
Abstract
Canine degenerative myelopathy (DM) is an adult-onset neurodegenerative disease considered a spontaneous model of human amyotrophic lateral sclerosis (ALS). Neuroinflammation occurs in both DM and ALS, and crosstalk between the central nervous system and systemic immunity has been demonstrated in ALS. To investigate this interaction in DM, we analyzed peripheral blood and spinal cord tissues using real-time RT-PCR and immunofluorescence. In peripheral blood, mRNA expression of interleukin (IL)-18 and nod-like receptor protein 3 was significantly increased compared with intervertebral disk herniation controls. IL-10 and caspase-1 were elevated, whereas tumor necrosis factor-α was decreased relative to healthy controls. C–C motif chemokine receptor 2 expression showed a moderate negative correlation with disease duration. Immunofluorescence revealed a few transmembrane protein 119− and mannose receptor C-type 1+ cells, indicating limited infiltration of peripheral blood-derived macrophages into the spinal cord. Transcriptional analysis of spinal cords with different degrees of degeneration showed increased expression of activated astrocyte markers (serping1 and S100A10) and C–C motif chemokine ligand 2 in moderately to severely degenerated tissues. Furthermore, immunohistochemical analysis revealed increased CCL2 protein expression in the affected spinal cords. These findings suggest that systemic immune activation contributes to spinal neuroinflammation in DM, although its limited cellular infiltration implies a minor role in neurodegeneration.
Similar content being viewed by others


Introduction
Canine degenerative myelopathy (DM) is an adult-onset progressive and fatal neurodegenerative disorder. Its histopathological features include axonal loss, demyelination, and neuronal loss of the spinal cord1,2. DM-affected dogs are homozygous for a superoxide dismutase-1 (SOD1) missense mutation3,4. In humans, some cases of familial amyotrophic lateral sclerosis (ALS) are caused by SOD1 gene mutations, sharing similar clinical signs and neuropathologic features with DM. Therefore, DM is considered a spontaneous model of ALS5; however, not all dogs with the genetic mutation develop DM, suggesting that other factors may contribute to the onset of DM.
Although the detailed pathogenesis of DM remains largely unknown, neuroinflammation mediated by glial cells is considered to be vital. An increased number of activated astrocytes and microglia is observed in the spinal cord of patients with DM1. Moreover, increased expression of interleukin (IL)−1β, tumor necrosis factor α (TNFα), C–C motif chemokine ligand 2 (CCL2), and vascular cell adhesion molecule 1 (VCAM1) in the spinal cord tissue has been reported6. The central nervous system is considered isolated from the peripheral immune system; however, evidence indicates that the immune response in the central nervous system actively communicates with the peripheral immune system in mice and humans7,8,9,10. Given the enhanced expression of CCL2 and VCAM1, which promotes macrophage migration into the inflammatory site in DM, some cells considered microglia in the spinal cord of DM may be derived from peripheral monocytes6.
Crosstalk between the central nervous system and systemic immunity has attracted attention in the pathophysiology of ALS11. The peripheral blood inflammatory response is frequently observed in patients with ALS. Moreover, increased numbers of neutrophils, CD4-positive lymphocytes, CD8-positive lymphocytes, and CD16-positive monocytes were observed in the peripheral blood of patients with ALS12. In addition, the levels of the serum inflammatory cytokines TNF-α, IL-1β, IL-6, and IL-8 were increased13,14. These findings suggest a systemic proinflammatory state during ALS. In an ALS mouse model, numerous macrophages infiltrated the spinal cord as the disease progressed. Because infiltrating macrophages indicate a cytotoxic phenotype, these cells considerably contributed to motor neuron loss in the ALS model mice15. However, no studies have demonstrated macrophage infiltration into the spinal cord or a systemic inflammatory state in dogs with DM. Furthermore, although accumulating evidence suggests a potential role of neuroinflammation in exacerbating disease pathology, it remains controversial whether these immune responses are a cause of the disease or merely a consequence of neurodegeneration. Determining whether neuroinflammation and systemic immunity can serve as therapeutic targets is crucial for the development of treatments for DM and ALS.
DM in dogs represents a naturally occurring ALS model that enable the evaluation of disease-associated immune responses in a setting that more closely reflects the physiological disease context of ALS compared with transgenic mouse models. Hypothetically, there is crosstalk between the spinal cord and systemic immunity in DM, resulting in a proinflammatory state that may contribute to disease progression. Therefore, the objective of this study was to identify changes in the transcription of inflammatory genes in the peripheral blood of DM and the infiltration of peripheral blood-derived macrophages into the spinal cord. To investigate whether changes in the transcription of inflammatory genes in the peripheral blood reflect neroinflammatory processes in the spinal cord during disease progression, we also analyzed the transcriptional levels of inflammatory genes in spinal cord tissues with various degrees of degeneration. By evaluating the temporal relationship between inflammatory changes and neuronal degeneration, we determined these inflammatory processes act as primary drivers of neurodegeneration or represent secondary phenomena accompanying disease progression in DM.
