
Abstract
High blood pressure (BP) has been linked to ambient air pollution, and cancer survivors may be particularly vulnerable due to an immune imbalance. We investigated the association between air pollution mixtures and BP among cancer survivors, and evaluated effect modification by physical activity (PA). We included 2,487 cancer survivors in the Korea National Health and Nutrition Examination Survey (2007–2021). The individual and joint associations of three-year average exposures to PM2.5, PM10, CO, NO2, and SO2 with BP were assessed using linear regression models and quantile-based g-computation (QGC), stratified by PA levels. The associations of PM and CO with higher diastolic blood pressure (DBP) were observed in the low PA group (β = 0.60, 95% CI = 0.21, 0.99, P-interaction = 0.018 for PM2.5; β = 1.24, 95% CI = 0.64, 1.83, P-interaction = 0.020 for PM10; β = 1.20, 95% CI = 0.41, 2.00 for CO). Similarly, the associations of air pollution mixtures with DBP were observed only in the low PA level (Ψ = 0.95, 95% CI = 0.30, 1.61 for PM2.5-based mixture; Ψ = 0.71, 95% CI = 0.10, 1.31 for PM10-based mixture), with PM contributing most (70–96%). Our findings suggest that PM and CO are associated with higher DBP among cancer survivors, with PM having the greatest contribution. PA may attenuate the hypertensive effects of air pollution.
Similar content being viewed by others

Introduction
High blood pressure (BP) is one of the most critical risk factors for cardiovascular disease and premature death worldwide1,2,3. Cancer survivors exhibit a higher prevalence of hypertension than cancer-free individuals, due in part to cancer-related factors, including tumor growth and cancer treatment. Tumor masses may invade or cause embolization of arteries or veins, as well as compress adjacent blood vessels4. Cancer treatments, such as chemotherapy and radiotherapy, can induce coagulopathy and cardiotoxicity by inhibiting cardiomyocyte differentiation and promoting thrombosis and angiostenosis4,5. This vascular and hemostatic dysregulation predisposes cancer survivors to hypertension6,7.
Ambient air pollutants such as particulate matter (PM) and several toxic gases, such as carbon monoxide (CO), nitrogen dioxide (NO2), and sulfur dioxide (SO2), have been linked to hypertension8. Inhaled nanoparticles of air pollutants penetrate the alveoli and enter the bloodstream, triggering vascular inflammation and oxidative stress9. The particles also contribute to alterations in the autonomic nervous system and hemodynamic dysfunction10,11 related to arterial vasoconstriction and platelet hyperactivation, thereby contributing to elevated BP5. In cancer survivors, for whom immune balance is disrupted, exposure to environmental toxicants–such as air pollutants–may further exacerbate endothelial injury and inflammation, thereby increasing the risk of hypertension12,13.
Previous studies have investigated the associations between air pollution and BP, primarily focusing on individuals without a history of cancer14,15. However, the findings remain inconclusive and vary depending on the type of pollutants. While PM has demonstrated consistent associations with hypertension, findings for CO, NO2, and SO2 have been inconsistent across studies8,16. In specific demographic subgroups such as men, Asians, and North Americans, stronger associations between ambient air pollution and hypertension or higher BP have been observed15; however, research on this association among cancer survivors remains scarce. Furthermore, the most influential air pollutant contributing to hypertension risk in this population has yet to be elucidated, highlighting the need for targeted investigations. Given that hypertension is associated with higher cardiovascular disease-related mortality in cancer survivors compared to individuals without a history of cancer17, identifying and managing relevant risk factors‒such as air pollution‒is crucial for health promotion in this group. Physical activity (PA) is known to reduce the risk of various chronic conditions, including hypertension18and cardiovascular diseases19; however, cancer survivors may experience challenges in maintaining regular exercise due to treatment-related functional limitations20, potentially placing them at greater risk of hypertension.
Here, we aimed to investigate the association between ambient air pollution and BP among cancer survivors. To disentangle the complex correlations among multiple air pollutants, we applied quantile-based g-computation (QGC) to assess their collective association with BP and examine the relative contributions of individual pollutants21. We hypothesized that air pollution is related to hypertension or higher BP, and that the magnitude of contribution to this association may vary across different air pollutants. We further hypothesized that these associations may be modified by levels of PA, given that PA reduces the risk of hypertension22 and may offer protective effects against PM exposure in cancer survivors23.
