
Abstract
According to the phospholipid membrane theory of psychotic disorders, fatty acid metabolism may play a role in the etiopathogenesis of schizophrenia (SCH) and related disorders. Weakened skin reactions to niacin have been documented in SCH and bipolar disorder (BD), prompting research into biomarkers underlying these responses. So far, there is also no standard for performing and interpreting the niacin skin flush test (NSFT) which creates an opportunity for development in this area. The NSFT was conducted based on the SKINREMS system and an original method of analyzing measurements. 120 individuals including 33 patients diagnosed with first-episode psychosis (FEP), 22 with BD, 13 with schizoaffective disorder (SA), 13 with chronic schizophrenia (CS), and 39 healthy controls (HC) participated in the study. NSFT differentiated patients from HC and among subgroups of patients based on color saturation, specific time points, and niacin solution concentrations. The NSFT is a fast, effective, and cheap method that allows the differentiation of individuals suffering from psychotic disorders from HC. Standardization of the test method may contribute to more precise searches for biomarkers responsible of responses in the NSFT and can support the diagnostic process. The presented study is preliminary and exploratory in nature. Developing a method of using NSFT may contribute to a more precise search for biomarkers responsible for the results and thus to the diagnostic process.
Similar content being viewed by others


Introduction
Nicotinic acid, an organic compound, an essential human nutrient, otherwise known as a water-soluble vitamin B, contributes to the production of prostaglandins, thereby causing skin flushing when applied to the skin or taken orally1. The reaction was discovered in 1959 by Thomas W. Murrell and William M. Taylor who initiated attempts to delve into its causes by subsequent researchers such as Abram Hoffer, Paul Fiedler, and David Horrobin2,3,4,5. There is extensive scientific evidence that in psychotic disorders, the skin response to niacin is negligible or significantly weakened6,7,8. There are many assumptions as to what exactly can lead to a weak skin reaction in response to the NSFT, including increased activity of phospholipase A2, altered expression of prostaglandin or niacin receptors, reduced arachidonic acid reserves, impaired phospholipid metabolism or impaired capillary wall motility9. Studies using the NSFT test have been conducted not only in the case of SCH, FEP, BD, or major depression, but also in other neuropsychiatric diseases such as autism, social phobia, dyslexia, or Huntington’s disease10,11,12,13. So far, many studies have been conducted using the NSFT, especially engaging patients suffering from SCH. In the 1970s, the phenomenon of a weakened or absent response to niacin in patients was mainly interpreted as a deficit of prostaglandin synthesis, which entailed the NSFT itself as an objective diagnostic biochemical parameter proposed by David Horrobin14. These conclusions provided the basis for the formulation of the membrane phospholipid hypothesis of SCH15.
As psychotic disorders include not only SCH but also BD and SA, it is worth noting that SA is used in clinical practice as an intermediate condition with a clinical manifestation of both psychosis and mood instability. Such a smooth division of diagnosis should probably be also reflected in the color spectrum results obtained in the NSFT. Regarding the reactions’ spectrum obtained, there are also studies that examined correlations between the intensity of symptoms and sensitivity to the NSFT test using various clinical scales, such as the PANSS scale, i.e. the study by Smesny et al. confirmed the assumptions regarding the intensity of symptoms and the redness of skin in the NSFT, which is a very interesting direction to develop in the context of the diversity of reactions occurring16. Over the years, the NSFT has been performed in many different ways. The interpretation of skin reaction was considered by thermal, optical, as well as blood flow and optical spectroscopy change measurements17,18,19,20.
Still, no standard has been established for performing the NSFT, which creates a space for development and attempts to standardize the method by various teams of researchers.
In this article, we would like to present preliminary study focused on the differentiation of patients diagnosed with FEP, CS, SA and BD using the SKINREMS system. The system was created by a multidisciplinary team of researchers from the 1st Department of Psychiatry, Psychotherapy and Early Intervention in Lublin and the Lublin University of Technology as a simple, easy-to-use, repeatable, portable, and economical device for performing the NSFT, along with an original method of analyzing the measurements taken. The analysis of the results obtained in the study is based on the C&RT algorithm to enhance differentiation between patients with FEP, CS, SA, and BD, and HC.
Results
Results of C&RT analysis between patients with specific DSM-5 diagnoses and the HC
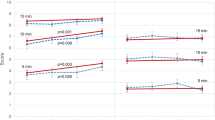
The results of the C&RT analysis are presented in Figs. 1, 2, 3, 4 and 5. We performed analyses to distinguish various patient samples from HC, considering the following groups: FEP, BD, SA, and CS patients. All C&RT analyses performed in the study revealed that the 0.1 M niacin concentration was the group-differentiating factor in each combination. Figure 5 presents a summary tree differentiating the group of patients from HC.
FEP patients vs. HC
The C&RT analysis showed two differentiating variables: Gmean_3_A and Bmean_6_A. After 2.5 min, an average green color less than or equal to 12.53 distinguished FEP patients from HC. As the test continued, after 5.5 min, an average blue color less than or equal to 23.24 further separated the FEP sample from HC. The ROC value was 0.80, which suggests a good ability to differentiate these groups (Fig. 1).

C&RT analysis for FEP and HC, B-blue; G-green; 3-measurement after 2.5-minutes; 6-measurement after 5.5-minutes; A-niacin concentration = 0.1 M.
