
Abstract
This study aimed to analyze the influencing factors for preterm birth (PTB) and low birth weight (LBW) among infants with congenital heart disease (CHD) in Changsha City and to provide a scientific basis for the development of targeted preventive measures. Data on infants with CHD were collected from all the birth defects (BDs) monitoring hospitals in Changsha City from January 1, 2022 to December 31, 2024. The diagnosis of BDs was coded according to the World Health Organization’s International Classification of Diseases. CHD was classified under codes Q20-Q26 in the ICD-10. Multivariable binary logistic regression was used to identify factors associated with PTB and LBW among infants with CHD. 1,460 infants with CHD were included. The overall rates of PTB and LBW among infants with CHD were 15.89% and 14.38%, respectively. Maternal folic acid supplementation was identified as a protective factor for PTB in infants with CHD (aOR = 0.40, 95%CI: 0.23–0.67), while gestational diabetes mellitus (GDM) (aOR = 3.28, 95%CI: 1.44–7.48), and comorbidity with other BDs (aOR = 1.82, 95%CI: 1.36–2.44) were identified as risk factors. Minority ethnicity was identified as a protective factor for LBW among infants with CHD (aOR = 0.35, 95%CI: 0.14–0.89), while rural residence (aOR = 1.46, 95%CI: 1.02–2.08), history of spontaneous abortion (aOR = 1.96, 95%CI: 1.33–2.87), pregnancy-induced hypertension (aOR = 3.31, 95%CI: 1.03–10.67), female sex (aOR = 1.59, 95%CI: 1.18–2.16), and comorbidity with other BDs (aOR = 2.31, 95%CI: 1.70–3.13) were identified as risk factors. The rates of PTB and LBW among infants with CHD were relatively high in Changsha City. For PTB, maternal folic acid supplementation was a protective factor, whereas GDM and comorbidity with other BDs were risk factors. For LBW, minority ethnicity was a protective factor, whereas rural residence, history of spontaneous abortion, pregnancy-induced hypertension, female sex, and comorbidity with other BDs were risk factors. Further studies are needed to elucidate the determinants of PTB and LBW among infants with CHD, with analyses stratified by specific CHD subtypes.
Similar content being viewed by others


Introduction
Congenital heart disease (CHD) is a structural abnormality of the heart or abnormal cardiovascular development at birth1. The incidence of CHD is estimated to be around 17–18 per 1,000 live births worldwide2. In China, the incidence is approximately 17.3‰, making CHD the most common birth defects (BDs) and a leading cause of neonatal mortality3. The reported incidence of CHD tends to be higher in developed regions, which is largely attributable to more advanced prenatal screening and diagnostic technologies that enhance detection capabilities4. From 1990 to 2021, the global age-standardized prevalence rate of CHD remained stable (estimated annual percentage change: 0.04%, 95% CI: 0.03%-0.05%)5. Analysis of the epidemiology of adverse pregnancy outcomes in infants with CHD has significant implications for clinical care and prevention, alongside contributing to the reduction of neonatal mortality.
Preterm birth (PTB) and low birth weight (LBW) are also important public health problems worldwide and are the major adverse pregnancy outcomes in perinatal health. CHD in infants is associated with various adverse pregnancy outcomes. Some studies have reported that infants with CHD have a higher risk of PTB and LBW than the general population6,7. In contrast, other studies suggested that PTB and LBW among infants with CHD may have higher risk factors for growth retardation8,9. Ishikawa et al. found that infants with a combination of CHD and LBW carried a higher risk of death beyond that of either alone10. Furthermore, adverse pregnancy outcomes are correlated with the subsequent growth and development of newborns. Shaw et al. found that PTB could be associated with poor neurodevelopment and behavioral outcomes11. Steurer et al. reported that PTB with a gestational age of 28–32 weeks have the highest mortality or morbidity compared with their peers without CHD12. Nakano et al. presented that LBW among infants might express adipose tissue maldevelopment and have a greater likelihood of developing insulin resistance and its associated comorbidities later in life13. While previous studies have linked CHD to adverse pregnancy outcomes such as PTB and LBW, most studies examined PTB and LBW separately or focus on narrow risk factors. Few studies have conducted comprehensive comparisons of demographic, obstetric, and neonatal factors for both PTB and LBW within the same CHD cohort in China. This hinders identification of shared and distinct etiological pathways needed for integrated prevention. Moreover, the majority of studies have been conducted in Western populations, and the findings may not be generalizable to Chinese populations due to significant differences in genetics, socioeconomic conditions, healthcare access, and maternal lifestyle.