Materials and methods
Study population
This study utilized data from the Korea National Health and Nutrition Examination Survey (KNHANES), conducted by the Korea Disease Control and Prevention Agency. KNHANES is a nationwide cross-sectional health survey that evaluates the health and nutritional status of the nationally representative and non-institutionalised population in Korea. KNHANES employs a multiple-stage sampling design based on stratified cluster sampling. The sampling units included districts (dong/eup/myeon), survey enumeration areas, and households, and the stratification variables were region (province), district, and housing type24. The sample weights were constructed to account for the complex survey design, non-response adjustment, and post-stratification to sex- and age-specific population distributions25. Of the 120,181 individuals who participated in KNHANES from 2007 to 2021, we excluded those under 19 years old (n = 26,062), residents of island regions (n = 1,966), pregnant women (n = 423), individuals without air pollution data (n = 4,493), and those with missing key covariates (n = 6,216), leaving 81,021 participants. As air pollution exposure was based on a 3-year average, participants diagnosed with hypertension before the exposure period (n = 14,857) were further excluded. Among 66,164 individuals with complete data on air pollution exposure and covariates, 2,487 participants who self-reported a physician-diagnosed cancer were defined as cancer survivors and included in the main analysis. Participant selection is summarized in Figure S1.
Air pollution exposure assessment
Air pollution exposure was assessed using data provided from the KNHANES26. Pollutant concentrations were estimated by integrating domestic air quality monitoring data, numerical modeling outputs, and satellite-based observations. The community multi-scale air quality model (CMAQ; version 4.7.1) was applied to estimate concentrations, incorporating meteorological inputs from the weather research and forecasting model (WRF; version 3.6.1) and emissions data from the sparse matrix operator kernel emissions model (SMOKE; version 2.7). These inputs allowed the simulation of air pollutant dispersion, chemical transformation, and transport of air pollutants across South Korea. The model produced nationwide air pollution estimates at a 9 km resolution, which were further refined by incorporating satellite-derived aerosol optical depth data to enhance spatial accuracy. A multiple regression model was applied to refine PM2.5 (particles ≤ 2.5 μm) and PM10 (particles ≤ 10 μm) concentrations by integrating aerosol optical depth, meteorological variables (e.g., temperature, humidity), and outputs from the CMAQ model, resulting in an adjusted spatial resolution of 1 km. Long-term air pollution exposure was estimated based on each participant’s residential administrative district. Three-year moving average concentrations of PM2.5, PM10, CO, NO2, and SO2 were calculated to estimate individual-level exposure. All pollutant exposures were standardized by interquartile range (IQR) to enable comparison of effect sizes across different pollutants in subsequent analyses.
Blood pressure measurement and definition of hypertension
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times in a sitting position27. According to the American Heart Association Scientific Statement, the first blood pressure reading obtained during a visit is often higher than subsequent readings, whereas the average of the second and third readings provides a more reliable estimate of blood pressure28. Accordingly, we utilized the average of the second and third readings. Participants were classified as having hypertension if they met one of the following criteria: SBP ≥ 140 mmHg and DBP ≥ 90 mmHg, the use of antihypertensive medication, or a physician’s diagnosis. Those who did not meet these criteria were classified as normotensive.
Physical activity classification
PA engagement was classified into two groups–low and high PA–based on the World Health Organization (WHO) guidelines29, considering both intensity and duration. PA intensity was defined according to the KNHANES questionnaire, which is based on the Global Physical Activity Questionnaire (GPAQ) and categorizes physical activity into moderate– and vigorous–intensity levels. Moderate-intensity activities involved a moderate increase in heart rate or mild shortness of breath, while vigorous-intensity activities caused a substantial increase in heart rate or heavy breathing. Participants who engaged in less than 150 min of moderate-intensity or less than 75 min of vigorous-intensity PA per week were classified as having low PA. Those meeting or exceeding these thresholds were classified as having high PA. Additionally, a separate analysis was conducted based on PA type, categorized into four groups: no exercise, moderate only, vigorous only, and both.
Statistical analysis
Characteristics of the study participants were summarized using descriptive statistics: means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. For air pollutants, summary statistics, including the mean, median, and IQR, were calculated for the 3-year average concentrations of PM2.5, PM10, CO, NO2, and SO2. Additionally, Pearson’s correlation among the five pollutants based on three-year average concentrations was examined.
