
Abstract
Depression is among the most prevalent mental disorders worldwide, carrying one of the highest burden of disease among all mental disorders. While invasive vagus nerve stimulation has been approved for treatment-resistant depression for decades, its clinical use is limited by surgical risks and heterogeneous clinical efficacy. Transcutaneous auricular VNS (tVNS) may offer a non-invasive alternative, but to date it remains experimental due to limited high-quality evidence, unclear biological mechanisms of action, and rudimentary knowledge on optimal stimulation parameters. To address these gaps, we initiated the AddVNS study. The AddVNS study (Add-on tVNS in depression) is a monocentric, exploratory, prospective, randomized, double-blind, sham-controlled interventional trial conducted at the Max Planck Institute of Psychiatry’s research hospital. Adult patients with a depressive episode (ICD-10: F31–33) were assigned to receive active or sham transcutaneous vagus nerve stimulation (tVNS) in addition to treatment-as-usual (TAU) over a six-week period. Stimulation is administered three times daily (30 to 60 min each), five days per week. A deep phenotyping strategy is applied, including repeated psychophysiological measures (e.g., pupillometry, ECG, photoplethysmography, electrogastrogram) and neuroimaging (structural and functional MRI) at baseline and post-intervention, continuous actigraphy, repeated blood and stool sample acquisition (pre-, mid-, and post-intervention) for multiomic investigation, comprehensive neuropsychology including self-rated personality assessment, and closely monitored clinical evaluations. The patient-reported outcomes are collected weekly, the clinician-rated scales pre-, mid-, and post-intervention. In addition, follow-up self-ratings are obtained at 6 and 12 weeks post-tVNS. The main objective of AddVNS is to improve our understanding of the biological effects elicited by tVNS in depression. By combining rigorous methodology with an extensive and longitudinal multimodal approach, AddVNS represents the most comprehensive investigation of tVNS effects and markers in depression to date. We believe it to significantly advance our mechanistic understanding and subsequently clinical translation of this promising intervention.
Similar content being viewed by others


Introduction
Depression is the second most prevalent mental disorder worldwide and is associated with the highest burden of disease among all psychiatric disorders1,2. The lifetime-prevalence of major depressive disorder (MDD) in Germany is estimated to be 11,6%3. MDD is a major risk factor for suicide and is associated with higher risk for somatic diseases and mortality4,5,6 and therefore it is also a vast burden for the healthcare system7,8. To treat depression, pharmacotherapy and psychotherapy are the standard of care. Still, response rates are in general moderate: approximately 30% of the patients show a treatment-resistant course of disease9. Especially for those patients, neurostimulation treatments like repetitive transcranial magnetic stimulation (rTMS), electroconvulsive therapy (ECT) or vagus nerve stimulation (VNS) are important therapeutic strategies10,11.
In Europe, invasive VNS has been approved for the treatment of drug-resistant epilepsy since 1994 and for the treatment of treatment-resistant depression (TRD) since 200112,13. In 2005, invasive VNS was approved by the US Food and Drug Administration (FDA) for the treatment of MDD that has not responded to at least four adequate trials of antidepressants14. Invasive VNS requires the surgical implantation of an impulse generator13. Because of the associated possible surgical complications as well as high treatment costs, invasive VNS is not often used in the treatment of depression15. Transcutaneous auricular VNS (tVNS), on the other hand, is a non-invasive alternative to traditional invasive VNS. During tVNS, a transcutaneous impulse generator stimulates the auricular branch of the vagus nerve (ABVN) using soft electrical currents. The direct neuroanatomical connection of the auricular branch of the vagus nerve to the nuclei of the brainstem is a possible pathway through which tVNS may exert its biological effects16. During the last decade, the effects of tVNS have been examined in an increasing number of clinical trials and across many different clinical populations and disorders, with depression being one of the most prominent areas of interest17. Studies have jointly suggested that tVNS may be an effective and well tolerated treatment for MDD18,19, peripartum depression20, and TRD21. Evidence for the potential of tVNS to improve MDD comes from meta-analyses, although these analyses included a relatively small number of studies, some of which exhibited methodological limitations22,23. Meanwhile, the safety and tolerability of tVNS is well established and it has not been associated with severe adverse effects unlike invasive VNS15,24. Potential side effects of tVNS are mild and local symptoms and include, but are not limited to, skin irritation along with non-specific symptoms like transient mild headache or dizziness15,25. Along with its tolerability, the enhanced accessibility and ease of application of tVNS, compared to other neurostimulation methods, further contribute to its feasibility26.
In the German, but also other national depression treatment guidelines, tVNS is still considered an experimental treatment11. Reasons for this categorization come from the relative novelty of the intervention, the limited high-quality evidence from randomized clinical studies, the not yet fully understood biological mechanisms of action26, and the limited knowledge about the optimal stimulation parameters25,27.
To date, numerous hypotheses have been proposed regarding the biological mechanisms underlying the antidepressant effects of invasive vagus nerve stimulation and, by extension, transcutaneous VNS. The proposed mechanisms include, but are not limited to, changes in functional brain connectivity, modulation of neurotrophins and subsequent increase of neurogenesis, inhibition of systemic inflammation, normalization of the hypothalamus-pituitary-adrenal (HPA) axis, modulation of neurotransmission, and changes in the gut microbiome26,27,28,29,30,31,32,33. For these hypotheses, there is only limited or indirect evidence primarily from preclinical studies or from application of VNS in other disorders26,30. To date, however, it is unclear which of these mechanisms contribute to the therapeutic effects of VNS in depression. It is thus not surprising that, so far, no reliable bio- or predictive markers exist for tVNS in depression25.
To address these issues, we developed and initiated the AddVNS study. The primary objective of the study is to identify biological, psychological, socio-demographic, and clinical biomarkers associated with augmentative tVNS in patients with a depressive episode.
Study design
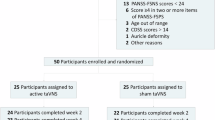
The AddVNS study is a monocentric, exploratory, prospective, randomized, double-blind, sham-controlled interventional study with a recruitment period of 3 years. It commenced in 2025 and is conducted at the research hospital of the Max Planck Institute of Psychiatry (MPIP). The study information has been aligned and filled out in the SPIRIT guidelines including a schematic participant timeline diagram (Fig. 1). Also, the research protocol version 1.0, structured in accordance with the Research Ethics Review Committee of the World Health Organization, can be found in the supplement.

Schematic diagram of participant timeline in the AddVNS study. Patient health questionnaire 9 and 15 (PHQ9 and PHQ15), Beck Depression Inventory II (BDI-II), Snaith-Hamilton-Pleasure-Scale (SHAPS), Rejection Sensitivity Questionnaire (RSQ), World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0.), Montgomery–Åsberg Depression Rating Scale (MADRS), Hamilton Rating Scale for Depression with 21 items (HAM-D21), Hamilton Rating Scale for Anxiety (HAM-A), Global Assessment of Functioning (GAF), Pulse plethysmography (PPG), Personality Inventory for DSM-5 Brief form (PDI-5), functional MRI (fMRI). Created with Biorender.com.