Results
Animals
The signalments of the animals are listed in Tables 1 and 2. Blood specimens were collected from 12 DM-affected, 6 inter vertebral disk heriation (IVDH)-affected, and 7 healthy control dogs. A total of 19 blood specimens from DM dogs were analyzed because 3 DM dogs were sampled on two separate occasions and 2 were sampled on 3 separate occasions. All 12 DM dogs included in the gene expression analysis were Pembroke Welsh Corgis (PWC), and all 7 healthy control dogs were Beagles. The IVDH dogs included two Beagles and one Miniature Dachshund, French Bulldog, Toy Poodle, and Yorkshire Terrier. The median ages of the DM, IVDH, and healthy control dogs during sample collection were 10 years and 11 months (range: 9 years and 5 months to 14 years), 9 years and 10.5 months (range: 5 years to 12 years and 8 months), and 7 years and 10 months (range: 6 years and 11 months to 9 years and 1 month), respectively. Of the 12 dogs, 10 were diagnosed with DM by postmortem histopathological examination. The remaining 2 dogs were diagnosed clinically. Based on previosuly described disease staging system that used clinical smptoms, eight samples were obtained at stage 1 (upper motor neuron paraparesis and general proprioceptive ataxia in pelvic limbs), eight samples at stage 2 (nonambulatory paraparesis to paraplegia in pelvic limbs), two samples at stage 3 (lower motor neuron paraplegia in pelvic limbs to thoracic limb paresis), and one sample at stage 4 (lower motor neuron tetraplegia and brain stem signs)16. Five of the IVDH dogs were grade 2, and one was grade 4 based on the modified Frankel scales17.
All of the DM samples used for immunofluorescence were from PWC that died of respiratory impairment resulting from DM. They were diagnosed by postmortem histopathological examination. Three non-DM tissues were from two Beagles and one Miniature Dachshund. A Beagle and a Miniature Dachshund died of non-neural malignant tumors, and the other Beagle was euthanized for an unrelated research project. The median ages of the DM and non-DM dogs were 14 years and 5 months (range: 13 years and 3 months to 16 years and 1 month) and 10 years and 4 months (range: 7 years and 6 months to 11 years and 4 months), respectively.
The cervical and thoracic spinal cords of 10 DM-affected, 5 DM-naive, and 8 non-DM control dogs were used for real-time RT-PCR analysis of glial cell markers. Two DM-naive dogs died of non-neural malignant tumors, two of pneumonia, and one was euthanized because of soft tissue tumor invasion into the spinal canal at T5–6. The T12 spinal cord was used for analyzing this dog. Two control dogs died of a malignant tumor and one of heart failure. Another five control dogs were euthanized for unrelated research projects. All DM-affected and DM-naive dogs were PWC. The control dogs included five Beagles and one Maltese, Miniature Dachshund, and Labrador Retriever. The median ages of the DM-affected, DM-naive, and healthy control dogs were 14 years (range: 11 years and 8 months to 16 years, 1 month), 11 years and 10 months (range: 8 years and 2 months to 15 years), and 9 years and 3 months (range: 6 years and 6 months to 11 years and 4 months), respectively.
Complete blood count and C-reactive protein concentration
Complete blood counts and C-reactive protein (CRP) concentration of the DM dogs were obtained at 13 and 12 of 19 timepoints, respectively. No increase in white blood cell count was observed (median, 10,000/µL; range, 5,100–14,500/µL; reference interval [RI], 6,000–17,000/µL). The lymphocyte count (median, 1,200/µL; range, 500–2,600/µL; RI, 1,000–4,800/µL) and monocyte count (median, 300/µL; range, 0–600/µL; RI, 150–1,350/µL) were also unchanged. The neutrophil count (median, 8,400/µL; range, 4,600–13,500/µL; RI, 3,000–11,800/µL) was not increased except in one case. Only one dog exhibited a mild increase in neutrophil count (13,500/µL) without an elevated white blood cell count or CRP concentration. No correlation was evident between the white blood cell or monocyte count and months from disease onset (Fig. 1). None of the DM dogs showed increased CRP concentrations (median, 0.05 mg/dL; range, 0–0.25 mg/dL; RI, < 0.7 mg/dL).

Correlation between white blood count, monocyte count, and duration from disease onset. Dot plot showing the relationship between white blood cell or monocyte count and months from disease onset. Correlations were determined using Spearman’s rank correlation analysis (n = 13). Neither white blood cell count nor monocyte count was significantly correlated with disease duration (p = 0.76 and p = 0.38, respectively).