To examine the association between air pollution exposure and BP-related outcomes, multiple linear regression was performed for continuous outcomes (SBP and DBP), and multiple logistic regression for the binary outcome of hypertension. Results were presented as regression coefficients (β) with 95% confidence intervals (CIs) for SBP and DBP, and odds ratios (ORs) with 95% CIs for hypertension. In addition to the crude model, we applied a reduced model for sensitivity analysis, adjusting for demographic factors (age, sex, residential region, education level, and household income) and lifestyle variables (smoking status, alcohol consumption, and PA engagement). The final model (full model) additionally controlled for metabolic health factors, including obesity, dyslipidemia, and antihypertensive medication use. Stratified analyses by PA level (low vs. high) were performed using the fully adjusted model, and interaction terms between air pollutants and PA levels were included to assess effect modification, with corresponding P-values for interaction reported. To examine the robustness of the associations by PA, we further conducted sensitivity analyses with PA type (no exercise, moderate, vigorous, and both).
To evaluate the joint effects of multiple air pollutants on BP-related outcomes, the QGC model was applied. QGC estimates the overall mixture effect (Ψ) by simultaneously increasing all components by one quantile and fitting a generalized linear model21. The Ψ value represents the expected change in BP associated with a one-quantile increase in all pollutants. In this model, each pollutant is assigned a weight that reflects both the direction and magnitude of its contribution to the overall association, thereby identifying the components that most strongly influence the mixture-outcome association. Positive weights indicate an association with increased BP, while negative weights indicate an association with decreased BP21. The direction of the overall association between mixture and BP reflects the sign of the dominant absolute contributions from positive and negative components30. Two separate mixture models were constructed for analysis: one including PM2.5, CO, NO2, and SO2, and the other including PM10, CO, NO2, and SO2. We conducted QGC analyses separately for PM2.5 and PM10 alongside other gaseous pollutants, given that PM2.5 is physically a subset of PM1031.
All statistical analyses were performed using SAS (version 9.4) and R (version 4.4.1), and the QGC analysis was conducted using the qgcomp package (version 2.17.4).
Results
Participants’ characteristics
The characteristics of the 2,487 cancer survivors included in the analysis are presented in Table 1. The mean age was 59.3 years, and 63.5% were female. The average SBP and DBP were 118.4 mmHg and 74.1 mmHg, respectively, and 17.4% of participants were classified as having hypertension. Additionally, 6.9% reported current use of antihypertensive medication. Based on PA engagement, 26.5% met the criteria for high PA. The majority of participants (63.9%) reported no engagement in physical activity, followed by those who performed only moderate-intensity exercise (20.3%). Additionally, 6.1% engaged only in vigorous-intensity exercise, while 9.7% reported participating in both moderate and vigorous activities. The three-year average concentrations of PM2.5, PM10, and CO were 24.3 µg/m3 (SD: 3.4), 49.1 µg/m3 (SD: 6.2), and 479.8 ppb (SD: 79.9), respectively (Table S1). Air pollutants showed weak to strong correlations ranging from 0.09 to 0.82 (P < 0.0001) (Figure S2).
Associations between air pollution and blood pressure in traditional regression models
In Table 2, greater exposure to PM2.5, PM10, and CO was associated with higher DBP in the full model (β = 0.37, 95% CI = 0.03, 0.70 for PM2.5; β = 0.91, 95% CI = 0.40, 1.42 for PM10; β = 0.89, 95% CI = 0.23, 1.55 for CO). The associations remained robust in the reduced model. We did not find any associations of PM and CO with SBP or hypertension status across the models.
The associations between air pollution and BP were consistent among participants with low PA engagement (Table 3). In the low PA group, we observed positive associations for PM2.5 with SBP (β = 0.70, 95% CI = 0.05, 1.35), and DBP (β = 0.60, 95% CI = 0.21, 0.99), for PM10 with DBP (β = 1.24, 95% CI = 0.64, 1.83), and for CO with DBP (β = 1.20, 95% CI = 0.41, 2.00). No statistically significant associations were observed in the high PA group. The association of PM2.5 and PM10 with DBP differed by PA engagement, with interaction P-values of 0.018 and 0.020, respectively. Table S2 presents the findings from the sensitivity analysis categorized by PA types. For DBP, associations were observed in the no-exercise group with PM2.5 (β = 0.64, 95% CI = 0.23, 1.05), PM10 (β = 1.24, 95% CI = 0.60, 1.88), and CO (β = 1.06, 95% CI = 0.21, 1.90). In the moderate-only group, associations were found with NO2 (β = 1.92, 95% CI = 0.10, 3.74) and CO (β = 2.15, 95% CI = 0.59, 3.72). No statistically significant associations were observed in the vigorous-only or moderate-and-vigorous groups.