Participants receive either tVNS or sham tVNS for 6 weeks in addition to treatment-as-usual (TAU). Psychophysiological assessments, clinical interviews, blood draws, and stool collection are scheduled at baseline as well as 3 and 6 weeks after tVNS start. A functional MRI (fMRI) session as well as an extensive neuropsychological assessment is performed at baseline and after 6 weeks post tVNS start. Additionally, a personality self-report assessment is acquired at baseline. Furthermore, participants are asked to complete self-rating questionnaires on a weekly basis. The optional questionnaire-based follow-ups are inquired 6 and 12 weeks after tVNS end. Study duration thus amounts to 8 weeks plus 12 weeks of follow-up.
The study will start with a pilot. Here, two additional psychophysiological measurements (amounts to a total of five measurement time points) will be conducted during tVNS stimulation up to 20 participants after the initial psychophysiological assessment at baseline and following 3 weeks of tVNS application. The objective of this pilot is to examine acute effects of tVNS on psychophysiological parameters, providing first insights into the potential mechanisms of action. Owing to the exploratory and first-in-field nature of this study, patient and public involvement was not included in the study design. The AddVNS study’s multi-omics read-outs are shown in Fig. 2.

Graphic summary of the AddVNS study’s multiomics approach. Created with Biorender.com.
Participants
Only adult patients (≥ 18 years) with current MDD or bipolar disorder with current depression (BD) who are treated at the MPIP’s research hospital (either inpatient or day clinic treatment) and are able and willing to give informed consent can participate in the AddVNS study. Inclusion criteria are: (1) age 18–65 years, legally competent and able to provide informed consent; (2) diagnosis of a depressive episode (MDD or BD) according to ICD-10 or ICD-11; (3) signed informed consent documents for the AddVNS study; (4) signed informed consent and participation in the biobanking project of MPIP (Project No. 338 − 15). Exclusion criteria are: (1) age < 18 years or age > 65 years; (2) pregnancy or planning to get pregnant during the study period, breastfeeding; (3) legal supervision; (4) pervasive developmental disorders and/or intellectual disability; (5) acute substance abuse (e.g., alcohol, prescription or illicit drugs); (6) severe neurological disease; (7) anatomical or technical impossibility of tVNS administration (e.g., microtia, anotia, or history of vagotomy); (8) current treatment with an established neurostimulation method (e.g., ECT, rTMS, VNS); (9) metallic foreign bodies, implanted intracranial devices or cerebral shunts; (10) severe general illness (e.g., relevant anemia requiring transfusion, high-grade cardiac arrhythmia, severe cardiomyopathy); (11) active implants (e.g., cochlear implant, pacemaker, implantable cardioverter-defibrillator).
Randomization and blinding
After inclusion, participants are randomized to verum or sham tVNS. Participants are blinded to their study arm, since the verum and sham electrode look alike and the weekly titration was performed in both groups. Investigators performing study assessment are also blinded to the study arm, except for study personnel responsible for the stimulation parameter settings and weekly titration. A block-wise randomization approach was chosen34. This design was selected to reduce the likelihood that participants in different intervention arms would share information about their stimulation-related experiences or sensations. Participants within a block receive the same intervention. Block sequence and size was based on an allocation list. A new block is started after the study participation for the patients of the previous is completed. Blinding integrity was assessed during the final week of the sham/verum tVNS by asking participants to indicate which treatment arm they believed they had been assigned to.
Intervention
Participants receive either tVNS or sham tVNS for a period of 6 weeks. Both interventions are administered as an adjunct to TAU, which is provided by the participants’ attending physicians and psychologists according to clinical expertise and guidelines. Both tVNS and sham tVNS intervention are carried out three times a day (morning, noon, evening) from Monday to Friday. Each of the three daily stimulation sessions lasts 30 to 60 min, depending on the individual tolerance (= individual subjective comfort and tolerability of stimulation) of the participant. Flexibility in stimulation duration was permitted to optimize adherence by accommodating individual tolerability, preferences, perceived autonomy, and comfort.
The stimulation is performed with the device tVNS E ® (tVNS Technologies GmbH, Erlangen, Germany). The device is CE certificated and approved as Class IIa medical device under the Medical Device Regulation of the European Union. The device consists of a stimulator the size of a small cell phone and an ear electrode that is placed at the stimulation site.
The stimulation protocol was developed considering earlier tVNS studies and the mandatory sections of the device’s instruction manual20,21,35. The stimulation site is the cymba concha of the left ear, since the latter is thought to be exclusively innervated by the vagus nerve36. Thus, the left vagus nerve is stimulated (similar to invasive VNS), which is thought to reduce the risk of bradycardia since the right vagus primarily innervates the sinoatrial node of the heart, although human studies are still needed to confirm this distinction and its clinical relevance37. Nonetheless, right-sided or even bilateral tVNS has been shown to be safe15. Prior to the actual stimulation, stimulation intensity (electrical current) is determined by titration. Here, the highest level (mA) tolerated by the patient, that is the value between the individual perception- and pain threshold, is used for the longitudinal tVNS stimulation. During weekly titration sessions, stimulation intensity was adjusted beginning at the lowest level (0.1 mA) and increased in 0.1 mA increments until a clearly perceptible yet comfortable sensation was achieved, without pain, up to a maximum of 5 mA. Electrical current of the tVNS E ® can be adjusted between 0.1 and 5.0 mA. Other stimulation parameters are set to the device’s default settings: biphasic stimulation, frequency 25 Hz, pulse-pause ratio 28 s : 32 s.
During the first tVNS stimulation session, study personnel provide detailed instructions on how to use the device in person. In the following sessions, participants perform the thrice daily stimulations by themselves and can reach out to study personnel if questions arise. Any adjustments to the current intensity, including titration during the intervention period, are performed by study personnel only. If a participant intentionally alters stimulation parameters including localization of the ear-electrode in a way that endangers either blinding or the study objective, the individual will be excluded from the study. In addition, regular check-ups are performed by study personnel to prevent errors during the stimulation.
Sham tVNS is performed identical to tVNS, with the only exception that the sham tVNS is conducted with no current using the manufacturer’s tVNS E ® sham electrode. Visually, the sham electrode cannot be distinguished from a regular stimulation electrode. This approach was chosen to maximize discrimination between specific neurostimulatory effects and non-specific contextual or placebo effects, while still matching key elements of intervention.
The time and duration of each stimulation session is documented by the patient. Additionally, the app (tVNS® Patient) is used to retrieve, track, and double-check stimulation parameters. This systematic documentation enables dose–response analyses. To prevent unblinding, only investigators responsible for stimulation have access to the app.
Measures
Sociodemographic data (e.g., age, sex and gender, occupation) and medical information (e.g., patient-, family-, and drug anamnesis, medication history and current medication, results of clinical diagnostics and clinical tests such as ECG and EEG) are extracted from patient records.
