
Abstract
Adverse childhood experiences (ACEs) pose significant mental health risks, and the greater the number of ACEs one has, the more pronounced the subsequent mental health issues become. In today’s world, the widespread application of artificial intelligence raises questions about its role in mediating the impact of ACEs on mental health, which remains unclear. Data were collected through questionnaire surveys from April to May 2025. Participants’ psychosocial characteristics were assessed using validated scales measuring stress, anxiety, depression, ACEs status, loneliness, sleep quality, and suicidal ideation. Data analysis incorporated propensity score matching and causal mediation analysis. Among participants, 794 (29%) reported ACE exposure. ACEs significantly impact loneliness, stress, anxiety, suicidal ideation, and depressive symptoms, with mediation of AI usage. Specifically, the total effect on loneliness is 0.24 (95% CI 0.18–0.31; P < 0.001), with a mediating effect proportion of 5.2%; the total effect on stress is 0.71 (95% CI 0.56–0.88; P < 0.001), with a mediating effect proportion of 4.4%; the total effect on anxiety symptoms is 0.65 (95% CI 0.51–0.81; P < 0.001), with a mediating effect proportion of 4.9%; the total effect on suicidal ideation is 0.07 (95% CI 0.06–0.09; P < 0.001), with a mediating effect proportion of 2.6%; and the total effect on depressive symptoms is 0.60 (95% CI 0.46–0.76; P < 0.001), with a mediating effect proportion of 5.4%. Findings highlight the critical mediating role of social AI in mental health outcomes among ACE-affected individuals.
Similar content being viewed by others
Introduction
Adverse childhood experiences (ACEs) refer to traumatic events that occur before the age of 18, including exposure to violence, suffering from abuse, neglect, and experiencing family dysfunction, among others. ACEs are prevalent worldwide. A multinational study covering 21 countries revealed that over one-third of adults have experienced at least one ACE, with the proportion approaching 40% in low-income and lower-middle-income countries. This indicates that, regardless of a country’s level of economic development, the overall incidence of ACEs remains high1. Adolescents are particularly affected. A 2021 survey conducted across 16 states in the United States found that 80.5% of adolescents have experienced at least one ACE, and 22.4% have endured four or more2. Similarly, the incidence of ACEs among children and adolescents in China continues to be concerning3 and a recent epidemiological study focusing on Chinese college students revealed that the overall ACEs exposure rate reached 57.7%4. Furthermore, research has shown that the exposure rate to ACEs among adolescents in low- and middle-income countries is even higher5,6. With the increasing prevalence of social media and the intensification of family stress in the post-pandemic era, the incidence of ACEs continues to rise.
ACEs impose a significant burden on adolescents’ mental health and trigger multifaceted adverse consequences through neurobiological and psychological pathways. Childhood traumatic events not only heighten an individual’s sensitivity to stress, exacerbating its negative effects, but also increase the risk of anxiety and depressive symptoms, collectively intensifying the onset and progression of mental health disorders7. Empirical evidence underscores a strong link between ACEs and suicidal tendencies, suggesting that such experiences elevate suicide risk through mediating mechanisms such as psychological distress and impaired resilience8. Notably, as the degree of ACE exposure increases, mental health deteriorates progressively, exhibiting a dose-dependent relationship: compared to individuals without ACE exposure, those who have experienced four or more ACEs face a 3.70-fold increased risk of anxiety disorders (95% confidence interval: 2.62–5.22; I2 = 82.2%), while those reporting more than two ACEs have a significantly higher likelihood of experiencing depressive mood (odds ratio = 7.99, P < 0.001)9. Dose–response analysis indicates that for every 1.8-unit increase in ACE exposure, the probability of depressive mood surges by 57%–76%, further confirming the aforementioned dose-gradient relationship. Most critically, suicide risk escalates progressively with the accumulation of ACE exposure, ultimately resulting in adolescents who have suffered multiple traumas facing a suicide risk approximately ten times higher than that of their unharmed peers10. Therefore, ACEs are not merely transient childhood adversities but represent a significant etiological factor underlying contemporary adolescent mental health crises, including anxiety disorders, clinical depression, and heightened suicidality.
