may also perpetuate dependency, highlighting the need for interventions that balance guidance with the promotion of autonomy.
A higher number of siblings was associated with poorer morning functioning, possibly reflecting competition for parental attention and household resources during busy preschool periods. This finding highlights the need to consider family structure when designing morning routine interventions, particularly in households with multiple children preparing for school simultaneously10,14.
Anxiety symptoms were associated with better nighttime functioning. This relationship may reflect greater parental involvement and vigilance at bedtime for children who are perceived as more anxious, which could help enforce bedtime routines. Nonetheless, excessive accommodation of anxiety can maintain or exacerbate OCD symptoms over time, suggesting the need for careful monitoring of family involvement during night-time routines.
Depressive symptoms were not significantly associated with overall functioning in the present analyses2,13,34. While depression is clinically known to impair motivation, energy, and concentration, our findings suggest that its independent contribution to daily functioning is not evident after accounting for other variables. Future studies with larger sample sizes may clarify whether depression exerts a broader impact on functioning in pediatric patients with OCD.
Taken together, these findings suggest that functional impairments in pediatric OCD are the result from a complex interplay of clinical symptoms and psychosocial context. Effective intervention requires tailoring strategies to specific times of the day in order to address not only OCD symptoms but also co-occurring emotional and behavioral problems, family structure, and parental involvement patterns.
Limitations
All participants were recruited from a single clinical center, which may have limited the external validity of our findings across different geographic regions and healthcare settings. Furthermore, we excluded cases with incomplete clinical records or missing questionnaire data, which could have introduced selection bias. These patients may have systematically differed in illness severity or sociodemographic characteristics. Additionally, the retrospective nature of data collection prevented a standardized assessment of potential confounders such as dietary habits, sleep patterns, and physical activity levels. Therefore, future studies should adopt prospective multicenter designs with predefined inclusion criteria and rigorous data-management protocols to minimize missing information.
In addition, while our findings suggest that the presence of siblings places a greater burden on parents, we were unable to assess more nuanced aspects of sibling dynamics, such as birth order or sex composition, due to inconsistent documentation in the clinical records. These variables may have significantly influenced family interactions and functional outcomes. Future studies should collect detailed family demographic information to enable stratified analyses and tailored, family-based interventions.
Furthermore, studies should integrate direct observational methods or digital activity monitoring with parent-reported QCD assessments to reduce reporting bias and provide a more comprehensive evaluation of daily functioning.
From a statistical perspective, the sample size, although adequate for primary analyses, may have been underpowered to detect smaller effect sizes, particularly in the multivariate regression models for individual QCD domains. This limitation increases the risk of type II errors, and the reported nonsignificant associations should be interpreted with caution. Moreover, we did not perform cross-or external validation of the regression models limiting the generalizability of the identified associations.
An important limitation is the absence of OCD-specific symptom severity measures such as the Children’s Yale-Brown Obsessive Compulsive Scale (CY-BOCS). Without these standardized OCD severity assessments, we were unable to examine associations between specific symptom dimensions (e.g., contamination, checking, symmetry) and time-of-day functioning patterns. All participants were treatment-naive for CBT specialized for children. While this ensures a uniform baseline, it limits our ability to examine how CBT influences time-specific functioning patterns. Additionally, we did not systematically collect information on concurrent pharmacotherapy. Finally, the cross-sectional design precludes causal inferences; longitudinal studies are needed to determine whether improvements in time-specific functioning predict overall treatment outcomes.
While we did not assess QOL and self-esteem directly, the observed impairments in daily functioning may reflect underlying deficits in these domains3,9,10,13,14,30,31,32,33. Future research should incorporate validated measures of QOL to further elucidate their contribution to caregiver burden in patients with OCD.
Clinical implications
This study highlights the importance of recognizing time-of-day-specific functional vulnerabilities in children with OCD. The QCD proved useful in identifying these periods, which can inform more targeted intervention strategies.
Morning: Establish structured wake-up routines with consistent parental support to reduce inertia and conflict during school preparation. Families with multiple children may require additional strategies to manage their competing demands.
After school: Introduce brief rest periods and low-demand activities to mitigate fatigue and prevent symptom escalation.
Evening: Promote predictable family-based routines. Provide psychoeducation to siblings to reduce unhelpful involvement in rituals and enhance supportive interactions.
