
Abstract
Older adults comprise the fastest growing demographic in correctional facilities in the United States. Studies have shown older adults in prison report difficulty accessing healthcare and navigating the prison environment. Little is known about how older adults navigate aging and access healthcare in the jail setting. We sought to explore experiences of older adults incarcerated in a county jail. We conducted semi-structured qualitative interviews with 20 older adults (> 50 years old) who were incarcerated at a local county jail and were referred to the emergency department for acute care needs. Interviews focused on experiences of aging while incarcerated and access to healthcare. We used an inductive approach to code data and identify overarching themes. Participant demographics were representative of the broader jail population demographics. Two major themes emerged. First, participants reported difficulty navigating the jail environment related to aging and unaddressed disabilities. Examples included climbing to use the top bunk of a bunk bed, difficulty grasping objects due to a Parkinsonian tremor, and significant visual impairments. Participants relied on other inmates for assistance with limited systemic accommodations. Second, participants faced numerous challenges when attempting to access healthcare, including lack of clarity around procedures for accessing care and mutual distrust sometimes marking their relationship with medical staff. Participants described difficulty using a digital kiosk system to submit medical requests, and successful healthcare experiences involved an element of serendipity such as advocacy from a sympathetic officer. Despite a constitutional right to healthcare and high rates of medical comorbidities, older prisoners experienced a challenging physical environment in jail and difficulty accessing healthcare. Further work is needed to identify potential age-friendly modifications to the jail environment and improved healthcare delivery.
Similar content being viewed by others

Introduction
The population of geriatric persons experiencing incarceration (PEI) worldwide is increasing. In western Europe, almost 20% of PEI are 50 and older1. In the United States, there has been a 5-time increase in the number of geriatric PEI over the past thirty years2,3.
Aging among geriatric PEI is a challenging phenomenon due to medical and environmental issues. Due to accelerated aging, the phenomenon of advanced progression of mortality and morbidity due in part to incarceration itself, the age threshold for geriatric PEI is commonly set at ≥50 years old4,5,6,7. Medically, geriatric PEI have been found to have higher rates of dementia and mild cognitive impairment at younger ages compared to their non-incarcerated counterparts8,9,10. Additionally, geriatric PEI face additional age-related challenges specific to the carceral environment11. In addition to functional impairment of activities of daily living, a survey study showed geriatric PEI also have difficulty performing prison activities of daily living (PADLs) such as hearing correctional officers’ commands and remaining standing for count12. Geriatric PEI may also have more difficulty performing prison jobs due to functional impairment and thus face financial difficulty paying for co-pays for prison infirmary visits13,14. Geriatric PEI with undiagnosed cognitive impairment have difficulty communicating their needs and concerns with the correctional triage nurse, who may lack geriatric training11,15,16.
However, little has been published about geriatric PEI in jails, particularly regarding the interplay of aging, incarceration, and healthcare. The existing literature is almost exclusively focused on PEI in prisons17. Jails typically have shorter periods of incarceration as PEI are awaiting trial and sentencing. As a result, jails tend to have higher turnover and may have fewer resources available, such as medical care and counseling. The jail population has been shown to have high utilization of the emergency department (ED)18,19. We sought to elucidate experiences of aging and healthcare while incarcerated in a jail through geriatric PEI receiving care in an ED.
Methods
Study design and setting
We conducted semi-structured interviews with geriatric PEI being evaluated in the public hospital emergency department (ED) from November 2024 to April 2025. This study was approved by the Baylor College of Medicine Institutional Review Board (H-56301). The study is reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (see Supplement A)20. All methods were performed in accordance with relevant guidelines and regulations.
We used a phenomenological approach based on participant experiences of aging and receiving healthcare while incarcerated. Participants were incarcerated patients receiving medical care in a county hospital ED with about 80,000 annual visits. The ED dedicates one care area to PEI aside from those being evaluated for trauma.