Artificial intelligence (AI) is now widely integrated into education, entertainment, healthcare, and social interaction, providing numerous conveniences. Representative tools like ChatGPT enhance student engagement, collaborative learning, and educational accessibility11, while also offering emotional support and gaming rewards12. However, in terms of specific usage purposes, AI use can be divided into different aspects such as learning/work, social interaction, and entertainment, and there are differences in usage durations under different purposes, which may have different impacts on mental health. Individuals with ACEs exhibit higher susceptibility to mental health challenges, including increased risks of depression, anxiety, and suicidal behaviors13. While AI interactions may temporarily alleviate their loneliness and emotional dysregulation, current systems primarily function as affective amplifiers, lacking intervention strategies and facing ethical, safety, and efficacy issues. Consequently, the use of AI may exacerbate anxiety and depression, potentially leading to severe outcomes such as heightened suicidal tendencies14,15.
Research indicates that individuals with ACEs are more prone to negative emotions, with depressive symptoms worsening in correlation with the number of ACEs experienced16. Although the link between ACEs and mental health is well-established, the impact of AI on the psychology of this link remains unclear. One theory posits that individuals with ACEs may resort to online engagement as a maladaptive coping mechanism to escape reality17. Specifically, for individuals with adverse childhood experiences, when using AI for learning/work purposes for a long time to assist in learning or work tasks, they may experience high levels of stress, which can trigger anxiety and depression. In terms of social interaction, excessive time spent on socializing with AI may reduce real—life social interactions, leading to a decline in social skills and subsequently affecting mental health. For entertainment purposes, long—term addiction to AI—based entertainment may disrupt life rhythms, trigger digital addiction problems, and increase the risks of anxiety and depression. Driven by real-world pressures, they may turn to the virtual world, where AI engagement could foster addiction-like behaviors, thereby increasing the risks of anxiety and depression18. Therefore, we hypothesize that the usage durations of AI for different purposes (learning/work, social interaction, and entertainment) mediate the relationship between adverse childhood experiences and mental health outcomes. In this study, we employ propensity score matching to control for confounders and conduct causal mediation analysis to explore the mechanisms among college students, aiming to clarify the potential mediating role of AI usage.
Methods
Participants and procedures
This study was conducted smoothly in Jiangxi Province, China, from April to May 2025. For participant selection, the study employed a convenience sampling method, choosing three universities within Jiangxi Province—Jiangxi Police College, Nanchang Medical College, and Nanchang University—as the primary research sites. Participants voluntarily registered for the study. Prior to data collection, researchers provided a comprehensive explanation of the research objectives, specific procedures, and participants’ rights to all potential participants. To ensure that each participant fully understood the research content and voluntarily participated, we obtained their informed consent. The study placed great emphasis on confidentiality and anonymity, solemnly assuring participants that their responses would be kept strictly confidential and used solely for the purpose of this research, thereby alleviating any concerns about the security of their personal information.
The research protocol underwent meticulous design and repeated deliberation, ultimately receiving ethical approval from the Medical Ethics Committee of the Health Science Center at Yangtze University (Approval Number: 202502001). During the implementation of the survey, investigators distributed questionnaire links via Wenjuanxing, a well-known online survey platform in China. The entire participation process strictly adhered to the principle of voluntariness, with informed consent obtained from all participants before data collection. To further ensure confidentiality and anonymity, researchers reiterated that participants’ responses would remain confidential. The questionnaire was scientifically designed, with an estimated completion time of 10 to 15 min. The survey was scheduled during class sessions or evening self-study periods organized by the universities. To express gratitude for participants’ support and cooperation, they received compensation ranging from 2 to 5 yuan upon completing the questionnaire.
During the data collection phase, a total of 3,674 students initially filled out the questionnaires. To ensure high-quality and reliable data, we carefully reviewed each questionnaire and excluded 338 due to logical inconsistencies in their answers, achieving a response rate of 89.2%. Additionally, it was found that 600 students had not used AI in the past month and therefore did not belong to the target research group, leading to their exclusion. Ultimately, we retained 2,736 valid questionnaires for subsequent analysis.
Measures
Basic demographic variables
Social demographic information was gathered, including age, gender, academic year, residence whether the participant was a single child, and their field of study.