Therefore, we conducted an epidemiological study on PTB and LBW among infants with CHD from the Birth Defects Surveillance System in Hunan Province, to describe the recent rates of PTB and LBW among infants with CHD in Changsha City, and identify the independent factors associated with PTB and LBW in this specific population, thereby filling a critical knowledge gap and informing region-specific preventive strategies.
Materials and methods
Data sources
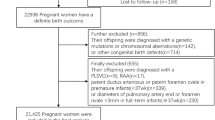
This study utilized data on infants with CHD obtained from the Hunan Provincial Birth Defects Surveillance System. These data were collected from all monitoring hospitals in Changsha City from January 1, 2022 to December 31, 2024. The diagnosis of BDs was coded according to the World Health Organization’s International Classification of Diseases. CHD was classified under codes Q20-Q26 in the ICD-10. Inclusion criteria: (1) diagnosis of CHD within seven days after birth; (2) singleton pregnancy; (3) live birth; (4) gestational age ≥ 28 weeks; (5) availability of comprehensive medical records. Exclusion criteria: (1) diagnosis of patent ductus arteriosus and/or patent foramen ovale solely due to prematurity; (2) diagnosis of isolated patent foramen ovale and/or patent ductus arteriosus (< 3 mm in diameter). Surveillance data included demographic characteristics, reproductive histories, maternal pregnancy information, newborn information, and other key information. Specifically, demographic characteristics included maternal age, ethnicity, education level, and residence. Reproductive histories included gravidity, parity, and history of stillbirth and spontaneous abortion. Maternal pregnancy information included maternal folic acid supplementation, mode of conception, pregnancy-induced hypertension, gestational diabetes mellitus (GDM), and threatened abortion. Newborn information included neonatal sex, and comorbidity with other BDs.
Definitions
PTB is defined as delivery occurring at a gestational age between 28 and 37 weeks. LBW is defined as a newborn weight less than 2,500 g when they were born.
Data quality control
To standardize the monitoring of BDs, the Changsha Municipal Health Commission organizes annual training courses related to BDs monitoring and carries out comprehensive quality control examinations each year. Additionally, comprehensive quality control inspections were conducted across the city. Data were meticulously collected and reported by experienced doctors, and subsequently reviewed by senior doctors to ensure accuracy and reliability. Finally, the supervisor and technical guidance departments checked and reviewed the collected data for completeness and accuracy.
Statistical analysis
Continuous data are presented as mean ± standard deviation. Categorical data are presented as frequencies and percentages, and inter-group comparisons are conducted using Chi-square tests.
Multivariable binary logistic regression analysis was used to identify factors associated with PTB and LBW among infants with CHD, and the results are presented as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). In model 1, the dependent variable was PTB (yes = 1, no = 0). In model 2, the dependent variable was LBW (yes = 1, no = 0). A P value of less than 0.05 was considered significant.
Ethics approval and consent to participate
This study was approved by the Changsha Hospital for Maternal & Child Health Care Affiliated to Hunan Normal University (NO: EC-20240625-19). The requirement for informed consent was waived by the Changsha Hospital for Maternal & Child Health Care Affiliated to Hunan Normal University due to the retrospective nature of the study. We confirmed that all methods were performed in accordance with the relevant guidelines and regulations.
Results
Rates of PTB and LBW among infants with CHD
A total of 238,144 live births were included in this study. Among them, 3,469 cases with BDs and 1,460 infants with CHD were identified. The overall rates of PTB and LBW among infants with CHD were 15.89% and 14.38%, respectively. From 2022 to 2024, the rates of PTB in infants with CHD were 14.11%, 16.04%, and 18.10%, respectively, and remained generally steady (χ2trend = 2.865, P = 0.091). From 2022 to 2024, the rates of LBW among infants with CHD were 12.14%, 14.58%, and 17.14%, respectively, and showed an upward trend (χ2trend = 4.891, P = 0.027) (Table 1).