Expression of peripheral inflammatory genes
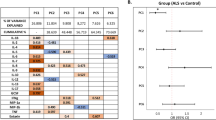
For group comparisons, only the final samples collected from each DM dog were used. The median age final sample collection was 10 years and 10.5 months (range: 10 years and 5 months–14 years). The distribution of the clinical stages at final sample collection was as follows: stage 1 (n = 4), stage 2 (n = 5), stage 3 (n = 2), and stage 4 (n = 1). The expressions of IL-10 and caspase 1 were significantly increased in DM dogs compared with healthy controls (p = 0.04 and 0.02, respectively). The expression of IL-18 and nod-like receptor 3 (NLRP3) were increased in DM dogs compared with IVDH dogs (p = 0.02 and 0.03, respectively) (Fig. 2), whereas C–C motif chemokine receptor 2 (CCR2) expression exhibited a moderate negative correlation with months from disease onset (p = 0.005, r = − 0.63) (Fig. 2). No correlation was observed between the other genes and months from disease onset. The association with clinical stage could not be evaluated because of the small sample size in stages 3 and 4.

Results of real-time RT-PCR analysis of peripheral blood. (A) IL-10 and caspase 1 expression were significantly increased in DM dogs compared with healthy controls (p = 0.04 and p = 0.02, respectively). IL-18 and NLRP3 expression were increased in DM dogs compared with IVDH dogs (p = 0.02 and p = 0.03, respectively). Statistical comparisons among groups were performed using the Steel–Dwass test (DM: n = 12; healthy controls: n = 7; IVDH: n = 6). Each box represents the interquartile range, and the line within the box indicates the median. *p < 0.05. (B) Dot plot showing the relationship between CCR2 expression and months from disease onset. Correlations were assessed using Spearman’s rank correlation analysis (n = 19). The black bar represents the approximate line. CCR2 expression exhibited a moderate negative correlation with months from disease onset (p = 0.005, r = − 0.63). DM, degenerative myelopathy; IVDH, intervertebral disk herniation; IL, interleukin; TNFα, tumor necrosis factor α; CCR2, C–C motif chemokine receptor 2; NLRP3, nod-like receptor protein 3.
The expression of several genes, including IL-6, interferon-γ, and IL-4, was undetectable, although the specificity of the primers was confirmed in a previous study by our group18. The expression of some inflammatory cytokines may be much lower in the peripheral blood.
Immunofluorescence
Transmembrane protein 119 (TMEM119) is a microglia-specific marker and is not expressed on peripheral blood-derived macrophages19. Mannose receptor C-type 1 (MRC1) is a marker of perivascular spinal macrophages, which include microglia and peripheral blood-derived macrophages20. Therefore, TMEM119−/MRC1+ cells are considered likely to represent infiltrating macrophages derived from peripheral monocytes. In the DM specimens, numerous TMEM119+/MRC1+ cells were present in all areas of the spinal cord, which is consistent with a previous report6; however, systematic quantification of these double-positive microglia was beyond the scope of the present study. Although TMEM119−/MRC1+ cells were absent in control dogs, a very small number were detected in the white matter of DM-affected dogs. The median number of TMEM119−/MRC1+ cells per entire transverse section was 2 (range: 2–3 cells) in the cervical cord of DM-affected dogs. The median number of TMEM119−/MRC1+ cells per entire transverse section was 2 (range: 1–3 cells) in the thoracic cord of DM-affected dogs. In the spinal cords from the control dogs, only TMEM119+/MRC1+ cells were observed (Fig. 3).

Immunofluorescence of TMEM119 and MRC1 in the cervical and thoracic spinal cord. A small number of TMEM119−/MRC1+ cells were observed in the white matter of the cervical and thoracic cords of the DM group (arrow). TMEM119+/MRC1+ cells were detected in the cervical cords of DM and non-DM dogs (arrowhead). Scale bar = 20 μm. Nuclei were counterstained with DAPI. DM, degenerative myelopathy; TMEM119, transmembrane protein 119; MRC1, mannose receptor C-type 1.
Transcriptional and immunohistochemical analyses of phenotype markers of glial cells and chemokines in the spinal cord
To determine whether the alterations in neuroinflammatory markers corresponded to the progression of the disease, the expression of phenotype markers of glial cells and chemokines in the spinal cord was compared among four groups: the cervical and caudal thoracic cord of DM-affected dogs, the caudal thoracic cord of DM-naive dogs, and the cervical cord of control dogs (Fig. 4). The degree of degeneration is most severe in the thoracic spinal cord of the DM-affected dogs, followed in order by the cervical spinal cord of DM-affected dogs and the thoracic spinal cord of DM-naive dogs1,21. Therefore, the severity of spinal cord degeneration was classified as follows: the thoracic cord of DM-affected dogs was considered severe, followed by the cervical cord of DM-affected dogs was moderate, the thoracic cord of DM-naive dogs was mild, and the cervical cord of non-DM control dogs was nondegenerated. The expression of neurotoxic (A1) astrocyte maker (Serping1), neuroprotective (A2) astrocyte marker (S100A10), neurotoxic (M1) microglial markers (IL-1β and inducible nitric oxide synthase [iNOS]), neuroprotective (M2) microglial markers (brain-derived neurotrophic factor [BDNF], nerve growth factor [NGF], and arginase-1 [Arg1]), and chemokine involved in monocyte migration (CCL2) was measured. Serping1 expression was significantly increased in severe and moderate lesions compared with the nondegenerated lesions (p = 0.005 and 0.04, respectively). The expression of S100A10 and CCL2 was significantly increased in severe lesions compared with that in the nondegenerated lesions (p = 0.03 and 0.03, respectively). IL-1β appeared to be upregulated in severe and moderate lesions compared with the nondegenerated lesions; however, the difference was not statistically significant.