Adverse childhood experiences
Adverse Childhood Experiences (ACEs) were measured using the Adverse Childhood Experiences Questionnaire in this study19. This questionnaire is designed to assess 10 types of childhood trauma. Five of these are personal traumas: physical abuse, verbal abuse, sexual abuse, physical neglect, and emotional neglect. The other five relate to family dysfunction: having an alcoholic parent, a mother who is a victim of domestic violence, a family member in prison, a family member diagnosed with a mental illness, and the disappearance of a parent due to divorce, death, or abandonment. Responses to the questionnaire were binary, recorded as either “yes” or “no,” and the total score was calculated by counting the number of “yes” responses. The total score ranges from 0 to 10, with higher scores indicating a greater severity of adverse childhood experiences. In this study, participants who scored 0 were classified into the “no ACEs” group, while those scoring between 1 and 10 were assigned to the “ACEs-exposed” group. The scale has been widely used in studies involving Chinese populations20. In this study, the Cronbach’s α = 0.78.
Depression and anxiety stress
In this study, we utilized the Chinese version of the Depression Anxiety and Stress Scale–21 (DASS-21) to evaluate the level of psychological distress among participants21. The DASS-21 consists of three subscales: depression, anxiety, and stress, with each subscale containing seven items. For example, an item from the depression subscale is “I was unable to become enthusiastic about anything”; an item from the anxiety subscale is “I felt scared without any good reason”; and an item from the stress subscale is “I tended to overreact to situations.” Participants rated each item on a four-point Likert scale to indicate how well the statements described their experiences over the previous week. Higher total scores on each subscale indicate greater levels of psychological distress. The DASS-21 has been extensively used in studies involving Chinese populations22. In this study, the Cronbach’s α values for each subscale were as follows: 0.87 for the stress subscale, 0.84 for the anxiety subscale, and 0.85 for the depression subscale.
Sleep quality
Sleep quality was assessed using the Single-Item Sleep Quality Scale (SQS) developed by Snyder et al.23. Participants were asked to respond to the question, “How would you rate your overall sleep quality over the past seven days?” They rated their sleep on an 11-point scale, ranging from 0 (indicating terrible sleep) to 10 (indicating excellent sleep). A higher score indicates better sleep quality. This scale has been widely utilized to measure sleep quality among the Chinese population24.
Loneliness
In this study, the Three-Item Loneliness Scale was utilized to assess loneliness among participants25. This scale employs a three-point Likert scale format, allowing participants to respond with “hardly ever,” “some of the time,” or “often.” One of the items on the scale asks, “How frequently do you feel that you lack companionship?” Total scores are calculated by summing the scores of individual items, with a possible range from 3 to 9. Higher total scores indicate a greater degree of loneliness. The Chinese version of the scale has demonstrated strong reliability and validity26. In this study, the Cronbach’s alpha for the scale was found to be 0.79.
Suicidal ideation
To assess suicidal ideation, we employed a single item: “In the past 12 months, have you had any suicidal thoughts?” We utilized a 5-point Likert scale for scoring, ranging from 1 (“never”) to 5 (“always”). This item has been widely adopted and validated in numerous previous studies, ensuring its reliability and relevance in the context of evaluating the mental health of college students27,28.
AI use
In this study, we assessed participants’ use of AI through a set of structured questions based on previous study29. First, participants were asked whether they use AI in their daily lives. If the answer was affirmative, they were then required to provide specific details on the duration of AI usage for different purposes. The study focused on three primary purposes of AI use: learning/work, social interaction, and entertainment. For learning/work, participants reported the time spent using AI for tasks such as writing papers or programming. For social interaction, they indicated the time spent chatting with AI and seeking virtual companionship. Lastly, for entertainment, participants noted the time allocated to gaming and creative activities involving AI. We utilized a scale similar to a 5-point Likert format to measure duration, where the values corresponded to the following time ranges: 1–0 to 0.5 h, 2–0.5 to 1 h, 3–1 to 2 h, 4–2 to 4 h, and 5–over 4 h. Each category included only one item (e.g., “On average, how much time do you spend using AI for social interaction per day?”).
Statistical analysis
Descriptive analysis
In this study, qualitative data were presented as frequencies (N) and percentages (%), while quantitative data were expressed as mean ± standard deviation (SD).
Propensity score matching analysis
To control for confounding bias, we conducted propensity score matching analysis. By statistically emulating a randomized controlled trial (RCT) design, we utilized nearest-neighbor matching with a caliper width of 0.05. This approach ensured that each participant in the experimental group (individuals with adverse childhood experiences) was paired with the closest match in the control group (college students without adverse childhood experiences), maintaining a maximum propensity score difference of 0.05 and preserving a 1:1 case–control ratio to ensure balanced groups.