Characteristics of the study population
Among 1,460 infants with CHD, 445 infants (30.5%) were comorbid with other BDs. Among this subgroup, 22.0% (98/445) were PTB and 22.2% (99/445) had LBW. The average maternal age was 30.9 ± 5.0 years, ranging from 17 to 55 years, and 38.0% of them were aged 30–34 years. The majority of ethnic groups were the Han ethnicity (94.6%). The largest proportion of mothers (73.9%) held a college degree or above. The majority (79.4%) resided in urban areas. About 37.0% of mothers were primigravidae and 56.9% were primipara. The proportions of mothers with no history of stillbirth and no history of spontaneous abortion were 97.1% and 85.9%, respectively. Folic acid supplementation was reported by 94.9% of mothers, and 91.6% of all mothers had a natural conception. Moreover, 99.1% had no pregnancy-induced hypertension, 98.2% had no GDM, and 98.9% had no threatened abortion. Among the infants, 52.2% were male, and 69.5% had no other BDs (Table 2).
Univariate analysis for PTB and LBW among infants with CHD
Univariate analysis identified the following factors associated with PTB in infants with CHD: education level, gravidity, stillbirth history, spontaneous abortion history, maternal folic acid supplementation, pregnancy-induced hypertension, GDM, and comorbidity with other BDs. Similarly, factors associated with LBW included: ethnicity, education level, residence, spontaneous abortion history, pregnancy-induced hypertension, GDM, comorbidity with other BDs, and neonatal sex (Table 2).
Multivariable binary logistic regression analysis for PTB in infants with CHD
Multivariable binary logistic regression analysis identified maternal folic acid supplementation as a protective factor for PTB in infants with CHD (aOR = 0.40, 95%CI: 0.23–0.67), while GDM (aOR = 3.28, 95%CI: 1.44–7.48) and comorbidity with other BDs (aOR = 1.82, 95%CI: 1.36–2.44) were identified as risk factors (Table 3).
Multivariable binary logistic regression analysis for LBW among infants with CHD
Multivariable binary logistic regression identified minority ethnicity as a protective factor for LBW among infants with CHD (aOR = 0.35, 95%CI: 0.14–0.89), while rural residence (aOR = 1.46, 95%CI: 1.02–2.08), history of spontaneous abortion (aOR = 1.96, 95%CI: 1.33–2.87), pregnancy-induced hypertension (aOR = 3.31, 95%CI: 1.03–10.67), female sex (aOR = 1.59, 95%CI: 1.18–2.16), and comorbidity with other BDs (aOR = 2.31, 95%CI: 1.70–3.13) were identified as significant risk factors (Table 4).
Discussion
Overall, we have described a contemporary population-based analysis using robust 2022–2024 surveillance data from Changsha, reflecting current medical and demographic trends. We performed a comprehensive, concurrent evaluation of potential risk factors for PTB and LBW in CHD infants across sociodemographic, reproductive, behavioral, clinical, and neonatal domains, and identified independent associated factors specific to this population, thereby providing actionable insights for targeted intervention.
This study found that the overall rates of PTB and LBW among infants with CHD in Changsha City between 2022 and 2024 were 15.89% and 14.38%, respectively, which are lower than those reported in previous studies for this population. For example, Olugbuyi et al. reported that the rates of PTB and LBW among infants with CHD in Canada (2008–2018) were 18.9% and 17.9%, respectively14. Mustafa et al. found that the PTB rate in infants with CHD was 23.2% between 2011 and 201615. Palma et al. found that the PTB rate in infants with CHD was 23% between 2003 and 201716. However, the rates of PTB and LBW among infants with CHD in Changsha City were higher than those reported for the general population in previous studies. For instance, in general infants, the rate of PTB was 6.27% in Shanghai City in 202017, and the rate of LBW was 7.7% in Ghana in 201718. Some previous studies found that CHD in fetuses would have an increased risk of adverse pregnancy outcomes such as stillbirths, neonatal deaths, PTB, and LBW15,19,20. The underlying reason may be that the pathophysiological stress of CHD in the fetus can trigger mechanisms that lead to preterm labor and impaired fetal growth. However, these mechanisms require further investigation. From 2022 to 2024, the rate of PTB in infants with CHD remained generally steady (χ2trend = 2.865, P = 0.091), yet the rate of LBW among infants with CHD showed an upward trend (χ2trend = 4.891, P = 0.027). We speculate that this increase may be attributable to improved survival rates among LBW infants with CHD, potentially due to incremental refinements in perinatal and neonatal care.