Transcriptional and immunohistochemical analyses in the spinal cord with varying degrees of degeneration. (A) The expression of Serping1 was significantly increased in the severe and moderate lesions compared with the nondegenerated lesions (p = 0.005 and p = 0.04, respectively). S100A10 and C–C motif chemokine ligand 2 (CCL2) expression were significantly increased in the severe lesions compared with the nondegenerated lesions (p = 0.03 and p = 0.03, respectively). Statistical comparisons among groups were performed using the Steel–Dwass multiple comparison test (nondegenerated lesion: n = 8; mild degenerated lesion: n = 5; moderate degenerated lesion: n = 10; severe degenerated lesion: n = 10). Nondegenerated lesions (labeled as “none” in the figure) correspond to non-DM control dogs; mild lesions correspond to DM-naive dogs; moderate lesions correspond to the cervical cord of DM-affected dogs; and severe lesions correspond to the thoracic cord of DM-affected dogs. Each box represents the interquartile range, and the line within the box indicates the median. *p < 0.05. (B) Immunofluorescence of CCL2 in dorsal funiculi. Scale bar = 20 μm. Nuclei were counterstained with DAPI. Increased CCL2 immunoreactivity was observed in the clinically affected DM cases compared with the non-DM and DM-naive controls. IL, interleukin; iNOS, inducible nitric oxide synthase; Arg1, arginase-1; BDNF, brain-derived neurotrophic factor; NGF, nerve growth factor; CCL2, C–C motif chemokine ligand 2.
To complement the transcriptional findings, an immunohistochemical analysis of CCL2 protein expression was performed in the spinal cord. Representative sections from non-DM controls, DM-naive cases, and dogs with clinically affected DM (cervical and thoracic spinal cord) were evaluated. Qualitative assessment revealed increased CCL2 immunoreactivity in the DM-affected spinal cords compared with non-DM and DM-naive cases, which is consistent with the transcriptional upregulation measured by real-time RT-PCR (Fig. 4).
Discussion
Neuroinflammation is characterized by microglial aggregation and astrocyte activation, and is one of the pathological feature of DM 1. To date, it is unclear whether crosstalk between the central nervous system and systemic immunity exists in DM. In this study, the infiltration of peripheral monocytes into the spinal cord of patients with DM, although small in number, suggested that neuroinflammation is related to systemic immunity. In contrast, the expression of some inflammation-related genes in the peripheral blood did not indicate that systemic immunity was in a proinflammatory state.
We used IVDH as a disease control and analyzed inflammation-related gene expression in the peripheral blood because IVDH causes compressive spinal injury with clinical signs similar to the early stages of DM. Moreover, PWC is a predominant breed for IVDH, and we often observe mild IVDH complications at necropsy or MRI examination of DM dogs22. Compared with IVDH, NLRP3 and IL-18 expression was increased in DM. In addition, caspase 1 was increased in DM dogs compared with the healthy controls. NLRP3 is expressed in immune-stimulated monocytes, macrophages, dendritic cells, and splenic neutrophils. When monocytes recognize antigens, such as pathogen-associated molecular patterns and danger-associated molecular patterns by the Toll-like receptor, NLRP3 forms an inflammasome with caspase1, leading to its activated23. This triggers the production of the proinflammatory cytokines IL-1β and IL-1824. Therefore, our findings suggest the activation of peripheral monocytes in DM dogs. Monocyte and microglial activation can be divided into cytotoxic M1 and neuroprotective M2 cells. Based on the increased transcription of NLRP3, caspase1, and IL-18, monocytes may be in a proinflammatory M1 state in DM, as reported in patients with ALS15. Microglia expressing mutant SOD1, which was isolated from mutant SOD1 transgenic mice, are also activated for NLRP3-mediated cytokine production25. Although the mechanism underlying increased NLRP3 expression in the peripheral blood of DM dogs is unclear, mutant SOD1 expressed in monocytes may have contributed to this upregulation. Although monocyte activation was suspected, the expression level of IL-10 was increased in DM dogs compared with healthy controls. Increased IL-10 levels may reflect active suppression of proinflammatory signaling through IL-10 mediated pathway, such as STAT3 activation26. This could represent a feedback mechanism aimed at limiting peripheral inflammation and may indicate an immune-regulatory skewing that differs from the cytotoxic profiles observed in human ALS13. It should be noted that the observed changes in gene expression may not directly correspond to protein level or biological activity. Further studies involving protein quantification and functional assay of monocytes and cytokines would be necessary to validate these transcriptional changes.
