
Abstract
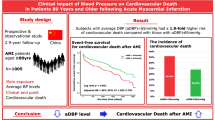
The combined effect of admission systolic (SBP) and diastolic blood pressure (DBP) on short- and long-term all-cause mortality in patients with acute aortic dissection (AAD) remains insufficiently characterized. This retrospective cohort study investigated these associations to identify potential blood pressure thresholds linked to minimized mortality risk. We utilized restricted cubic splines (RCS) to characterize nonlinear associations, identifying specific BP levels (nadirs) associated with the lowest risk of mortality. Segmented analysis was employed to assess linear relationships flanking these nadirs, and multivariable Cox regression models were applied to evaluate the impact of different BP ranges after adjusting for potential confounders. Our results revealed a significant J-shaped correlation for admission SBP and DBP regarding long-term mortality. Mortality risks escalated at SBP levels departing from a nadir of 143.4 mmHg and at DBP departing from 83.7 mmHg. Specifically, an admission SBP/DBP range of 130–160/80–88 mmHg was associated with the lowest long-term all-cause mortality risk, serving as the risk-nadir interval in this cohort. Other independent predictors of mortality included advanced age, myocardial infarction, higher heart rate, history of heart bypass, elevated NT-proBNP and hsTNT, while type B AAD, normal heart rhythm and surgery within 24 h were protective factors. In conclusion, admission SBP and DBP exhibit significant nonlinear associations (J-shaped) with long-term all-cause mortality in AAD. The identified 130–160/80–88 mmHg range represents a potential reference interval for admission hemodynamic management, while acknowledging the need for validation in diverse clinical settings.
Similar content being viewed by others

Introduction
Acute aortic dissection (AAD) is a life-threatening cardiovascular emergency characterized by a rapid clinical progression. If left untreated, the mortality rate for complicated cases reaches 40% upon admission, with a subsequent hourly increase of 1%1,2. Despite advancements in surgical and medical interventions, AAD remains a leading cause of sudden death among thoracic aortic diseases3,4. Consequently, identifying robust admission predictors is essential for early risk stratification and improving patient survival. Blood pressure (BP) is a fundamental hemodynamic parameter influencing outcomes across various cardiovascular conditions5. While a non-linear J-shaped relationship between BP and vascular events has been well-documented in coronary artery disease6, its prognostic role in AAD remains less clear. Current research has predominantly focused on the association between systolic blood pressure (SBP) and in-hospital mortality7,8,9,10. In contrast, the prognostic value of diastolic blood pressure (DBP) is frequently overlooked, with only limited evidence from small-scale studies (n = 72) suggesting a potential inverse relationship with mortality11.This gap in the literature leads to significant clinical uncertainty regarding optimal BP targets12,13,14,15,16. Most existing studies focus on isolated SBP values, neglecting the integrated influence of both SBP and DBP on long-term outcomes. To address this, the present study systematically evaluates the short- and long-term impact of admission SBP and DBP on all-cause mortality in a large AAD cohort. By defining precise reference thresholds, we aim to provide evidence-based guidance for blood pressure regulation to maximize survival in this high-risk population.
Materials and methods
Study design and study population
This study was a multicenter retrospective cohort study that included 726 patients diagnosed with AAD from two provincial hospitals in Guangxi: The People’s Hospital of Guangxi Zhuang Autonomous Region and the Affiliated Hospital of Guilin Medical University, spanning from January 2015 to November 2023. These hospitals are situated in the southern and northern regions of Guangxi, respectively. Of the 726 patients, 16 were lost to follow-up after being discharged alive from the hospitals. After discharge, 53 patients were confirmed to have died through nursing follow-up, but the exact date of their death cannot be determined. To minimize selection bias and maximize the utilization of available data, these 69 patients were right-censored at the date of their last known follow-up in accordance with standard survival analysis protocols. The study was approved by Research Ethics Committee at the People’s Hospital of Guangxi Zhuang Autonomous Region, China (IRB-KY-ZC-2023-049). We confirmed that all methods were performed in accordance with the relevant guidelines and regulations.
Definition of acute aortic dissection
The diagnosis of type A and type B AAD was established using contrast-enhanced computed tomography upon admission for all patients. Types A and B AAD were defined as non-traumatic dissections of the aorta that occur proximal and distal to the left subclavian artery, respectively, and presenting within 14 days of the onset of symptoms17.