Linear regression and causal mediation analysis
We employed linear regression to examine the relationships among key variables, including adverse childhood experiences, AI usage, stress, anxiety, depression, sleep quality, loneliness, and suicidal ideation. Subsequently, focusing on the potential mediating role of AI usage between adverse childhood experiences and mental health outcomes, we performed causal mediation analysis to decompose the total effects of outcomes into direct and indirect pathways (mediated by specific variables). The analysis outputs included the average causal mediation effect (ACME), average direct effect (ADE), and total effect.
All statistical analyses were conducted using SPSS version 21.0, while PSM and the causal mediation models were implemented in R version 4.1.3 (mediation package). A two-tailed test was employed, with statistical significance set at P < 0.05.
Results
Sample Characteristics
A total of 2,736 college students participated in this survey, with 794 (29.0%) classified into ACEs group and the remaining 1,942 in the non-ACEs group. The gender distribution revealed a female predominance, comprising 1,129 males (41.2%) and 1,607 females (58.7%). In terms of academic standing, juniors constituted the largest subgroup (35.4%, n = 968), while medical majors represented the highest professional proportion (22.3%, n = 610). Notably, 2,012 participants (73.5%) came from single-child families. Regarding residence, 1,372 (50.1%) were urban residents and 1,364 (49.9%) were rural residents. The mean age was 18.55 years (SD = 1.46; SE = 20.49). Detailed demographic information is presented in Table 1.
Propensity Score Matching Analysis
To minimize confounding bias, we implemented propensity score matching to balance covariates between the ACEs and non-ACEs groups. Figure 1 and Table 2 illustrate the pre- and post-matching changes in sample sizes and propensity score distributions. The standardized mean difference (SMD) decreased from 0.2799 pre-matching to 0.0043 post-matching, well below the 0.1 threshold. The validity of the matching was confirmed through comparisons of demographic characteristics within the ACEs group: for the academic field, the pre-matching χ2 test showed significant group differences (χ2 = 11.4, P = 0.022), which became non-significant post-matching (χ2 = 1.029, P = 0.905). These results demonstrate that PSM effectively controlled for confounding factors, thereby reducing bias in the observed associations.

The distribution of propensity score before and after PSM analysis.
Results of liner regression analysis
Table 3 presents the results of linear regression analyses examining the associations between ACEs and various mental health outcomes, including depressive symptoms, anxiety symptoms, stress levels, loneliness, sleep quality, and suicidal ideation. After controlling for basic socio-demographic variables, two models were constructed for each mental health variable: Model 1 included only ACEs, while Model 2 incorporated both ACEs and AI usage. The analyses revealed that higher ACEs scores were associated with more severe mental health issues. Specifically, depressive symptoms were significantly positively correlated with ACEs (Model 1: β = 0.600, P < 0.001; Model 2: β = 0.565, P < 0.001). Anxiety symptoms exhibited a similar positive association (Model 1: β = 0.654, P < 0.001; Model 2: β = 0.617, P < 0.001). Stress levels showed a strong positive correlation with ACEs (Model 1: β = 0.708, P < 0.001; Model 2: β = 0.674, P < 0.001). Furthermore, loneliness was significantly positively related to ACEs (Model 1: β = 0.241, P < 0.001; Model 2: β = 0.227, P < 0.001). Additionally, sleep quality was negatively correlated with ACEs, indicating poorer sleep quality associated with higher ACEs scores (Model 1: β = -0.19, P < 0.001; Model 2: β = -0.186, P < 0.001). Lastly, suicidal ideation was positively associated with ACEs (Model 1: β = 0.074, P < 0.001; Model 2: β = 0.072, P < 0.001).
In terms of AI usage, social AI usage was positively correlated with depressive symptoms (Model 2: β = 0.409, P < 0.001), anxiety symptoms (Model 2: β = 0.338, P < 0.001), stress levels (Model 2: β = 0.366, P < 0.001), loneliness (Model 2: β = 0.167, P < 0.001), and suicidal ideation (Model 2: β = 0.034, P < 0.05). However, learning/work-related AI usage did not show significant associations with the examined mental health outcomes. Entertainment-related AI usage was only found to be associated with anxiety symptoms (Model 2: β = 0.257, P < 0.05).