CCR2 is a major chemotactic receptor on monocytes that responds to CCL227. A previous study demonstrated that chemoattraction through CCL2–CCR2 recruits monocytes into the spinal cord in ALS model mice15. Notably, despite increased CCL2 gene expression in the severely degenerated spinal cord, which was supported by increases in CCL2 protein immunoreactivity on immunohistochemical analysis, CCR2 expression in the peripheral blood decreased as the disease progressed. In this study, only whole blood was analyzed, and CCR2 expression in isolated monocyte was not specifically assessed. However, because the monocyte count did not decrease with the progression of DM, the reduction of CCR2 in the peripheral blood may reflect decreased expression by monocytes rather than decreasing its numbers. Peripheral blood contains a subset of monocytes with low CCR2 expression, which are primarily involved in patrolling rather than active recruitment to inflammatory sites28. Accordingly, the reduced CCR2 gene expression may indicate an alteration in monocyte subset, which in turn could contribute to the limited spinal cord infiltration in DM. Evidently, patients with ALS show decreased expression of CCR2 in peripheral monocytes29. Although the mechanism underlying the downregulation of CCR2 expression in monocytes remains unclear, the previous report revealed that it may not be due to receptor–ligand interaction. The downregulation of CCR2 has been implicated in the prolonged survival of patients with ALS29. Thus, decreased CCR2 expression may serve to attenuate excessive inflammation, which could, in part, account for delayed progression of neurodegeneration. Although protein-level expression of CCR2 was not evaluated in our research for targeting DM, similar pathological mechanisms to those in ALS may be present.
As indicated above, decreased CCR2 expression may limit the recruitment of circulating monocytes into the spinal cord during DM progression. Consistently, only a very small number of TMEM119−/MRC1+ cells, which are presumed to represent peripheral blood–derived macrophages, were obtained per entire transverse section in end-stage DM dogs. Although the presence of these cells suggests an interaction between systemic immunity and neuroinflammation, the limited number indicates that peripheral monocyte infiltration is unlikely to be a major driver of neurodegeneration in DM. This finding contrasts with the results in ALS model mice, in which robust infiltration of proinflammatory macrophages was reported, which may contribute substantially to motor neuron loss15. In contrast, studies of human ALS spinal cord tissue have indicated that infiltrating monocytes/macrophages are present but relatively sparse, with approximately a dozen cells per Sects30,31.. The degree of monocyte infiltration observed in DM dogs in the present study more closely resembles that reported in human ALS compared with ALS model mice. Because ALS model mice are produced by overexpression of mutant proteins, inflammatory responses in these models may not fully reflect the complex, heterogeneous pathophysiology of naturally occurring disease32. Therefore, the results in DM dogs suggest that peripheral monocyte infiltration may play a more limited role in spontaneous ALS-like neurodegeneration than has been gleaned from transgenic mouse models.
Real-time RT-PCR analysis of the spinal cord tissues revealed an increase in Serping1 and S100A10 expression in the spinal cord in which degeneration was more severe. These results indicate that cytotoxic (A1) and neuroprotective (A2) type astrocytes increase as the DM stage progresses, and the increase in activated astrocytes is consistent with the pathological findings33. Conversely, no significant differences were detected in markers of activated microglia, despite the presence of increased activated microglia in histological findings of DM spinal cord6. A1 astrocytes are known to be induced by cytokines secreted by M1 microglia34. These discrepancies may be due to cellular heterogeneity in whole spinal cord samples, potentially obscuring focal microglial activation. Immunohistochemical or single-cell analyses with extracted microglia are needed to assess the microglial phenotype. Importantly, the lack of significant upregulation of the marker of reactive A1 astrocyte in DM-naive dogs, which already show mild neurodegeneration, argues against a primary role of glial mediated neuroinflammation in initiating pathology21. If glial activation were causative, one would expect robust activation of neuroinflammatory markers even at the early preclinical stage. The absence of such early upregulation suggests that glial activation is more likely a secondary response to ongoing neurodegeneration rather than its initiating cause. Moreover, CCL2 upregulation was primarily observed in more advanced stages of DM. Based on the role of CCL2 in immune cell recruitment, its late-stage increase may reflect a secondary reactive response to progressive tissue degeneration rather than an initiating pathogenic mechanism. This is consistent with the absence of robust early glial activation in DM-naive cases and supports the concept that that neuroinflammation in DM is predominantly reactive. In previous studies of DM and ALS, it was debated whether neuroinflammation is a primary pathogenic trigger or a secondary consequence of neuronal injury. Our results support the latter interpretation, indicating that in a spontaneous animal model of ALS-like disease, glial activation may represent a secondary reactive process. This distinction has important implications for translational strategies targeting neuroinflammation in ALS and DM.