Data collection
The demographic and admission clinical characteristics and in-hospital outcomes were extracted from medical records. The death outcome for patients discharged alive from the hospitals was achieved from many ways including nursing follow-up, linkage with the National mortality surveillance system data and Guangxi health insurance system.
Study endpoints and follow-up
This study involved a single patient cohort, with the baseline defined as the date of hospital admission. To comprehensively assess the prognosis of Acute Aortic Dissection, we defined two primary endpoints: (1) Short-term Outcome: All-cause mortality within 30 days of admission. (2) Long-term Outcome: Cumulative all-cause mortality within 2 years of admission. The observation period for each patient commenced at admission and continued until the occurrence of death or the date of censorship. Patients were censored at the earlier of the following: the predefined follow-up mark (30 days or 2 years, respectively) or the last known date they were confirmed to be alive (for those lost to follow-up or with unknown death dates). For the 2-year analysis, those who survived beyond 30 days remained in the at-risk pool until the end of the 2-year follow-up.
Exposure variable
The combined SBP/DBP was the primary exposure variable in our study. Restricted cubic splines (RCS), a nonparametric modeling technique based on spline functions, was used to explore the potential nonlinear dependency in the relationship between the risk of 30-day or 2-year mortality and SBP and DBP, respectively. RCS is essentially a piecewise polynomial function that is continuous and has continuous second-order derivatives at each knot point18. In this segment of the analysis, SBP and DBP were maintained as continuous variables. If a nonlinear and significant association was observed, the nadirs for SBP and DBP would be determined. Subsequently, SBP and DBP would be categorized into subgroups, which would then be analyzed in combination to assess their effects on mortality.
Covariates
Our study attempted to include as many as variables as the covariates to control the potential confounding. Covariates in the multivariable models included baseline characteristics (age, gender, and AAD type), medical history, clinical biomarkers, and presenting signs and symptoms at admission. The comprehensive list of all adjusted variables and their specific definitions is provided in Supplementary Table S1. Continuous covariates were stratified into normal range, below and/or over normal range, except for D-dimer was divided into four quantiles based on interquartile interval.
The final model was selected based on clinical relevance and statistical stability [assessed via Akaike Information Criterion (AIC) and C-index].
Statistical analysis
Statistical analyses were performed using R (version 4.3.2). Categorical variables were compared between survivors and non-survivors using Chi-square tests. Mortality rates were calculated per 100 person-days for the total cohort and stratified subgroups. Potential non-linear associations between BP and all-cause mortality were explored using RCS with three knots. Thresholds for joint hemodynamic phenotypes were derived from RCS-identified risk-inflection points and established clinical guidelines, as detailed in Table 2; Fig. 2.The independent prognostic value of BP was evaluated through six sequential Cox proportional hazards models.Model 1: Crude model. Model 2: Adjusted for age, gender, and AAD type. Models 3–5: Model 2 plus medical history, signs/symptoms, and biomarkers, respectively (Supplementary Table S1). Model 6 (Full Model): Model 5 plus emergency surgery (< 24 h). Sensitivity analyses were conducted based on re-evaluating associations with 5-knot RCS, and categorizing SBP [< 100, 100–160 (Ref.), and > 160 mmHg] and DBP [< 80, 80–89 (Ref.), 90–99, and ≥ 100 mmHg] to assess the impacts of hypotension and hypertension. The proportional hazards assumption was verified for all models. RCS and Cox analyses utilized the “rms”, “survival”, and “ggrcs” packages. All tests were two-sided, with statistical significance defined as P < 0.05.
Results
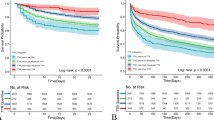
As shown in the study flowchart (Fig. 1), 700 patients were included for analysis after excluding 26 individuals with missing admission BP data. The cohort comprised 306 (43.7%) patients with Stanford type A and 394 (56.3%) with type B AAD. During follow-up, 152 all-cause deaths occurred within 30 days, increasing to 175 within 2 years. Age distribution was skewed toward younger groups: one-third each for < 50 and 50–59 years, 25% for 60–69 years, and 17% for ≥ 70 years.

Flowchart of participants with aortic dissection admission enrollment.