Psychophysiological assessment and actigraphy
Psychophysiological measurements are conducted at baseline, after 3 weeks of intervention and at the end of the 6-week intervention period. These three measurements are acquired without simultaneous tVNS. In the pilot (n = 20), additional psychophysiological measurements will be additionally conducted immediately after starting the morning tVNS stimulation session at baseline and following 3 weeks of tVNS application. The measures encompass an N-Back task and a reward task. In the N-back task, which evaluates the working memory capacity, a sequence of stimuli is presented to the subjects, who indicate through pressing a button, if the current stimulus matches a stimulus presented N steps earlier in the sequence38. In AddVNS, the visual stimuli are capital letters (the consonants B, C, D, G, P, T, W). The reward task has been reported in earlier studies of our institute39. The variant that will be used in the AddVNS study comprises four conditions: a potentially rewarding response condition with a reward stimulus, a neutral response condition (neutral stimulus), a potential loss condition and a control condition without a response requirement (stimulus without response). After the presentation of the stimuli and a brief flash of light, the subjects must respond by pressing a button. If they respond fast enough, they will receive a financial reward (1 €) or a non-monetary reward (a green checkmark symbol). If the reaction is too slow, a red cross appears, which is followed by a financial loss (-1 €) in the loss condition. In the control condition, no flash is presented and therefore no reaction is required. An adaptive algorithm ensures that participants are successful in around 50% of reward trials. Pupil measurements and reaction times are recorded during the reward task. Furthermore, short measurements (e.g. resting state pupillometry, pupillometry during five separate light flashes, word-pairs association task) will be used as control conditions.
For the psychophysiology measurements, we use Biopac’s MP150 System (Goleta CA, USA, biopac.com) in our psychophysiology lab. Pupillometry is assessed with an inhouse Unity-based presentation environment (stimuli are presented on a screen in an Office) for an HTC Vive Pro Eye system with Tobii Eye-Tracking, with a sampling rate of 120 Hz (HTC Corporation, Taoyuan, Taiwan). During the psychophysiological measurements in our psychophysiology lab, the following parameters are assessed using the MP150 system with Bionomadix Wireless units: a 3-lead ECG with one electrode under the right collar bone, one under the left collar bone and one above the left-front side of the hip (LEAD II), respiration with a respiratory belt on the lowest part of the diaphragm, pulse plethysmography acquired on the left middle finger and a 3-lead electrogastrogram on the stomach area. The activity pattern and continuous physiology of participants over the 6-week intervention including the repeated psychophysiology lab session are measured using a wrist-worn actigraph (ActiGraph LEAP, Ametris, Pensacola FL), which provides continuous measures of activity, heart rate, oxygen saturation, and skin temperature, among others. The heart rate signal forms the basis for further processing, with the RR-intervals as inputs for segmented, sliding-window-based heart rate variability analyses (spectral metrics, statistical metrics, and respiratory-sinus arrhythmia-based metrics).
For pupillometry, the primary focus of the analyses will be on measures summarizing the pupillary light reflex (e.g., constriction velocity, amplitude), pupillary unrest (e.g., mean and variance metrics) during a 6-minute resting-state, mean pupil values during working memory blocks, and pupil responses during reward anticipation as in40,41. Pupillometric data will be pre-processed with linear blink-interpolation, smoothing and z-transformation, among others40,41, with in-house scripts in Matlab 2025 (The Mathworks Inc., Natick, Massachusetts, 2025). EGG will be spectrally analyzed according to consecutive 256s epochs, with 192s overlap according to the Handbook of Psychophysiology, Chap. 12 – Levine et al.42.
MRI scans
Two identical MRI sessions are acquired. The first session is scheduled at baseline, the second one after the 6-week of tVNS. The elements of the MRI assessment are shared with the imaging protocols of our institute’s deep-phenotyping study BeCOME (Project No. 350 − 14)43. MRI protocols include an anatomical T1-weighted sequence, a diffusion tensor imaging (DTI) and an axial fluid-attenuated-inversion-recovery (FLAIR) sequence. Moreover, resting state functional MRI (rs-fMRI) and the following specific fMRI sequences and tasks are obtained:
-
(i)
Neuromelanin (NM)-sensitive MRI: this sequence will be used to measure the functional and structural status of the locus coeruleus, the substantia nigra and the area tegmentalis ventralis (VTA). It is an established method used in the research of the noradrenergic and dopaminergic neurotransmission44,45,46,47. The NM-sensitive sequence will also allow to precisely localise these brainstem structures for the functional analyses.
-
(ii)
Brainstem-sensitive fMRI-BOLD sequences: This is a sequence for fMRI-BOLD time series aligned to methodological recommendations of a sequence and post-processing comparison for brainstem imaging48. It allows, in combination with appropriate post-processing, the investigation of the functional relationship between individual brainstem nuclei48.
-
(iii)
Reward anticipation task: This established task43 allows the quantification of three key circuits during reward anticipation (early activation of the ventral striatum, later activation of the salience network and deactivation of the default mode network). As described earlier for the reward task during psychophysiological measurements, a further stimulus type, which results in a small loss of money if performance is too low, will be added to the three established stimuli (possibility of winning money, verbal feedback, no possibility of winning). Overall, small symbolic play money sums with maximum total gains of 1–5 € will be used. The dynamic aspects of the task have been studied using combined fMRI/pupillometry experiments in healthy subjects39 and patients with major depressive disorder49. To allow for flexible secondary statistical methods, we will define between 2 and 5 regions-of-interest per network from large independent samples that have undergone the same task (e.g.43.
-
(iv)
Short imaging stress test (short-IST): This task is a reduced version of an imaging stress test43,50 that combines arithmetic calculation with (negatively feedback) evaluation. This reduced 10’ version presents 1-minute-episodes of arithmetic calculations with mild evaluation alternating with 40 s of pausing, causing marked autonomous nervous system (ANS) response that can be mapped to central ANS perception or regulation processes51.
rs-fMRI and reward-fMRI are carried out with simultaneous eye tracking and pupillometry (EyeLink 1000 Plus System with long range (MR) Mount, SR Research). Furthermore, heart and respiratory rate are recorded throughout the MRI scan using pulse plethysmography and a respiratory belt. No MRI contrast agent is injected.
Blood-based multiomics
The collected blood samples will be used for genome-wide genotyping and epigenetic/DNA methylation analysis as well as mRNA sequencing, analysis of neuron-derived exosomes, cytokine and immune metabolite analysis, immune cell phenotyping and analysis of metabolic and endocrine markers. For more details on blood-based analyses, we refer the interested reader to the published protocol of DetECT study52, which proposes the same multiomics measures.
Stool samples
Stool samples are collected at baseline and after 6 weeks of verum or sham tVNS using the Bunny Wipe Fecal Sample Collector System (Zymo Research). If tolerated by a participant, additional sample collection after three weeks of tVNS is performed. Stool samples will undergo shotgun metagenomic sequencing, as done in related studies, to enable taxonomic and functional characterization of the gut microbiome over time.
Psychometric measures
Self-rating questionnaires along with clinician-rating scales are used to systematically evaluate the patients’ mental and physical condition in detail and to assess the effects of tVNS over the course of treatment. All questionnaires and rating scales used in the AddVNS study are well established and standardized instruments in clinical practice and research. Only German versions of the questionnaires and rating scales are used.
Participants are asked to fill out the following questionnaires once a week: patient health questionnaire (PHQ) 953,54,55 and 1553,56, Beck Depression Inventory II (BDI-II)57, the Snaith-Hamilton-Pleasure-Scale (SHAPS-D)58,59 and the Questionnaire for complaints of cognitive disturbances (FLEI)60. The PHQ-9 with nine items, the BDI-II with 21 items and the SHAPS-D with 14 items are self-rated scales used widely in the treatment and research of depression. The PHQ-15 with will be used to assess the physical symptoms of the participants. Free fields were added to the PHQ-15 for the patients to report side effects or physical complaints related or attributed to tVNS. The FLEI World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0.) with 35 questions is used to evaluate the patients’ neurocognitive symptoms. At baseline and after the 6-week intervention, participants also fill out the Rejection Sensitivity Questionnaire (RSQ)61,62 and the World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0.) questionnaire63. The German modified version of RSQ with 20 items62 is a measure of rejection sensitivity (RS) to explore the role of RS in the context of tVNS in depressive disorders. The WHODAS 2.0. questionnaire is a self-rating instrument with 36 items for the assessment of health, functioning, disability and health-related quality of life which can be used across all diseases63. Questionnaires are available as paper-pencil printed version or electronically (QR-code or email link or tablet computer, all via a secure study platform).
