
Abstract
Disposable scalpel blades are routinely used in oral surgical procedures; however, their cutting-edge integrity may be compromised during clinical use, particularly during full-thickness flap elevation. Evidence regarding the relationship between incision length and blade deformation in intraoral surgery remains limited. This study aimed to evaluate the presence and extent of deformation of commonly used dental scalpel blades as a function of the linear length of full-thickness oral incisions using scanning electron microscopy (SEM). An in vivo study was conducted on 96 patients undergoing oral surgical procedures requiring full-thickness flaps. Scalpel blades no. 11 and no. 15 from two manufacturers were evaluated and grouped according to incision length (0–2 cm, 2–4 cm, 4–6 cm, and 6–8 cm). Blade deformation was assessed under SEM by recording the presence of deformation, deformation length, and deformation width. Statistical analysis was performed using ANOVA with Tukey post-hoc tests (P ≤ 0.05). Overall, 94 of 96 blades (97.9%) exhibited deformation following clinical use. Deformation was observed in 91.7% of blades used for incisions up to 2 cm and in 100% of blades used for incisions exceeding 2 cm. Both deformation length and deformation width increased significantly with increasing incision length (P < 0.05). Blade morphology influenced deformation characteristics, with blade no. 15 showing greater deformation length and blade no. 11 exhibiting greater deformation width. No statistically significant differences were observed between manufacturers for blades of identical morphology (P > 0.05). Based on the present findings, disposable scalpel blades no. 11 and no. 15 undergo measurable deformation during clinical use in full-thickness oral surgical procedures. The presence, length, and width of blade deformation increase with the linear length of the incision, regardless of the manufacturer.
Similar content being viewed by others


Introduction
In dentistry, disposable surgical scalpels are widely used in a variety of clinical situations involving the incision of oral soft tissues, ranging from small millimetric incisions to the elevation of large surgical flaps, as performed during complex and extensive procedures such as multiple dental implant insertions1. Disposable surgical scalpels are characterised by several parameters, including the materials used, as well as blade shape, length, and thickness. Currently, the market offers disposable scalpels with plastic handles equipped with blades of different shapes, as well as single-use disposable blades that can be mounted on sterilizable and reusable metal handles2. Manufacturers adhere to current European regulations, including British Standard BS 2982:1992 and ISO standards ISO 7740:1985, ISO 7153-1:1991, and EN 10088-3:20053.
Scalpel blades are commonly manufactured from high-quality carbon steel or stainless steel, which are biocompatible and highly resistant to corrosion4. In addition, advanced blades with zirconium nitride coatings on the cutting edge are available to meet stringent surgical requirements5. These surface-treated blades are designed to enhance durability, allowing the cutting edge to remain sharp over repeated incisions due to their increased hardness and resistance to wear6,7,8. Scalpel blades are identified by numbers corresponding to different shapes, including 10, 11, 12, 15, 20, 21, 22, 23, and 24. In dentistry, blades no. 11 and no. 15 are the most commonly used because their morphology and dimensions are particularly suited to the anatomical constraints of the oral cavity. Nevertheless, individual operator preference and surgical technique may influence the selection of alternative blade types9,10.
In dental surgery, scalpels are used to raise either partial-thickness or full-thickness flaps, a distinction of considerable clinical importance. In partial-thickness flaps, the scalpel is confined to the soft tissues and does not contact the cortical bone, thereby preserving the periosteum. In contrast, full-thickness flaps require the blade to incise the soft tissues while maintaining firm contact with the cortical bone, cutting through the periosteum to fully expose the underlying bone, which remains included in the flap thickness11,12.
In full-thickness flap procedures, the periosteum must be incised precisely and without laceration. Consequently, the scalpel blade is subjected to substantial mechanical stress as it is forced against the hardness of the maxillary or mandibular cortex. Under these conditions, the delicate sharpening of the blade may undergo rapid alteration, leading to a progressive loss of sharpness4,13. This phenomenon is clinically relevant, as an ineffective blade may lacerate rather than cleanly incise soft tissues, potentially impairing wound healing and increasing the risk of postoperative pain and oedema due to flap trauma. Moreover, incomplete incisions can result in tearing of the soft tissues during flap elevation and the formation of irregular flap margins13.
