
Abstract
The aim of this study was to determine whether a low-intensity exercise may influence outcomes of skin temperature measured by infrared thermography (IRT) in the presence or not of delayed-onset muscle soreness (DOMS). Seventeen participants were recruited (12 men, age 24 ± 6 years, body mass 72.6 ± 12.5 kg, and height 1.8 ± 0.1 m). They visited the laboratory on two days with 48 h in between. On day 1, participants performed a 10-minute low-intensity treadmill walk followed by a squat protocol to induce DOMS (10 sets of 10 repetitions at 70% of body mass). On day 2, when participants reported DOMS, they returned to the laboratory and completed another 10-minute low-intensity treadmill walk. On each day, quadriceps DOMS was assessed using a numerical pain rating scale, and skin temperature was measured using IRT on both days. The skin temperature was higher before (p = 0.01; d=-0.44) and after walking (p = 0.03; d=-0.39) on the second day when significant DOMS was reported by the participants. However, skin temperature was not altered by light walking prior to the measurements on day 2. In conclusion, low-intensity walking did not induce detectable changes in skin temperature in the quadriceps before or after DOMS, suggesting that that acute, low-intensity exercise is unlikely to be a relevant confounder or enhancer of IRT-based assessment of DOMS.
Similar content being viewed by others

Introduction
Infrared thermography (IRT) measures the surface temperature of an object at a distance, which is advantageous in the case of human assessment for the diagnosis of breast cancer, diabetic neuropathy, or infectious diseases, among others1,2,3,4. However, the outcomes of IRT in sports sciences and rehabilitation, especially for the diagnosis of overuse and traumatic injuries including follow-up of rehabilitation protocols, is still controversial5,6. For example, IRT detects changes in skin temperature (Tsk) depending on the training protocol, but complementary physiological measurements are still necessary for better monitoring athletes’ performance and muscle health7. Similarly, asymmetries in Tsk have been related to lower limb injuries during a soccer season, but in this case, the diagnosis was also dependent on additional measures8. More recently, researchers have been studying whether IRT could be useful as a non-invasive monitoring technique for delayed onset muscle soreness (DOMS)9,10,11.
DOMS is often reported as a response to acute increases in training load, especially those involving exercises with a predominance of eccentric muscle actions12. Its symptoms are also associated with an inflammatory response to micro-ruptures of muscle fibers13. Recent studies have shown that the Tsk measured using IRT might not relate to creatine kinase activity at the peak of DOMS in sedentary people, who are most susceptible to this impairment14,15,16. If DOMS results from inflammation, which in turn produces heat, why is IRT unable to capture this heat? One hypothesis is that, although inflammation increases muscle blood flow17, muscle damage may cause skin vasoconstriction, so limiting heat transference from the muscle to the skin18,19. Recently a study showed that high-intensity exercise increases Tsk 24 h after exercise but the presence of DOMS decreases this response20. For this reason, some studies have evaluated methods to alter peripheral vascularity (such as cooling tests), aiming to enhance the capacity of IRT to detect muscle damage or fatigue by providing a greater gradient between skin and deeper tissues to assess the Tsk recovery under these conditions21,22. However, it is sometimes difficult to control the conditions for these methods in the clinical environment, so simpler evaluations are desired. A low-intensity walking may offer a simple and accessible approach to influence peripheral thermal responses in the presence of exercise-induced muscle damage. Therefore, the aim of this study was to determine whether a low-intensity walking exercise elicits changes in Tsk in participants with DOMS.
Materials and methods
We recruited 17 participants for this study (12 men) from the university community. They had mean (standard deviation) age of 24 (6) years, body mass of 72.6 (12.5) kg, and height of 1.8 (0.1) m being all of similar physical activity level according to the International Physical Activity Questionnaire (IPAQ-SF). Sample size complied with the sample estimation of a minimum of 15 participants for a large effect size expected (ESF = 0.4) for data on mean Tsk variation, with an α error of 5% and a power of 95%23, considering a repeated measure ANOVA design. Sample size calculation was performed with the software G*Power (University of Düsseldorf, Düsseldorf, Germany).