Clinical interviews are conducted at baseline, after 3 weeks of intervention and after 6 weeks of intervention. During these interviews, trained study personnel obtains the following scales: Montgomery–Åsberg Depression Rating Scale (MADRS)64,65, Hamilton Rating Scale for Depression with 21 items (HAM-D21)66,67,68 and Hamilton Rating Scale for Anxiety (HAM-A)69. The Global Assessment of Functioning (GAF)70,71 will also be obtained using information provided by the patient`s clinical ward team at the same time points. The MADRS (10 items) and the HAM-D21 are used to assess the severity of the present depressive episode. The GAF, which is a compound scale derived from the DMS-IV that rates global socioemotional impairment of patients with mental disorders, is used as a functionality proxy.
Neuropsychological assessment and personality assessment
Neuropsychological assessment is carried out at baseline and after the 6-week intervention using the Cognitive Basic Assessment Test set (COGBAT)72 as well as the “Mehrfachwahl-Wortschatz-Intelligenztest” (MWT-B)73 and an episodic memory test74. The COGBAT was administered using the standardized software and hardware provided by the test distributor (Schuhfried). The MWT-B and the episodic memory test are administered in their respective standardized printed formats in accordance with the publishers’ guidelines.
Personality assessment is performed at baseline using the German short version of the Personality Inventory for DSM-5 (PID-5-BF + M) and the German short version of the Level of Personality Functioning Scale-Brief Form 2.0 (LPFS-BF 2.0)75,76,77. Both questionnaires can be filled out quickly by patients and allow a reliable assessment of personality traits. In the AddVNS study, PID-5-BF + M and LPFS-BF 2.0 will be used to investigate the role of personality traits in the depressive episode in the content of the biological effects of tVNS.
Follow-up
To assess the long-term effects of tVNS, including the lasting self-reported clinical effects in e.g. the home environment after discharge from clinical care, we ask the participants to fill out self-rating questionnaires 6 and 12 weeks after the end of the intervention. At each of these two points, the questionnaires BDI-II, PHQ-9, PHQ-15, SHAPS-D, FLEI and WHODAS 2.0. are obtained. In case the participants have been discharged prior to the follow-up, they will receive the paper-pencil questionnaires (by mail) or be asked to complete them electronically after receiving a link via email, in accordance with our data protection and privacy policy.
Sample size calculation
Earlier tVNS studies with a design similar to AddVNS, which have focused on clinical outcomes rather than biological ones, have shown low to moderate effect sizes18,19,23,35. Moreover, depression is a complex and multifactorial disease, which emerges through the long-time interaction between genetic predisposition and environmental factors78. Since no prior multi-omics studies on tVNS effects are available, the sample size calculation was based on the average effect sizes reported in existing clinical tVNS studies. This approach assumes that clinical efficacy reflects the aggregate downstream effects of multiple interacting biological pathways underlying tVNS and can therefore serve as a pragmatic proxy of expected average effect size of omics domains in the absence of direct multi-omics effect size estimates. Such an approach can be considered contemporary and appropriate for early-phase or exploratory multi-omics trials52,79,80. In addition, the AddVNS study incorporates an internal pilot phase. Should pilot data unexpectedly indicate that the main assumption regarding effect size is significantly inaccurate, sample size estimates will be updated prior to completion of recruitment, in line with established methodological recommendations81,82. Using a G-power calculation tool83, we estimated a sample size of n = 86 (ANOVA with repeated measures, 2 groups, effect size Cohen’s f = 0.25, significance level a = 0.05, power = 0.95, allocation in study arms 1:1, correlation between repeated measures = 0.3).
Based on prior experience with stimulation studies conducted at our clinic52, the AddVNS study anticipates a study discontinuation rate (including loss to follow-up) of approximately 30%. To account for this, we plan to recruit up to n = 112 participants, ensuring that at least n = 86 complete datasets are available for statistically meaningful analyses in accordance with the sample size calculation. Data from participants who discontinue the study will be included in the final analyses under an intention-to-treat framework. In addition, if more than 10% of data are missing, missing values will be handled using established imputation methods and the results will be compared with those obtained from the intention-to-treat analyses. Using heart rate variability-based stratification, among other psychophysiological and fMRI measured (e.g., pupil size), subgroup analyses will be performed.
Main hypotheses and statistical analyses
The focus of the statistical analyses in the AddVNS study is to examine the longitudinal changes between the two study arms (tVNS vs. sham tVNS) at the level of neurobiological readouts. Our aim is to identify parameter patterns that allow direct or indirect conclusions primarily about the biological effects of tVNS and secondarily, its clinical effects. Age, sex, socioeconomic status, BMI, smoking status, and pharmacological treatment (psychiatric and otherwise) as well as comorbidities will be integrated as covariates. Analyses will be performed regularly (e.g., after the pilot phase) as well as at the study’s end.
At the neuroimaging level, given the neuroanatomy of tVNS16 several functional readouts will be used for the study of tVNS effects over 6 weeks, contrasted against sham treatment. The general underlying hypothesis is that the 6-week stimulation course produces midterm-lasting functional effects that could underlie parallel or future clinical effects.
-
(i)
Functional reward system response changes that comprise the VTA and nucleus accumbens / ventral striatum, and possibly also the locus coeruleus itself, can be detected by the monetary delay reward task43.
-
(ii)
Exploratively, comparisons of task-free brainstem fMRI data will be performed after brainstem-focused preprocessing, based on reports on short term effects in downstream targets of vagal afferents including the nucleus of the solitary tract, the substantia nigra, subthalamic nucleus and periaqueductal gray84,85,86,87. Brainstem intrinsic connectivity changes will be explored by simple-ROI-by-ROI cross correlation analysis, and emerging focal brainstem effects can be followed up by seed-to-brain analyses.
-
(iii)
Using the short-IST, we investigate if the central cortical mapping of sympathetic-parasympathetic balance – as monitored by the task/rest switches – change over 6 weeks of treatment. Established parametric modulation techniques will be used here to fuse autonomous signals (e.g., heart rate) with the fMRI time series analysis51.
-
(iv)
NM-sensitive imaging: Direct quantification of the LC (and other structures with a NM-positive signal such as the VTA and the substantia nigra) will be used for baseline/follow-up comparisons after adequate preprocessing to evaluate potential differences in noradrenergic or dopaminergic trafficking. To date, it is not known if mid-term effects (follow-up measurement days after the last tVNS/sham stimulation) can be captured using this technique.
Study objectives
The primary hypothesis of our study is that tVNS induces biological and psychophysiological changes in patients with depression, and that the magnitude of these changes is associated with the antidepressant effects of tVNS. All collected data will be used to evaluate whether beneficial tVNS effects (in addition to TAU) can be predicted. Results will be presented on conferences and published in peer-reviewed journals and, if appropriate, on the Max-Planck-Institutes website in plain language for relevant groups (e.g., participants, physicians).