Mixture association of air pollutants with blood pressure outcomes
Figure 1 illustrates the QGC results for the total population, showing both the collective association between air pollutant mixtures and DBP, and the relative contributions of individual mixture components. A one-quantile increase in air pollutant exposure (a mixture of PM2.5, CO, NO2, and SO2) was associated with an average of 0.93 mmHg higher DBP (Ψ = 0.93, 95% CI = 0.37, 1.50) (Fig. 1a). A one-quantile increase in air pollutant exposure (a mixture of PM10, CO, NO2, and SO2) was associated with an average of 0.73 mmHg higher DBP (Ψ = 0.73, 95% CI = 0.21, 1.25) (Fig. 1b). In both models, PM exhibited the largest positive weight, indicating the strongest contribution among mixture components. For the PM2.5 mixture, the weights were: PM2.5 (0.49), NO2 (0.29), SO2 (0.22), and CO (–1.00). For the PM10 mixture, weights were: PM10 (0.74), SO2 (0.15), NO2 (0.11), and CO (–1.00).

Mixture analysis of air pollutants and blood pressure in the total population. *p < 0.05.
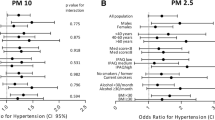
Figure 2 shows the QGC results stratified by PA engagement. Among individuals with low PA (Fig. 2a and c), greater exposure to the air pollutant mixtures was associated with higher DBP (Ψ = 0.95, 95% CI = 0.30, 1.61 for PM2.5 mixture; Ψ = 0.71, 95% CI = 0.10, 1.31 for PM10 mixture). In the PM2.5 mixture, PM2.5 was the greatest contributor to higher DBP (weight: 0.70), followed by CO (weight: 0.23) and SO2 (weight: 0.07). In the PM₁₀ mixture, PM10 was the greatest contributor to higher DBP (weight: 0.96), followed by CO (weight: 0.04). In contrast, no statistically significant associations were observed among individuals with high PA (Fig. 2b and d).

Mixture analysis of air pollutants and blood pressure stratified by physical activity engagement. *p < 0.05.
Table S3 presents results from a multi-pollutant regression model that simultaneously adjusted for PM, CO, NO2, and SO2. Consistent with the QGC results, PM10 showed an association with DBP (β = 0.92, 95% CI = 0.23, 1.61), whereas no statistically significant associations were observed for SBP or hypertension status.
Discussion
This study investigated the association of ambient air pollution with hypertension and higher BP among cancer survivors. In traditional regression models, PM2.5, PM10, and CO were associated with higher DBP. Mixture analysis results further suggested that PM (PM2.5 and PM10) contributed most substantially to the positive association between air pollution and DBP, compared to other gaseous pollutants. These associations were consistent in the low PA groups, with PM accounting for the largest contribution to higher DBP. Our findings highlight the importance of both promoting PA among cancer survivors and implementing strategies to reduce air pollution exposure in this vulnerable population.
Air pollution may play a role in vascular complications, including hypertension, through multiple biological mechanisms in cancer survivors. Inhaled air pollutants activate oxidative pathways in epithelial cells and trigger the release of cytokines and chemokines, leading to elevated levels of proatherogenic chemicals32, leukocytes, and plasma fibrinogen33. Along with the imbalance of the autonomic nervous system, this inflammation and endothelial dysfunction can contribute to increased BP and hypertension34. Although the specific pathways underlying heightened vulnerability to hypertension in cancer survivors are not yet fully elucidated, potential mechanisms may include tumor invasion or compression of blood vessels, intravascular coagulopathy, and systemic infection due to immunosuppression6. In addition, cancer treatments such as chemotherapy, radiotherapy, and surgery may cause endothelial toxicity and hemostatic disturbances6,7. Taken together, cancer survivors exposed to air pollution may be particularly vulnerable to elevated BP through a combination of these multifaceted biological pathways and cancer-related factors.