To take part in the study, participants should have at least one year of prior practice in strength exercises and be familiar with squat exercises on Smith machines. Despite all being physically active, they were instructed to avoid performing physical exercises from 2 days before the start of the tests until the end of their participation in the study, as well as not to intake any anti-inflammatory drugs or analgesics, energy drinks, sports supplements, tobacco and alcohol24. Participants with a history of lower limb injuries over the previous 6 months were excluded25. All participants signed an informed consent form following the Declaration of Helsinki, and the implementation of the study was approved by the Committee of Ethics and Human Research of the University of Valencia (IRB: 2626957).
Experimental design
The protocol consisted of two days of measurements, with two moments each day: before (PRE-WALKNODOMS) and after low-intensity walking (POST-WALKNODOMS) on day 1 without the presence of DOMS, and before (PRE-WALKDOMS) and after low-intensity walking (POST-WALKDOMS) on day 2 with the presence of DOMS. On day 1, participants performed a low-intensity walking task followed by a squat protocol to induce muscle damage and DOMS. On day 2 (48 h after day 1), the low-intensity walking was performed again. Before and after both walks (days 1 and 2) and the squat exercise (day 2), measurements of IRT and rate of perceived exertion were performed. Muscle soreness perception was measured on both days only before walking. Figure 1 summarizes the experimental design.

The experimental design depicts the two days of data collection, separated by a day of rest with measures before (PRE-WALKNODOMS) and after walking (POST-WALKNODOMS) without delayed onset muscle soreness (DOMS) on day 1 and before (PRE-WALKDOMS) and after walking (POST-WALKDOMS) with presence of DOMS on day 2. IRT: Infrared thermography; NPRS: Numeric pain rate scale (for DOMS evaluation); Borg: report of rate of perceived exertion using Borg’s scale.
Walking protocol
A low-intensity walking protocol was conducted aimed at disturbing skin blood flow and therefore showing the susceptibility of IRT measurements to changes in Tsk in the region of interest (ROI) over a muscle under a condition of DOMS or not. The walking was performed on an ergometric treadmill (Jog Forma DDJ5EL, TechnoGym, Gambettola, Italy) set at a 1% slope, lasted 10 min, with the participants walking at their preferred speed26. The speed was adjusted by the participants in the initial 3 min so that they experienced a rate of perceived exertion corresponding to 12 (light) points as measured by the Borg scale27. They should not run during the walking exercise. After the 3 initial minutes, the same speed as day 1 was set for 10 min of walking on day 2.
DOMS induction
To induce DOMS in the lower limbs, with greater emphasis on the quadriceps muscles, all participants performed 10 sets of 10 repetitions of squats with 2 min of rest between sets. The squats were performed at a rhythm controlled by a metronome at 60 bpm, marking 1 s for extension and 2 s for knee flexion, thus ensuring emphasis on the eccentric phase28. Participants completed the squat protocol on a Smith machine with a load adjusted to 70% of the individual body mass29. The task consisted of holding a barbell attached to a Smith machine with the load on the shoulders, and perform a squat until the knees reached a 90° flexion angle. To ensure this angulation and the correct completion of the task, an evaluator provided verbal guidance as well as verbal feedback for postural adjustment and movement execution. The power output of all repetitions was monitored with an encoder (Chronojump, Barcelona, Spain) (Fig. 2), observing an excellent intraclass correlation coefficient (single rater-measurement, absolute-agreement, and 2-way random-effects model; ICC = 0.98 & p < 0.001, CI95%[0.96, 0.99])30, and therefore suggesting a homogeneity of power output production during all the repetitions. For this variable, one participant’s file was corrupted, so only the results of 16 participants are presented.

Squat protocol with the mean power output of 10 repetitions in each set. The figure was obtained with the data of 16 participants as one participant was removed due to problems in power output acquisition. W: Watts.