The main objective of the study is therefore to identify neuroimaging and psychophysiological changes associated with tVNS. The study’s secondary objective is the exploratory investigation of individual markers or clusters of clinical, psychometric, and biological markers which may relate to the course of tVNS in depressive patients receiving TAU (multiomics). Moreover, these parameters as well as the course of treatment (e.g. effects and side effects) will be correlated with the tVNS stimulation paradigm, such as current intensity and daily stimulation duration. The collected data will be used to develop predictive models aiming to identify factors associated with beneficial effects of tVNS in patients with depression.
Ethics
The study has been approved by the ethics committee of the Ludwig-Maximilians-University Munich (project registration number: 24–0985). The study is registered in the U.S. National Institute of Health (NIH) clinical study register www.clinicalTrials.gov (ID: NCT07022171; registration date: 16/05/2025). The study was developed and is conducted in accordance with the Declaration of Helsinki and all relevant national and international regulations.
All participants must provide a signed informed consent obtained in person by a trained study physician. Participants are further informed that they can withdraw from the study at any time without consequences or disadvantages for their clinical treatment. Participation in the study is voluntary and not compensated or paid. Protocol modifications will be reviwed by the ethics committee prior to implementation. Protocol and informed consent versions are documented on the respective documents.
Discussion
In summary, the AddVNS study will investigate the change of multimodal biological markers during adjuvant tVNS and the relationship to clinical course and change in depressive symptoms during adjuvant tVNS in patients with MDD. This will be achieved by leveraging the sham-controlled design.
To date, our biological and clinical understanding of tVNS in depression is limited and reliable biomarkers are lacking25. Still, functional MRI studies have already produced promising results: tVNS can modulate the functional connectivity (FC) in the striatum and in the default mode network (DMN) in patients with MDD88,89. Moreover, an increased activity of the left insular cortex was observed in depressed patients receiving auricular tVNS with partial predictive value for treatment success90. It is also worth mentioning that modulation of the locus coeruleus (LC) through tVNS has been shown in patients suffering from migraine91. Despite these promising findings, functional neuroimaging studies still face significant challenges, which are to some extent the result of the specific technical requirements needed to reliably detect activation of brainstem nuclei, such as high spatial resolution or advanced postprocessing methods25,92. To address this issue, we have incorporated an NM-sensitive sequence into our MRI protocol, which enables a reliable visualization of the LC, along with brainstem-sensitive fMRI-BOLD sequences. This approach overlaps with recommendations regarding the utilization of fMRI in tVNS trials25. Another novel aspect of the MRI protocol used here is the inclusion of two fMRI tasks that allow for insights into depression-circuit specific effects of tVNS. First, an established monetary incentive delay task by its VTA and ventral striatum / nucleus accumbens activation provides a functional readout of reward anticipation processes that are disturbed in MDD93. Novel results from high resolution imaging suggest a closer convolution between the LC-NE-system (also see below) and the substantia nigra/VTA system than long assumed94. Further, the task produces robust default mode deactivation and salience network activation, interlinked with pupil responses, that can be analyzed as previously reported in healthy subjects and MDD patients39,40,95. Second, we employ a short version of an imaging stress test (short-IST) to calculate individual maps of the central/peripheral ANS interaction. Using the full version of stress test, ANS responses modulated BOLD signals in areas of the default mode network and salience network (including the insula), but also in hubs of stress response regulation such as the anterior hippocampus and amygdala51. The shorter version used here is also explored because of its translatability to clinical routine protocols.
The LC is a brainstem nucleus that serves as the primary source of noradrenaline (NE) in the brain96. The LC-NE system is relevant for a variety of psychiatric and neurological disorders, such as Parkinson’s disease97,98, Alzheimer’s disease98 and depression99. Since the ABNV projects to the Nucleus tractus solitarius (NTS), which in turn projects to the LC and many other brain regions including amygdala and insula, the NTS and LC are considered main target sites of tVNS16. Pupillometry is a precise and sensitive measurement method for mapping the neuronal activity of the LC100. However, studies on the effects of tVNS on pupil alteration have so far yielded heterogeneous results and focused on healthy individuals101,102,103. AddVNS is, to the best of our knowledge, among the first studies that examine the effects of 6 weeks of thrice daily tVNS on pupil dilation dynamics in depressed patients. Besides pupillometry, the psychophysiological assessment during the AddVNS study also includes heart rate variability, which is viewed as a biomarker candidate for tVNS101, and the evaluation of gastric mobility using an electrogastrogram. The latter represents a potentially relevant parameter for VNS in general, due to the vagus nerve’s intense innervation of the stomach. However, it has not yet been utilized in the context of tVNS in depression.
Although the identification of psychophysiological and imaging biomarkers for tVNS is the main goal of the current study, other biomarker candidates, with a specific focus on blood-based multiomics will be analyzed. The bidirectional relationship between depression and inflammation has been well established104, with studies suggesting that approximately 30% of depressive patients show mild signs of systemic inflammation105,106. At the same time, animal studies have shown that the vagus nerve exhibits an anti-inflammatory function as part of the cholinergic anti-inflammatory pathway (CAP)107. Nevertheless, two recent meta-analyses have found no clear indication for the anti-inflammatory effect of VNS in humans30,108. A major limiting factor of these findings is the great heterogeneity of the reviewed and analyzed studies, particularly regarding patient populations and control conditions108. The above-mentioned meta-analyses also did not include studies utilizing tVNS in depression30,108. Thus, the effects of tVNS on systemic inflammation in depression should be considered undefined, for the time being. Here, the AddVNS study may help bridge this knowledge gap. Moreover, the multiomics approach includes the analysis of both purinergic signaling pathways and neural cell-derived exosomes. These parameters have been repeatedly linked to neuropsychiatric disorders including depression and course of disease and are therefore emerging biomarker candidates109,110,111,112,113. They have, however, not been examined in the context of tVNS in depression. The latter also applies to gut microbiome. The vagus nerve is a prominent part of the microbiota-gut-brain axis, which is more and more considered to play an important role in the pathogenesis of depressive disorders114. Many mechanisms, through which the microbiota-gut-brain axis can modulate the onset and course of depression, have been proposed, such as immunomodulation, modulation of the HPA axis and modulation of neurotransmitters28,115. Nevertheless, the specific neuronal networks involved in the microbiota-gut-brain axis as well as the exact mechanisms of interaction between the vagus nerve, the microbiota and the immune system remain to be elucidated115,116. The AddVNS study is, to the extent of our knowledge, the first study to examine the effects of tVNS on the gut microbiome of depressive patients.
Another strength of the presented study is the detailed documentation of the tVNS procedure, including stimulation parameters such as total stimulation intensity, duration, and cumulative electrical charge delivered along with possible adverse events. This allows us to overcome a key drawback of earlier studies, which inconsistently reported tVNS stimulation parameters and side effects17,24,25,101. Furthermore, in contrast to our study, many investigations of the biological mechanisms or potential biomarkers of tVNS have examined healthy individuals or lacked a valid control group101. Even when a control condition was included, many studies likely suffered from functional unblinding. We aim to circumvent the latter by implementing an elaborate blinding procedure including a sham tVNS electrode indistinguishable from the real one as well as a block-wise randomization strategy to minimize the risk of participants discussing the physical sensations experienced during stimulation across treatment groups. Creating an appropriate sham tVNS protocol is a noted challenge92 and does apply to our as well as all other tVNS studies.