CS patients vs. HC
The group consisted of CS individuals (more than five years diagnosed with SCH according to DSM-5). C&RT analysis showed three combinations of differentiating variables: Bmean_6_A, Rmedian_3_A, and Bmedian _3_A. After 5.5-minutes the average blue color less than or equal to 4.19 differentiated CS patients from the HC. HC were also differentiated by the median red color equal to or below 20.50 after only 2.5-minutes of performing the test. At the same time, the median blue color value below or equal to 25.50 distinguished the HC from the patients. The ROC value of 0.90 suggests excellent differentiation ability (Fig. 2).

C&RT analysis for CS and HC, B-blue; R-red, 3-measurement after 2.5-minutes; 6-measurement after 5.5-minutes; A-niacin concentration = 0.1 M.
SA patients vs. HC
C&RT analysis showed that the mean green color intensity less than or equal to 3.20 after 3.5-minutes distinguished the SA from the HC group. After 3.5-minutes the median blue color less than or equal to 13.5 also discerned the group further. The ROC value was equal to 0.79 suggests a fair differentiation ability (Fig. 3).

C&RT for SA and HC, G-green; B-blue; 4-measurement after 3.5-minutes; A-niacin concentration = 0.1 M.
BD patients vs. HC
C&RT analysis also identified an average green color of less than or equal to 6.02, which differentiated BD patients from the HC after 3.5-minutes. The ROC value was equal to 0.64 suggests a poor differentiation ability (Fig. 4).

C&RT analysis for BD and HC, G-green; 4-measurement after 3.5-minutes; A-niacin concentration = 0.1 M.
C&RT analysis summarizing the differentiation between patients and HC without disease entities division
RGB was the model differentiating in the study, as opposed to the HSV, which was also analyzed. The most differentiating were the measurements after 2.5, 3.5, 4.5, and 5.5-minutes. Additionally, measurements within the concentration of 0.1 M were significant, compared to 0.01 M and 0.001 M, which were also performed. The ROC value for differentiating BD patients is equal to 0.88 and suggests a good differentiation ability (Fig. 5).

C&RT for the whole group of patients (PD) and HC without disease entities division, G-green; B-blue; R-red; 3-measurement after 2.5-minutes; 4-measurement after 3.5-minutes; 5-measurement after 4.5-minutes; 6-measurement after 5.5-minutes; A-niacin concentration = 0.1 M.
Results of C&RT analysis between patients with specific DSM-5 diagnoses
The results of the C&RT analysis are presented in Figs. 6, 7 and 8. We performed analyses to distinguish various patient samples with specific DSM-5 diagnoses from each other.
FEP patients vs. CS patients
C&RT analysis showed that the average green color less than or equal to 26.65 after 2.5-minutes of the test, and the blue color less than or equal to 3.34 after 5.5 min, which differentiated the groups. The ROC value of 0.86 suggests a good differentiation ability (Fig. 6).

C&RT analysis for FEP and CS patients, B-blue; G-green; 3-measurement after 2.5-minutes; 6-measurement after 5.5-minutes; A-niacin concentration = 0.1 M.
SA patients vs. CS patients
C&RT analysis showed the mean green saturation of less than or equal to 36.77 after 2.5 min differentiated these two groups. Further, the mean blue saturation of less than or equal to 16.80 and the mean green color less than or equal to 22.94 after 5.5 min also discriminates individuals in this group. The ROC was equal to 0.89 suggest a good differentiation ability (Fig. 7).

C&RT analysis for SA and CS patients, B-blue; G-green; 3-measurement after 2.5-minutes; 5-measurement after 4.5-minutes; 6-measurement after 5.5-minutes; A-niacin concentration = 0.1 M.
BD patients vs. SA patients
C&RT analysis showed that after 2.5-minutes, the group was differentiated by the maximum saturation of green color. After 3.5 and later 5.5-minutes patients were differentiated by the mean and median saturation of green color. The ROC value of 0.80 suggests a good differentiation ability (Fig. 8).

C&RT analysis for BD and SA patients, G-green; 3-measurement after 2.5-minutes; 4-measurement after 3.5-minutes; 5-measurement after 4.5-minutes; A-niacin concentration = 0.1 M.
Below we present a summary in Table 1 that includes the results discussed above.
Discussion
The aim of the study was to verify that NSFT based on the SKINREMS method and the author’s original analysis of the results would differentiate the group of patients from the HC. Conclusions should be drawn here regarding the observation of the study methodology itself. Firstly, as regards the concentrations of niacin used in the NSFT, the only differentiating concentration for all comparisons was the concentration of 0.1 M. Secondly, NSFT in our study performance lasted 15-minutes. What is significant, the C&RT analysis showed that the most diagnostic measurements were those lasting from 2.5-minutes to 5.5-minutes of the NSFT. Moreover, in the RGB color analysis, the most differentiating colors were green and blue. Only in the case of CS patients did the saturation of the red color differentiate the group from the HC. Importantly, in each case of differentiating patients from the HC, we must take into account the combination of these three variables, i.e. niacin concentration, time, and color. In our study, no clear influence of the following parameters: age, gender, presence of chronic disease, family history of mental health problems, BMI, physical activity, or tobacco smoking on group stratification in NSFT was observed.
Since there is still no standard for NSFT, there are many reports that show a variety of study results21,22. There are also scientific reports about recurrent unipolar depressive disorder and NSFT23. Many studies also differ in the time to perform the NSFT24,25. Some reports are consistent with our study regarding the most reliable concentration for differentiating patients from HC26. Although from 1986, there is also scientific evidence stating that NSFT is not diagnostic for SCH27.