The county hospital serves as the primary referral center for PEI at the local county jail system, the fourth largest in the United States. Approximately 15% of the county jail inmates are geriatric, defined as 50 years and older21. About 50% identify as Black, Non-Hispanic; 25% identify as White, Non-Hispanic; 22% identify as White, Hispanic; and 0.7% identify as Black, Hispanic21. PEI can place an appointment request for medical attention via digital kiosks located throughout the jail. A medical team triages appointment requests, so more urgent requests are prioritized. Each section of the jail also has a correctional officer who can send PEI for immediate medical attention. The infirmary is staffed by physicians, nurse practitioners, and physician assistants who can refer PEI to an outside hospital ED for further evaluation and treatment, such as cross-sectional imaging or urgent evaluation by specialists. The primary referral center is the county hospital ED used as our study site.
Data collection
Based on a literature review, priorities, and prior experiences (clinical practice, research, and advocacy) of the research team, we developed an interview guide regarding health concerns, the jail environment, and experiences accessing and receiving healthcare before and during incarceration. The interview guide was pilot tested and refined with 6 PEI. Some were under the age threshold of 50. Pilot interviews were conducted in English and Spanish to ensure questions made sense to participants; we made serial minor modifications to the ordering and phrasing of questions to facilitate participant comprehension.
Two research assistants, medical students with no role in ED patients’ clinical care, monitored the ED census during business hours for eligible participants. Inclusion criteria were age ≥50 years old, currently incarcerated in the local county jail, English or Spanish speaking, and able to consent based on Evaluate to Sign Consent measure22. Exclusion criteria included patients with critical illness, altered mental status, and non-English nor Spanish speaking. Critical illness was defined as receiving care in the critical care area, being triaged as a level 1 trauma code, or a level 2 trauma code with a distracting injury.
Two research assistants presented the study while potential participants were in a private room of the ED. These research assistants informed participants that participating in the study was completely voluntary and would not impact their clinical care or parole. Participants were also informed that they could stop an interview at any time. Informed consent was collected after research assistants performed the Evaluate to Sign Consent measure22. Both research assistants received training in qualitative interviewing and performed semi-structured interviews in the ED based on the interview guide. To contextualize responses, participants were also screened for cognitive impairment using the Six-Item Screener, which is validated for the ED, frailty using the Clinical Frailty Scale23,24,25,26. Chart review was performed to calculate a Charlson Comorbidity index and assess jail infirmary, ED, and hospital utilization. Although we did not use field notes, interviewers took notes on participant responses after every interview and made memos from group discussions. Participants received $20 compensation as a commissary payment or a gift card to a non-incarcerated contact. We spoke to correctional staff to determine an amount of compensation that would not be coercive. Interviews were recorded and transcribed for analysis.
Analysis
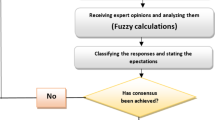
Initially, deidentified transcripts were coded into pre-specified domains of interest: challenges managing health needs, barriers and facilitators to accessing healthcare, process of accessing healthcare, and continuity of care (Supplement B). Coding discrepancies were resolved through consensus discussions. We identified themes via an inductive approach which uncovers repeated patterns and meanings (Fig. 1). Thematic saturation was reached after 9 interviews, indicating adequate sample size. We followed established principles in reporting thematic saturation, or the point at which no new themes appear in subsequent interviews, with a base number of 6 and a run number of 127,28. The research team was composed of two academic emergency physicians, two internal medicine physicians with experience working in correctional healthcare, three medical students, and one anthropologist/non-clinician. There were four male and four female team members. Of the research team, three members were Spanish-speaking, two of whom were native speakers. The study was designed around the limited window of opportunity for interacting with patients experiencing incarceration, namely when they were in the ED. As a result, triangulation was not possible.

Schema of codes, themes, and subthemes.
Results
Participant information
Recruitment took place over the span of five months with 80% of eligible participants consenting to the study. Twenty-five individuals were approached for recruitment. Five did not participate in the study; two expressed interest but due to ongoing patient care activities were not interviewed; others did not provide reasons for declining. Twenty interviews were completed, with an average duration of 31 min and a range of 17–60 min. Participants were on average 61 years old. All participants were being held in the county jail. The study population self-identified as 100% male, 45% White, 50% Black, and 35% Hispanic/Latino. This sample was representative of the broader demographics of the jail population. The sample had an average Charlson comorbidity index of 5.6, ranging from 1 to 14 (see Table 1). They had high rates of jail infirmary visits, ED visits, and hospital admissions over the past 12 months (see Table 1).