The AddVNS study may advance our understanding of the biological effects of tVNS in depression. Ultimately, data and results will determine the extent to which AddVNS can translate into clinically meaningful benefits, guide personalized treatment strategies, and inform future large-scale trials.
Data availability
The datasets used and/or analyzed during the current study will be made available from the corresponding authors upon reasonable request, contingent on participants informed-consent approval for respective data sharing and only in compliance with the applicable regulations.
References
WHO. Depression and Other Common Mental Disorders: Global Health Estimates. Licence: CC BY-NC-SA 3.0 IGO, (2017).
Spencer, J. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392 (10159), 1789–1858 (2018).
Jacobi, F. et al. Psychische Störungen in der Allgemeinbevölkerung. Der Nervenarzt. 85 (1), 77–87 (2014).
Steffen, A. et al. Mental and somatic comorbidity of depression: a comprehensive cross-sectional analysis of 202 diagnosis groups using German nationwide ambulatory claims data. BMC Psychiatry. 20 (1), 142 (2020).
Kessler, R. The costs of depression. Psychiatr. Clin. North Am. 35, 1–14 (2012).
Cai, H. et al. Prevalence of suicidality in major depressive disorder: a systematic review and meta-analysis of comparative studies. Front. Psychiatry. 12, 690130 (2021).
König, H., König, H. H. & Konnopka, A. The excess costs of depression: a systematic review and meta-analysis. Epidemiol. Psychiatric Sci. 29, e30 (2020).
Greenberg, P. et al. The economic burden of adults with major depressive disorder in the United States (2019). Adv. Ther. 40 (10), 4460–4479 (2023).
McIntyre, R. S. et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry. 22 (3), 394–412 (2023).
Kraus, C. et al. Prognosis and improved outcomes in major depression: a review. Transl. Psychiatry. 9 (1), 127 (2019).
Bundesärztekammer, K. B. & Fachgesellschaften, A. W. M. Nationale VersorgungsLeitlinie - Unipolare Depression [Langfassung]. 2022, ÄZQ – Redaktion Nationale VersorgungsLeitlinien. p. AWMF-Register-Nr. nvl-005 (2025).
Fetzer, S. et al. A systematic review of magnetic resonance imaging in patients with an implanted vagus nerve stimulation system. Neuroradiology 63 (9), 1407–1417 (2021).
Reif-Leonhard, C. et al. Vagus nerve stimulation for difficult to treat depression. Nervenarzt 93 (9), 921–930 (2022).
Milev, R. V. et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 4. neurostimulation treatments. Can. J. Psychiatry. 61 (9), 561–575 (2016).
Kim, A. Y. et al. Safety of transcutaneous auricular vagus nerve stimulation (taVNS): a systematic review and meta-analysis. Sci. Rep. 12 (1), 22055 (2022).
Butt, M. F. et al. The anatomical basis for transcutaneous auricular vagus nerve stimulation. J. Anat. 236 (4), 588–611 (2020).
Gerges, A. N. H. et al. Clinical application of transcutaneous auricular vagus nerve stimulation: a scoping review. Disabil. Rehabil 2024, 1–31 (2024).
Rong, P. et al. Effect of transcutaneous auricular vagus nerve stimulation on major depressive disorder: a nonrandomized controlled pilot study. J. Affect. Disord. 195, 172–179 (2016).
Li, S. et al. Comparative effectiveness of transcutaneous auricular vagus nerve stimulation vs citalopram for major depressive disorder: a randomized trial. Neuromodulation 25 (3), 450–460 (2022).
Deligiannidis, K. M. et al. Effect of transcutaneous auricular vagus nerve stimulation on major depressive disorder with peripartum onset: a multicenter, open-label, controlled proof-of-concept clinical trial (DELOS-1). J. Affect. Disord. 316, 34–41 (2022).
Evensen, K. et al. Transcutaneous vagal nerve stimulation in treatment-resistant depression: a feasibility study. Neuromodulation 25 (3), 443–449 (2022).
Wu, C. et al. Transcutaneous auricular vagus nerve stimulation in treating major depressive disorder: a systematic review and meta-analysis. Med. (Baltim). 97 (52), e13845 (2018).
Tan, C. et al. The efficacy and safety of transcutaneous auricular vagus nerve stimulation in the treatment of depressive disorder: a systematic review and meta-analysis of randomized controlled trials. J. Affect. Disord. 337, 37–49 (2023).
Redgrave, J. et al. Safety and tolerability of Transcutaneous Vagus Nerve stimulation in humans; a systematic review. Brain Stimul. 11 (6), 1225–1238 (2018).
Farmer, A. D. et al. International consensus based review and recommendations for minimum reporting standards in research on transcutaneous vagus nerve stimulation (Version 2020). Front. Hum. Neurosci. 14, 568051 (2020).
Parente, J. et al. Neural, anti-inflammatory, and clinical effects of transauricular vagus nerve stimulation in major depressive disorder: a systematic review. Int. J. Neuropsychopharmacol. 27, 3 (2024).
Austelle, C. W. et al. A comprehensive review of vagus nerve stimulation for depression. Neuromodulation 25 (3), 309–315 (2022).
Liu, C. H. et al. Neural networks and the anti-inflammatory effect of transcutaneous auricular vagus nerve stimulation in depression. J. Neuroinflamm. 17 (1), 54 (2020).
Rosso, P. et al. Vagus nerve stimulation and neurotrophins: a biological psychiatric perspective. Neurosci. Biobehav Rev. 113, 338–353 (2020).
de Melo, P. S. et al. A mechanistic analysis of the neural modulation of the inflammatory system through vagus nerve stimulation: a systematic review and meta-analysis. Neuromodulation (2024).
Grimonprez, A. et al. The antidepressant mechanism of action of vagus nerve stimulation: evidence from preclinical studies. Neurosci. Biobehav. Rev. 56, 26–34 (2015).
Carreno, F. R. & Frazer, A. Vagal nerve stimulation for treatment-resistant depression. Neurotherapeutics 14 (3), 716–727 (2017).
Wang, Y. et al. Vagus nerve stimulation in brain diseases: therapeutic applications and biological mechanisms. Neurosci. Biobehav. Rev. 127, 37–53 (2021).
Berger, V. W. et al. A roadmap to using randomization in clinical trials. BMC Med. Res. Methodol. 21 (1), 168 (2021).
Hein, E. et al. Auricular transcutaneous electrical nerve stimulation in depressed patients: a randomized controlled pilot study. J. Neural Transm. (Vienna) 120 (5), 821–827 (2013).
Peuker, E. T. & Filler, T. J. The nerve supply of the human auricle. Clin. Anat. 15 (1), 35–37 (2002).
Dolphin, H. et al. "The Wandering Nerve Linking Heart and Mind" - the complementary role of transcutaneous vagus nerve stimulation in modulating neuro-cardiovascular and cognitive performance. Front. Neurosci. 16, 897303 (2022).
Gilmour, G. et al. Relating constructs of attention and working memory to social withdrawal in Alzheimer’s disease and schizophrenia: issues regarding paradigm selection. Neurosci. Biobehav. Rev. 97, 47–69 (2019).