A major limitation of this study is that the cytokines in the peripheral blood can be influenced by other diseases. Complications, such as pressure ulcers and cystitis, are also common in end-stage DM cases. In this study, only cases with no other diseases in the medical record were included, to minimize the potential influence of complications on cytokine levels. In addition, there were no cases with increased white blood cell counts or CRP concentrations. A second limitation is that DM-naive dogs with SOD1 mutations were used as models for the early stages of DM. DM-affected dogs are rarely euthanized in Japan, and dogs heterozygous for the SOD1 mutation suffer from mild neurodegeneration21. It is confirmed that the spinal cord of the DM-naive dogs used in this study also exhibited mild spinal degeneration. Therefore, we selected DM-naive dogs with SOD1 mutations as a model for early stages. A third limitation of this study is that the DM, IVDH, and healthy control groups were not strictly matched for age and breed. Blood samples from healthy controls were collected from dogs housed at the university, which made it difficult to match the age and breed of the DM cohort. In addition, dogs with IVDH tended to present at a younger age compared with DM dogs, further complicating precise age matching among groups22. Because genetic background and age may affect immune-related parameters, we cannot completely exclude confounding effects; however, age was not significantly correlated with the measured variables. In addition, because approximately 80% of older PWCs are homozygous or heterozygous for the SOD1 gene mutation in Japan, collecting specimens from SOD1 wild-type PWCs was difficult35. Another limitation of this study is that inflammatory cytokines were not quantified at the protein level in peripheral blood. Measurement of circulating cytokine concentrations would have provided complementary information regarding systemic immune activation; however, sufficient serum samples were not available for protein analyses. In addition, unbiased transcriptomic approaches, such as RNA sequencing, were not performed, which could provide insight into the molecular pathways involved in neuroinflammation and neurodegeneration in DM. Future studies incorporating protein-level analyses and transcriptome-wide approaches will be important to clarify the role of immune responses in disease progression.
To our knowledge, this is the first report to analyze the expression of inflammatory genes in the peripheral blood and monocyte infiltration in the spinal cord of dogs with DM. The peripheral blood analyses indicated that NLRP3-mediated monocyte activation occurs in DM. However, the anti-inflammatory response was activated simultaneously. In fact, only a small number of TMEM119−/MRC1+ cells, which are presumably derived from peripheral monocytes, were observed in the spinal cord of patients with DM. The rarity of infiltrating monocytes suggests the possibility that these cells do not play a direct causal role in neurodegeneration. Moreover, the transcriptional analysis of spinal cord tissues indicated that glial cells are activated as degeneration progresses. The lack of significant upregulation of activated glial cell markers in spinal cords with only mild neurodegeneration suggests that glial-mediated neuroinflammation occur secondary to neuronal degeneration. Consistent with this interpretation, CCL2 expression was primarily increased in clinically affected DM cases, whereas no marked upregulation was observed in DM-naive dogs. Because of the established role of CCL2 in microglial and monocyte recruitment, its late-stage elevation further supports the notion that chemokine-driven immune activation is a response to ongoing tissue injury rather than an initiating pathogenic event. These results differ from observations in certain transgenic ALS mouse models, in which inflammatory activation precedes or accelerates neurodegeneration. Importantly, our results refine the understanding of DM pathophysiology by delineating the temporal and cellular characteristics of inflammatory responses. Although systemic and central immune alterations occur, there was no evidence indicating that they directly promote progression. These findings suggest that immune activation in DM may represent secondary or compensatory processes. Elucidating the sequence of neurodegeneration and neuroinflammation is essential for developing therapeutic strategies that target the immune response without disrupting potentially protective mechanisms.
Methods
Animals
We reviewed the clinical and necropsied dog records stored at Gifu University from January 2012 to December 2018. All dogs were enrolled in the study with their owners’ permission. All DM dogs were PWC and confirmed to carry the homozygous C.118G > A missense mutation (A/A). The genotypes were determined using real-time PCR as described previously36. DM dogs were diagnosed by postmortem histopathological examination or using clinical information, which combined the clinical signs, clinical examination, including magnetic resonance imaging and computed tomography to exclude other diseases, gene mutation, and clinical course until death. Dogs diagnosed with IVDH were enrolled as disease controls. IVDH was diagnosed using a combination of clinical signs, radiography, magnetic resonance imaging, and computed tomography. Healthy dogs with no clinical signs were included as controls for peripheral blood analyses. Cases of DM and IVDH concurrent with other diseases noted in the medical record were excluded. DM dogs were not given any medications for DM other than supplement products throughout the treatment period.
For the analysis of spinal cord tissues, non-DM dogs with no SOD1 gene mutations and who were euthanized for an unrelated research project or died from non-neural diseases were included. In addition, PWCs that were homozygous or heterozygous for the SOD1 gene mutation that did not show neurological signs before death were included as DM-naive controls.
Collection of the blood specimens
Blood specimens were collected from DM- or IVDH-affected dogs and healthy control dogs into PAXgene Blood RNA tubes (PreAnalytiX, Hombrechtikon, Switzerland). Blood samples from DM dogs were collected at the time of diagnosis or during follow-up visits, whereas samples from IVDH dogs were collected only at the time of diagnosis. Only the final sample obtained from each dog was included in the comparisons of DM, IVDH, and the healthy control groups. For the correlation analyses with disease duration, repeat samples from the same individuals were included to reflect longitudinal changes over time. All samples were incubated at room temperature for at least 2 h and stored at − 20 °C until further analysis. The collection of blood specimens was approved by the institutional committee. All procedures were performed based on the guidelines regulating animal use and ethics at Gifu University (approval number 16090).