Two major themes emerged regarding navigating the jail environment and accessing healthcare (see Table 2). First, participants had physical disabilities and limited autonomy that made the jail environment challenging. Second, participants had difficulty accessing healthcare in the jail setting due to personal and systemic barriers.
Theme 1: challenges navigating jail environment
First, participants reported challenges in the jail environment due to disability, with limited autonomy to address their needs. These challenges caused difficulty in their day-to-day life in the jail setting, including basic needs such as diet and sleep.
Subtheme 1: disability as an unaddressed barrier
Participants described physical disabilities that caused functional impairments. One participant had a tremor due to Parkinson’s and could not grasp objects around him. Visual impairments, whether from cataracts or other causes, also were a significant disability. As a result, participants reported difficulty, such as reading printed instructions. Although the jail policy includes a medical and dental screening exam for all inmates, only one participant reported being flagged as a fall risk.
Participants repeatedly cited sleeping arrangements, specifically the inaccessibility of top bunk beds, as a challenge. Although participants had received a bottom bunk pass from the correctional facility, they reported officers and staff would not enforce the pass system. Participants described physical violence and social bullying from younger inmates if older inmates tried to use their bottom bunk pass. As a result, participants described sleeping on the floor.
“You apply for a bottom bunk pass, but when [the guards] come around, do they check who got one? I got five old guys sleeping on the floor. [The younger inmates] know they don’t got a bottom bunk pass, but they still won’t get out.”
- Participant 7.
Participants described some systemic accommodations for inmates. For the jail counts, participants could remain seated rather than standing throughout the whole process. Additionally, inmates who could not travel to the mess hall for meals had the option of meals being brought to them. However, participants reported that delivered meals were often stolen by other inmates if the recipient was sleeping during delivery.
Subtheme 2: limited autonomy to address self-identified needs
Although aware of their own needs, participants found the jail environment challenging to fully address those needs. For example, access to time and space to exercise was limited. Although participants could request to go outside for exercise, they reported going outside once a week. Participants also reported a limited ability to follow healthy diets.
“[We] try to be healthy but it’s difficult… We go through the commissary to buy certain stuff like vitamins to complement [the hall food].”
- Participant 1.
Participants also had difficulty receiving care for their chronic conditions. For example, inmates described interruptions to their home medications due to formulary limitations.
“When I was arrested, I was in process of packing my car up to leave, and they pulled up, and I told him to make sure, if you take me to jail, get my medications and all that out of my car. And he did, but [the staff] are telling me that half of [my medications], I’m not going to get anywhere. It’s terrible because [the jail] don’t supply those that they don’t have [on formulary].”
-Participant 6.
Many jail processes relied on kiosks and a tablet system, including commissary purchases and infirmary requests. Inmates who had difficulty navigating these technologies would ask other inmates for assistance. However, some inmates posed a financial threat for older, less technologically savvy inmates. Participants emphasized the need for caution, as some inmates would use it as an opportunity to steal commissary funds or other valuable information for themselves.
“So most inmates are computer illiterate, especially some of the elderly and the ones who don’t have any formal education, so they’ll have to ask around and ask around [to request medical attention on the kiosk], and then in the process of doing that, they have to be careful, because inmates steal their [inmate ID] numbers and get access to their phone codes, and they steal the information. So, you know, you have to be careful who you ask.”
-Participant 4.
Theme 2: challenges navigating acute healthcare needs
Second, participants faced numerous delays attempting to access healthcare, including lack of clarity around procedures for accessing care and perceived skepticism about the veracity of their medical complaints from correctional facility staff. Participants reported individual staff members were significant resources or barriers for receiving care.
Subtheme 1: confusion around policies
Confusion regarding how to access healthcare led to delays in receiving medical attention. When every participant was asked how to seek medical attention while in jail, they gave varying answers. Some participants reported not receiving orientation and relying on word of mouth for instructions. Others correctly reported the kiosk system as the primary inmate-initiated way to request medical attention but then described difficulty using the kiosk or broken kiosks in their jail area. Participants often described using informal workarounds, such as relying on family to email correctional staff or asking the staff during medication administration time for assistance. Participants also described the presence of an in-unit officer who could flag inmates for immediate medical attention. Facilitators were most commonly people, including in-unit officer, family members. However, some participants did not understand the process of asking for medical attention. One participant did not know there was a jail infirmary and reported being sent to the hospital for medical evaluation was contingent on good behavior.