The overall mortality rate for patients with AAD was 0.794 (95% CI: 0.789–0.801) per 100 person-days in the 30-day cohort and 0.044 (95% CI: 0.043–0.046) per 100 person-days in the 2-year cohort, respectively. Baseline characteristics, including demographics, medical history, clinical biomarkers, and presenting symptoms, are compared between survivors and non-survivors for both the 30-day and 2-year endpoints in Supplementary Table S2 and Table 1. Compared to survivors, non-survivors at both endpoints exhibited significant differences in age, AAD type, cardiac function (LVEF, NT-proBNP, hsTNT), biomarkers (FPG, D-dimer), and clinical complications [e.g., heart failure, Intramural Hematoma (IMH), ST-T changes; all P < 0.05]. Additionally, disparities in hemoglobin and creatinine levels reached statistical significance only at the 2-year mark.
As illustrated in Fig. 2, RCS models, using the RCS function with 3 knots for SBP or DBP, adjusted for demographics, medical history, presenting signs and symptoms and clinical biomarkers at admission, revealed a consistent J-shaped relationship between admission blood pressure and mortality risk across both endpoints. However, these associations did not reach statistical significance in the 30-day cohort (SBP: P overall = 0.069, P non-linear = 0.126; DBP: P overall = 0.215, P non-linear = 0.082). In contrast, significant non-linear associations were observed for the 2-year mortality risk (SBP: P overall = 0.009, P non-linear = 0.008; DBP: P overall = 0.020, P non-linear = 0.005), with risk nadirs identified at 143.7 mmHg for SBP and 83.7 mmHg for DBP. Sensitivity analyses using 5-knot models confirmed these non-linear trends (Figure S1). For 2-year mortality, the non-linear association remained robust across different knot specifications (P nonlinear = 0.008 for 3-knot vs. 0.041 for 5-knot in SBP; 0.005 vs. 0.025 in DBP). Notably, while the DBP nadir showed a modest shift with additional knots (from 83.7 to 94.2 mmHg), both models consistently identified a stable low-risk plateau between 80 and 95 mmHg. This range aligns with the clinical objective of balancing aortic wall tension reduction against the maintenance of end-organ perfusion. To ensure a parsimonious model that avoids overfitting, the 3-knot-derived nadirs were utilized as the formal cut-off points for all subsequent piecewise linear and categorical Cox analyses.


Restricted Cubic Spline (RCS) Curves for the Association of Admission Blood Pressure with Short-term and Long-term Mortality. Adjusted Hazard Ratios (HRs) for the associations of admission systolic blood pressure (SBP) and diastolic blood pressure (DBP) with 30-day and 2-year all-cause mortality are shown via RCS models with 3 knots. The models were adjusted for: (1) Demographics: age, gender, type of AAD; (2) Medical history: Hypertension, coronary heart disease, type 2 diabetes mellitus, Marfan syndrome, heart bypass surgery, heart valve replacement; (3) Clinical biomarkers: NTproBNP and hsTNT at admission; (4) Presenting signs and symptoms at admission: Heart rhythm regularity, aortic aneurysm, thoracodynia, back pain, abdominal pain, syncope, pericardial effusion, and myocardial infarction. Figure 2 − 1 and 2–2 represent the dose-response relationship between admission SBP and DBP and the risk of 30-day mortality. Figure 2-3 and 2-4 represent the relationship between admission SBP and DBP and the risk of 2-year mortality. The solid blue lines indicate the estimated HRs, and the shaded light-blue areas represent the corresponding 95% confidence intervals (CIs). The pink histograms in the background reflect the density distribution of blood pressure values among the study participants. The horizontal dashed line is positioned at HR = 1.0 as the reference point. For 30-day mortality, the associations for SBP (P overall = 0.069) and DBP (P overall = 0.215) did not reach statistical significance. For 2-year mortality, significant non-linear associations were observed for both SBP (P overall = 0.009, P nonlinear = 0.008) and DBP (P overall = 0.020, P nonlinear = 0.005), indicating a J-shaped prognostic relationship.
Based on the identified RCS nadirs (Table 2), piecewise linear regression was performed to quantify the risk trends on either side of the inflection points. Below the SBP threshold of 143.4 mmHg, an inverse association with 2-year mortality was observed (OR: 0.994 per 1-mmHg increase; 95% CI: 0.991–0.997; P < 0.001). Conversely, above this threshold, the risk exhibited a significant ascending trend (OR: 1.017; 95% CI: 1.001–1.033; P = 0.043). Similarly, for DBP, a significant risk reduction was observed as levels increased toward 83.7 mmHg (OR: 0.953; 95% CI: 0.920–0.987; P = 0.006). However, beyond this point, the positive association between higher DBP and mortality did not reach statistical significance (OR: 1.028; 95% CI: 0.995–1.061; P = 0.097).