Improved clinical outcomes may be achieved by enhancing the dental community’s understanding of the factors contributing to scalpel blade deformation and by selecting cutting-edge designs appropriate for specific surgical demands. Ongoing research and strict adherence to safety standards are essential to optimise scalpel performance and minimise surgical trauma associated with loss of cutting efficiency. Although several scientific studies have investigated scalpel characteristics, none have specifically addressed blade sharpness loss as a function of the linear length of the incision during intraoral surgical flap procedures. The present study aims to fill this gap in the literature.
Accordingly, this study evaluates, using scanning electron microscopy (SEM), how the blades of different types of scalpels commonly used in dentistry undergo morphological changes as a function of the linear length of tissue incised during full-thickness flap procedures. SEM provides high-resolution imaging that enables detailed observation of blade deformation and assessment of structural integrity. Conducted in vivo, this study simulates routine clinical conditions in which the clinician may use the same scalpel for either small flaps or larger, more complex surgical interventions. This study aimed to evaluate the presence and extent of deformation of commonly used dental scalpel blades as a function of the linear length of full-thickness oral incisions using scanning electron microscopy (SEM).
Materials and methods
The clinical study adhered to the principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board of the Paolo Giaccone University of Palermo (Protocol Code # 4-19-04-23). All participants received detailed information about the study and provided written informed consent to participate and to allow publication of anonymized data. Ethical conduct was ensured throughout the study, with full respect for participant rights and well-being. Although the authors are not affiliated with the Paolo Giaccone University of Palermo, the clinical procedures were performed at a dental facility operating under the ethical oversight of its Institutional Review Board; therefore, approval was obtained from this committee in accordance with its jurisdiction over the study setting.
This in vivo study was conducted on patients requiring surgical dental procedures involving full-thickness mucoperiosteal incisions in the mandible and/or maxilla. The surgical procedures included complex tooth extractions, periodontal surgeries, and dental implant placement. A total of 96 patients (49 males and 47 females), aged between 18 and 68 years, all of Italian nationality, were enrolled. Patients outside this age range and those undergoing more complex procedures (e.g., maxillofacial surgery), in which flap thickness and incision characteristics could vary substantially, were excluded. This selection was intended to minimize procedural variability related to incision type and surgical complexity.
Scalpel blades and study groups
Disposable scalpel blades no. 11 and no. 15 from two different manufacturers were evaluated. The blades were divided into four experimental groups as follows:
-
Group A: Brand Benefis, blade no. 11.
-
Group B: Brand Benefis, blade no. 15.
-
Group C: Brand Ysis, blade no. 11.
-
Group D: Brand Ysis, blade no. 15.
Blade no. 11 is characterised by a straight, pointed cutting edge, whereas blade no. 15 presents a rounded tip followed by a straight cutting section. The morphological characteristics of the blades are illustrated in Fig. 1.

On the left, the blade shape n. 15 and on the right blade shape n. 11.
All blades were manufactured from stainless steel; however, the precise alloy composition was not disclosed by the manufacturers. Each group consisted of 24 scalpel blades, with one blade used per patient. Accordingly, 24 patients were treated using blades from each group.
Subgroup classification according to incision length
Based on the linear length of the full-thickness incision, each group was further divided into four subgroups:
-
Subgroup 1: incision length up to 2 cm.
-
Subgroup 2: incision length between 2 and 4 cm.
-
Subgroup 3: incision length between 4 and 6 cm.
-
Subgroup 4: incision length between 6 and 8 cm.
Combining the four blade groups with the four incision-length subgroups resulted in 16 experimental combinations (A1–A4, B1–B4, C1–C4, D1–D4). Each combination included six clinical cases, yielding a total of 96 observations. The distribution of groups and subgroups is summarized in Table 1.
Surgical standardization and blade handling
All incisions were performed by a single experienced dentist to eliminate inter-operator variability. Full-thickness incisions were carried out with continuous and stable contact between the blade and the cortical bone, as required by the surgical technique. To further standardize the procedure, the scalpel was consistently held at a 30° angle relative to the bone surface along the entire incision length. Variations in blade angulation were avoided, as uncontrolled angles could influence mechanical stress and blade deformation.
After clinical use, the blade was carefully detached from the handle, placed in a numbered plastic container, and cleaned in an ultrasonic bath for 5 min to remove organic residues. Special care was taken to prevent accidental contact with other surfaces that could artificially alter the cutting edge. Each blade was then individually wrapped and sterilized in an autoclave at 132 °C for 12 min for safety purposes prior to analysis.