“There’s not an infirmary at this jail. So you have to find somebody then they judge whether you’ve been like good or bad and then they send you here.”
- Participant 2 (Spanish speaking).
Inmates who did not know how to navigate the kiosk system to request medical attention received care through a set of fortuitous circumstances. One participant was actually found lying on the ground after having fallen in the jail and brought in for medical attention. However, he was only discovered when staff entered the cell for a different inmate who had fallen.
Subtheme 2: distrust and skepticism
Participants described distrust and skepticism in the healthcare setting impeding their ability to receive timely medical attention. Participants acknowledged the distrust from correctional staff stemmed from other inmates malingering but felt that older inmates should be viewed as more trustworthy given their complex medical conditions.
“I can see where they’re coming from, because so many guys in [jail], they’re fake. You know, they’re just trying to get out or get pills or something to make stuff up, but I don’t know, maybe anybody over a certain age is actually believable?”
- Participant 3.
Participants also described distrust towards the medical staff. While participants acknowledged the helpfulness of some staff, other staff were viewed as uninterested in assisting inmates. Participants described the perception that some healthcare staff were providing substandard care that did not address inmates’ concerns or their health needs.
“[The staff] don’t look at your problems. Doctors don’t actually sit there and give you examinations. When you sit down in the chair, they type on the board without putting the [stethoscope] on your heart, and then they go by what’s on the board and that’s it. That’s the best. If you say something, it’s causing a disturbance. Only the doctor gets to talk, and you just sit there and let him see what he’s going to do. So how can you say? How can I tell you what’s wrong with me if I don’t talk?”
- Participant 12.
Discussion
Our qualitative study of geriatric county jail patients receiving care in the county ED described challenges with aging and healthcare. Participants faced challenges in their daily lives in the jail due to unaddressed disability and limited autonomy to address their needs. We also found widespread confusion and wide variability in participant abilities to request medical attention for acute healthcare need, with feelings of distrust present in the patient-physician relationship.
Our findings demonstrate an element of serendipity that impacted the healthcare experience. A sympathetic officer, a cellmate’s medical need prompting the discovery of a geriatric PEI found down, and an involved family member with strong advocacy skills are examples of ways geriatric PEI in our sample received care. Conversely, the system was difficult for many geriatric PEI to navigate. Many participants showed difficulty describing the process in which to receive care; from describing the kiosk system to using the kiosks themselves, geriatric PEI found the existing system inaccessible.
Our study findings are in line with similar studies conducted internationally and in the prison setting. Specifically, there are multiple structural challenges to providing healthcare in correctional environments including the built environment11; limited or nonexistent accommodations for functional and age-related impairments17; insufficient levels of staffing and training particularly regarding geriatric conditions29; and lack of autonomy among PEI30. However, in studies conducted internationally and in the prison setting, social ties and informal workarounds are also frequently utilized to facilitate healthcare31. However, the transient nature of jail incarceration may make these social ties more tenuous than prison incarceration.
Our study suggests room for multiple potential age-friendly interventions in the jail setting to address healthcare access for geriatric PEI. Reliance on digital technology may be more difficult for geriatric PEI, particularly those with histories of prolonged incarceration32. Multiple participants in our study described relying on a fellow inmate to submit requests via the digital kiosk system. Formalizing this process may be an effective way to assist geriatric PEI while also developing job skills for other PEI. Peer caregiving has been piloted in some United States prisons with inmates who have dementia and should be trialed in jail settings33,34. The use of peer community health workers has been effective helping geriatric and recently incarcerated patients navigate healthcare access35,36. While certain prison systems have begun implementing dementia-friendly units, further work is needed in jail systems. Multiple states have introduced dementia training for staff, facility environment modifications and other interventions37,38, but this has been largely limited to prisons and not jails. Furthermore, abolition medicine argues for envisioning alternative placements for PEI given “the contradictions inherent in providing health care” in a carceral setting39. However, despite the rise of geriatric parole laws in the United States, this mechanism of release has not been widely utilized40.