Previous studies have reported the adverse effects of PM on BP, aligning with our results. PM, a mixture of solid particles or liquid droplets suspended in the air35, has been associated with an increased risk of hypertension and increased BP (SBP and DBP for PM2.5; SBP for PM10) in cancer-free populations8,15. Similarly, in our study, both PM2.5 and PM10 were related to higher DBP in the overall participants and in the low PA group, whereas PM2.5 was additionally linked to higher SBP in the low PA group. PM2.5 can penetrate the alveolar and enter the bloodstream more easily compared to coarser particles like PM1036, which may explain its slightly broader effect on higher BP.
In contrast to PM, the effects of CO, NO2, and SO2 on BP have remained unclear in previous research16. While associations between CO and hypertension have been rarely reported, our analysis showed that cancer survivors exposed to CO were likely to have higher DBP, with CO contributing the second most to the overall positive association. One possible explanation is that chronic CO exposure may influence an increase in vascular resistance37, potentially leading to hypertension. CO induces hypoxia by binding to hemoglobin with far greater affinity than oxygen, thereby forming carboxyhemoglobin (COHb)38. This reduces oxygen delivery into tissues and activates compensatory cardiovascular mechanisms, contributing to hemodynamic instability and increased BP39,40. The lack of consistent evidence linking CO to hypertension in prior studies may be attributed to insufficient research using CO16 and publication bias8. Meanwhile, consistent with the heterogeneous evidence in previous studies16, there were no associations between NO₂ or SO₂ and increased BP.
Across our results, air pollution showed robust associations with higher DBP, while no association was observed with higher SBP, except for PM2.5 in the low PA group. This discrepancy between SBP and DBP implies that air pollution may be more closely associated with elevated peripheral resistance, given that DBP mainly reflects peripheral vascular resistance41 and SBP is primarily influenced by the stiffness and reduced elasticity of the major arteries42,43. However, the mechanisms underlying SBP and DBP elevations are interrelated, functioning in a dynamic and reciprocal system, and should not be considered entirely independent. Therefore, further investigation is warranted to better understand the biological pathways underlying these differential associations.
Our results imply that PA may attenuate the impact of air pollution on higher DBP among cancer survivors. The low PA group, defined as individuals who did not meet the WHO exercise guidelines in our study, showed an association between air pollution and higher DBP. Similarly, previous studies have shown that cancer survivors who met WHO recommendations had lower SBP and a reduced risk of hypertension22. Also, in our study, the association between air pollution and higher DBP was evident only among cancer survivors who did not engage in any physical activity or performed only moderate-intensity activity, but not among those with high-intensity activity. In contrast, previous research has reported that PA at any intensity level-even in small amounts-may help counteract the risk of elevated BP44,45. These findings support the WHO’s recommendation that cancer survivors engage in at least 150 min of moderate-intensity or at least 75 min of vigorous-intensity exercise per week, and further suggest that incorporating vigorous activity, either alone or combining it with moderate activity, may contribute to promoting better BP control. However, cancer survivors may face challenges in maintaining regular PA due to functional limitations20, highlighting the need for clinical support to enhance physical performance. Additionally, efforts to stay active may conflict with the need to limit outdoor air pollution exposure, underscoring the importance of policy-level interventions to reduce ambient air pollution. Given the prominent role of PM in our findings, PM may be a key pollutant requiring prioritized intervention to lower the risk of hypertension.
To our knowledge, this study is one of the first to examine the association between air pollution and hypertension or high BP in cancer survivors, stratified by PA level. Building on previous research that examined the association between air pollution and incident cardiovascular diseases in cancer survivors23, our findings highlight the relationship of PM and CO with higher DBP, a known precursor to cardiovascular conditions. Furthermore, we applied QGC, a flexible mixture analysis method that combines features of weighted quantile sum (WQS) regression and g-computation, allowing for the estimation of joint effects of multiple pollutants on high BP46. Lastly, this research utilized data from a nationally representative sample of South Korea, obtained through multi-stage cluster probability sampling, capturing the diversity of regional, demographic, and socioeconomic characteristics across the population.
Our study has several limitations to consider. First, due to the data constraints, cancer-related variables such as survivorship stage, cancer stage, cancer type, and treatment details were not included in the analysis. These factors‒particularly cancer severity and cancer-specific therapies (e.g., chemotherapy and radiotherapy)‒can affect vascular complications as well as psychological conditions6,7,47, both of which may lead to hypertension. Future studies are needed to examine the association between air pollution and hypertension among cancer survivors while accounting for these cancer-related covariates. Second, air pollution exposure was estimated based on participants’ residential addresses, which may introduce measurement bias and not accurately reflect actual exposure across other environments, such as workplaces or recreational areas. Future methodological advancements should aim to assess exposure more precisely by incorporating individual mobility patterns. Finally, future research with repeated measurements of BP will enhance our understanding of the longitudinal association between air pollution and hypertension.