The phenomenon in which the green and blue channels demonstrate higher predictive value than the red channel in differentiating erythematous responses in NSFT can be explained by both biological mechanisms and image-analysis methodology. Although erythema is classically associated with an increase in the red component, digital colorimetric analysis enables detection of subtle hemodynamic changes that do not necessarily manifest as intense visible redness.
From a biological perspective, the spectral absorption characteristics of hemoglobin play a key role28,29. Oxyhemoglobin (HbO₂) exhibits two principal absorption maxima: in the range of 415–425 nm (blue light) and 540–580 nm (green–yellow light), whereas deoxyhemoglobin (Hb) shows increased absorption around approximately 555 nm and reduced absorption in the blue range30,31,32,33. Variations in capillary blood oxygenation within the superficial layers of the skin, occurring in response to the inflammatory stimulus induced by niacin, may lead to shifts in light absorption and reflectance that are detected earliest and most distinctly in the green and blue channels. This effect is particularly relevant in the initial phases of the reaction, when microvascular alterations and oxygenation shifts are not yet visible to the naked eye as erythema. Moreover, red light (with a longer wavelength) penetrates deeper skin layers and undergoes greater scattering, resulting in lower contrast between the reaction area and surrounding tissue, as well as a higher risk of digital signal saturation in cases of strong inflammatory responses34.
From a methodological standpoint, the green and blue channels provide a broader dynamic range and higher sensitivity to minor changes in blood perfusion and oxygenation within superficial skin layers. In the red channel, an intense vascular response may lead to digital signal saturation, thereby limiting the ability to differentiate between response levels, which was clearly observed during the experiment. At the same time, temporal variability of green and blue channel intensities enables capture of earlier and more subtle stages of the skin response that may have diagnostic relevance before the development of fully expressed erythema. The application of differential color analysis relative to control regions (skin not exposed to niacin) reduced the influence of individual pigmentation and lighting conditions, further improving the precision of change detection in these channels. These mechanisms confirm that the green and blue channels provide more informative signals regarding the vascular and metabolic response of the skin than the red channel, particularly in the context of early and moderate reactions. Consequently, their higher predictive value in NSFT analysis is not inconsistent with the physiology of erythema, but rather complements it by highlighting the need to consider the full spectrum of colorimetric changes in the assessment of skin responses to niacin. Transformation into the HSV color space is nonlinear and results in mixing of information from the three RGB channels. Parameters such as Hue become unstable at low color saturation, while Saturation and Value do not clearly separate the contributions of hemoglobin and melanin. As a result, the direct RGB channels retain a stronger relationship with the physical processes of light absorption by blood, which explains their greater predictive utility compared with HSV parameters35,36,37. The variability in NSFT outcomes across psychiatric diagnoses highlights its potential to reveal pathophysiological mechanisms underlying specific disorders. Our findings highlight the importance of standardizing NSFT protocols, as the differentiation ability of the test was significantly influenced by the concentration of niacin used and the timing of the measurements, which could account for discrepancies observed in previous studies. Table 2 below presents an overview of studies using NSFT, arranged chronologically with the most important observations from the studies conducted.
Limitations
There are many variables that can contribute to the wide range of different skin reactions in the NSFT. It can be influenced by skin and ambient temperature, humidity, proximity of vessels in the application area of the niacin solution, hormonal status, niacin concentration, length of the test, and method of evaluation.
Regarding the limitations of our method, there are issues that could be improved. The first one is the application of niacin solutions, which were performed manually. It can be expected that the test time for every niacin solution patch could be somehow shifted. Automating the method of applying solutions at the same time would contribute to increasing the precision of the test.
Considering the individual limb structures, the application distances between the niacin patches should be organized the same. On the other hand, the study showed that the only best-differentiating concentration of niacin solution is equal to 0.1 M.
We used C&RT analysis to predict the NSFT variables linked to psychiatric diagnosis. The C&RT disadvantages should be taken into consideration in the interpretation of obtained results. This data mining method generates binary trees and cannot handle multiclass problems. We analyzed populations with different diagnoses, and multi-analysis could better characterize the examined population51. However, considering the common psychopathology of examined diseases, multiclass analysis could be confusing and flatten the problem of diagnostic similarities. Overfitting is another issue in C&RT analysis. The most used solution is preparing by setting a criterion during the tree growth process51. We limited the variables input in the model by the initial selection and the elimination parameters dependent on clinical or sociodemographic factors. Another limitation of this study is that although sociodemographic, lifestyle, and health-related variables were systematically examined and excluded in the algorithm proposed by us, their potential indirect effects on NSFT-based group stratification and the presented results cannot be completely ruled out. This study should be interpreted as hypothesis-generating, and in future studies performed on larger cohorts, preferably from different countries or geographical areas, formal internal validation of the models will be needed. The relatively small number of participants in the study may have influenced the statistical power; therefore, the results cannot be generalized to larger populations, as the study’s character is preliminary and experimental.
Conclusions
To conclude, the NSFT shows great promise as a practical diagnostic tool for distinguishing individuals with FEP, SCH, SA, and BD from healthy controls. This simple test, which assesses fatty acid content in cell membranes, could also play a role in personalizing treatment strategies, particularly through tailored dietary recommendations. For instance, supplementing polyunsaturated fatty acids might help delay the onset or slow the progression of these disorders, even in their early stages. Improving the methodology of the NSFT and exploring the factors that influence its outcomes could expand its utility, not only in diagnostics but also in developing therapeutic and preventive strategies. Moreover, the test’s ability to reveal insights into the underlying psychopathology of specific psychiatric disorders highlights its broader potential in both clinical practice and research. However, to fully realize its capabilities, it is essential to establish a validated and standardized protocol for conducting the NSFT and interpreting its results reliably.