This study has several limitations. Although recruited from a county ED sample, all participants in this study were incarcerated in the county jail, rather than a mixture of correctional facilities. In addition to the transient nature of the jail environment compared to the prison setting, there is also wide variability among specific correctional systems’ medical capabilities that limit the generalizability of our findings. Furthermore, our sample was 100% male so experiences may not be generalizable to the experiences of women, nonbinary, or transgender PEI. Because our sample was limited to PEI in the ED and successfully accessed healthcare, we do not know barriers encountered by PEI who never were evaluated in the ED. Similarly, we only included participants who were able to consent and not critically ill, so we do not know the experiences of PEI with significant cognitive impairment or critical illness. Because we only interviewed English- and Spanish-speaking patients in this study, PEI who speak other languages may experience language barriers and other unique challenges to accessing healthcare. Further research is needed in these populations. We also did not interview correctional officers and healthcare staff. This was because we were interested in exploring PEI’s perceptions and experiences. We relied solely on interviews. Additionally, we were unable to return transcripts nor results to participants for feedback due to logistical challenges with follow up. Similarly, triangulation was not possible. We did not take field notes. However, interviewers took notes on participant responses and after every interview, we debriefed and made memos from group discussions.
Our novel study focused on experiences of geriatric PEI in jail showed multiple challenges of aging and healthcare access with limited autonomy and resources to address them. Participants expressed confusion about navigating the jail environment and healthcare system, in addition to distrust complicating the relationship between PEI and staff. Further work is needed to elicit the perspectives of correctional officers, healthcare workers, and PEI with cognitive impairment, different languages, and gender diverse experiences and elucidate potential interventions to address aging and healthcare while incarcerated.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Aebi, M. F. & Cocco, E. SPACE I: Prison Populations. Council of Europe Annual Penal Statistics;1–132 .
Buehler, E. D. & Kluckow, R. Correctional Populations in the United States, 2022 – Statistical Tables 1–22 (US Department of Justice. Office of Justice Programs. Bureau of Justice Statistics., 2024).
Widra, E. The Aging Prison Population: Causes, Costs, and Consequences. Prison Policy Initiative; 2023. Accessed January 3, 2025. https://www.prisonpolicy.org/blog/2023/08/02/aging/
Patterson, E. J. The Dose–Response of time served in prison on mortality: new York State, 1989–2003. Am. J. Public. Health. 103 (3), 523–528. https://doi.org/10.2105/AJPH.2012.301148 (2013).
Berg, M. T., Rogers, E. M., Lei, M. K. & Simons, R. L. Losing years doing time: incarceration exposure and accelerated biological aging among African American adults. J. Health Soc. Behav. 62 (4), 460–476. https://doi.org/10.1177/00221465211052568 (2021).
Brinkley-Rubinstein, L. & Cloud, D. H. Mass incarceration as a Social-Structural driver of health inequities: A supplement to AJPH. Am. J. Public. Health. 110 (S1), S14–S15. https://doi.org/10.2105/AJPH.2019.305486 (2020).
Kouyoumdjian, F. G., Andreev, E. M., Borschmann, R., Kinner, S. A. & McConnon, A. Do people who experience incarceration age more quickly? Exploratory analyses using retrospective cohort data on mortality from Ontario, Canada. PLoS One. 12 (4), e0175837. https://doi.org/10.1371/journal.pone.0175837 (2017).
Lloyd, L. Cognitive health and incarceration among older adults. J. Am. Geriatr. Soc. 67 (3), 622–623. https://doi.org/10.1111/jgs.15699 (2019).
Greene, M., Ahalt, C., Stijacic-Cenzer, I., Metzger, L. & Williams, B. Older adults in jail: high rates and early onset of geriatric conditions. Health Justice. 6, 3. https://doi.org/10.1186/s40352-018-0062-9 (2018).
Baillargeon, J. et al. The prevalence of cognitive impairment and dementia in incarcerated older adults. Journals Gerontology: Ser. B. 78 (12), 2141–2146. https://doi.org/10.1093/geronb/gbad136 (2023).