DOMS and rate of perceived exertion assessment
DOMS was assessed using a numeric pain rating scale (NPRS). After familiarization to the scale, participants were asked to verbally report soreness intensity on a scale from 0 (minimum) to 10 (maximum)31. To assess DOMS, the participants were instructed to perform a squat until reaching 90° of knee flexion, and to report quadriceps soreness for each leg32. The DOMS assessments were always performed by the same researcher.
The rate of perceived exertion was assessed using the 20 points Borg scale27, in which participants gave a verbal numerical result corresponding to their perception after being questioned by the evaluator. Just as for DOMS, participants were introduced to the scale and instructed in its application. DOMS was assessed before walking on day 1 and day 2.
Skin temperature
Tsk was assessed using a thermographic camera (resolution of 320 × 240 pixels, NETD < 40 mK at 30º, and measurement uncertainty of ± 2 °C or 2%, E54 model, Flir Systems Inc., Wilsonville, Oregon, USA) at four moments: before days 1 and 2 baseline measurements and after days 1 and 2 walks. Firstly, the camera was turned on 10 min before taking measurements and participants were asked to undertake a room adaptation routine for 10 min in the measurement room33. The participants remained at rest in an orthostatic position with their lower limbs exposed and instructed to move as little as possible and not touch the evaluated regions. All thermal images were taken 1 m from the participant, with the camera lens positioned perpendicular to the participants25. The collection and processing of thermographic data followed the parameters recommended by the TISEM checklist24.
ROIs were defined as the anterior and posterior thighs and anterior and posterior legs for both lower limbs. The demarcation of each thigh was carried out by identifying the point closest to the groin; then a horizontal line was drawn to the lateral edge of the thigh; the line contoured the thigh down to the height of the upper edge of a netting fabric that supported equipment from another study; and then the line was led horizontally to the medial edge of the thigh; finally, the line was drawn around the thigh until it joins the initial point. The lower height of the contralateral thigh ROI was delimited at the same height to that which had the netting attached. For the posterior portion of the thigh, the same references were used. A similar process was used to define leg ROIs. The upper limit was the widest part of the calf, while the lower limit was the narrowest part of the tibia. An example of the delimitation of ROIs is shown in Fig. 3.

Regions of interest (ROIs) are demarcated by green lines on each limb and bilaterally for (A) anterior thigh, (B) posterior thigh, (C) anterior leg and (D) posterior leg. All thermographic photos were taken from the same distance. The examples above have been zoomed in for better visualization.
To obtain the mean temperature from the ROIs, we used an emissivity of 0.98 and a commercial software package (Thermacam Researcher Pro 2.10 software, FLIR, Wilsonville, Oregon, USA). We also calculated the temperature variation for each moment (Post – Pre walking) on both days as a function of the baseline measurement of each day (∆Tsk). All measurements were performed in a temperature-controlled laboratory with air conditioning. The mean (standard deviation) of the ambient conditions for day 1 was 21.9 (0.6) °C and relative humidity of 51.8 (6.5) %, and for day 2 was 22.2 (0.7) °C and relative humidity of 50.1 (13.9) %.
Statistical analyses
Statistical analyses were undertaken using RStudio (version 2023.03.1). Data normality (mean temperature and ∆Tsk) was verified using the Shapiro-Wilk test (p > 0.05). The homoscedasticity of the data was verified with Levene’s test and the sphericity with Mauchly’s test. A Friedman test was carried out to compare rate of perceived effort. Also, a one-way ANOVA was used to compare DOMS at PRE-WALKNODOMS (day 1), PRE-WALKDOMS and POST-WALKDOMS (day 2). Also, an ANOVA of repeated measures was performed for the mean temperature with the following intra-subject factors: laterality [right, left], moment [Baseline, Post-walking], day [day 1, day 2 (with DOMS)] and ROI [anterior thigh, posterior thigh, anterior leg, posterior leg]. For ∆Tsk, a similar analysis was performed without the moment factor. Bonferroni tests were used as a pairwise comparison. These analyses were complemented with the effect size: the partial eta squared (η2) for the ANOVAs, classified as large (> 0.14), moderate (0.06–0.13) and small (0.01–0.05), and the Cohen effect (d’ Cohen) for pairwise comparisons, which were classified as large (> 0.8), moderate (0.5–0.8) and small (0.2–0.5). These results were graphed using the ggstatsplot package (version 0.10)34. The significance level was set at 0.05.