We categorized patients into eight BP phenotypes based on RCS-identified nadirs, sample size distribution and clinical thresholds (130/160 mmHg for SBP; 80/88/100 mmHg for DBP). The “130–160 / 80–88 mmHg” group was designated as the reference, representing the lowest risk nadir (Table 3). These phenotypes were then analyzed via sequential Cox models to determine their independent associations with 2-year mortality. Multivariable Cox regression analysis revealed that the “>160/89–100 mmHg” phenotype was consistently associated with the highest risk of 2-year mortality across all adjusted models (Table 3). In the fully adjusted model (Model 6), this group demonstrated a nearly three-fold increase in mortality risk (HR 2.77, 95% CI 1.22–6.27, P = 0.015). The “<130/<80 mmHg” group also exhibited a significant risk elevation in Model 6 (HR 1.96, 95% CI 1.00–3.81, P = 0.049), maintaining a trend observed throughout the sequential adjustment process. Other phenotypes, such as > 160/≤88 mmHg and > 160/>100 mmHg, showed significant or near-significant associations in several adjustment models but exhibited wider confidence intervals in the final model, potentially due to smaller subgroup sample sizes or treatment bias. These categorical findings provide quantitative support for the non-linear risk patterns identified in the continuous RCS analysis.
Sensitivity analyses further evaluated the independent prognostic value of BP components and extreme hypotension. When analyzed independently of SBP, a DBP of 90–99 mmHg was associated with increased 30-day mortality risk (HR 1.95, 95% CI: 1.06–3.59, P = 0.032; Table S3), though this significance did not persist at 2 years. Furthermore, patients with admission hypotension (SBP < 100 mmHg) exhibited a higher prevalence of high-risk clinical features, including inter-arm BP differences and STEMI (Table S4-1), resulting in significantly higher crude mortality rates at both 30 days and 2 years. After full multivariable adjustment (Model 6), SBP < 100 mmHg maintained a consistent trend toward increased mortality risk (30-day HR 1.17; 2-year HR 1.33) compared to the 100–160 mmHg range, although these associations did not reach formal statistical significance (Table S4-2).
Figure 3 illustrates the independent predictors of 2-year mortality in the fully adjusted model (Model 6). Beyond the BP phenotypes, several baseline factors emerged as significant risk indicators. Advanced age (60–69 years: HR 1.98, 95% CI 1.18–3.31; ≥70 years: HR 2.22, 95% CI 1.27–3.89) and a heart rate > 100 bpm (HR 1.69, 95% CI 1.09–2.61) were associated with increased mortality. High-risk clinical presentations, particularly concomitant elevated myocardial infarction (STMI) (HR 3.63, 95% CI 1.81–7.26) and a history of heart bypass (HR 3.99, 95% CI 1.04–15.22), as well as elevated biomarkers including NTproBNP > 100 (HR 3.89, 95% CI 1.17–12.94) and hsTNT > 0.04 (HR 1.62, 95% CI 1.04–2.54), also demonstrated substantial risk elevation. Conversely, protective factors included Type B AAD (vs. Type A: HR 0.57, 95% CI 0.39–0.84), normal heart rhythm (HR 0.64, 95% CI 0.41–0.99), and undergoing surgery within 24 h (HR 0.35, 95% CI 0.23–0.54).

Forest plot displaying the significant variables identified in the full model. HR refers to adjusted hazard ratio, SBP refers to systolic blood pressure, DBP refers to diastolic blood pressure, AAD refers to acute aortic dissection, STMI refers to Elevated myocardial infarction upon admission, NTproBNP refers to N-terminal pro-B-type natriuretic peptide, hsTNT refers to High-sensitivity troponin T, Operation within 24 h denotes underwent surgery within 24 h up admission.