Kaiksow, F. A., Brown, L. & Merss, K. B. Caring for the rapidly aging incarcerated population: the role of policy. J. Gerontol. Nurs. 49 (3), 7–11. https://doi.org/10.3928/00989134-20230209-02 (2023).
Williams, B. A. et al. Being old and doing time: functional impairment and adverse experiences of geriatric female prisoners. J. Am. Geriatr. Soc. 54 (4), 702–707. https://doi.org/10.1111/j.1532-5415.2006.00662.x (2006).
Beleckis, J. Perpetuating poverty: Formerly incarcerated people warn of agonizing choices around Wisconsin’s prison copays. WPR. (2022). https://www.wpr.org/justice/perpetuating-poverty-formerly-incarcerated-people-warn-agonizing-choices-around-wisconsins-prison. June 8, Accessed January 4, 2025.
Lupez, E. L. et al. Health, access to care, and financial barriers to care among people incarcerated in US prisons. JAMA Intern. Med. 184 (10), 1176–1184. https://doi.org/10.1001/jamainternmed.2024.3567 (2024).
Kitt-Lewis, E. & Loeb, S. J. Emerging need for dementia care in prisons: opportunities for gerontological nurses. J. Gerontol. Nurs. 48 (2), 3–5. https://doi.org/10.3928/00989134-20220111-01 (2022).
Gaston, S., Porritt, K. & Jordan, Z. Dementia care behind prison walls: A descriptive study Understanding nurse’s knowledge and educational needs. Nurse Educ. Pract. 72, 103787. https://doi.org/10.1016/j.nepr.2023.103787 (2023).
Di Lorito, C., Völlm, B. & Dening, T. The individual experience of ageing prisoners: systematic review and meta-synthesis through a good lives model framework. Int. J. Geriatr. Psychiatry. 33 (2), 252–262. https://doi.org/10.1002/gps.4762 (2018).
Eswaran, V. et al. Understanding the association between frequent emergency department use and jail incarceration: A cross-sectional analysis. Acad. Emerg. Med. 29 (5), 606–614. https://doi.org/10.1111/acem.14437 (2022).
Maher, P. J. et al. Emergency department utilization by a jail population. Am. J. Emerg. Med. 36 (9), 1631–1634. https://doi.org/10.1016/j.ajem.2018.06.034 (2018).
Booth, A. COREQ (Consolidated criteria for reporting qualitative Studies). In: Guidelines for Reporting Health Research: A User’s Manual. Wiley-Blackwell; 214–226. (2014).
Jail Population. Harris County Jail. Accessed January 20. charts. (2025). hctx.net/jailpop/App/JailPopCurrent
Resnick, B. et al. Reliability and validity of the evaluation to sign consent measure. Gerontologist 47 (1), 69–77. https://doi.org/10.1093/geront/47.1.69 (2007).
Callahan, C. M., Unverzagt, F. W., Hui, S. L., Perkins, A. J. & Hendrie, H. C. Six-item screener to identify cognitive impairment among potential subjects for clinical research. Med. Care. 40 (9), 771–781. https://doi.org/10.1097/00005650-200209000-00007 (2002).
Carpenter, C. R., DesPain, B., Keeling, T. N., Shah, M. & Rothenberger, M. The Six-Item screener and AD8 for the detection of cognitive impairment in geriatric emergency department patients. Ann. Emerg. Med. 57 (6), 653–661. https://doi.org/10.1016/j.annemergmed.2010.06.560 (2011).
Rockwood, K. et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 173 (5), 489–495. https://doi.org/10.1503/cmaj.050051 (2005).
Elliott, A., Phelps, K., Regen, E. & Conroy, S. P. Identifying frailty in the emergency Department—feasibility study. Age Ageing. 46 (5), 840–845. https://doi.org/10.1093/ageing/afx089 (2017).
Guest, G., Bunce, A. & Johnson, L. How Many Interviews Are Enough? An Experiment with Data Saturation and Variability. Field Methods. 18(1). Accessed November 3. (2022). https://doi.org/10.1177/1525822x05279903
Guest, G., Namey, E. & Chen, M. A simple method to assess and report thematic saturation in qualitative research | PLOS ONE. PLoS ONE. 15 (5). https://doi.org/10.1371/journal.pone.0232076 (2020).