Several factors associated with PTB and LBW among infants with CHD were identified in this study. First, maternal folic acid supplementation was identified as a protective factor for PTB in infants with CHD, which is consistent with a previous study21. Wu et al. found that folic acid supplementation for at least 3 months during pregnancy was associated with a 20% lower risk of PTB compared with no supplementation22. Bortolus et al. reported that folic acid 4.0 mg versus 0.4 mg daily supplementation started before pregnancy to 12th gestational week was associated with fewer spontaneous abortions, PTB and with a better composite outcome23. However, a systematic review and meta-analysis of randomized controlled trials reported that folic acid supplementation during pregnancy did not prevent PTB24. In this study, folic acid supplementation was not associated with LBW infants with CHD. The lack of association could be explained by several factors. First, the preventive effect of folic acid on fetal growth restriction seems to be limited. For instance, a previous study reported that cumulative folic acid supplementation for more than 4 months was a protective factor for the delivery of small-for-gestational-age infants25. Second, it may also be influenced by the timing of folic acid supplementation during pregnancy, the dosage taken, and interactions with other nutritional supplements. Furthermore, the etiology of LBW is highly complex. Beyond gestational age, it is strongly influenced by factors such as placental function, maternal nutritional status, and other pregnancy complications. The confounding effects of these factors may have obscured a protective effect of folic acid per se.
Second, GDM was identified as a risk factor for PTB in infants with CHD. This finding is consistent with the general newborn population26, indicating that the adverse effect of GDM on pregnancy outcomes remains significant even in the presence of CHD. Lin et al. reported that pregnant women with GDM have a higher risk of LBW (aOR = 1.18, 95%CI: 1.06–1.32)27. This may occur because high amniotic glucose levels in GDM promote increased amniotic fluid secretion by the amnion, which in turn raises the risk of premature rupture of membranes (PROM) and can lead to PTB.
Third, comorbidity with other BDs was identified as a risk factor for both PTB and LBW among infants with CHD. Dolan et al. reported that a singleton liveborn infant with BDs was 2.7 times more likely to be delivered preterm before 37 weeks of gestation and 3.6 times more likely to have a LBW at less than 2,500 g28. Our findings strongly align with and extend the work of Adam et al., who recently reported elevated risks of PTB and LBW in infants with major congenital anomalies29. By focusing specifically on infants with CHD who have additional BDs, we demonstrate that the cumulative burden of congenital malformations significantly exacerbates the risk of adverse perinatal outcomes, even when the primary defect is cardiac in nature. This underscores the importance of enhanced prenatal monitoring for pregnancies where CHD is diagnosed alongside other anomalies.
Fourth, spontaneous abortion history was identified as a risk factor for LBW infants with CHD. This association is notably aligned with the report by Sun et al., who demonstrated that pregnant women with a history of spontaneous abortion had significantly higher odds of PTB (aOR = 1.38, 95%CI: 1.07–1.79) compared to those without such a history30. Given that PTB is a leading cause of LBW, we postulate that the observed link between spontaneous abortion history and LBW in infants with CHD is likely mediated, at least in part, by an increased rate of PTB. The association may be driven by the mechanism of cervical insufficiency in women with prior spontaneous abortion, which can cause painless second-trimester dilation and lead to PTB or prelabor rupture of membranes.
Fifth, pregnancy-induced hypertension was identified as a risk factor for LBW infants with CHD. This finding is consistent with previous studies of the general population31,32,33. A meta-analysis showed that the odds of LBW increased nearly four times among women with pregnancy-induced hypertension than normotensive women34. The underlying mechanism is thought to involve vascular endothelial injury and microthrombus formation, which impairs placental exchange function. A key consequence is hypertension-induced insufficient utero-placental perfusion, leading to fetal intrauterine growth restriction and LBW35. Therefore, systematic monitoring and management of blood pressure during pregnancy is crucial for reducing the risk of LBW.