Night: While higher anxiety may prompt greater parental supervision, care should be taken to counteract maladaptive bedtime rituals.
Integrating QCD assessments into routine care can help clinicians identify vulnerable time periods and develop individualized, time-sensitive intervention plans that address both core OCD symptoms and relevant family or psychosocial factors.
Conclusion
Children and adolescents with OCD demonstrate marked domain-specific functional impairments, with the greatest difficulties during school, after-school, and nighttime routines. Behavioral problems were associated with better functioning in the morning and evening, possibly reflecting increased parental engagement. Family structure, particularly the presence of siblings, influenced morning routine. Depressive symptoms were not significantly associated with overall functioning in the present analyses.
These findings underscore the need for time-of-day-aligned intervention strategies to address both OCD symptoms and broader psychosocial contexts. Future longitudinal research should further refine these temporal profiles and evaluate targeted treatment protocols to improve daily functioning and the overall quality of life in this population.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
References
Krebs, G. & Heyman, I. Obsessive-compulsive disorder in children and adolescents. Arch. Dis. Child. 100, 495–499. https://doi.org/10.1136/archdischild-2014-306934 (2015).
Stiede, J. T. et al. Obsessive–Compulsive disorder in children and adolescents. Annu. Rev. Clin. Psychol. 20, 355–380 (2023).
Sukhodolsky, D. G. & others. Functional impairment and family factors in pediatric obsessive–compulsive disorder. J. Am. Acad. Child. Adolesc. Psychiatry (2005).
Weidle, B., Jozefiak, T., Ivarsson, T. & Thomsen, P. H. Quality of life in children with OCD with and without comorbidity. Health Qual. Life Outcomes. 12, 152 (2014).
Walitza, S. et al. Zwangsstörung Im kindes- und jugendalter. Deutsches Arzteblatt. 108, 173–179. https://doi.org/10.3238/arztebl.2011.0173 (2011).
Al-Sharbati, Z., Al-Sharbati, M. & Gupt, I. Cognitive behavioral therapy for obsessive compulsive disorder. In Obsessive-Compulsive Disorder - The Old and the New Problems. 10.5772/57332. (InTech, 2014).
Clinical Review Obsessive-Compulsive Disorder.
Chowdhury, M. H. R., Mullick, M. S. I. & Arafat, S. M. Y. Clinical profile and comorbidity of Obsessive-Compulsive disorder among children and adolescents: A Cross-Sectional observation in Bangladesh. Psychiatry J. 2016, 1–7 (2016).
Lebowitz, E. R. Parent-based treatment for childhood and adolescent OCD. J. Obsessive Compuls. Relat. Disord. 2, 425–431 (2013).
Peris, T. S. et al. Family factors predict treatment outcome for pediatric obsessive-compulsive disorder. J. Consult Clin. Psychol. 80, 255–263 (2012).
Stewart, E. et al. Elevated autism spectrum disorder traits in young children with OCD. Child. Psychiatry Hum. Dev. 47, 993–1001 (2016).
Bastiaansen, D., Ferdinand, R. F. & Koot, H. M. Predictors of quality of life in children and adolescents with psychiatric disorders. Child. Psychiatry Hum. Dev. 51, 104–113 (2020).
Farrell, L., Waters, A., Milliner, E. & Ollendick, T. Comorbidity and treatment response in pediatric obsessive-compulsive disorder: A pilot study of group cognitive-behavioral treatment. Psychiatry Res. 199, 115–123 (2012).
Barrett, P., Healy-Farrell, L. & March, J. S. Cognitive-Behavioral family treatment of childhood Obsessive-Compulsive disorder: A controlled trial. J. Am. Acad. Child. Adolesc. Psychiatry. 43, 46–62 (2004).
Torp, N. C. et al. Effectiveness of cognitive behavior treatment for pediatric obsessive-compulsive disorder: acute outcomes from the nordic Long-term OCD treatment study (NordLOTS). Behav. Res. Ther. 64, 15–23 (2015).
Comer, J. S. et al. Internet-delivered, family-based treatment for early-onset OCD: A pilot randomized trial. J. Consult Clin. Psychol. 85, 178–186 (2017).
Chessell, C. et al. Therapist guided, parent-led cognitive behavioural therapy (CBT) for pre-adolescent children with obsessive compulsive disorder (OCD): a non-concurrent multiple baseline case series. Behav. Cogn. Psychother. 52, 243–261 (2024).