Williams, B. A. et al. Caregiving behind bars: correctional officer reports of disability in geriatric prisoners. J. Am. Geriatr. Soc. 57 (7), 1286–1292. https://doi.org/10.1111/j.1532-5415.2009.02286.x (2009).
James, J. E. We’re not Patients. We’re inmates: older black women’s experience of Aging, Health, and illness during and after incarceration. Gerontologist 64 (4), gnad114. https://doi.org/10.1093/geront/gnad114 (2024).
O’Neill, A. et al. Social care for older adults in the criminal justice system: a brief report from a nominal group. J. Forensic Psychiatr. Psychol. 36 (1), 37–49. https://doi.org/10.1080/14789949.2024.2437449 (2025).
Hwang, Y. I. et al. (eds) (Jane),. Population ageing, incarceration and the growing digital divide: Understanding the effects of digital literacy inequity experienced by older people leaving prison. PLoS One. 19 (4), e0297482 (2024). https://doi.org/10.1371/journal.pone.0297482
Stewart, W. & Prost, S. G. Supporting Older, Frail, and vulnerable adult prisoners through peer care: Observations, Reflections, and recommendations based on a UK/U.S. Researcher exchange visit. J. Correctional Health Care. 30 (3), 149–152. https://doi.org/10.1089/jchc.23.11.0095 (2024).
Hongo, A. et al. The Gold Coats-An Exceptional Standard of Care 1st edn (CreateSpace Independent Publishing Platform, 2016).
Knowles, M., Crowley, A. P., Vasan, A. & Kangovi, S. Community health worker integration with and effectiveness in health care and public health in the united States. Annu. Rev. Public. Health. 44, 363–381. https://doi.org/10.1146/annurev-publhealth-071521-031648 (2023).
Ohuabunwa, U. et al. An integrated model of care utilizing community health workers to promote safe transitions of care. J. Am. Geriatr. Soc. 69 (9), 2638–2647. https://doi.org/10.1111/jgs.17325 (2021).
Gruss, V. & Hasnain, M. Addressing the needs of incarcerated inmates with dementia: creating Dementia-Friendly prisons. Innov. Aging. 3 (Suppl 1), S433. https://doi.org/10.1093/geroni/igz038.1620 (2019).
Ewing, M. When Prisons Need to Be More Like Nursing Homes. The Marshall Project. August 27, 2025. Accessed April 14. (2015). https://www.themarshallproject.org/2015/08/27/when-prisons-need-to-be-more-like-nursing-homes
DiZoglio, J. D. & Telma, K. Proposing abolition theory for carceral medical education. J. Med. Humanit. 43 (2), 335–342. https://doi.org/10.1007/s10912-021-09695-1 (2022).
State Medical and Geriatric Parole Laws. Accessed April 14. (2025). https://www.ncsl.org/civil-and-criminal-justice/state-medical-and-geriatric-parole-laws
Acknowledgements
Thank you to Annika Bhananker and Kelly Keene for your assistance with this study.
Funding
Research reported in this publication was supported by the National Institute On Drug Abuse of the National Institutes of Health under AwardNumber T32DA013911. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NationalInstitutes of Health.
Author information
Authors and Affiliations
Contributions
- MS: conception and design of the work, analysis and interpretation of the data, and drafting the manuscript- SC and MB: acquisition and analysis of the data- SY and NL: analysis and interpretation of the data- MR: design and acquisition of the data- JR: revisions of the manuscript- ANC: conception and design of the work, analysis and interpretation of the data, and revisions of the manuscript- All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Baylor College of Medicine Institutional Review Board (H-56301). Participants were approached for inclusion in the study if they had the ability to consent based on the Evaluate to Sign Consent measure. Only participants who consented were included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Suh, M.I., Chen, S., Benavides, M. et al. Incarcerated geriatric patients’ experiences of aging and healthcare. Sci Rep 16, 9936 (2026). https://doi.org/10.1038/s41598-026-40298-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-40298-9