Results
There was no difference in the rate of perceived effort during the walking conditions between any of the measures and conditions [p(3,18) = 0.345; X² = 3.318; PRE-WALKNODOMS (7.5 ± 1.6 points), POST-WALKNODOMS (8.0 ± 1,5 points), PRE-WALKDOMS (7.9 ± 2.1 points), POST-WALKDOMS (8.0 ± 1.7 points).
DOMS results are summarized in Fig. 4. In the right thigh, DOMS values were higher at PRE-WALKDOMS [p(1,18) < 0.001; F = 16.11] compared to PRE-WALKNODOMS. Similarly, the left thigh showed higher DOMS values at PRE-WALKDOMS [p(1,18) < 0.001; F = 16.84] compared to PRE-WALKNODOMS.

Delayed onset muscle soreness report (points 0 to 10) during the quadriceps squat task for each leg before (PRE-WALKNODOMS) and after walking (POST-WALKNODOMS) without delayed onset muscle soreness on day 1 and before (PRE-WALKDOMS) and after walking (POST-WALKDOMS) with presence of DOMS on day 2.
Leg effects were not significant in the mean Tsk (p = 0.83) and pre – post difference in Tsk (∆Tsk, p = 0.64), and no main interaction between factors were identified (p > 0.84). Therefore, leg preference was not considered a factor in the following results.
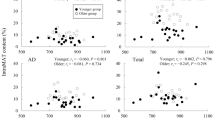
Figure 5 shows the plots comparing both days of measurement at each moment (before and after walking). Before walking, mean Tsk was higher 48 h after DOMS induction for the anterior thigh (small effect size), posterior thigh (moderate effect size), anterior leg (moderate effect size) and posterior leg (large effect size). After walking, mean Tsk was also higher 48 h after DOMS induction for the posterior thigh (small effect size), anterior leg (moderate effect size) and posterior leg (moderate effect size). For ∆Tsk, the main effect on the measurement day was not significant (p = 0.19, Fig. 6).

Comparison of both days of measurement by box plots with individual responses (points and dashed lines) of mean skin temperature. (A) before (PRE-WALKNODOMS) and after walking (POST-WALKNODOMS) without delayed onset muscle soreness (DOMS) on day 1. (B) before (PRE-WALKDOMS) and after walking (POST-WALKDOMS) with presence of DOMS on day 2.

Comparison of both days of measurement by box plots with individual responses (points and dashed lines) of mean skin temperature variation before (PRE-WALKNODOMS) and after walking (POST-WALKNODOMS) without delayed onset muscle soreness (DOMS) on day 1 and before (PRE-WALKDOMS) and after walking (POST-WALKDOMS) with presence of DOMS on day 2.
Discussion
In this study, we investigated whether walking as a strategy to stimulate changes in blood circulation in the lower limbs could influence the measurements of Tsk using IRT when participants refer to the presence of DOMS. The relevance of this question is twofold: for improving protocols for IRT measurements and also to identify possible confounding factors when taking IRT measurements without proper control of prior individual physical activity before the measurement session. Our main results were that 48 h after the induction of DOMS, Tsk was higher in the lower limbs before and after walking, but there was no different response of Tsk (difference between pre- and post-walking Tsk) at muscles with the presence of DOMS due to the low-intensity walking exercise.