Schneider, M. et al. Disentangling reward anticipation with simultaneous pupillometry / fMRI. Neuroimage 178, 11–22 (2018).
Brendler, A. et al. Assessing hypo-arousal during reward anticipation with pupillometry in patients with major depressive disorder: replication and correlations with anhedonia. Sci. Rep. 14 (1), 344 (2024).
Fietz, J. et al.Data-Driven pupil response profiles as transdiagnostic readouts for the detection of neurocognitive functioning in affective and anxiety disorders. Biol. Psychiatry Cogn. Neurosci. Neuroimaging. 9 (6), 580–587 (2024).
Levine, M. E. et al. Gastrointestinal ssystem. In Handbook of Psychophysiology (eds. Cacioppo, J. T. et al.) 258–283 (Cambridge University Press, 2016).
Brückl, T. M. et al. The biological classification of mental disorders (BeCOME) study: a protocol for an observational deep-phenotyping study for the identification of biological subtypes. BMC Psychiatry. 20 (1), 213 (2020).
Trujillo, P., Aumann, M. A. & Claassen, D. O. Neuromelanin-sensitive MRI as a promising biomarker of catecholamine function. Brain 147 (2), 337–351 (2024).
Reneman, L. et al. Imaging of the dopamine system with focus on pharmacological MRI and neuromelanin imaging. Eur. J. Radiol. 140, 109752 (2021).
Langley, J. et al. Reproducibility of locus coeruleus and substantia nigra imaging with neuromelanin sensitive MRI. MAGMA 30 (2), 121–125 (2017).
Chen, X. et al. Simultaneous imaging of locus coeruleus and substantia nigra with a quantitative neuromelanin MRI approach. Magn. Reson. Imaging. 32 (10), 1301–1306 (2014).
Mohamed, A. Z. et al. Functional MRI of the brainstem for assessing its autonomic functions: from imaging parameters and analysis to functional Atlas. J. Magn. Reson. Imaging (2024).
Schneider, M. et al. Pupil dilation during reward anticipation is correlated to depressive symptom load in patients with major depressive disorder. Brain Sci. 10, 12 (2020).
Elbau, I. G. et al. The brain’s hemodynamic response function rapidly changes under acute psychosocial stress in association with genetic and endocrine stress response markers. Proc. Natl. Acad. Sci. U S A. 115 (43), E10206–e10215 (2018).
Erhart, M. et al. Capturing inter-individual variability in stress dynamics with heart rate traces reveals activity in the bilateral hippocampus, amygdala, and insula. Imaging Neurosci. (Camb) 2, 256 (2024).
von Mucke-Heim, I. A. et al. Multiomics and blood-based biomarkers of electroconvulsive therapy in severe and treatment-resistant depression: study protocol of the DetECT study. Eur. Arch. Psychiatry Clin. Neurosci. 274 (3), 673–684 (2024).
Löwe, B., Zipfel, S. R. & Herzog, S. W, Gesundheitsfragebogen für Patienten (PHQ D). Komplettversion und Kurzform. Testmappe mit Manual (Pfizer, 2002).
Levis, B., Benedetti, A. & Thombs, B. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ 365, l1476 (2019).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16 (9), 606–613 (2001).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom. Med. 64 (2), 258–266 (2002).
Beck, A. T. & Brown, S. R. Beck depressions-inventar. 2 Auflage, in M Hautzinger, FK Kühner, editor, BDI-II; Revision; Manual. 2009, PSychCorp / Pearsons Assessment (Frankfurt, 2009).
Snaith, R. P. et al. A scale for the assessment of hedonic tone the Snaith-Hamilton Pleasure Scale. Br. J. Psychiatry. 167 (1), 99–103 (1995).
Franz, M. et al. German version of the Snaith-Hamilton-Pleasure Scale (SHAPS-D). Anhedonia in schizophrenic and depressive patients. Fortschr. Neurol. Psychiatr. 66 (9), 407–413 (1998).
Beblo, T. et al. Entwicklung eines Fragebogens zur subjektiven Einschätzung der geistigen Leistungsfähigkeit (FLei) bei Patienten mit psychischen Störungen. Z. für Neuropsychol. 21 (3), 143–151 (2010).
Downey, G. & Feldman, S. I. Implications of rejection sensitivity for intimate relationships. J. Pers. Soc. Psychol. 70 (6), 1327–1343 (1996).
Staebler, K. et al. Rejection sensitivity and borderline personality disorder. Clin. Psychol. Psychother. 18 (4), 275–283 (2011).
Üstün, T. et al. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0 (World Health Organization, 2010).
Montgomery, S. A. & Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry. 134, 382–389 (1979).
Schmidtke, A. et al. [Studies of the reliability and validity of the German version of the Montgomery-Asberg Depression Rating Scale (MADRS)]. Schweiz. Arch. Neurol. Psychiatr (1985). 139 (2), 51–65 (1988).
Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry. 23 (1), 56–62 (1960).
Zimmerman, M. et al. Severity classification on the Hamilton Depression Rating Scale. J. Affect. Disord.. 150 (2), 384–388 (2013).
Schmitt, A., Kulzer, B. & Hermanns, N. German version of the GRID Hamilton Rating Scale for Depression (GRID-HAMD). (2015).
Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 32 (1), 50–55 (1959).
Aas, I. H. M. Guidelines for rating Global Assessment of Functioning (GAF). Ann. Gen. Psychiatry. 10 (1), 2 (2011).
Aas, I. H. M., Sonesson, O. & Torp, S. A qualitative study of clinicians experience with rating of the global assessment of functioning (GAF) scale. Commun. Ment. Health J. 54 (1), 107–116 (2018).
Aschenbrenner, S. et al. Wiener Testsystem: Testset Kognitive Basistestung (CogBat) (Schuhfried, 2012).
Lehrl, S. Mehrfachwahl-Wortschatz-Intelligenztest MWT-B (Spitta, 2005).
Balzer, C. et al. Materialien und Normwerte für die neuropsychologische Diagnostik MNND (Normdaten, 2011).
Zimmermann, J. et al. Maladaptive Persönlichkeitseigenschaften gemäß DSM-5. PTT - Persönlichkeitsstörungen: Theorie und Therapie 2014, 46–58 (2014).
Zimmermann, J. et al. The structure and correlates of self-reported DSM-5 maladaptive personality traits: findings from two German-speaking samples. J. Pers. Disord. 28 (4), 518–540 (2014).
Spitzer, C. et al. The German version of the level of personality functioning scale-brief form 2.0 (LPFS-BF): latent structure, convergent validity and norm values in the general population. Psychother. Psychosom. Med. Psychol. 71 (7), p284–293 (2021).
Lopizzo, N. et al. Gene–environment interaction in major depression: focus on experience-dependent biological systems. Front. Psychiatry 6, 68 (2015).
Leon, A. C., Davis, L. L. & Kraemer, H. C. The role and interpretation of pilot studies in clinical research. J. Psychiatr. Res. 45 (5), 626–629 (2011).
Blainey, P., Krzywinski, M. & Altman, N. Replication. Nat. Methods 11 (9), 879–880 (2014).
Friede, T. & Kieser, M. Sample size recalculation in internal pilot study designs: a review. Biom. J. 48 (4), 537–555 (2006).
Wittes, J. & Brittain, E. The role of internal pilot studies in increasing the efficiency of clinical trials. Stat. Med. 9 (1–2), 65–71 (1990). discussion 71 – 2.