Results of causal mediation analysis
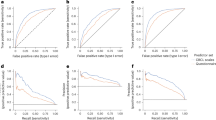
Figure 2 presents the detailed results of the causal mediation analysis. In the relationship between adverse childhood experiences (ACEs) and loneliness, both direct and indirect effects significantly contribute to the increased odds of loneliness, with socializing acting as a mediating factor. The total effect is 0.24 (95% confidence interval [CI]: 0.18–0.31; P < 0.001), the Average Causal Mediation Effect (ACME) is 0.01 (95% CI 0.01–0.02; P < 0.001), the Average Direct Effect (ADE) is 0.23 (95% CI 0.16–0.30; P < 0.001), and the proportion of the mediated effect is 5.2% (95% CI 2.2%–10.0%; P < 0.001). For stress, both direct and indirect effects are also significant. The total effect is 0.71 (95% CI 0.56–0.88; P < 0.001), the ACME is 0.03 (95% CI 0.01–0.06; P < 0.001), the ADE is 0.68 (95% CI 0.53–0.85; P < 0.001), and the proportion of the mediated effect is 4.4% (95% CI 1.6%–8.0%; P < 0.001). For anxiety symptoms, both direct and indirect effects are significant as well. The total effect is 0.65 (95% CI 0.51–0.81; P < 0.001), the ACME is 0.03 (95% CI 0.01–0.06; P < 0.001), the ADE is 0.62 (95% CI 0.49–0.78; P < 0.001), and the proportion of the mediated effect is 4.9% (95% CI 2.1%–9.0%; P < 0.001). For suicidal ideation, both direct and indirect effects are significant. The total effect is 0.07 (95% CI 0.06–0.09; P < 0.001), the ACME is 0.002 (95% CI 0.001–0.003; P < 0.001), the ADE is 0.07 (95% CI 0.06–0.09; P < 0.001), and the proportion of the mediated effect is 2.6% (95% CI 0.6%–6.0%; P < 0.01). For depressive symptoms, both direct and indirect effects play significant roles. The total effect is 0.60 (95% CI 0.46–0.76; P < 0.001), the ACME is 0.03 (95% CI 0.01–0.06; P < 0.001), the ADE is 0.57 (95% CI 0.43–0.73; P < 0.001), and the proportion of the mediated effect is 5.4% (95% CI 2.2%–10.0%; P < 0.001).

Causal mediation analysis of Socializing/Enterainment in the relationship between adverse childhood experiences and mental health outcomes among the participants. ACME, average causal mediation effect; ADE, average direct effect; proportion mediated = ACME (average)/total effect.
Finally,
Fig. 2 also demonstrates that entertainment can also act as a mediating factor, significantly increasing the likelihood of anxiety in individuals with adverse childhood experiences, both directly and indirectly. The total effect is 0.65 (95% CI 0.52–0.82; P < 0.001), the ACME is 0.03 (95% CI 0.01–0.05; P < 0.001), the ADE is 0.63 (95% CI 0.49–0.79; P < 0.001), and the proportion of the mediated effect is 4.2% (95% CI 1.8%–8.0%; P < 0.001).
Discussion
This study reveals the complex associations between ACEs and various negative psychological conditions. The results indicate that ACEs significantly impact loneliness, stress, anxiety, suicidal ideation, and depressive symptoms, with AI usage playing a mediating associated role. Specifically, the total effect on loneliness is 0.24 (95% CI 0.18–0.31; P < 0.001), with a mediating effect proportion of 5.2%; the total effect on stress is 0.71 (95% CI 0.56–0.88; P < 0.001), with a mediating effect proportion of 4.4%; the total effect on anxiety symptoms is 0.65 (95% CI 0.51–0.81; P < 0.001), with a mediating effect proportion of 4.9%; the total effect on suicidal ideation is 0.07 (95% CI 0.06–0.09; P < 0.001), with a mediating effect proportion of 2.6%; and the total effect on depressive symptoms is 0.60 (95% CI 0.46–0.76; P < 0.001), with a mediating effect proportion of 5.4%. Additionally, the exposure rate of ACEs in this sample is 29%. The proportion of ACE exposure among respondents varies across different studies, which may be attributed to the diversity of participant samples or variations in the selection and measurement of ACE types9,30.