Materials and methods
Characteristics of study participants
The study group consisted of 120 individuals: 33 FEP, 22 BD, 13 SA, 13 CS patients, and 39 HC. Among patients, there were 41 females (50.62%), 24 cigarette smokers (29.63%), and 18 individuals diagnosed with additional somatic diseases (22.22%). A family history of mental health conditions was declared by 20 individuals (24.69%). The median age in the group was 27 years (15–56 years). The statistical difference at the level of p = 0.002 was demonstrated by body mass index (BMI) variable, among patients the median BMI was 24.58 kg/m2, while the HC group showed a BMI of 21.31 kg/m2. Another statistically significant difference was in level of physical activity p = 0.005, expressed in minutes per week. In the patient’s group, it was 0 min, while in the study group, the median was 45 min per week. Additionally, the median duration of illness for patients in years was 5, the median number of hospitalizations was 2, the olanzapine equivalent in relation to the used antipsychotic drugs 25 mg, and the median score on the Positive and Negative Syndrome Scale (PANSS) scale was 74 points (Table 3)52.
Criteria for the study
Inclusion criteria for patients:
(1) Informed written consent, (2) Women and men aged 18–50, (3) Diagnosis of SCH, BD with psychosis, or SA according to DSM-5 criteria.
Inclusion criteria for HC:
(1) Informed written consent, (2) Women and men aged 18–50.
Exclusion criteria for patients:
-
1.
Lack of consent.
-
2.
The occurrence of diseases that may affect vascular tone, skin diseases, autoimmune, cancer, cardiovascular diseases, and other somatic in an unstable phase or active inflammation.
-
3.
Current use of antibiotics, lipid-lowering drugs, antihistamines, anti-inflammatory drugs, and drugs that change the calcium metabolism.
-
4.
Use of supplements such as unsaturated fatty acids, particularly omega-3 fatty acids within the three months before the study.
-
5.
Use of vitamins or a dietary supplement containing niacin dose above 100 mg/day or the use of any dose of cannabidiol.
-
6.
Allergies, including known allergies to the test compound.
-
7.
Organic damage to the nervous system.
-
8.
Addiction other than to caffeine and/or nicotine.
-
9.
The occurrence of major mental disorders other than SCH, SA, and BD according to DSM-5.
-
10.
Pregnancy or breastfeeding.
Exclusion criteria for the HC:
-
1.
Lack of consent.
-
2.
The occurrence of diseases that may affect vascular tone, skin diseases, autoimmune, cancer, cardiovascular diseases, and other somatic diseases in an unstable phase or active inflammation.
-
3.
Current use of antibiotics, lipid-lowering drugs, antihistamines, anti-inflammatory drugs, and drugs that change the calcium metabolism.
-
4.
Use of supplements such as omega-3 fatty acids within the three months before study.
-
5.
Use of vitamins or a dietary supplement containing niacin dose above 100 mg/day or the use of any dose of cannabidiol.
-
6.
Allergies, including known allergy to the test compound.
-
7.
Organic damage to the nervous system.
-
8.
Addiction other than to caffeine and/or nicotine.
-
9.
The occurrence of SCH, SCHAD, BD or other major mental disorders according to DSM-5.
-
10.
The prevalence of mental illness in the family.
-
11.
Pregnancy or breastfeeding.
Measurement of skin reactions using niacin
The measurements were conducted under the same clinical laboratory conditions. The study used a niacin solution applied to the forearm skin in three concentrations: 0.1 M, 0.01 M, and 0.001 M. Tissue papers (2 × 2-cm) soaked in the niacin solution were in contact with the skin for 90 s. Then, the measuring device recorded the reactions on the skin.
To ensure strict standardization of lighting and limb positioning, the SKINREMS device functions as a closed measurement chamber that isolates the measurement field from external environmental variability. The forearm is inserted through a dedicated opening and positioned on a fixed internal support, which stabilizes limb orientation and maintains a constant camera-to-skin distance across all examinations. This mechanical constraint minimizes variability related to posture, rotation, and viewing angle. The construction is based on a rectangular frame made of aluminum profiles. The system walls are made of polymethyl methacrylate impermeable to light. The device has holes for the camera and the limb. Illumination is provided by an integrated LED light source mounted in a fixed position inside the enclosure. The light spectrum and intensity remain constant during all measurements, and the polymethyl methacrylate walls block ambient light, eliminating fluctuations caused by daylight or room lighting. As a result, all images are acquired under reproducible photometric conditions, which is critical for reliable quantitative color analysis. Camera exposure parameters (focus, exposure time, ISO, and white balance) were fixed within the acquisition application and remained unchanged throughout each session. The lamp used has a convenient power supply from the USB socket al.lowing mobility. The system enables standardized and repeatable measurements. Image acquisition was performed using a 64 MPx (Redmi Note 9 Pro mobile phone) camera at equal time intervals, with a dedicated application controlling the acquisition process. The applied design and procedural solutions enabled the collection of fully repeatable and comparable data, providing a reliable basis for assessing the response to NSFT. A detailed description of the measurement system with diagrams was shown in the previous review paper published by the team44,53.