The squat protocol successfully induced DOMS, which was verified by a NPRS scale and consistent with previous literature12,13,35. The attempt to implement IRT as an objective alternative to DOMS measurements is not new. Previous studies have shown the applicability of this technology for monitoring muscle damage to be less efficient than for diagnosing microinjuries6,14,36. Furthermore, a systematic review found that IRT does not predict CK activity derived from muscle damage resulting from strenuous exercise37, the same situation that generates DOMS. Therefore, it is possible that the key to successfully measuring DOMS and muscle damage with IRT is to modify the data collection protocol. For example, the use of cold heat stress appears to be able to indicate the vasoconstrictor pattern of athletes after a marathon21. Similarly, a factor capable of disrupting muscle homeostasis was proposed to check whether Tsk responses were different in the presence of DOMS21. Acute exercises may generate transient muscle vasodilation followed by vasoconstriction in the lower limbs and, mainly the behavior of the vessels, is intensity-dependent38. Hence, in our experimental design, the participants performed intense exercise to induce DOMS, which would generate vasoconstriction, and were later subjected to a low-intensity walk aimed at altering their Tsk.
We found that anterior thigh Tsk was not significantly affected by low-intensity walking. This result may indicate that thermoregulatory mechanisms, for example sweating39, could have been activated after this protocol, even though the intensity was controlled and kept at low levels. On the other hand, and contrary to expectations, in the anterior thigh, the mean temperature was higher 48 h post-exercise before walking compared to baseline values. Our hypotheses were doubly rejected. On the one hand, walking could not generate clinically useful changes in Tsk, while IRT was able to describe DOMS even without walking. It is considered advantageous from a clinical point of view. Despite having correlated mechanisms, DOMS and muscle damage do not necessarily exhibit similar behavior over time40. Therefore, despite the presence of DOMS, the muscle damage might not have been sufficient to trigger the mechanisms of muscular vascular constriction suggested before41, through which walking could generate an effect on Tsk.
When comparing the situations with and without DOMS after walking, only the posterior thigh showed a temperature variation, with an increase. The hamstring region was not an agonist in the performance of the exercise that generated DOMS, but showed a thermal response. Yoshizawa et al.38 indicated that the control limb of a DOMS induction also undergoes changes in femoral arterial blood flow, which in this study may have generated changes in Tsk in this region. Future studies may investigate the factors that generate a non-localized effect of DOMS on Tsk in response to muscle damage.
Our study has its limitations. As we did not record participants’ training level and routine with anything more sophisticated than a simple questionnaire, the physical fitness condition may have differed between participants and represented an important confounding factor. Biomarkers of muscle damage, such as creatine kinase, were not included, which can be considered a limitation. Furthermore, we were unable to analyze muscle vasoconstriction and blood flow in the lower limbs. A short-term, low-intensity walking exercise may induce peripheral vasodilation via rhythmic muscle contractions and increased metabolic activity, mechanisms that are well established even at low exercise intensities. While muscle blood flow was not directly measured, the increase in Tsk observed after walking suggests a functional vascular response consistent with reduced vasoconstriction. Although the extent of exercise-induced muscle damage was not quantified in terms of vascular impairment, the temperature response indicates that walking was sufficient to counteract peripheral cooling mechanisms and promote heat dissipation at the skin level.
Conclusion
Low-intensity walking did not induce detectable changes in Tsk in the quadriceps before or after DOMS. Although Tsk was higher when DOMS was present, this increase appeared independent of the acute walking stimulus, suggesting that acute, low-intensity exercise is unlikely to be a relevant confounder or enhancer of IRT-based assessment of DOMS.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Lahiri, B. B., Bagavathiappan, S., Jayakumar, T. & Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 55, 221–235 (2012).
Khaksari, K. et al. Review of the efficacy of infrared thermography for screening infectious diseases with applications to COVID-19. J. Med. Imaging 8, (2021).
Ring, E. F. J. & Ammer, K. Infrared thermal imaging in medicine. Physiol. Meas. 33, R33–R46 (2012).
Kesztyüs, D., Brucher, S. & Kesztyüs, T. Use of infrared thermography in medical diagnostics: a scoping review protocol. BMJ Open. 12, e059833 (2022).
Ioannou, S. Functional infrared thermal imaging: A contemporary tool in soft tissue screening. Sci. Rep. 10, 9303 (2020).
Ramirez-GarciaLuna, J. L., Bartlett, R., Arriaga-Caballero, J. E., Fraser, R. D. J. & Saiko, G. Infrared thermography in wound Care, Surgery, and sports medicine: A review. Front. Physiol. 13, 838528 (2022).