Sixth, minority ethnicity was identified as a protective factor for LBW in infants with CHD. This finding is consistent with a prior local study reporting an association between ethnicity and birth weight in Changsha’s general population36. While studies in other contexts, such as the United States, have highlighted how maternal anthropometry, gestational weight gain, and parental ethnicity collectively shape ethnic disparities in LBW rates37, the protective effect observed in our setting likely arises from a distinct set of factors. These may include unique genetic backgrounds, cultural practices, socioeconomic profiles, lifestyle patterns, and dietary habits prevalent among the minority ethnic groups in our region.
Seventh, mothers living in rural areas had a higher risk of LBW infants with CHD. Yan et al. reported that maternal place of residence was associated with birth weight among infants with CHD21, which is consistent with our study. Some previous studies of the general population reported that mothers living in rural areas had a higher risk for LBW than in urban areas such as in Changsha City38, in India39. A previous study in Tanzania reported that area of residence was found to be maternal factors associated with LBW40. This disparity may be attributed to socioeconomic inequalities, including lower average incomes, poorer access to prenatal care and health education, and differences in nutritional awareness among women in rural areas compared to their urban counterparts. Moreover, female sex was identified as a risk factor for LBW infants with CHD, which is consistent with some previous studies of the general population such as in Changsha City41, Guangxi Province42, Kenya43. However, some previous studies reported that male sex was a significant risk factor for LBW44,45.
Limitation
Our study has limitations. First, the retrospective design, reliant on surveillance data, inherently lacks control over potentially confounding variables. Notably, important risk factors such as PROM, maternal smoking, or fetal growth restriction, were not available for analysis. The absence of these variables may lead to residual confounding. Second, we analyzed CHD as a collective entity without further classification. CHD encompasses a wide spectrum of defects with vastly different hemodynamic impacts. This lack of stratification limits the clinical specificity of our results. Finally, regarding folic acid, our data only captured supplementation as a binary variable (yes/no). Information on the timing, duration, and dosage of supplementation was not available, which might explain the lack of an observed protective effect against LBW and deserves further investigation.
Conclusion
In summary, our data indicated that the rates of PTB and LBW among infants with CHD were relatively high in Changsha City. For PTB, maternal folic acid supplementation was a protective factor, whereas GDM and comorbidity with other BDs were risk factors. For LBW, minority ethnicity was a protective factor, whereas rural residence, history of spontaneous abortion, pregnancy-induced hypertension, female sex, and comorbidity with other BDs were risk factors. Further studies are needed to elucidate the determinants of PTB and LBW among infants with CHD, with analyses stratified by specific CHD subtypes.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Zikarg, Y. T., Yirdaw, C. T. & Aragie, T. G. Prevalence of congenital septal defects among congenital heart defect patients in East africa: A systematic review and Meta-Analysis. Plos One. 16, e250006 (2021).
Wu, W., He, J. & Shao, X. Incidence and mortality trend of congenital heart disease at the Global, Regional, and National Level, 1990–2017. Med. (Baltimore). 99, e20593 (2020).
Chen, Z., Wang, Y., Lan, F., Li, S. & Wang, J. An expanded view of infertility: the challenge of the changing profiling of major birth defects in China. Biosci. Trends. 17, 318–321 (2023).
Chen, X. et al. Incidence, Distribution, disease Spectrum, and genetic deficits of congenital heart defects in china: implementation of prenatal ultrasound screening identified 18,171 affected fetuses from 2,452,249 pregnancies. Cell. Biosci. 13, 229 (2023).
Zhang, X. et al. Global, Regional, and National burden of congenital heart disease, 1990–2021: A systematic analysis for the global burden of disease study 2021. Eur. J. Pediatr. 184, 253 (2025).
Reddy, R. K. et al. Prematurity and congenital heart disease: A contemporary review. Neoreviews 23, e472–e485 (2022).
Cabral, G. et al. Congenital heart disease: epidemiological profile of live Births, geographical distribution and Temporal trends in Brazil from 2012 to 2022. Bmc Cardiovasc. Disord. 25, 599 (2025).