SEM analysis and deformation assessment
All blades were examined using a scanning SEM (JEOL JSM 6390 LV), mounted on dedicated holders. Prior to observation, blades underwent plasma cleaning for 10 min in a controlled nitrogen and oxygen atmosphere (South Bay Technologies P2000) to optimize surface visualization.
The samples were observed under SEM (JEOL JSM 6390 LV) by positioning them on suitable supports for electron microscopy (Fig. 2). The morphological analysis under scanning electron microscopy was performed using a secondary electron detector to obtain high-resolution images of the blade surface and to document overall cutting-edge deformation following clinical use, without attempting to distinguish alterations caused exclusively by soft tissue contact from those resulting from contact with the cortical bone.

Example of SEM visualization of blade deformation (top right); detail of the deformed area (top left); detail of the loss of sharpness.
All incisions were performed as full-thickness flaps, which inherently require continuous and deliberate contact between the scalpel blade and the cortical bone. Therefore, no attempt was made to distinguish blade deformation caused exclusively by soft tissue contact from that caused by bone contact. The observed deformations were interpreted as resulting from the combined mechanical action of soft tissue incision and forced contact with the cortical bone. To support this interpretation, unused blades of each type were examined under SEM as morphological controls, allowing post-use alterations to be attributed to intraoperative mechanical stress rather than manufacturing defects.
To correctly interpret the SEM images, three new blades for each type of scalpel tested were also examined to identify the initial morphology of the blade and the possible presence of manufacturing defects. This test revealed no defects in the new samples examined.
The SEM observation also allowed us to precisely measure some dimensional values of the scalpels tested to evaluate the homogeneity of the construction dimensional parameters and any differences between groups A, B, C and D. New blades were also observed for each type of scalpel belonging to all four groups to verify the initial morphological and dimensional conditions precisely. This allowed us to better evaluate and understand the SEM images of the deformed scalpels after clinical use (Fig. 3).

Example of a scalpel tip blade number. 15 new unused shows sharpness without alterations.
Definition of evaluated outcomes and SEM assumptions
The study evaluated three distinct deformation-related outcomes:
-
1.
Presence or absence of blade deformation.
-
2.
Length of the deformed section, measured longitudinally along the cutting edge.
-
3.
Width of the deformation, defined as the maximum protrusion or flattening relative to the original blade profile.
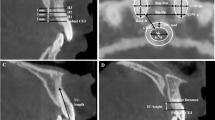
Measurements were performed using the integrated SEM image analysis software. Deformation length and deformation width were measured independently on high-resolution SEM images (Fig. 4).

SEM images of a deformation of the cutting edge of the scalpel. On the left, the deformation amplitude at the broadest point was measured. The measurement relating to the length of the deformed section is shown on the right.
Because all incisions were performed as full-thickness flaps with deliberate and sustained contact with the cortical bone, the observed deformations were interpreted as resulting from the combined mechanical action of soft tissue incision and forced contact with bone. The use of unused blades as morphological controls allowed deformation features observed after clinical use to be attributed to intraoperative mechanical stress, rather than pre-existing manufacturing characteristics.
Statistical analysis
SEM-derived quantitative data were analysed using IBM SPSS Statistics (version 30). Descriptive statistics were calculated for all outcome variables. One-way analysis of variance (ANOVA) was used to assess differences in deformation length and deformation width across incision-length subgroups, blade types (no. 11 vs. no. 15), and manufacturers. When ANOVA indicated statistically significant differences, post hoc multiple comparisons were performed using the Tukey honestly significant difference (HSD) test to identify specific group differences.
The level of statistical significance was set at P ≤ 0.05. The null hypotheses tested were:
-
(i)
incision length does not influence blade deformation;
-
(ii)
no differences exist between blade no. 11 and blade no. 15;
-
(iii)
no differences exist between blades of identical morphology from different manufacturers.
Results
Overall, 94 out of 96 scalpel blades (97.91%) showed evidence of deformation following clinical use. Deformations were already observed after short incision lengths, with 22 of 24 blades (91.66%) in subgroup 1 (0–2 cm) showing detectable alterations. In contrast, all blades (100%) in subgroups 2, 3, and 4 (incisions > 2 cm) exhibited deformation (Table 2).