Discussion
This study identified a significant J-shaped association between admission BP and 2-year all-cause mortality in AAD, whereas short-term associations were less pronounced. By utilizing RCS analysis, we established objective risk nadirs at SBP 143.4 mmHg and DBP 83.7 mmHg, identifying a risk-nadir range of 130–160/80–88 mmHg associated with the lowest long-term risk. Beyond BP thresholds, advanced age, cardiovascular comorbidities, and elevated biomarkers (NT-proBNP and hsTNT) emerged as independent risk factors, while surgery within 24 h provided significant survival benefits. These findings suggest that admission SBP and DBP exhibit a complex, non-linear prognostic impact, necessitating a holistic hemodynamic assessment to optimize long-term survival in this high-risk population.
The J-shaped relationship between BP and cardiovascular outcomes is well-documented, particularly regarding coronary heart disease and all-cause mortality19. Our findings extend this paradigm to AAD, identifying that both excessively low (SBP < 130, DBP < 80 mmHg) and excessively high values (SBP > 160, DBP > 88 mmHg) are detrimental to long-term survival. While a previous IRAD study reported a J-shaped association between admission SBP and in-hospital mortality7, our results confirm that this non-linear risk profile persists over a 2-year follow-up, representing a true biological inflection point in this population.
The risk escalation at the higher end of the spectrum reflects a state of extreme hemodynamic derangement. Our joint category analysis, pre-specified based on RCS nadirs, identified the > 160/89–100 mmHg phenotype as carrying the highest prognostic risk. This highlights a synergistic effect where severe systolic hypertension is exacerbated by concurrent diastolic elevation. According to Laplace’s Law, this specific combination maximizes circumferential wall stress which is the primary mechanical driver for false lumen expansion or rupture20,21,22. While DBP showed modest standalone value, it acts as a critical risk potentiator, the consistent results across both categorical and continuous RCS models reinforce that SBP > 160 mmHg, when coupled with elevated DBP, significantly intensifies the pulsatile load on the weakened aortic wall.
Conversely, our study underscores the clinical gravity of admission hypotension. Patients with SBP < 100 mmHg exhibited significantly higher crude mortality, identifying it as a “red flag” for catastrophic complications such as cardiac tamponade or malperfusion23. Although multivariable HRs (1.17–1.33) remained elevated but non-significant, this likely reflects the adjustment for strong mediators—such as pericardial effusion and myocardial ischemia—which lie on the causal pathway between the aortic event and hypotension24,25. Nevertheless, the sharp risk escalation at the lower end of our RCS curves robustly supports the danger of “too low” admission BP, aligning with evidence that malperfusion confers heightened risk in AAD26,27,28.
The validity of our findings is reinforced by the convergence between the categorical models and continuous splines. Our RCS analysis identified a relatively stable risk plateau for DBP between 80 and 95 mmHg (Fig. 2), which is consistent with the categorical findings in Table 3. Specifically, within the SBP 130–160 mmHg strata, deviations in DBP above 88 mmHg (group 130–160/>88 mmHg) did not result in a statistically significant increase in mortality risk (Model 6: HR = 1.63, P = 0.229), supporting the existence of a moderate “hemodynamic window”. However, this DBP plateau appears context-dependent, when SBP exceeded 160 mmHg, even a moderate elevation of DBP (89–100 mmHg) triggered a sharp and significant escalation in risk (HR = 2.77, P = 0.015). This suggest that while the 80–95 mmHg DBP range may be relatively well-tolerated under controlled systolic tension, it becomes a critical contributor to aortic wall failure when coupled with severe systolic hypertension.
The risk-nadir range identified in our study (130–160/80–88 mmHg) appears higher than the intensive targets (< 120/80 mmHg) recommended by current guidelines. This discrepancy highlights the critical “organ perfusion balance” in AAD. Overly aggressive BP reduction may exacerbate malperfusion in patients whose true lumen is compromised or whose autoregulation curves are shifted by chronic hypertension29. Furthermore, the increased mortality at lower BP levels likely reflects “reverse causality”, where hypotension serves as a marker for frailty or impending cardiac tamponade rather than a direct cause of death30,31,32. Our findings thus suggest that while long-term intensive control is vital for atherosclerotic prevention, the acute and subacute management of AAD requires a nuanced ‘safety zone’ to balance aortic protection against systemic perfusion33.
Finally, several non-BP factors emerged as independent predictors of mortality. Advanced age, heart rate over 100 bpm and concomitant myocardial infarction at admission were associated with poor prognosis, consistent with previous reports34,35,36,37. The high risk associated with elevated NT-proBNP and hsTNT likely reflects acute cardiac strain and abnormalities in left ventricular function secondary to chronic hypertension or aortic regurgitation38,39,40. While Type B AAD41 and timely surgical intervention (within 24 h)42 were protective, a normal heart rhythm at admission also favored survival. Normal sinus rhythm may reflect a more stable hemodynamic state and the absence of conductive system involvement by the dissection flap, whereas arrhythmias often herald severe metabolic derangement or direct myocardial ischemia43.