Sasaki, Y. et al. Concerns expressed by parents of children with pervasive developmental disorders for different time periods of the day: A case- control study. PLoS One. 10, e0124692 (2015).
Usami, M. et al. What time periods of the day are concerning for parents of children with attention deficit hyperactivity disorder? PLoS One. 8, e79806 (2013).
Loades, M. E. et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J. Am. Acad. Child. Adolesc. Psychiatry. 59, 1218–1239e3 (2020).
Usami, M. et al. Care for children’s mental health during the COVID-19 pandemic in Japan. Glob Health Med. 3, 119–121 (2021).
Usami, M. et al. No change in the severity of eating disorders in Japanese children during the COVID-19 pandemic. Psychiatry Clin. Neurosciences Rep. 3, e237 (2024).
Usami, M. et al. The COVID-19 pandemic-induced behavioral restrictions and their impact on child and adolescent psychiatric units—Infection control or freedom. Psychiatry Clin. Neurosci. Rep. 3, (2024).
Usami, M. et al. A case-control study of the difficulties in daily functioning experienced by children with depressive disorder. J. Affect. Disord. 179, 167–174 (2015).
Sasaki, Y. et al. Evaluating the daily life of child and adolescent psychiatric outpatients during temporary school closure over COVID-19 pandemic: A single-center case-control study in Japan. Glob Health Med. 4, 159–165 (2022).
Usami, M. et al. The reliability and validity of the Questionnaire - Children with difficulties (QCD). Child. Adolesc. Psychiatry Ment Health. 7, 11 (2013).
Murata, T. & Samy., O. Childhood depressive state in the school situation: consideration from the birleson’s scale. Sa1ishin Seishin Igaku. 1, 131–138 (2006).
Spence, S. H. A measure of anxiety symptoms among children. Behav. Res. Ther. 36, 545–566 (1998).
Harada, Y. et al. The reliability and validity of the oppositional defiant behavior inventory. Eur. Child. Adolesc. Psychiatry. 13, 185–190 (2004).
Coluccia, A., Ferretti, F., Fagiolini, A. & Pozza, A. Quality of life in children and adolescents with obsessive–compulsive disorder: a systematic review and meta-analysis. Neuropsychiatr Dis. Treat. 13, 597 (2017).
Storch, E. A. et al. Quality of life in children and youth with Obsessive-Compulsive disorder. J. Child. Adolesc. Psychopharmacol. 28, 104 (2018).
Vivan, A., de Rodrigues, S., Wendt, L., Bicca, G., Cordioli, A. V. & M. G. & Quality of life in adolescents with obsessive-compulsive disorder. Brazilian J. Psychiatry. 35, 369–374 (2013).
Moritz, S. et al. Quality of life in obsessive-compulsive disorder before and after treatment. Compr. Psychiatry. 46, 453–459 (2005).
Nazeer, A. & others. Pediatric obsessive–compulsive disorder: epidemiology and course. Child. Adolesc. Psychiatr Clin. N Am. 9, 76–93 (2015).
Funding
This study was supported by grants from the Japan Institute for Health Security (24A1014 and 24 ri 005) and a Health Labour Sciences Research Grant (23GC0013). The funder had no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
UM designed the study and drafted the manuscript. YS, MI, MM, AH, SK, NK, RM, MO, YH, YK, HM, YN, MM, YS, MO, KI, KY, MT, YY, SI, MI, KI, YH, and YM collected clinical data. MI, KM and NT managed the registry and discussed the results. All authors contributed to the study meaningfully, providing feedback on the interpretation of the results and on the writing of the paper.
Corresponding author
Ethics declarations
Competing interests
Katsunaka Mikami has received honoraria from Shionogi & Co., Ltd., SumitomoPharma Co., Ltd., Takeda Pharmaceutical Co., Ltd., Lundbeck Japan K.K., and OtsukaPharmaceutical Co., Ltd., and a consulting fee from Shionogi & Co., Ltd, EA PharmaCo., Ltd., Sumitomo Pharma Co., Ltd. and Otsuka Pharmaceutical Co., Ltd. The otherauthors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Usami, M., Sasaki, Y., Ichikawa, M. et al. Time-of-day differences in daily functioning in children with obsessive-compulsive disorder. Sci Rep 16, 7252 (2026). https://doi.org/10.1038/s41598-026-37027-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-37027-7