When the 16 experimental combinations were analyzed, the absence of deformation was observed only in two cases, both involving blade no. 15 used for incisions up to 2 cm (combinations B1 and D1). All other combinations demonstrated deformation in every examined blade (Table 3). No statistically significant differences in deformation prevalence were observed between blades from different manufacturers when comparing identical blade types (P > 0.05).
Regarding deformation length, a progressive increase was observed with increasing incision length across all blade groups (A–D), with statistically significant differences between subgroups (P < 0.05). The highest deformation lengths were consistently recorded in subgroup 4 (6–8 cm incisions), particularly for blade no. 15. Mean deformation length values for each group and subgroup are reported in Table 4.
Inferential statistical analysis (Table 5) confirmed a significant association between incision length and blade deformation, with both deformation length and deformation width increasing progressively across incision-length subgroups (P < 0.05). Post-hoc comparisons demonstrated that longer incisions, particularly those exceeding 4 cm, were associated with significantly greater deformation compared with shorter incisions. Blade morphology influenced deformation characteristics, with blade no. 15 exhibiting greater deformation length, while blade no. 11 showed greater deformation width (P < 0.05). In contrast, no statistically significant differences were observed between manufacturers for blades of identical morphology (P > 0.05), indicating comparable performance across brands.
Post-hoc analysis (Table 6) using the Tukey HSD test demonstrated that significant differences in both deformation length and deformation width emerged primarily between shorter and longer incision-length subgroups. Specifically, incisions exceeding 4 cm (Subgroups 3 and 4) showed significantly greater deformation compared with Subgroup 1, while Subgroup 4 also differed significantly from Subgroup 2 (P < 0.05). These findings indicate that blade deformation increases in a stepwise manner with increasing incision length, with statistically significant changes becoming evident beyond shorter incision ranges.
Discussion
Our study aims to evaluate how the blade of scalpels, commonly used in dentistry, deforms as a function of the linear length of the incisions. The results of our research show that the sharp, cutting blade of the scalpel can deform precisely when it is performing its function, which is to counteract the elasticity of the mucosa by cutting it, allowing the tissues to separate.
The consistency of the oral tissues is not high, but when, as in our study, the scalpel blade is pushed firmly against the bone cortex to cleanly cut the periosteum without tearing it, it undergoes alterations in shape which gradually cause it to lose its sharpness. This is what the manufacturer created. Our study highlights that the length of the cut soft tissues influences the extent of the deformations, both when these are measured as a linear measurement on the blade and when measured as a width on the profile of the blade.
Therefore, the null hypothesis, which predicted that there were no differences in the deformation induced on the blade during use as a function of how many millimeters of tissue were cut, must be rejected in the fact that the highest deformation values are present in the samples of subgroup 4 which involve the blade pushed against the cortex for 8 cm. In any case, the values relating both to the deformation measured along the blade and those relating to the protrusion of the deformation increase going from subgroup 1 to subgroup 4; this increasing deformation was noted for scalpels from both manufacturers chosen for the study and for scalpels no. 11 and those n. 15, highlighting that there are no differences between the two different scalpel manufacturers tested in the study.
The null hypothesis that there were differences in the deformations found between the two brands of blades must be rejected (P < 0.05). Going into detail regarding the comparison between the manufacturers, in the comparison between the two groups A with C and B with D, it can be stated, based on our data, that there are no differences between the blades of the two different brands, considering both the length of the deformations and the protrusion concerning the profile.
The null hypothesis, according to which there were no differences in the deformation between the two types of blades (no. 11 and no. 15), must also be rejected (P < 0.05), in fact, by comparing the deformations of the two different morphologies of blades, both considering the length and the width of the deformations, statistically significant differences were highlighted. Blade no. 11, under the same clinical conditions understood as linear mm of soft tissue cutting, showed deformations measured as widths that were larger and, therefore, more deformable than blade no. 15. These results are probably justified by the fact that at the end of blade no. 11 concentrates all the forces applied by the operator when he pushes the cutting edge against the bone cortex. To support this concept, we should consider the lengths of the deformations observed under SEM on the blades n. 11, these are reduced compared to blades n. 15.