Several limitations should be acknowledged. First, the retrospective design may introduce inherent selection and information bias. Although the loss-to-follow-up rate was under 10%, missing data for certain variables remains a constraint. Second, admission BP values may not fully reflect the hyperacute hemodynamic status, and patients with pre-hospital mortality were not captured, potentially leading to a survival bias. Third, while the high C-index (0.783) indicates strong discriminative power, the high number of covariates relative to events (EPV approximately 2) suggests a risk of overfitting in the full model. Fourth, treatment decisions (surgical vs. medical) were individualized by physicians, which may introduce residual confounding despite statistical adjustments. Finally, the generalizability (external validity) of our findings may be limited. As this study was conducted in southwestern China, the patient characteristics, risk factors (e.g., hypertension control), and clinical outcomes may differ from those in other geographic regions or ethnic populations. Nonetheless, this study of 700 patients offers critical insights into the regional prognostic patterns of AAD, contributing significantly to the broader understanding of the disease.
Conclusion
Admission SBP and DBP exhibit significant J-shaped associations with long-term all-cause mortality in AAD, a trend less pronounced in short-term outcomes. We identified a risk-nadir range of 130–160/80–88 mmHg associated with the lowest long-term mortality. These findings suggest that admission hemodynamics serve as a critical prognostic indicator, necessitating a holistic management strategy that balances aortic wall tension reduction against the maintenance of end-organ perfusion.
Data availability
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants but are available from the first author Y.C., [chenyi1109@126.com](mailto: chenyi1109@126.com) upon reasonable request.
Abbreviations
- HTN:
-
Hypertension
- RBC:
-
Red blood cell
- HB:
-
Hemoglobin
- WBC:
-
White blood cell
- NE:
-
Neutrophils
- Lym:
-
Lymphocyte
- FPG:
-
Fasting plasma glucose
- TG:
-
Triglycerides
- TC:
-
Total cholesterol
- HDLC:
-
High-density lipoprotein cholesterol
- LDLC:
-
Low-density lipoprotein cholesterol
- Cr:
-
Creatinine
- UA:
-
Uric acid
- CRP:
-
C-Reactive protein
- NTproBNP:
-
N-terminal pro-B-type natriuretic peptide
- hsTNT:
-
High-sensitivity troponin T
- LVEF:
-
Left ventricular ejection fraction
- LVD:
-
Left ventricular end-diastolic diameter
- IMH:
-
Intramural hematoma
- IRAD:
-
International register of acute aortic dissection
References
Isselbacher, E. M. Thoracic and abdominal aortic aneurysms. Circulation 111, 816–828 (2005).
Kalkan, A. K. et al. The predictive value of admission fragmented QRS complex for in-hospital cardiovascular mortality of patients with type 1 acute aortic dissection. Ann. Noninvasive Electrocardiol. 20 (5), 454–463 (2014).
Tsai, T. T., Nienaber, C. H. & Eagle, K. A. Acute aortic syndromes. Circulation 112, 3802–3813 (2005).
Olsson, C. et al. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 114, 2611–2618 (2006).
Dawber, T. R., Moore, F. E. & Mann, G. V. II. Coronary heart disease in the framingham study. Int. J. Epidemiol. 44 (6), 1767–1780 (2015).
Bangalore, S. et al. J-curve revisited: an analysis of blood pressure and cardiovascular events in the Treating to New Targets (TNT) Trial†. Eur. Heart J. 31 (23), 2897–2908 (2010).
Bossone, E. et al. Presenting systolic blood pressure and outcomes in patients with acute aortic dissection. 71(13). (2018).
Zhang, J., Jiang, Y., Gao, C., Feng, J. & Wang, A. Risk factors for hospital death in patients with acute aortic dissection. Heart Lung Circulation. 24 (4), 348–353 (2015).
Zhang, R. et al. Biomarkers investigation for in-hospital death in patients with stanford type A acute aortic dissection. Int. Heart J. 57 (5), 622–626 (2016).