Straburzyńska-Lupa, A., Korman, P., Śliwicka, E., Kryściak, J. & Ogurkowska, M. B. The use of thermal imaging for monitoring the training progress of professional male sweep rowers. Sci. Rep. 12, 16507 (2022).
Menezes, P., Rhea, M. R., Herdy, C. & Simão, R. Effects of strength training program and infrared thermography in soccer athletes injuries. Sports Basel Switzerland 6, (2018).
Al-Nakhli, H. H., Petrofsky, J. S., Laymon, M. S. & Berk, L. S. The use of thermal Infra-Red imaging to detect delayed onset muscle soreness. J. Vis. Exp. 3551 https://doi.org/10.3791/3551 (2012).
Stewart, I. B. et al. Thermal infrared imaging can differentiate skin temperature changes associated with intense single leg Exercise, but not with delayed onset of muscle soreness. J. Sports Sci. Med. 19, 469–477 (2020).
Doménech-García, V., Boudreau, S. A. & Giner-Nicolás, R. Bellosta-López, P. Skin temperature normalizes faster than pressure pain thresholds, pain intensity, and pain distribution during recovery from eccentric exercise. J. Therm. Biol. 111, 103423 (2023).
Cleak, M. J. & Eston, R. G. Muscle soreness, swelling, stiffness and strength loss after intense eccentric exercise. Br. J. Sports Med. 26, 267–272 (1992).
Hotfiel, T. et al. Advances in Delayed-Onset muscle soreness (DOMS): part I: pathogenesis and diagnostics. Sportverletz · Sportschaden. 32, 243–250 (2018).
da Silva, W. et al. Can exercise-induced muscle damage be related to changes in skin temperature? Physiol. Meas. 39, 104007 (2018).
de Carvalho, G., Girasol, C. E., Gonçalves, L. G. C., Guirro, E. C. O. & Guirro, R. R. J. Correlation between skin temperature in the lower limbs and biochemical marker, performance data, and clinical recovery scales. PloS One. 16, e0248653 (2021).
Barboza, J. A. M. et al. Can skin temperature be altered after different magnitudes of eccentric Exercise-Induced muscle damage? Res. Q. Exerc. Sport. 93, 702–709 (2022).
Selkow, N. M. et al. Blood flow after Exercise-Induced muscle damage. J. Athl Train. 50, 400–406 (2015).
Percival, J. M. nNOS regulation of skeletal muscle fatigue and exercise performance. Biophys. Rev. 3, 209–217 (2011).
Chalacheva, P. et al. High levels of peripheral vasoconstriction detected by polysomnography predict more acute severe pain episodes in children with sickle cell anemia. Blood 134, 894–894 (2019).
Da Silva, W. et al. Effect of different volumes of exercise on skin temperature responses over the following 24 hours. J. Therm. Biol. 123, 103923 (2024).
Priego-Quesada, J. I. et al. Effect of a marathon on skin temperature response after a Cold-Stress test and its relationship with Perceptive, Performance, and Oxidative-Stress biomarkers. Int. J. Sports Physiol. Perform. 15, 1467–1475 (2020).
Muñoz-Alcamí, M. et al. Effect of fatigue strength exercise on anterior thigh skin temperature rewarming after cold stress test. J. Therm. Biol. 101, 103098 (2021).
da Silva, W. et al. Relationship between exercise-induced muscle soreness, pain thresholds, and skin temperature in men and women. J. Therm. Biol. 100, 103051 (2021).
Moreira, D. G. et al. Thermographic imaging in sports and exercise medicine: A Delphi study and consensus statement on the measurement of human skin temperature. J. Therm. Biol. 69, 155–162 (2017).
Application of Infrared Thermography in Sports Science. https://doi.org/10.1007/978-3-319-47410-6 (Springer International Publishing, 2017).
Jones, A. M. & Doust, J. H. A 1% treadmill grade most accurately reflects the energetic cost of outdoor running. J. Sports Sci. 14, 321–327 (1996).