Blade no. 15 has a rounded shape, allowing cutting to distribute the force applied over a length slightly more significantly than the sharpening, which is not affected at the tip but at a distance from it; in conclusion, the blades no 15 are deformed for a longer distance, but the deformation’s width is smaller than that of blade no. 1114 (Figs. 5 and 6).

A left a blade n. 15, which is altered by use at a distance from the tip because it works on the most protruding part of the convexity. On the right is an example of blade no. 11, which presents a deformation that starts right from the tip, is subjected to a concentration of forces and is consequently deformed.

Example of a scalpel number. 11, whose large deformation is shown at the end of the blade.
However, our research has highlighted that the scalpel blade is quite resistant, but in contact with the bone cortex, as in the case of the type of incision tested in our study, it can easily give way regardless of the shape of the scalpel and the manufacturer15. Beyond 2 centimeters of cut tissue, the deformations are evident on both blades, n. 11 and n. 15. From a clinical point of view, episodes of sensation of loss of cutting ability after use for more than 6 linear cm have been reported by the dentist who carried out the incisions. The blade, losing sharpness and deforming, probably transmits the sensation of losing sharpness and becoming less effective to the operator. Therefore, the scalpel must be pushed with more force16,17,18,19. Disposable surgical blades #11 and #15 undergo deformation during incisions for full-thickness flaps in oral surgery procedures. The most affected areas are the tip of the #11 blade and the tip and convex curvature of the #15 blade. Furthermore, the extent of blade damage is directly proportional to the length of the incision, indicating a progressive deterioration with increased use.
Our study has the limitation of having tested the scalpels only for full-thickness flaps; probably, if we had tested the blades when performing partial-thickness flaps, avoiding contact with the bone cortex, the results would have been different, this clinical condition, although less probable in everyday dental clinical reality, is worthy of scientific study and could be the subject of further developments of the present study. The same scalpels used on tissues of different consistencies and in other fields of medicine would probably have given different results20,21.
It remains to be explored what the clinical and microscopic implications are on tissues cut by blades that have undergone deformations such as those observed under SEM by our research; in this regard, a further study is underway, which will evaluate these parameters. Even if our research aimed to eliminate the operator variable using a single experimenter, testing and comparing the results from operators with different clinical experiences would be helpful. This article is part of a line of research that intends to continue investigations into the other variables mentioned above22,23.
Conclusions
Based on the present findings, disposable scalpel blades no. 11 and no. 15 undergo measurable deformation during clinical use in full-thickness oral surgical procedures. The presence, length, and width of blade deformation increase with the linear length of the incision, regardless of the manufacturer.
Data availability
The author Enzo Cumbo will make the data available upon reasonable request.
References
Esteban, E. I. Surgical instruments (I). An introduction to surgical instruments. Revista de enfermeria. (Barcelona Spain). 28 (4), 64–66 (2005).
Shetty, P. P., Hatton, R. W., Barnett, A. C., Homich, A. J. & Moore, J. Z. Modeling the cutting edge geometry of scalpel blades. Proc. Inst. Mech. Eng. Part B J. Eng. Manufacture. 231(1):65–72 (2017).
Croke, L. Key considerations for processing surgical instruments. AORN J. 113 (3), P9–11 (2021).
Bhasin, Y., Liu, A. & Bowyer, M. Simulating surgical incisions without polygon subdivision. Stud. Health Technol. Inform. 111, 43–49 (2005).
Pinca, K. C., Ontoria, A. B. & Vasquez, M. R. Jr Properties of Nitride-Coated surgical scalpel blades. Plasma Med. ;13(3). (2023).
Morco, S. R., Larsen, J. M., Jensen, B. D. & Bowden, A. E. Carbon-Infiltrated Carbon Nanotube Coating Applications: Scalpel Blades and External Fixators.
McCarthy, C. T., Hussey, M. & Gilchrist, M. D. An investigation into scalpel blade sharpness using cutting experiments and finite element analysis. Key Eng. Mater. 293, 769–776 (2005).
Barbosa, R. R. Surgical scalpel handles and blades. Br. J. Surg. 109 (10), 916–920 (2022).
Nelson, C. A. Material selection indices for design of surgical instruments with long tubular shafts. J. Med. Eng. Technol. 37 (2), 102–108 (2013).