Yang, G. et al. Admission Systolic Blood Pressure and In-hospital Mortality in Acute Type A Aortic Dissection: A Retrospective Observational Study. Front. Med. (Lausanne). 8, 542212 (2021).
Sari, S. et al. Check the diastolic blood pressure twice in aortic dissection as it is associated with prognosis. Pak J. Med. Sci. 37 (2), 339–344 (2021).
Strachan, D. P. Predictors of death from aortic aneurysm among middle-aged men: The. Whitehall study. Br. J. Surg. 78 (4), 401–404 (1991).
Reed, D., Reed, C., Stemmermann, G. & Hayashi, T. Are aortic aneurysms caused by atherosclerosis? Circulation 85 (1), 205–211 (1992).
Age-specific relevance. of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 360 (9349), 1903–1913 (2002).
Kobeissi, E., Hibino, M., Pan, H. & Aune, D. Blood pressure, hypertension and the risk of abdominal aortic aneurysms: a systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 34 (6), 547–555 (2019).
Hibino, M. et al. Blood pressure, hypertension, and the risk of aortic dissection incidence and mortality: results from the J-SCH study, the UK biobank study, and a meta-analysis of cohort studies. Circulation 145 (9), 633–644 (2022).
Erbel, R. et al. [2014 ESC Guidelines on the diagnosis and treatment of aortic diseases]. Kardiol Pol. 72 (12), 1169–1252 (2014).
Durrleman, S. & Simon, R. Flexible regression models with cubic splines. Stat. Med. 8 (5), 551–561 (1989).
Whelton, P. K., O’Connell, S., Mills, K. T. & He, J. Optimal Antihypertensive Systolic Blood Pressure: A Systematic Review and Meta-Analysis. Hypertension 81 (11), 2329–2339 (2024).
Haykowsky, M. J. et al. Aorta wall stress during exercise in patients with an ascending thoracic aortic aneurysm: insights from a case series. Aorta (Stamford). 12 (5), 108–116 (2025).
Sundt, T. M. Indications for aortic aneurysmectomy: Too many variables and not enough equations? J. Thorac. Cardiovasc. Surg. 145 (3), S126–S129 (2013).
Beller, C. J., Gebhard, M. M., Karck, M. & Labrosse, M. R. Usefulness and limitations of computational models in aortic disease risk stratification. J. Vasc. Surg. 52 (6), 1572–1579 (2010).
Winzap, P. A. et al. Initial systolic blood pressure associates with systemic inflammation, myocardial injury, and outcomes in patients with acute coronary syndromes. Eur. Heart Journal: Acute Cardiovasc. Care. 12 (7), 437–450 (2023).
Sánchez-Enrique, C. et al. Cause and long-term outcome of cardiac tamponade. Am. J. Cardiol. 117 (4), 664–669 (2016).
Orbach, A., Schliamser, J. E., Flugelman, M. Y. & Zafrir, B. Contemporary evaluation of the causes of cardiac tamponade: Acute and long-term outcomes. Cardiol. J. 23 (1), 57–63 (2016).
D’Agostino, R. B., Belanger, A. J., Kannel, W. B. & Cruickshank, J. M. Relation of low diastolic blood pressure to coronary heart disease death in presence of myocardial infarction: the Framingham Study. BMJ 303 (6799), 385–389 (1991).
Böhm, M. et al. Achieved blood pressure and cardiovascular outcomes in high-risk patients: results from ONTARGET and TRANSCEND trials. Lancet 389 (10085), 2226–2237 (2017).
Messerli, F. H. et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann. Intern. Med. 144 (12), 884–893 (2006).
Dell’Aquila, A. M. et al. Malperfusion syndrome in patients undergoing repair for acute type A aortic dissection: Presentation, mortality, and utility of the Penn classification. J. Thorac. Cardiovasc. Surg. 170 (3), 687–697 (2025).
Li, J. W. et al. Longitudinal blood pressure and cardiovascular outcomes in heart failure: An individual patient data pooling analysis of clinical trials. Eur. J. Heart Fail. 27 (9), 1686–1694 (2025).
Shoji-Asahina, A., Usui, T. & Tabara, Y. U-shaped association between blood pressure and all-cause mortality in older adults: the Shizuoka study. J. Hum. Hypertens. 39 (1), 66–71 (2025).