Analyzing skin changes required image processing algorithms and began with the video recording video for 15-minutes. Time-lapse videos included the propagation of skin changes. The photos were triggered automatically every 60 s. For each individual 15 images for every niacin concentration were obtained during one examination. The observed formation, disappearance, and intensity of the reaction changed over time. The video files were divided into individual frames, which were the subject of further image analysis. The acquired data were subjected to processing based on parameters that may contain diagnostically significant information. A schematic representation of the SKINREMS measurement system is shown in Fig. 9, which presents the first conceptual design of the device developed by an interdisciplinary research team.

Schematic representation of the SKINREMS device showing the conceptual design of the measurement chamber, illumination system, camera positioning, and subject stabilization developed by an interdisciplinary research team. 1 - Camera, 2 - Plexiglass plate, 3 - Sliding wall handle, 4 - Aluminum profile, 5 -Foam cut-out wall for forearm placement, 6 - Ring lamp.
Image processing and skin color model description
Image processing was conducted using a semi-automatic MATLAB-based pipeline. First, frames were extracted at fixed 60-second intervals. Next, regions of interest (ROIs) corresponding to each niacin application site and adjacent control skin areas were defined. ROI boundaries were refined using edge detection and morphological operations to reduce background influence. For each ROI and time point, statistical descriptors of RGB and HSV channels (mean and median) were computed. Final diagnostic variables were expressed as differences between post-niacin ROIs and baseline control skin ROIs from the same frame, thereby reducing the influence of individual skin tone and residual lighting inhomogeneity. The Image Processing Procedure is shown in Table 4.
Image processing involved isolating ROIs changed by the niacin from areas with no solution, and background areas. The first step was to determine the baseline parameters for each individual patient. In the next step, image parameters within individual changes related to the application of the niacin solution were determined. The areas subjected to analysis were separated using edge and texture filtration and morphological operations (closure, opening, erosion, or dilation operations).
The original images were preserved in their original colors to expand the number of parameters describing the appearance and area affected by the skin change. The access to the color variables of the physiological reaction (Red, Green, Blue [RGB] and Hue, Saturation, Value [HSV]) with the possibility of comparison with the skin control areas were obtained. Acquisition of RGB variables allowed for a certain standardization of the reaction types in NSFT through the statistical description of particular intensity color changes and the control areas (determination of the mean and median of intensities in the area of isolated limb).
The determination of skin color parameters was performed using the MATLAB R2023b program and a processing algorithm designed by the authors. This algorithm allowed viewing images, selecting areas for analysis, and automatically determining coefficients characterizing skin color. Due to the high sensitivity of the digital camera, even despite the use of a proprietary measurement system, the results may be distorted by changes in lighting conditions invisible to the human eye, therefore the differences in the values of the color components between adjacent irritated and non-irritated skin areas appear to be small.
Skin areas were manually marked to account for natural skin color variations and cases of no skin reaction. Skin response was characterized by differences in color component values, expressing the color change of the irritated area. Color component values were vectors in Cartesian RGB and cylindrical HSV spaces. The RGB and HSV models are used to represent colors, but they differ in their basic assumptions and primary applications. Conversion between RGB and HSV color spaces was performed in the MATLAB environment. The conversion was performed similarly as in the Karakuła-Juchnowicz et al.44:
Finally, color characteristics were determined for each ROI. The set of representative values included: mean, median, mode, range, minimum, and maximum values of the R, G, B, H, S, and V components. The results were collected in the Excel spreadsheet. The values in each of the tested color spaces in individual measurements were subtracted from the base values of skin tones not exposed to the niacin solution. This was to highlight the features that distinguish the skin after the application of the solution from its normal shade. The measurement of natural skin color included determining RGB, HSV components, and their indicators for the entire area of the automatically extracted limb. The aim was to extract features of changes without the influence of the individual skin color of the subjects. To avoid ambiguity in the interpretation of color-related variables, it should be emphasized that all reported RGB and HSV values represent dimensionless numerical intensity levels of digital image channels, derived from pixel brightness values within the analyzed regions of interest. These parameters describe the mean or median signal intensity per pixel and do not refer to pixel count, area, or spatial dimensions.
Statistical analysis
Obtained data were analyzed using Statistica 13.3 (TIBCO Software Inc., Tulsa, USA) with p < 0.05 indicating significant differences. The Shapiro-Wilk test was used to determine the distribution of quantitative data. As most variables had non-normal distributions, the variables were expressed as median and range. The significance of differences between datasets from study groups was defined using the chi-square (for qualitative data), Student’s t-test, and Mann–Whitney U-test (for quantitative data). The correlation between examined parameters was analyzed using Pearson and Spearman’s rank correlation coefficients. A binary partitioning statistical data-mining technique: C&RT algorithm was used to find the NSFT-based model for classifying subgroups of patients based on diagnosis. The diagnostic ability of the proposed models was further tested using receiver operating characteristic curve (ROC) analysis.
Establishing a model for the classification of psychiatric disorders
In biological datasets, high variance often occurs in individuals with the same clinical conditions due to their multi-factorial origin. In diseases that involve genetics and environmental factors, explaining the obtained results is challenging. The study uses a five-step approach to classify the psychiatric conditions.
Step 1: Screening procedure of potential variables differentiate individuals with psychiatric diseases.