Conclusion
In conclusion, our findings suggest that air pollution is associated with higher DBP in cancer survivors, with PM showing the greatest contribution among the components of ambient air pollution. Adequate engagement in PA may help mitigate the adverse effects of ambient air pollution on BP in this population. Policy-level interventions aimed at reducing air pollution may contribute to lowering the risk of high blood pressure among cancer survivors.
Data availability
The data used in this study were obtained from the Korea National Health and Nutrition Examination Survey (KNHANES), provided by the Korea Disease Control and Prevention Agency (KDCA), and are publicly available at https://knhanes.kdca.go.kr/knhanes/main.do.
References
Mills, K. T., Stefanescu, A. & He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 16(4), 223–237. https://doi.org/10.1038/s41581-019-0244-2 (2020).
Kontis, V. et al. Regional contributions of six preventable risk factors to achieving the 25x25 non-communicable disease mortality reduction target: a modelling study. Lancet Global Health. 3(12), e746–e757. https://doi.org/10.1016/S2214-109X(15)00179-5 (2015).
Zhou, B., Perel, P., Mensah, G. A. & Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Reviews Cardiol. 18(11), 785–802. https://doi.org/10.1038/s41569-021-00559-8 (2021).
Zhang, F. et al. Risk of stroke in cancer survivors: A meta-analysis of population-based cohort studies. Neurology 96(4), e513–e526. https://doi.org/10.1212/WNL.0000000000011264 (2021).
Koene, R. J., Prizment, A. E., Blaes, A. & Konety, S. H. Shared risk factors in cardiovascular disease and cancer. Circulation 133(11), 1104–1114. https://doi.org/10.1161/CIRCULATIONAHA.115.020406 (2016).
Zhang, F. et al. Risk of stroke in cancer survivors. Neurology 96(4), e513–e526. https://doi.org/10.1212/WNL.0000000000011264 (2021).
Choi, S. et al. Association between post-diagnosis particulate matter exposure among 5-year cancer survivors and cardiovascular disease risk in three metropolitan areas from South Korea. Int. J. Environ. Res. Public Health. 17(8), 2841 (2020).
Qin, P. et al. Long-term association of ambient air pollution and hypertension in adults and in children: A systematic review and meta-analysis. Sci. Total Environ. 796, 148620. https://doi.org/10.1016/j.scitotenv.2021.148620 (2021).
Miller, M. R. et al. Inhaled nanoparticles accumulate at sites of vascular disease. ACS Nano. 11(5), 4542–4552. https://doi.org/10.1021/acsnano.6b08551 (2017).
Miller, M. R., Shaw, C. A. & Langrish, J. P. From particles to patients: oxidative stress and the cardiovascular effects of air pollution. Future Cardiol. 8(4), 577–602. https://doi.org/10.2217/fca.12.43 (2012).
Pope, C. A. et al. Exposure to fine particulate air pollution is associated with endothelial injury and systemic inflammation. Circul. Res. 119(11), 1204–1214. https://doi.org/10.1161/CIRCRESAHA.116.309279 (2016).
Hasan Khan, M., Pathak, S., Yadav, U., Rochlani, Y. & Aronow, W. S. Hypertension in cancer survivors. Curr. Hypertens. Rep. 24(10), 435–443. https://doi.org/10.1007/s11906-022-01208-2 (2022).
Rodriguez-Iturbe, B., Pons, H. & Johnson, R. J. Role of the immune system in hypertension. Physiol. Rev. 97(3), 1127–1164. https://doi.org/10.1152/physrev.00031.2016 (2017).
Qin, P. et al. Long-term association of ambient air pollution and hypertension in adults and in children: A systematic review and meta-analysis. Sci. Total Environ. https://doi.org/10.1016/j.scitotenv.2021.148620 (2021).
Yang, B. Y. et al. Global association between ambient air pollution and blood pressure: A systematic review and meta-analysis. Environ. Pollut. 235, 576–588. https://doi.org/10.1016/j.envpol.2018.01.001 (2018).