In this comprehensive study, our findings unveil the underlying mechanisms through which AI exerts adverse effects on mental health, however, we should also recognize that AI is not entirely negative, and its possible adaptive uses may bring positive effects. This discovery challenging the prevailing belief in its therapeutic benefits. Numerous previous studies have claimed that AI can significantly improve mental health issues and even hold potential for clinical application31. Existing trials demonstrating the mental health benefits of AI predominantly focus on its instrumental applications, such as structured therapeutic tools. In fact, in certain specific situations, AI does show the value of its adaptive applications. For example, for some people who are unable to engage in face-to-face social interactions due to physical reasons, structured therapeutic tool-type AI can provide a convenient way of communication, to some extent meeting their social needs and relieving part of their psychological pressure. Moreover, the relationship between AI and mental health is bidirectional. It can not only cause problems but also play a positive role under appropriate guidance and use. However, individuals with ACEs often develop a compensatory over-reliance on virtual relationships, which may ultimately lead to anxiety and pathological dependence32,33. Empirical research indicates a positive correlation between depressive symptoms and the frequency of using companion AI. Those with heightened feelings of loneliness or tendencies toward rumination are especially prone to engaging in maladaptive interactions with chatbots. Frequent AI interactions not only fail to alleviate their psychological distress but may also exacerbate it33,34. In previous studies, researchers typically employed professional social AI with therapeutic effects and implemented intervention measures through algorithms, yielding positive and effective outcomes31. Nevertheless, most AI used by people in daily life lacks the professional capabilities necessary for psychological counseling. Our study also corroborates this point: non-therapeutic-oriented social AI plays a significant partial mediating role in nearly all mental health issues faced by ACE patients, while entertainment-focused AI only mediates the risk factor of anxiety. This strongly suggests that the use of non-therapeutic social AI may further aggravate psychological problems.
Our research findings further reveal that AI acts as a partial mediator association between ACEs and various mental health issues, highlighting the complex and far-reaching impact of social AI usage on the mental health of individuals with ACEs. The potential pathway for this impact may be outlined as follows: adverse childhood experiences lead to impaired social functioning→individuals tend to engage in low-risk AI-based social activities→mental health problems are further exacerbated→reliance on social AI deepens. Existing research indicates that ACE experiences can negatively affect an individual’s interpersonal relationships and may trigger anxiety35,36,37,38. For those experiencing anxiety symptoms, excessive use of social AI may worsen their conditions. Individuals with high levels of anxiety often avoid interpersonal interactions, leading to increased feelings of isolation and entrapment in a cycle of repetitive negative thinking. To address their emotional needs and mitigate negative emotions, they may turn to social media. However, this passive, non-face-to-face mode of interaction frequently results in heightened loneliness39. Moreover, compared to human interactions, engagements with AI do not fully satisfy our basic social needs. This unmet need can lead to feelings of social deprivation, thereby increasing tendencies toward depression and loneliness40. Therefore, it is crucial to recognize that the inappropriate use of social AI can have significant adverse effects on the ACE population.
Several limitations in this study need to be addressed: 1.Measurement Issues: Recall bias, social desirability bias, and self-reporting bias may interfere with the estimation of effect sizes. Additionally, in this study, a single—item approach was used to measure the duration of AI usage for different purposes. Since a single item has limitations when measuring complex concepts, this can also affect the reliability and validity of the measurement results. Moreover, variables such as “previous mental illness history”, “recent negative life events (e.g., academic failure)”, and “social support level” were not included in the measurement tools in this study. These factors may simultaneously affect ACEs exposure, AI usage, and mental health, leading to result bias, which is also one of the limitations of this study. 2. Sampling Concerns: The convenience sampling of Chinese university students is susceptible to selection bias; therefore, stratified random sampling is preferred for future research. 3. Design Limitations: Under the cross-sectional design, despite utilizing Propensity Score Matching (PSM) and mediation analysis, it is challenging to clarify the sequence of variables and establish causality. Additionally, unmeasured confounders and the potential for reverse causality may also exist.