To determine the potential variables that vary between individuals with psychiatric disease and HC, we compare the results obtained between HC and patient groups. According to analysis, 469 from 1184 (1091 with a non-normal distribution) variables differed between examined populations and were used for analysis.
Step 2: Exclusion of the variables affected by sociodemographic, lifestyle and health-related factors.
Many studies confirm NSFT exhibits a strong relationship with age, gender, food habits, tobacco and others. We excluded the NSFT data connected with sociodemographic, lifestyle, and health factors to minimize the risk of bias due to confounders. The relationship was assessed for both groups in the order determined by the researchers. The variable was removed if the connection was found in any group, independently from the strength of the relationship. The following parameters were put into the analysis: age, gender, presence of chronic disease, family history of mental health problems, body mass index (BMI), physical activity (minutes per week) and tobacco smoking (Picture 1). After this step, 137 (92 with a non-normal distribution) variables were found to be not affected by the factors mentioned above.

The relationship between NSFT results and sociodemographic, lifestyle and health-related factors.
Step 3: Exclusion of the variables affected by the disease-related factors.
This step was performed only in the patient group. The concept that lipid metabolism is engaged in the pathophysiology of psychiatric diseases is well known, and due to potential disturbance, some clinical-related factors may affect NSFT. The ideal diagnostic biomarker should not be affected by drugs or disease severity, progression, or other disease-related factors. We excluded NSFT data connected with disease-related factors such as duration of illness, number of hospitalizations, equivalents of olanzapine, and severity of symptoms. 53 variables have been excluded in this step.
Step 4: Machine learning model implementation.
In diagnostic studies, the test should yield binary outcomes, i.e., the presence or absence of the feature. The approach which allows this solution is to determine cut-off points for variables. The continuous values of NSFT were transformed into dichotomous ones (below and upon the cut-off point) using the C&RT method. C&RT allow the identification of features of mutually exclusive populations easily. During analysis, the algorithm generates rules based on which the individuals can be assigned to one of two subpopulations. We established a two-step classification model:
-
a.
Presence or absence of psychiatric disease.
-
b.
Psychiatric diagnosis decision trees applied in patient groups.
Step 5: Assess the accuracy of models.
ROC curve analyses were then applied to assess the efficacy of C&RT analysis results, using NSFT combined results as a biomarker/ the characteristic features for/of examined patient subgroups.
Step 6: Integration of data from C&RT analysis.
We attempted to characterize individual mental disorders based on the obtained cut-off points of NSFT. Using this integrative approach (combining the results from obtained trees), we identified the variables that were repeated within two groups and removed them. The remaining variables were considered to be characteristics of particular groups of patients and HC. A summary of the following steps is presented in Scheme 1.

Graphical presentation of methodology for model fit.
Data availability
The data presented in this study are available on request from the corresponding author.
Abbreviations
- NSFT:
-
Niacin skin flush test
- SCH:
-
Schizophrenia
- CS:
-
Chronic schizophrenia
- SA:
-
Schizoaffective disorder
- BD:
-
Bipolar affective disorder
- C&RT:
-
Classification and regression tree
- ROC:
-
Receiver operating characteristic curve
References
Bosveld-van Haandel, L., Knegtering, R., Kluiter, H. & van den Bosch, R. J. Niacin skin flushing in schizophrenic and depressed patients and healthy controls. Psychiatry Res. 143(2–3), 303–306. https://doi.org/10.1016/j.psychres.2005.10.010 (2006).
Murrell, T. W. The cutaneous reaction to nicotinic acid (niacin)-Furfuryl. Arch. Dermatol. 79(5), 545. https://doi.org/10.1001/archderm.1959.01560170043008 (1959).
Hoffer, A. Adverse effects of niacin in emergent psychosis. JAMA: J. Am. Med. Association. 207(7), 1355. https://doi.org/10.1001/jama.1969.03150200121025 (1969b).
Fiedler, P., Wolkin, A. & Rotrosen, J. Niacin-induced flush as a measure of prostaglandin activity in alcoholics and schizophrenics. Biol. Psychiatry. 21(13), 1347–1350. https://doi.org/10.1016/0006-3223(86)90321-5 (1986).
Horrobin, D. F. Schizophrenia: A biochemical disorder? Biomedicine 32(2), 54–55 (1980). PMID: 7388116.
Wang, D. D. et al. Attenuated and delayed niacin skin flushing in schizophrenia and affective disorders: A potential clinical auxiliary diagnostic marker. Schizophr Res. 230, 53–60 (2021).
Messamore, E. The niacin skin flush abnormality in schizophrenia: A quantitative dose–response study. Schizophr Res. 62, 251–258 (2003).
Puri, B. K., Easton, T., Das, I., Kidane, L. & Richardson, A. J. The niacin skin flush test in schizophrenia: A replication study. Int. J. Clin. Pract. 55, 368–370 (2001).
Hudson, C. J., Lin, A., Cogan, S., Cashman, F. & Warsh, J. J. The niacin challenge test: Clinical manifestation of altered transmembrane signal transduction in schizophrenia? Biol. Psychiatry. 41(5), 507–513. https://doi.org/10.1016/s0006-3223(96)00112-6 (1997).
Puri, B. K. & Singh, I. Normal phospholipid-related signal transduction in autism. Prog. Neuropsychopharmacol. Biol. Psychiatry. 26(7–8), 1405–1407. https://doi.org/10.1016/s0278-5846(02)00303-2 (2002).