Cai, Y. et al. Associations of short-term and long-term exposure to ambient air pollutants with hypertension: A systematic review and meta-analysis. Hypertension 68(1), 62–70. https://doi.org/10.1161/HYPERTENSIONAHA.116.07218 (2016).
Ramin, C. et al. All-cause and cardiovascular disease mortality among breast cancer survivors in CLUE II, a long-standing community-based cohort. JNCI: J. Natl. Cancer Inst. 113(2), 137–145. https://doi.org/10.1093/jnci/djaa096 (2020).
Diaz, K. M. & Shimbo, D. Physical activity and the prevention of hypertension. Curr. Hypertens. Rep. 15(6), 659–668. https://doi.org/10.1007/s11906-013-0386-8 (2013).
Oguma, Y. & Shinoda-Tagawa, T. Physical activity decreases cardiovascular disease risk in women - Review and meta-analysis. Am. J. Prev. Med. 26(5), 407–418. https://doi.org/10.1016/j.amepre.2004.02.007 (2004).
Stein, K. D., Syrjala, K. L. & Andrykowski, M. A. Physical and psychological long-term and late effects of cancer. Cancer-Am Cancer Soc. 112(11), 2577–2592. https://doi.org/10.1002/cncr.23448 (2008).
Keil, A. P. et al. A quantile-based g-computation approach to addressing the effects of exposure mixtures. Environ. Health Perspect. 128(4), 47004. https://doi.org/10.1289/EHP5838 (2020).
Kang, D-W. et al. Associations between physical activity and comorbidities in Korean cancer survivors. J. Cancer Surviv. 12(4), 441–449. https://doi.org/10.1007/s11764-018-0683-y (2018).
Choi, D. et al. Combined associations of physical activity and particulate matter with subsequent cardiovascular disease risk among 5-year cancer survivors. J. Am. Heart Association. 11(9), e022806. https://doi.org/10.1161/JAHA.121.022806 (2022).
Chung, C-E. Complex sample design effects and inference for Korea National Health and Nutrition Examination Survey data. Kjn 45(6), 600–612. https://doi.org/10.4163/Kjn.2012.45.6.600 (2012).
Kweon, S. et al. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 43(1), 69–77. https://doi.org/10.1093/ije/dyt228 (2014).
Hwang, M. J. et al. Establishment of the Korea National Health and Nutrition Examination Survey air pollution study dataset for the researchers on the health impact of ambient air pollution. Epidemiol. Health. 43, e2021015. https://doi.org/10.4178/epih.e2021015 (2021).
Kim, H. L. et al. Standardized protocol of blood pressure measurement and quality control program for the Korea National Health and Nutrition Examination Survey. Clin. Hypertens. https://doi.org/10.1186/s40885-023-00252-7 (2023).
Muntner, P. et al. Measurement of blood pressure in humans ascientific statement from the American Heart Association. Hypertension 73(5), E35–E66. https://doi.org/10.1161/Hyp.0000000000000087 (2019).
Bull, F. C. et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54(24), 1451–1462. https://doi.org/10.1136/bjsports-2020-102955 (2020).
Lee, D. E. et al. Differential contributions of cardiovascular health-related lifestyle factors to epigenetic ageing: implications for healthy longevity. BMC Med. https://doi.org/10.1186/s12916-025-04394-3 (2025).
Fan, H., Zhao, C., Yang, Y. & Yang, X. Spatio-Temporal variations of the PM2.5/PM10 ratios and its application to air pollution type classification in China. Original research. Front. Environ. Sci. https://doi.org/10.3389/fenvs.2021.692440 (2021).
Araujo, J. A. & Nel, A. E. Particulate matter and atherosclerosis: role of particle size, composition and oxidative stress. Part. Fibre Toxicol. 6, 24. https://doi.org/10.1186/1743-8977-6-24 (2009).
Su, T. C. et al. Urban air pollution increases plasma fibrinogen and plasminogen activator inhibitor-1 levels in susceptible patients. Eur. J. Cardiov Prev. R. 13(5), 849–852. https://doi.org/10.1097/01.hjr.0000219116.25415.c4 (2006).
Sanidas, E. et al. Air pollution and arterial hypertension. A new risk factor is in the air. J. Am. Soc. Hypertens. 11(11), 709–715. https://doi.org/10.1016/j.jash.2017.09.008 (2017).