Lee, J. S., Noh, O. K. & Park, J. E. Neonatal risk factors for growth retardation in infants with congenital heart disease. J. Korean Med. Sci. 38, e196 (2023).
Trivedi, A., Browning, C. K., Jatana, V., James-Nunez, K. & Gordon, A. Growth and risk of adverse Neuro-Developmental outcome in infants with congenital heart disease: A systematic review. Acta Paediatr. 112, 53–62 (2023).
Ishikawa, T. et al. The association between congenital heart disease and small for gestational age with regard to the prevalence and outcomes. Acta Paediatr. 110, 1009–1016 (2021).
Shaw, J. C., Crombie, G. K., Palliser, H. K. & Hirst, J. J. Impaired oligodendrocyte development following preterm birth: promoting Gabaergic action to improve outcomes. Front. Pediatr. 9, 618052 (2021).
Steurer, M. A. et al. Mortality and major neonatal morbidity in preterm infants with serious congenital heart disease. J. Pediatr. 239, 110–116 (2021).
Nakano, Y. Adult-Onset diseases in low birth weight infants: association with adipose tissue maldevelopment. J. Atheroscler Thromb. 27, 397–405 (2020).
Olugbuyi, O. et al. Impact of socioeconomic status and residence distance on infant heart disease outcomes in Canada. J. Am. Heart Assoc. 11, e26627 (2022).
Mustafa, H. J. et al. Preterm birth of infants prenatally diagnosed with congenital heart Disease, Characteristics, Associations, and outcomes. Pediatr. Cardiol. 41, 972–978 (2020).
Palma, A., Morais, S., Silva, P. V. & Pires, A. Congenital heart defects and preterm birth: outcomes from a referral center. Rev. Port Cardiol. 42, 403–410 (2023).
Lv, Y., Xu, L., He, Z., Liu, X. & Guo, Y. The association between pregnancy levels of blood lipids and the risk of preterm birth. Sci. Rep. 14, 10800 (2024).
Banchani, E. & Tenkorang, E. Y. Determinants of low birth weight in ghana: does quality of antenatal care matter? Matern Child. Health J. 24, 668–677 (2020).
De Silvestro, A. et al. Morbidity and mortality in premature or low birth weight patients with congenital heart disease in three European pediatric heart centers between 2016 and 2020. Front. Pediatr. 12, 1323430 (2024).
Chen, X., Bhombal, S., Kwiatkowski, D. M., Ma, M. & Chock, V. Y. Impact of congenital heart disease on the outcomes of very low birth weight infants. Am. J. Perinatol. 41, 1815–1821 (2024).
Yan, H. et al. Prevalence of congenital heart disease in Chinese children with different birth weights and its relationship to the neonatal birth weight. Front. Pediatr. 10, 828300 (2022).
Wu, Y. et al. The association between periconceptional folic acid supplementation and the risk of preterm birth: A Population-Based retrospective cohort study of 200,000 women in China. Eur. J. Nutr. 60, 2181–2192 (2021).
Bortolus, R. et al. Efficacy of 4.0 Mg versus 0.4 Mg folic acid supplementation on the reproductive outcomes: A randomized controlled trial. Nutrients 13, (2021).
Saccone, G. & Berghella, V. Folic acid supplementation in pregnancy to prevent preterm birth: A systematic review and Meta-Analysis of randomized controlled trials. Eur. J. Obstet. Gynecol. Reprod. Biol. 199, 76–81 (2016).
Zhang, J. et al. Association between maternal folic acid supplementation in pregnancy and abnormal fetal growth: evidence from a birth cohort baseline survey. Clin. Nutr. Espen. 66, 135–141 (2025).
Wei, Y. et al. Preconception diabetes mellitus and adverse pregnancy outcomes in over 6.4 million women: A Population-Based cohort study in China. Plos Med. 16, e1002926 (2019).
Lin, R. et al. Association of gestational diabetes mellitus diagnosed at different time points in oral glucose tolerance test with adverse pregnancy outcomes: A retrospective cohort study. Front. Endocrinol. 16, 1493520 (2025).
Dolan, S. M. et al. The contribution of birth defects to preterm birth and low birth weight. Obstet. Gynecol. 110, 318–324 (2007).