Katzman, M. et al. Methyl nicotinate-induced vasodilation in generalized social phobia. Neuropsychopharmacology 28(10), 1846–1851. https://doi.org/10.1038/sj.npp.1300227 (2003).
Cyhlarova, E., Montgomery, P., Ross, M. A. & Richardson, A. J. Niacin skin test response in dyslexia. Prostaglandins, Leukot. Essent. Fatty Acids. 77(2), 123–128. https://doi.org/10.1016/j.plefa.2007.08.005 (2007).
Puri, B. K. Impaired phospholipid-related signal transduction in advanced Huntington’s disease. Exp. Physiol. 86(5), 683–685. https://doi.org/10.1113/eph8602216 (2001).
Horrobin, D. F. Schizophrenia: A biochemical disorder? Biomedicine 32, 54–55 (1980).
Horrobin, D. F., Glen, A. I. M. & Vaddadi, K. The membrane hypothesis of schizophrenia. Schizophr. Res. 13(3), 195–207. https://doi.org/10.1016/0920-9964(94)90043-4 (1994).
Smesny, S. et al. Potential use of the topical niacin skin test in early psychosis -- a combined approach using optical reflection spectroscopy and a descriptive rating scale. J. Psychiatr. Res. 37(3), 237–247. https://doi.org/10.1016/s0022-3956(03)00006-2 (2003).
Rybakowski, J. & Weterle, R. Niacin test in schizophrenia and affective illness. Biol. Psychiatry. 29, 834–836 (1991).
Glen, A. I. M. et al. Membrane fatty acids, niacin flushing and clinical parameters. Prostaglandins Leukot. Essent. Fat. Acids. 55, 9–15 (1996).
Smesny, S. et al. Potential use of the topical niacin skin test in early psychosis—A combined approach using optical reflection spectroscopy and a descriptive rating scale. J. Psychiatr Res. 37, 237–247 (2003).
Ross, B. Reduced vasodilatory response to methylnicotinate in schizophrenia as assessed by laser Doppler flowmetry. Eur. Neuropsychopharmacol. 14, 191–197 (2004).
Liu, C. M. et al. Absent response to niacin skin patch is specific to schizophrenia and independent of smoking. Psychiatry Res. 152(2–3), 181–187. https://doi.org/10.1016/j.psychres.2006.10.002 (2007).
Smesny, S. et al. The influence of age and gender on niacin skin test results – implications for the use as a biochemical marker in schizophrenia. J. Psychiatr. Res. 38(5), 537–543. https://doi.org/10.1016/j.jpsychires.2004.01.007 (2004).
Smesny, S., Baur, K., Rudolph, N., Nenadic, I. & Sauer, H. Alterations of niacin skin sensitivity in recurrent unipolar depressive disorder. J. Affect. Disord. 124(3), 335–340. https://doi.org/10.1016/j.jad.2009.12.017 (2010).
Kerr, M. et al. The topical niacin sensitivity test: An inter- and intra-rater reliability study in healthy controls. Prostaglandins, Leukot. Essent. Fatty Acids. 79(1–2), 15–19. https://doi.org/10.1016/j.plefa.2008.06.001 (2008).
Ward, P. E., Sutherland, J., Glen, E. M. T. & Glen, A. I. M. Niacin skin flush in schizophrenia: A preliminary report. Schizophr. Res. 29(3), 269–274. https://doi.org/10.1016/s0920-9964(97)00100-x (1998).
Chang, S. S. et al. Impaired flush response to niacin skin patch among schizophrenia patients and their nonpsychotic relatives: The effect of genetic loading. Schizophr. Bull. 35(1), 213–221. https://doi.org/10.1093/schbul/sbm153 (2008).
Wilson, D. W. S. & Douglass, A. B. Niacin skin flush is not diagnostic of schizophrenia. Biol. Psychiatry. 21(10), 974–977. https://doi.org/10.1016/0006-3223(86)90274-x (1986).
Stamatas, G. N. & Kollias, N. Blood stasis contributions to the perception of skin pigmentation. J. Biomed. Opt. 9(2), 315. https://doi.org/10.1117/1.1647545 (2004a).
Xian, Y. L., Dai, Y., Gao, C. M. & Du, R. Dual-wavelength retinal images denoising algorithm for improving the accuracy of oxygen saturation calculation. J. Biomed. Opt. 22(01), 1. https://doi.org/10.1117/1.jbo.22.1.016004 (2017).
Gruensfelder, H. D. et al. Characterization of biological absorption spectra spanning the visible to the short-wave infrared. J. Visualized Experiments. 215 https://doi.org/10.3791/67403 (2025).
Liu, P., Zhu, Z., Zeng, C. & Nie, G. Specific absorption spectra of hemoglobin at different PO2 levels: Potential noninvasive method to detect PO2 in tissues. J. Biomed. Opt. 17(12), 125002. https://doi.org/10.1117/1.jbo.17.12.125002 (2012).
Burns, J. M., Saager, R., Majaron, B., Jia, W. & Anvari, B. Optical properties of biomimetic probes engineered from erythrocytes. Nanotechnology 28(3), 035101. https://doi.org/10.1088/1361-6528/28/3/035101 (2016).
Zijlstra, W. G., Buursma, A. & van Assendelft, O. W. Visible and near Infrared Absorption Spectra of Human and Animal Haemoglobin. https://doi.org/10.1201/9780429071096 (2021).
Yang, B. et al. Color structured light imaging of skin. J. Biomed. Opt. 21(5), 050503. https://doi.org/10.1117/1.jbo.21.5.050503 (2016).