Brunekreef, B. & Holgate, S. T. Air pollution and health. Lancet 360(9341), 1233–1242. https://doi.org/10.1016/S0140-6736(02)11274-8 (2002).
Harrison, R. M. & Yin, J. Particulate matter in the atmosphere: which particle properties are important for its effects on health? Sci. Total Environ. 249(1), 85–101. https://doi.org/10.1016/S0048-9697(99)00513-6 (2000).
Penney, D. G. & Howley, J. W. Is there a connection between carbon monoxide exposure and hypertension? Environ. Health Perspect. 95, 191–198. https://doi.org/10.1289/ehp.9195191 (1991).
Carrola, A., Romão, C. C. & Vieira, H. L. A. Carboxyhemoglobin (COHb): unavoidable bystander or protective player? Antioxidants 12(6), 1198 (2023).
Kakavas, S. et al. Carboxyhemoglobin and methemoglobin levels as prognostic markers in acute pulmonary embolism. Am. J. Emerg. Med. 33(4), 563–568. https://doi.org/10.1016/j.ajem.2015.01.046 (2015).
Conway, K., Rayes, O., Brown, T. & Webb, M. Atherosclerotic and hypertensive cardiovascular disease are associated with death at sublethal carboxyhemoglobin levels: A postmortem study. J. Forensic Sci. 65(3), 855–859. https://doi.org/10.1111/1556-4029.14261 (2020).
Luo, J. et al. Differing associations of PM2.5 exposure with systolic and diastolic blood pressures across exposure durations in a predominantly non-Hispanic black cohort. Sci. Rep. 14(1), 20256. https://doi.org/10.1038/s41598-024-64851-6 (2024).
Smulyan, H. & Safar, M. E. Blood pressure measurement: retrospective and prospective views. Am. J. Hypertens. 24(6), 628–634. https://doi.org/10.1038/ajh.2011.22 (2011).
Tin, L. L., Beevers, D. G. & Lip, G. Y. H. Systolic diastolic blood pressure and the burden of hypertension. J. Hum. Hypertens. 16(3), 147–150. https://doi.org/10.1038/sj.jhh.1001373 (2002).
Ekelund, U., Sanchez-Lastra, M. A., Dalene, K. E. & Tarp, J. Dose–response associations, physical activity intensity and mortality risk: A narrative review. J. Sport Health Sci. 13(1), 24–29. https://doi.org/10.1016/j.jshs.2023.09.006 (2024).
Bull, F. C. et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54(24), 1451–1462. https://doi.org/10.1136/bjsports-2020-102955 (2020).
Keil, A. P. et al. A Quantile-Based g-Computation approach to addressing the effects of exposure mixtures. Environ. Health Perspect. ;128(4) (2020).
Lee, D-E., Kim, Y., Kim, Y-M. & Cho, S-I. Changes in work status after cancer diagnosis and their associations with depressive symptoms among cancer survivors: findings from the Korean longitudinal study of ageing. BMC Psychol. 12(1), 551. https://doi.org/10.1186/s40359-024-01970-9 (2024).
Funding
This study was supported by the grants from the National Research Foundation of Korea (NRF), funded by the Ministry of Science and Technology (Grant RS-2024-00405650); the National Cancer Center, funded by the Korean government (Grant NCC-2510431).
Author information
Authors and Affiliations
Contributions
Concept and design: D Lee; J Hwang; HJ Kim; K Kim; Acquisition, analysis, or interpretation of data: D Lee; J Hwang; HJ Kim; K Kim; Drafting of the manuscript: D Lee; J Hwang; Critical revision of the manuscript for important intellectual content: D Lee; J Hwang; HJ Kim; K Kim; Statistical analysis: J Hwang; Obtained funding: HJ Kim; K Kim; Administrative, technical, or material support: HJ Kim; K Kim; Supervision: HJ Kim; K Kim.
Corresponding authors
Ethics declarations
Ethics approval
All individuals provided informed consent before enrollment for the Korea National Health and Nutrition Examination Survey (KNHANES). The protocol of this study was reviewed and approved by the Institute Review Board at Sungkyunkwan University (No. SKKU 2025-04-024).
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lee, De., Hwang, J., Kim, K. et al. Modifying role of physical activity in associations between air pollutants and blood pressure among cancer survivors. Sci Rep 16, 8794 (2026). https://doi.org/10.1038/s41598-026-39815-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-39815-7