Borg, G. A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 14, 377–381 (1982).
Burt, D. G., Lamb, K., Nicholas, C. & Twist, C. Effects of exercise-induced muscle damage on resting metabolic rate, sub-maximal running and post-exercise oxygen consumption. Eur. J. Sport Sci. 14, 337–344 (2014).
Byrne, C. & Eston, R. The effect of exercise-induced muscle damage on isometric and dynamic knee extensor strength and vertical jump performance. J. Sports Sci. 20, 417–425 (2002).
Weir, J. P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength. Cond Res. 19, 231–240 (2005).
Hawker, G. A., Mian, S., Kendzerska, T. & French, M. Measures of adult pain: visual analog scale for pain (VAS pain), numeric rating scale for pain (NRS pain), McGill pain questionnaire (MPQ), short-Form McGill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short Form-36 bodily pain scale (SF. Arthritis Care Res. 63, S240–S252 (2011).
Goodall, S. & Howatson, G. The effects of multiple cold water immersions on indices of muscle damage. J. Sports Sci. Med. 7, 235–241 (2008).
Marins, J. C. B. et al. Time required to stabilize thermographic images at rest. Infrared Phys. Technol. 65, 30–35 (2014).
Patil, I. Visualizations with statistical details: the ‘ggstatsplot’ approach. J. Open. Source Softw. 6, 3167 (2021).
Vickers, A. J. Time course of muscle soreness following different types of exercise. BMC Musculoskelet. Disord. 2, 5 (2001).
Fernández-Cuevas, I., Arnáiz Lastras, J., Escamilla Galindo, V. & Gómez Carmona, P. Infrared thermography for the detection of injury in sports medicine. In Application of Infrared Thermography in Sports Science (ed. Priego Quesada, J. I.) 81–109. https://doi.org/10.1007/978-3-319-47410-6_4 (Springer International Publishing, 2017).
Santos, T. M. D., Bunn, P. D. S., Aidar, F. J., Mello, D. & Neves, E. B. Correlation between creatine kinase (CK) and thermography: a systematic review with meta-analysis. Motricidade 18 (3). https://doi.org/10.6063/MOTRICIDADE.26751 (2022).
Yoshizawa, M., Shimizu-Okuyama, S. & Kagaya, A. Transient increase in femoral arterial blood flow to the contralateral non-exercising limb during one-legged exercise. Eur. J. Appl. Physiol. 103, 509–514 (2008).
Gagnon, D. & Crandall, C. G. Sweating as a heat loss thermoeffector. In Handbook of Clinical Neurology 156 211–232 (Elsevier, 2018).
Nosaka, K., Newton, M. & Sacco, P. Delayed-onset muscle soreness does not reflect the magnitude of eccentric exercise-induced muscle damage. Scand. J. Med. Sci. Sports. 12, 337–346 (2002).
Larsen, R. G., Hirata, R. P., Madzak, A., Frøkjær, J. B. & Graven-Nielsen, T. Eccentric exercise slows in vivo microvascular reactivity during brief contractions in human skeletal muscle. J. Appl. Physiol. 119, 1272–1281 (2015).
Funding
JMMF contribution was funded by a predoctoral grant from the Ministry of Universities of Spain (FPU20/01060). This study was also partially funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES, Financing Code 001) funding WS, and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico funding FPC (CNPq, process 306401/2022-3 and 402108/2023-0) and ASM (process 169461/2023-8).
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. ASM, WdS, ALL, MMF and CSP acquire the data. ASM and JIP-Q worked on the analysis of the data. IA-A, FPC and JIP-Q supervised the project and provided the resources. ASM worked in the first draft of the manuscript. All the authors reviewed and contributed to the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Machado, Á.S., da Silva, W., Lemos, A.L. et al. Impact of a low-intensity exercise prior to infrared thermography measurements on skin temperature under conditions of muscle soreness. Sci Rep 16, 10380 (2026). https://doi.org/10.1038/s41598-026-38531-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-38531-6