Cai, L. & Pfob, A. Processing HSV Colored Medical Images and Adapting Color Thresholds for Computational Image Analysis: a Practical Introduction to an open-source tool. https://arxiv.org/abs/2404.17878 (2024).
Kumar, K. & chaduvula A Detailed Survey On Feature Extraction Techniques In Image Processing For Medical Image Analysis. (2021).
Hassan, R., Ema, R. & Islam, T. Color Image Segmentation using Automated K-Means Clustering with RGB and HSV Color Spaces. 17. 33–41. (2017).
Hudson, C., Gotowiec, A., Seeman, M., Warsh, J. & Ross, B. M. Clinical subtyping reveals significant differences in calcium-dependent phospholipase A2 activity in schizophrenia. Biol. Psychiatry. 46, 401–405 (1999).
Puri, B. K., Hirsch, S. R., Easton, T. & Richardson, A. J. A volumetric biochemical niacin flush-based index that noninvasively detects fatty acid deficiency in schizophrenia. Prog Neuro-Psychopharmacol Biol. Psychiatry. 26, 49–52 (2002).
Tavares, H., Yacubian, J., Talib, L. L., Barbosa, N. R. & Gattaz, W. F. Increased phospholipase A2 activity in schizophrenia with absent response to niacin. Schizophr Res. 61, 1–6 (2002).
Lin, S. H. et al. Familial aggregation in skin flush response to niacin patch among schizophrenic patients and their nonpsychotic relatives. Schizophr Bull. 33, 174–182 (2006).
Yao, J. K. et al. Prevalence and specificity of the abnormal niacin response: A potential endophenotype marker in schizophrenia. Schizophr Bull. 42, 369–376 (2015).
Sun, L. et al. Identification of the niacin-blunted subgroup of schizophrenia patients from mood disorders and healthy individuals in Chinese population. Schizophr Bull. 44, 896–907 (2017).
Karakula-Juchnowicz, H. et al. SKINREMS—A new method for assessment of the niacin skin flush test response in schizophrenia. J. Clin. Med. 9, 1848 (2020).
Hu, Y. et al. A potential objective marker in first-episode schizophrenia based on abnormal niacin response. Schizophr Res. 243, 405–412 (2021).
Zhang, T. et al. Association of attenuated niacin response with inflammatory imbalance and prediction of conversion to psychosis from clinical high-risk stage. J. Clin. Psychiatry, 84(5). (2023).
Ju, M. et al. Cognitive impairments in first-episode psychosis patients with attenuated niacin response. Schizophr. Res. 40, 100346 (2025).
Wang, J. et al. Efficacy of identifying treatment-resistant and non-treatment-resistant schizophrenia using niacin skin flushing response combined with clinical feature. Schizophrenia. 11(1) (2025).
Lyu, X., Goperma, R., Wang, D., Wan, C. & Zhao, L. An open dataset and machine learning algorithms for niacin skin-flushing response based screening of psychiatric disorders. BMC Psychiatry. 25(1). (2025).
Chen, H. et al. Blunted niacin skin flushing response in violent offenders with schizophrenia: A potential auxiliary diagnostic biomarker. J. Psychiatr. Res. 184, 249–255 (2025).
Li, L. Application of machine learning and data mining in medicine: Opportunities and considerations. Artif. Intell. https://doi.org/10.5772/intechopen.113286 (2023).
Leucht, S., Samara, M., Heres, S. & Davis, J. M. Dose equivalents for antipsychotic drugs: The DDD method: Table 1. Schizophr. Bull. 42(suppl 1). https://doi.org/10.1093/schbul/sbv167 (2016).
Sitarz, R. et al. Niacin skin flush backs—from the roots of the test to nowadays hope. J. Clin. Med. 12(5), 1879. https://doi.org/10.3390/jcm12051879 (2023).
Funding
The study was financed from the grant registered under number GW/PB/6/2022, PBsd101 based on the provisions of Annex No. 2 to Order No. 12/2021 of the Rector of the Medical University of Lublin of January 27, 2021.
Author information
Authors and Affiliations
Contributions
R.S., J.R., R.K., A.M., K.K., J.B., D.J., A.R. A.S., H.K.JConceptualization - R.S., J.R., R.K., A.M., K.K., J.B., D.J., A.R. A.S., H.K.JMethodology - R.S., R.K., A.M., J.R., H.K.J. Formal Analysis - R.S., R.K., A.M.Investigation - R.S., J.R., R.K., A.M., K.K., J.B., D.J., A.R. A.S., H.K.JWriting-original draft preparation - R.S., J.R., R.K., A.M., K.K., J.B., D.J., A.R., A.S., H.K.JWriting-review and editing - R.S., J.R., R.K., A.M., K.K., J.B., D.J., A.R., A.S., H.K.JVisualization - R.K., A. M. Supervision - D.J., H.K.J. Project administration - R.S. Funding aquisition - R. S., H.K.J.
Corresponding author
Ethics declarations
Informed consent
Informed consent was obtained from all individuals involved in the study.
Institutional review board statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Medical University of Lublin, Poland (project identification code: KE-0254/213/2021).
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sitarz, R., Rog, J., Karpiński, R. et al. Differentiation of psychotic and affective disorder patients from healthy controls using the niacin skin flush test: a novel analytical method and the SKINREMS system—preliminary research. Sci Rep 16, 8896 (2026). https://doi.org/10.1038/s41598-026-42991-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-42991-1