Conclusion
This study clearly indicates that the exposure rate of ACEs in the research sample is 29%. Additionally, it explicitly reveals the intricate associations between ACEs and various negative psychological conditions, with AI usage serving a mediating role. The research results demonstrate that ACEs significantly impact loneliness, stress, anxiety symptoms, suicidal ideation, and depressive symptoms. There are variations in the total effects of ACEs on different negative psychological conditions as well as in the proportions of the mediating effects of AI usage. For instance, the total effect of ACEs on loneliness is 0.24 (95% CI 0.18–0.31; P < 0.001), with a mediating effect proportion of 5.2%. These findings offer a novel perspective for the in-depth exploration of the psychological impact mechanisms of ACEs and provide a crucial basis for the subsequent development of targeted intervention strategies that incorporate AI factors.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AI:
-
Artificial intelligence
- ACEs:
-
Adverse childhood experiences
- PSM:
-
Propensity score matching
- CMA:
-
Causal mediation analysis
- DASS-21:
-
The depression anxiety and stress scale-21
- SASS:
-
Self-consciousness scale
- ACME:
-
The average causal mediation effect
- ADE:
-
The average direct effect
References
Kessler, R. C. et al. Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. Br. J. Psychiatr. J. Ment. Sci. 197(5), 378–385 (2010).
Swedo, E. A. et al. Prevalence of adverse childhood experiences among adolescents. Pediatrics 154(5), e2024066633 (2024).
Mao, P. et al. Progress in qualitative study on mental health service demand of children and adolescents with adverse childhood experiences. J. Central South Univ. Med. Sci. 47(8), 1163–1170 (2022).
Xue, J. et al. Patterns of adverse childhood experiences and their associations with depression, life satisfaction and short-form video addiction in Chinese college students. Child Abuse Negl. 158, 107091 (2024).
Wado, Y. D. et al. The association between adverse childhood experiences and mental disorders among adolescents in Kenya, Indonesia, and Vietnam: Evidence from the National Adolescent Mental Health Surveys. Child Adolesc. Psychiatr. Ment. Health 19(Suppl 1), 86 (2025).
Madigan, S. et al. Adverse childhood experiences: A meta-analysis of prevalence and moderators among half a million adults in 206 studies. World Psychiatr. Off. J. World Psychiatr. Assoc. 22(3), 463–471 (2023).
Wang, L., Keyworth, C. & O’Connor, D. B. Effects of childhood trauma on mental health outcomes, suicide risk factors and stress appraisals in adulthood. PLoS ONE 20(6), e0326120 (2025).
Yao, K. et al. The effect of childhood trauma on suicide risk: The chain mediating effects of resilience and mental distress. BMC Psychiatr. 23(1), 865 (2023).
Hughes, K. et al. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Publ. Health 2(8), e356–e366 (2017).
Meeker, E. C. et al. The impact of adverse childhood experiences on adolescent health risk indicators in a community sample. Psychol. Trauma Theory Res. Pract. Policy 13(3), 302–312 (2021).
Amarathunga, B. J. A. E. & Studies, D. ChatGPT in education: Unveiling frontiers and future directions through systematic literature review and bibliometric analysis. Asian Educ. Dev. Stud. 13(5), 412–431 (2024).
Ta, V. et al. User experiences of social support from companion chatbots in everyday contexts: Thematic analysis. J. Med. Internet Res. 22(3), e16235 (2020).
Jin, Y. et al. The lasting effects of childhood trauma on developing psychiatric symptoms: A population-based, large-scale comparison study. Global Ment. Health (Cambridge, Engl.) 11, e98 (2024).
Graham, S. et al. Artificial intelligence for mental health and mental illnesses: An overview. Curr. Psychiatr. Rep. 21(11), 116 (2019).
Salil, R., Jose, B., Cherian, J., Sheeja, P. R. & Vikraman, N. Digitalized therapy and the unresolved gap between artificial and human empathy. Front. Psych. 15, 1522915 (2024).
Merrick, M. T. et al. Unpacking the impact of adverse childhood experiences on adult mental health. Child Abuse Negl. 69, 10–19 (2017).
Nagata, J. M. et al. Adverse childhood experiences and early adolescent cyberbullying in the United States. J. Adolesc. 95(3), 609–616 (2023).
Shannon, H., Bush, K., Villeneuve, P. J., Hellemans, K. G. & Guimond, S. Problematic social media use in adolescents and young adults: Systematic review and meta-analysis. JMIR Ment. Health 9(4), e33450 (2022).
Felitti, V. J. et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ACE) study. Am. J. Prevent. Med. 14(4), 245–258 (1998).
Zhu, B. et al. Adverse childhood experiences and depressive symptoms among lesbian and bisexual women in China. BMC Womens Health 23(1), 679 (2023).
Lovibond, P. F. & Lovibond, S. H. The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 33(3), 335–343 (1995).
Wang, C. et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Publ. Health 17(5), 1729 (2020).