Faul, F. et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods. 39 (2), 175–191 (2007).
Kraus, T. et al. CNS BOLD fMRI effects of sham-controlled transcutaneous electrical nerve stimulation in the left outer auditory canal - a pilot study. Brain Stimul. 6 (5), 798–804 (2013).
Borgmann, D. et al. Technical Note: modulation of fMRI brainstem responses by transcutaneous vagus nerve stimulation. Neuroimage 244, 118566 (2021).
Sclocco, R. et al. The influence of respiration on brainstem and cardiovagal response to auricular vagus nerve stimulation: a multimodal ultrahigh-field (7T) fMRI study. Brain Stimul. 12 (4), 911–921 (2019).
Sclocco, R. et al. Stimulus frequency modulates brainstem response to respiratory-gated transcutaneous auricular vagus nerve stimulation. Brain Stimul. 13 (4), 970–978 (2020).
Zhang, S. et al. Prolonged longitudinal transcutaneous auricular vagus nerve stimulation effect on striatal functional connectivity in patients with major depressive disorder. Brain Sci. 12, 12 (2022).
Sun, J. et al. Immediate modulatory effects of transcutaneous auricular vagus nerve stimulation on the resting state of major depressive disorder. J. Affect. Disord. 325, 513–521 (2023).
Fang, J. et al. Early cortical biomarkers of longitudinal transcutaneous vagus nerve stimulation treatment success in depression. Neuroimage Clin. 14, 105–111 (2017).
Zhang, Y. et al. Transcutaneous auricular vagus nerve stimulation at 1 Hz modulates locus coeruleus activity and resting state functional connectivity in patients with migraine: an fMRI study. Neuroimage Clin. 24, 101971 (2019).
Ludwig, M. et al. Current challenges in reliably targeting the noradrenergic locus coeruleus using transcutaneous auricular vagus nerve stimulation (taVNS). Auton. Neurosci. 236, 102900 (2021).
Geugies, H. et al. Decreased reward circuit connectivity during reward anticipation in major depression. Neuroimage Clin. 36, 103226 (2022).
Hall, J. M., Shahnazian, D. & Krebs, R. M. Exploring distinct and joint contributions of the locus coeruleus and the substantia nigra/ventral tegmental area complex to reward and valence processing using high-resolution fMRI. Imaging Neurosci. (Camb.) (2024).
Schneider, M. et al. Spontaneous pupil dilations during the resting state are associated with activation of the salience network. Neuroimage 139, 189–201 (2016).
Poe, G. R. et al. Locus coeruleus: a new look at the blue spot. Nat. Rev. Neurosci. 21 (11), 644–659 (2020).
Bari, B. A., Chokshi, V. & Schmidt, K. Locus coeruleus-norepinephrine: basic functions and insights into Parkinson’s disease. Neural Regen. Res. 15 (6), 1006–1013 (2020).
Krohn, F. et al. Noradrenergic neuromodulation in ageing and disease. Neurosci. Biobehav. Rev. 152, 105311 (2023).
Bernard, R. et al. Altered expression of glutamate signaling, growth factor, and glia genes in the locus coeruleus of patients with major depression. Mol. Psychiatry. 16 (6), 634–646 (2011).
Viglione, A., Mazziotti, R. & Pizzorusso, T. From pupil to the brain: new insights for studying cortical plasticity through pupillometry. Front. Neural Circuits. 17, 1151847 (2023).
Burger, A. M. et al. Moving beyond belief: a narrative review of potential biomarkers for transcutaneous vagus nerve stimulation. Psychophysiology 57 (6), e13571 (2020).
Capone, F. et al. The effects of transcutaneous auricular vagal nerve stimulation on pupil size. Clin. Neurophysiol. 132 (8), 1859–1865 (2021).
Lloyd, B. et al. Short-term transcutaneous vagus nerve stimulation increases pupil size but does not affect EEG alpha power: a replication of Sharon et al. (2021, Journal of Neuroscience). Brain Stimul. 16 (4), 1001–1008 (2023).
Beurel, E., Toups, M. & Nemeroff, C. B. The bidirectional relationship of depression and inflammation: double trouble. Neuron 107 (2), 234–256 (2020).
Raison, C. L. & Miller, A. H. Is depression an inflammatory disorder? Curr. Psychiatry Rep. 13 (6), 467–475 (2011).
Nobis, A., Zalewski, D. & Waszkiewicz, N. Peripheral markers of depression. J. Clin. Med. 9 (12), 3793 (2020).
Kelly, M. J. et al. Manipulation of the inflammatory reflex as a therapeutic strategy. Cell. Rep. Med. 3 (7), 100696 (2022).
Schiweck, C. et al. No consistent evidence for the anti-inflammatory effect of vagus nerve stimulation in humans: a systematic review and meta-analysis. Brain Behav. Immun. 116, 237–258 (2024).
Bartoli, F. et al. Purinergic signaling and related biomarkers in depression. Brain Sci. 10 (3), 160 (2020).
von Mucke-Heim, I. A. & Deussing, J. M. The P2X7 receptor in mood disorders: emerging target in immunopsychiatry, from bench to bedside. Neuropharmacology 224, 109366 (2023).
Bhatt, S. et al. Exosomes: a novel therapeutic paradigm for the treatment of depression. Curr. Drug Targets. 22 (2), 183–191 (2021).
Shetgaonkar, G. G. et al. Exosomes as cell-derivative carriers in the diagnosis and treatment of central nervous system diseases. Drug Deliv. Transl. Res. 12 (5), 1047–1079 (2022).
Saeedi, S. et al. The emerging role of exosomes in mental disorders. In Translational Psychiatry 1–11 (Nature Publishing Group, 2019).
Chang, L., Wei, Y. & Hashimoto, K. Brain-gut-microbiota axis in depression: a historical overview and future directions. Brain Res. Bull. 182, 44–56 (2022).
Cryan, J. F. et al. The microbiota-gut-brain axis. Physiol. Rev. 99 (4), 1877–2013 (2019).
Bonaz, B., Bazin, T. & Pellissier, S. The vagus nerve at the interface of the microbiota-gut-brain axis. Front. Neurosci. 12, 49 (2018).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
EK and I-AMH wrote the manuscript text. I-AMH prepared the figure. EK, I-AMH, JP, NG, AE, PGS, VS, NG, EBB, and PF contributed to the study conception, hypothesis generation, measure selection, and study design. NG, EBB, and PF provided constant scientific support and supervised the study development and manuscript drafting. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
EK nothing to disclose. I-AMH nothing to disclose. JP nothing to disclose. NG nothing to disclose. AE nothing to disclose. PGS nothing to disclose. VS: patent applications PCT/EP2024/071376 and PCT/EP2024/071377, consultancy for Roche, Sony, Boehringer-Ingelheim, co-founder of Biomentric UG (entrepreneurial company), equity in Biomentric UG. EB nothing to disclose. NG nothing to disclose. PF gives payed talks and is partly a member of the advisory board at BMS, Richter, Johnson and Johnson and Otsuka.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kokolakis, E., von Mücke-Heim, IA., Pape, J.C. et al. Protocol of the randomized double blind sham controlled AddVNS study of transcutaneous vagus nerve stimulation mechanisms in depression. Sci Rep 16, 8149 (2026). https://doi.org/10.1038/s41598-026-42459-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-42459-2