Díaz-Caballero, A., Tarón-Dunoyer, A. & Hernandez-Ligardo, R. Data of fracture effort in the deformation of the cutting surface of scalpel blades. Data brief. 22, 98–103 (2019).
Díaz Caballero, A., Tarón Dunoyer, A., Hernández Ligardo, R., Camacho Vergara, Á. & Fortich Mesa, N. Deformation of scalpel blades after incision of gingival tissue in pig mandibles. An ex vivo study. Revista odontológica Mexicana. 21 (3), 173–179 (2017).
Szindler, M., Szindler, M., Basiaga, M., Łoński, W. & Kaim, P. Application of ALD thin films on the surface of the surgical scalpel blade. Coatings 11 (9), 1096 (2021).
Chandra, S., Podder, I., Chatterjee, M. & Field, L. Anatomy and applications of the# 15 scalpel blade and its variations. J. Cutan. Aesthetic Surg. 11 (2), 79–82 (2018).
de Melo Costa, D. et al. Evaluation of stainless steel surgical instruments subjected to multiple use/processing. Infect. Disease Health. 23 (1), 3–9 (2018).
Mejia, E., Mejia, J., Delgado, J., Avilés, O. & Amaya, D. Transducer device for measuring force and speed in a task of scalpel cutting. Rev. EIA Esc Ing. Antioq. 14, 147–160 (2010).
Díaz-Caballero, A., Tarón-Dunoyer, A. & Cerpa, B. M. Alteration of cutting edge of scalpel blades after incising animal gingiva. J. Int. Dent. Med. Res. 16 (3), 931–935 (2023).
Pietkiewicz, P. et al. One blade, two cuts? A multidisciplinary survey investigating practice variability of scalpel blade change for simultaneous excision of multiple skin lesions in the same patient. Int. J. Dermatol. 64 (2), 377–384. https://doi.org/10.1111/ijd.17416 (2025).
Prescher, H., Ling, M. X., Bigdelle, V., Spiro, C. L. & Lee, R. C. Scalpel edge roughness affects post-transection peripheral nerve regeneration. Surg. Open. Sci. 4, 1–6 (2020).
Chanthasopeephan, T., Desai, J. P. & Lau, A. C. Measuring forces in liver cutting: new equipment and experimental results. Ann. Biomed. Eng. 31, 1372–1382 (2003).
Chanthasopeephan, T., Desai, J. P. & Lau, A. C. Study of soft tissue cutting forces and cutting speeds. InMedicine Meets Virtual Reality 12 IOS press. (2004) (pp. 56–62).
Giovannini, M. & Ehmann, K. Vibrational cutting of soft tissue with micro-serrated surgical scalpels. Procedia CIRP. 45, 199–202 (2016).
Patel, A., Pope, J. & Neilson, M. Design considerations for medical device manufacturers. Biomedical Instrum. Technol. 46 (sp12), 73–75 (2012).
Mohan, A., Rangwala, M. & Boringwala, A. Q. Keratome, a better alternative scalpel to 15 blade for finer Incision-Randomized control trial. Indian J. Plast. Surg. 55 (3), 277–281. https://doi.org/10.1055/s-0042-1756126 (2022).
Acknowledgements
The authors express their thanks and gratitute to AlMaarefa High Impact Research Support Program under Researchers Supporting Project number: MHIRSP-2025001, AlMaarefa University, Riyadh, Saudi Arabia.
Funding
This research received no funding.
Author information
Authors and Affiliations
Contributions
E.C., P.M., G.A.S., and M.I.K. planned and designed the study. E.C., P.M., G.G., and G.A.S. performed the experiment. E.C., PM and G.G drafted the manuscript. Additionally, G.A.S, M.F., and M.I.K. conducted the editing and final proofreading of the entire document and reviewed the article and contributed to the interpretation. However, all authors critically revised drafts and approved the final work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Ethical approval
The current research adhered to the principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board of the Paolo Giaccone University of Palermo (Protocol Code: #4-19-04-23). All patients participating in the study were provided with a declaration of consent, which they read and signed to express their willingness to participate in the research and to consent to the publication of data.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cumbo, E., Messina, P., Gallina, G. et al. SEM morphological analysis of the deformation on disposable scalpels used in dentistry. Sci Rep 16, 8787 (2026). https://doi.org/10.1038/s41598-026-40261-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-40261-8