Snyder, E., Cai, B., DeMuro, C., Morrison, M. F. & Ball, W. A new single-item sleep quality scale: Results of psychometric evaluation in patients with chronic primary insomnia and depression. J. Clin. Sleep Med. 14(11), 1849–1857 (2018).
Chen, S., Sun, L. & Zhang, C. Adaptation and validity of the sleep quality scale among Chinese drivers. PLoS ONE 16(11), e0259813 (2021).
Hughes, M. E., Waite, L. J., Hawkley, L. C. & Cacioppo, J. T. A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 26(6), 655–672 (2004).
Yang, M., Wang, H. & Yao, J. Relationship between intergenerational emotional support and subjective well-being among elderly migrants in China: The mediating role of loneliness and self-esteem. Int. J. Environ. Res .Publ. Health 19(21), 14567 (2022).
Zhao, J. et al. Shame and suicidal ideation among undergraduates in China: The mediating effect of thwarted belongingness and perceived burdensomeness. Int. J. Environ. Res. Publ. Health 17(7), 2360 (2020).
Kessler, R. C., Berglund, P., Borges, G., Nock, M. & Wang, P. S. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990–1992 to 2001–2003. JAMA 293(20), 2487–2495 (2005).
Wang, Y. et al. Epidemiology of mental health problems among patients with cancer during COVID-19 pandemic. Transl. Psychiatr. 10(1), 263 (2020).
Madigan, S. et al. Prevalence of adverse childhood experiences in child population samples: A systematic review and meta-analysis. JAMA Pediatr. 179(1), 19–33 (2025).
D’Alfonso, S. AI in mental health. Curr. Opin. Psychol. 36, 112–117 (2020).
Li, L. et al. Network analysis of adverse childhood experiences and problematic internet use among Chinese adolescents. Addict. Behav. 165, 108300 (2025).
Fang, C. M., Liu, A. R., Danry, V., Lee, E., Chan, S. W. T., Pataranutaporn, P., Maes, P., Phang, J., Lampe, M. & Ahmad, L. How AI and human behaviors shape psychosocial effects of Chatbot use: A longitudinal randomized controlled study (2025).
Lai, L., Pan, Y., Xu, R. & Jiang, Y. Depression and the use of conversational AI for companionship among college students: The mediating role of loneliness and the moderating effects of gender and mind perception. Front. Public Health 13, 1580826 (2025).
Antoniou, G., Lambourg, E., Steele, J. D. & Colvin, L. A. The effect of adverse childhood experiences on chronic pain and major depression in adulthood: a systematic review and meta-analysis. Br. J. Anaesth. 130(6), 729–746 (2023).
Fitzgerald, M. & Gallus, K. Emotional support as a mechanism linking childhood maltreatment and adult’s depressive and social anxiety symptoms. Child Abuse Negl. 108, 104645 (2020).
Baldini, V. et al. Association between adverse childhood experiences and suicidal behavior in affective disorders: A systematic review and meta-analysis. Eur. Psychiatr. J. Assoc. Eur. Psychiat. 68(1), e58 (2025).
Baldini, V. et al. Association between adverse childhood experiences and suicidal behavior in schizophrenia spectrum disorders: A systematic review and meta-analysis. Psychiatry Res. 329, 115488 (2023).
Kardefelt-Winther, D. Behavior DJCiH: A conceptual and methodological critique of internet addiction research: Towards a model of compensatory internet use. Comput. Human Behav. 31(31), 351–354 (2014).
Roberts, J. A., Young, P. D., David, M. E. & Publications, J. S. The epidemic of loneliness: A 9-year longitudinal study of the impact of passive and active social media use on loneliness.
Acknowledgements
We would like to thank all participants who generously shared their time to participate in this survey.
Author information
Authors and Affiliations
Contributions
YY W, MX L, H R, ZZ D WQL analyzed the data and wrote manuscript; JY Z, XF H, YD Y and M L revised the manuscript; ZZ D and WQ L edited the manuscript, YY W, MX L, H R, JY Z, XF H, YD Y collected data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
All participants provided written informed consent, and the Medical Ethics Committee of the Health Science Center, Yangtze University (Approval Number: 202502001) approved this study. And all methods were performed in accordance with t Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Y., Lv, M., Huang, R. et al. Mediation role of artificial intelligence exposure in adverse childhood experiences: related mental health risks among college students. Sci Rep 16, 6278 (2026). https://doi.org/10.1038/s41598-026-37352-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-37352-x