Böhm, M. et al. Myocardial reperfusion reverses the J-curve association of cardiovascular risk and diastolic blood pressure in patients with left ventricular dysfunction and heart failure after myocardial infarction: insights from the EPHESUS trial. Eur. Heart J. 41 (17), 1673–1683 (2020).
Aïdoud, A. et al. High Prevalence of Geriatric Conditions Among Older Adults With Cardiovascular Disease. J. Am. Heart Assoc. 12 (2), e026850 (2023).
Catalano, M. A. et al. Age, sex, and contemporary outcomes in surgical repair of type A aortic dissection: Insights from the National Inpatient Sample. JTCVS Open. 11, 23–36 (2022).
Salem, M. et al. Risk factors for mortality in acute aortic dissection type A: A centre experience over 15 Years. Thorac. Cardiovasc. Surg. 69, 322–328 (2020).
Wang, J. X. et al. The impact of age in acute type A aortic dissection: a retrospective study. J. Cardiothorac. Surg. 17 (1), 40 (2022).
Carrel, T., Sundt, T. M., Von Kodolitsch, Y. & Czerny, M. Acute aortic dissection. Lancet 401 (10378), 773–788 (2023).
Vrsalovic, M., Vrsalovic Presecki, A. & Aboyans, V. N-terminal pro-brain natriuretic peptide and short-term mortality in acute aortic dissection: A meta-analysis. Clin. Cardiol. 43 (11), 1255–1259 (2020).
Talwar, S. et al. Profile of plasma N-terminal proBNP following acute myocardial infarction; correlation with left ventricular systolic dysfunction. Eur. Heart J. 21 (18), 1514–1521 (2000).
Jenab, Y., Ahmadi-Tafti, S. H., Davarpasand, T., Jalali, A. & Khederlou, H. Association of the high-sensitive cardiac troponin T levels and long-term mortality in patients with acute aortic dissection type A. J. Cardiovasc. Thorac. Res. 15 (2), 116–120 (2023).
Ahn, J. M. et al. Differential clinical features and long-term prognosis of acute aortic syndrome according to disease entity. Eur. Heart J. 40 (32), 2727–2736 (2019).
Nazerian, P. et al. Diagnostic performance of the aortic dissection detection risk score in patients with suspected acute aortic dissection. Eur. Heart J. Acute Cardiovasc. Care. 3 (4), 373–381 (2014).
Samet, P. Hemodynamic sequelae of cardiac arrhythmias. Circulation 47 (2), 399–407 (1973).
Acknowledgements
We extended our heartfelt gratitude to the committed personnel at the Affiliated Hospital of Guilin Medical University in Guilin and the People’s Hospital of Guangxi Zhuang Autonomous Region in Nanning, Guangxi, China, for their essential role in the precise and diligent gathering of data.
Funding
This work was supported by the Scientific Research Project of Health Commission of Guangxi Zhuang Autonomous Region (Z-A20230040); Guangxi Science and Technology Base and Special Talents’ Project (GK AD17129026); Guangxi Science and Technology Specialized Project (GKG 14124003-9); Fund Project of Guangxi Zhuang Autonomous Region Health Commission (S2020116-1) and Guangxi Medical and health key cultivation discipline construction project. The funders had no role in the study design, data collection, analysis, interpretation, or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Y.C., QW. J and XW.L. were responsible for study design and planning. XR.S. , XX.P. , N.C. and L.S. contributed to data collection and cleaning. Y.C., LM.Z. and XR.S. contributed to data analysis. Y.C. and XX.P. contributed to writing the original report. QW.J., XW.L. and L.L. contributed to writing-review and editing. All authors read and approved the final version of the article.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The current study was a retrospective study, the nursing follow-up was conducted by staff out of our study team, the personal information for patients was de-identified after data extraction, so no direct patient was involved in this research. Therefore, informed consent from each participant was waived. The waiver of informed consent for the study was approved by the Research Ethics Committee at the People’s Hospital of Guangxi Zhuang Autonomous Region, China (IRB-KY-ZC-2023-049). This study protocol was reviewed and approved by the Research Ethics Committee at the People’s Hospital of Guangxi Zhuang Autonomous Region, China (IRB-KY-ZC-2023-049) as well.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, Y., Peng, X., Ji, Q. et al. Admission blood pressure and mortality in acute aortic dissection: Southwest China multicenter retrospective cohort study. Sci Rep 16, 12798 (2026). https://doi.org/10.1038/s41598-026-43101-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-43101-x