Adam, H. et al. Impact of major congenital anomalies on preterm birth and low birth weight. Sci. Rep. 15, 24872 (2025).
Sun, H., Mao, J., Su, X. & Du, Q. Impact of spontaneous abortion history and induced abortion history on perinatal outcomes of Singleton pregnancies. Bmc Public. Health. 23, 2360 (2023).
Habtegiorgis, S. D. et al. Prevalence and determinants of low birth weight in ethiopia: A multilevel Meta-Analysis and systematic review. Public. Health. 239, 215–223 (2025).
Arabzadeh, H. et al. The maternal factors associated with infant low birth weight: an umbrella review. Bmc Pregnancy Childbirth. 24, 316 (2024).
Mettananda, S. et al. Composition, Determinants, and risk factors of low birth weight in Sri Lanka. Plos One. 20, e318554 (2025).
Getaneh, T., Negesse, A., Dessie, G. & Desta, M. The impact of pregnancy induced hypertension on low birth weight in ethiopia: systematic review and Meta-Analysis. Ital. J. Pediatr. 46, 174 (2020).
Zhang, H. G., Yang, L., Qiao, Z. X. & Guo, W. Effect of gestational hypertension on fetal growth Restriction, endocrine and cardiovascular disorders. Asian J. Surg. 45, 1048–1049 (2022).
Sun, M. et al. Association between paternal Pre-Pregnancy body mass index with preterm birth and low birth weight. Front. Pediatr. 10, 955544 (2022).
Dola, S. S. & Valderrama, C. E. Exploring parental factors influencing low birth weight on the 2022 Cdc natality dataset. Bmc Med. Inf. Decis. Mak. 24, 367 (2024).
Huang, Z., Tan, X., Wang, J. & Zhang, A. Maternal Pre-Pregnancy body mass index and gestational weight gain on adverse birth outcomes in Chinese newborns: A retrospective study. J. Heatlh Popul. Nutr. 43, 165 (2024).
Singh, D. et al. Prevalence and correlates of low birth weight in india: findings from National family health survey 5. Bmc Pregnancy Childbirth. 23, 456 (2023).
Lyimo, G. S. & Moshi, F. V. The prevalence of low birth weight and its associated maternal factors among women of reproductive age who gave birth to live babies within five years preceding the survey in tanzania: an analysis of data from the 2015-16 Tanzania demographic and health survey and malaria indicators survey. Bmc Pregnancy Childbirth. 24, 523 (2024).
Zhang, A. et al. The epidemic characteristics of low birth weight and its influencing factors in Changsha from 2018 to 2021. J. Hunan Normal Univ(Med Sci). 21, 116–127 (2024).
Feng, B. Y. et al. Risk factors for adverse pregnancy outcomes among Zhuang ethnic pregnant women: A cohort study in Guangxi, China. Curr. Med. Sci. 41, 219–227 (2021).
Kassie, G. A. et al. Socioeconomic inequality and determinants of low birth weight in kenya: A multilevel analysis using 2022 demographic and health survey. Ital. J. Pediatr. 51, 222 (2025).
Rao, J. et al. Trend and risk factors of low birth weight and macrosomia in South China, 2005–2017: A retrospective observational study. Sci. Rep. 8, 3393 (2018).
Lat, C., Murila, F. & Wamalwa, D. Prevalence and factors associated with low birth weight among newborns in South Sudan. Afr. Health Sci. 23, 149–158 (2023).
Acknowledgements
The authors are grateful to all staff participating in the research.
Author information
Authors and Affiliations
Contributions
Jin Fu: Manuscript preparation, data collection, study design, statistical analysis, writing and editing. Jing Liu: Study design, statistical analysis, and writing. Bei Zhang, Jinlian Wang, and Yongchun Wen: Data collection. Jie Fang: Manuscript revision. Huan Chen: Manuscript preparation, study design, review, and editing. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fu, J., Liu, J., Zhang, B. et al. Factors associated with preterm birth and low birth weight among infants with congenital heart disease in Changsha City, China, 2022–2024. Sci Rep 16, 6308 (2026). https://doi.org/10.1038/s41598-026-37371-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-37371-8