The complete blood counts and CRP concentrations of the DM samples during blood collection were reviewed, if available from the clinical data.
Spinal cord tissue collection
Spinal cord tissues were collected from DM and DM-naive PWCs and non-DM dogs. For real-time RT-PCR, the spinal cord tissues from dogs who died within 24 h were collected in RNAlater® (Sigma-Aldrich, STL, USA) and stored at − 20 °C. For immunofluorescence analysis, the spinal cord tissues were embedded in optimal cutting temperature compound and stored at − 80 °C.
Real-time RT-PCR
Total RNA was isolated from the blood specimens using the PAXgene Blood RNA Kit (PreAnalytiX). Total RNA from the spinal cord tissues was isolated using the RNeasy® Lipid Tissue Mini Kit (Qiagen, Venlo, Netherlands). Genomic DNA was removed using the TURBO DNA-free™ Kit (Applied Biosystems, CA, USA). Ethanol precipitation was performed for the blood specimens using the Dr.GenTLE™ Precipitation Carrier (Takara Bio, Inc., Shiga, Japan). Total RNA was reverse-transcribed into cDNA using ReverTra Ace α® (TOYOBO, Osaka, Japan). Two-step real-time RT-PCR was performed using TB Green® Premix Ex Taq™ Ⅱ (Takara Bio Inc). The expression of 10 canine genes associated with inflammation in the peripheral blood was analyzed and included IL-1β, IL-4, IL-6, IL-10, IL-18, TNFα, interferon-γ, CCR2, NLRP3, and caspase 1. Two genes (CG148980 and TBP) were used as reference genes. The expression of neurotoxic and neuroprotective glial cell markers and chemokines in the spinal cord tissues was analyzed. These included IL-1β, Serping1, S100A10, iNOS, Arg1, BDNF, NGF, and CCL2. Two genes (RPL32 and TBP) were used as references. The primer sequences are listed in Table 2. Amplification was performed using a Thermal Cycler Dice® Real Time System Ⅲ (Takara Bio) and comprised an activation step (95 °C for 10 s), followed by 40 cycles of PCR (95 °C and 60 °C for 5 and 30 s) and dissociation (95 °C, 60 °C, and 95 °C for 15, 30, and 15 s, respectively). The cycle threshold (Ct) values for each mRNA were subtracted from the geometric mean of the Ct values of the two reference genes (ΔCt). All samples were measured in duplicate, and the mean value of the ΔCt was calculated. The expression of each mRNA was calculated by 2−ΔCt, resulting in the evaluation of samples as n-fold differences from the mean value of the two reference genes.
Immunofluorescence of the spinal cords
To determine whether macrophages infiltrate into the spinal cord during DM and to evaluate CCL2 protein expression within the affected tissue, we performed an immunofluorescence assay. Optimal cutting temperature compound-embedded frozen sections containing caudal cervical and caudal thoracic spinal cords were prepared from four DM and three non-DM control dogs. The sections were cut at 10 μm and fixed by immersion in 4% paraformaldehyde for 15 min. The sections were blocked with 10% normal goat serum in phosphate-buffered saline conataing 0.05% Tween 20. For macrophage analysis, the sections were incubated with anti-TMEM119 mouse monoclonal antibody (1:200) (Proteintech, Philadelphia, PA, USA) and anti-MRC1 rabbit polyclonal antibody (1:200) (Bioss Inc, Woburn, MA, USA) at room temperature for 1 h. For CCL2, the sections were incubated overnight at 4 °C with anti-CCL2 mouse monoclonal antibody (1:100) (R&D Systems, Minneapolis, MN, USA). the sections were then incubated with Alexa Fluor® 488-conjugated goat anti-mouse immunoglobulin secondary antibody (1:500) (Thermo Fisher Scientific, Waltham, MA, USA) and Alexa Fluor® 594-conjugated goat anti-rabbit immunoglobulin secondary antibody (1:500) (Thermo Fisher Scientific) at room temperature for 1 h. The nuclei were stained with DAPI. Fluorescence images of the spinal white and gray matter were captured under a fluorescence microscope (BZ-X810, Keyence, Osaka, Japan).
Statistical analyses
Comparison of inflammatory gene expression in the peripheral blood among the DM, IVDH, and healthy control dogs was performed using the Steel–Dwass test because the sample sizes for the IVDH and healthy control groups were small and normality was not determined. Correlations between the expression of each gene and the duration from DM onset were determined using Pearson’s correlation coefficient, as the normality of the variables was confirmed using the Shapiro–Wilk test. The real-time RT-PCR results for the spinal cord tissues were compared between the non-DM controls, DM-naive dogs, and the cervical and thoracic spinal cords of DM-affected dogs using the Steel–Dwass test. The confidence interval was 95%, and significance was set at p < 0.05. Statistical analyses were conducted using JMP® Pro 17.0.0 software (SAS Institute, Cary, NC, USA).
Data availability
All data generated for this study are available upon request from the corresponding author.
Abbreviations
- ALS:
-
amyotrophic lateral sclerosis
- Arg1:
-
Arginase-1
- BDNF:
-
Brain-derived neurotrophic factor
- CCL2:
-
CC motif chemokine ligand 2
- CCR2:
-
C-C motif chemokine receptor 2
- DM:
-
degenerative myelopathy
- IL:
-
interleukin
- iNOS:
-
inducible nitric acid synthase
- MRC1:
-
mannose receptor C-type 1
- NGF:
-
Nerve growth factor
- NLRP3:
-
nod-like receptor protein 3
- TMEM119:
-
transmembrane protein 119
- TNFα:
-
tumor necrosis factorα
- RI:
-
reference interval
References
March, P. A. et al. Degenerative myelopathy in 18 Pembroke Welsh Corgi dogs. Vet. Pathol. 46, 241–250. https://doi.org/10.1354/vp.46-2-241 (2009).
Ogawa, M. et al. Neuronal loss and decreased GLT-1 expression observed in the spinal cord of Pembroke Welsh Corgi dogs with canine degenerative myelopathy. Vet. Pathol. 51, 591–602. https://doi.org/10.1177/0300985813495899 (2014).
Awano, T. et al. Genome-wide association analysis reveals a SOD1 mutation in canine degenerative myelopathy that resembles amyotrophic lateral sclerosis. Proc. Natl. Acad. Sci. U S A. 106, 2794–2799. https://doi.org/10.1073/pnas.0812297106 (2009).
Wininger, F. A. et al. Degenerative myelopathy in a Bernese Mountain Dog with a novel SOD1 missense mutation. J. Vet. Intern. Med. 25, 1166–1170. https://doi.org/10.1111/j.1939-1676.2011.0760.x (2011).
Nardone, R. et al. Canine degenerative myelopathy: a model of human amyotrophic lateral sclerosis. Zool. (Jena). 119, 64–73. https://doi.org/10.1016/j.zool.2015.09.003 (2016).
Hashimoto, K. et al. Up-regulated inflammatory signatures of the spinal cord in canine degenerative myelopathy. Res. Vet. Sci. 135, 442–449. https://doi.org/10.1016/j.rvsc.2020.11.001 (2021).
Carson, M. J., Doose, J. M., Melchior, B., Schmid, C. D. & Ploix, C. C. CNS immune privilege: hiding in plain sight. Immunol. Rev. 213, 48–65. https://doi.org/10.1111/j.1600-065X.2006.00441.x (2006).
Ley, K., Laudanna, C., Cybulsky, M. I. & Nourshargh, S. Getting to the site of inflammation: the leukocyte adhesion cascade updated. Nat. Rev. Immunol. 7, 678–689. https://doi.org/10.1038/nri2156 (2007).
Appel, S. H., Beers, D. R. & Henkel, J. S. T cell-microglial dialogue in Parkinson’s disease and amyotrophic lateral sclerosis: are we listening? Trends Immunol. 31, 7–17. https://doi.org/10.1016/j.it.2009.09.003 (2010).
Zigmond, R. E. & Echevarria, F. D. Macrophage biology in the peripheral nervous system after injury. Prog Neurobiol. 173, 102–121. https://doi.org/10.1016/j.pneurobio.2018.12.001 (2019).
McCauley, M. E. & Baloh, R. H. Inflammation in ALS/FTD pathogenesis. Acta Neuropathol. 137, 715–730. https://doi.org/10.1007/s00401-018-1933-9 (2019).
Murdock, B. J. et al. Correlation of Peripheral Immunity With Rapid Amyotrophic Lateral Sclerosis Progression. JAMA Neurol. 74, 1446–1454. https://doi.org/10.1001/jamaneurol.2017.2255 (2017).
Lu, C. H. et al. Systemic inflammatory response and neuromuscular involvement in amyotrophic lateral sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 3, e244. https://doi.org/10.1212/NXI.0000000000000244 (2016).
Hu, Y. et al. Increased peripheral blood inflammatory cytokine levels in amyotrophic lateral sclerosis: a meta-analysis study. Sci. Rep. 7, 9094. https://doi.org/10.1038/s41598-017-09097-1 (2017).
Butovsky, O. et al. Modulating inflammatory monocytes with a unique microRNA gene signature ameliorates murine ALS. J. Clin. Invest. 122, 3063–3087. https://doi.org/10.1172/JCI62636 (2012).
Shelton, G. D. et al. Degenerative myelopathy associated with a missense mutation in the superoxide dismutase 1 (SOD1) gene progresses to peripheral neuropathy in Pembroke Welsh corgis and boxers. J. Neurol. Sci. 318, 55–64. https://doi.org/10.1016/j.jns.2012.04.003 (2012).
Davies, J. V. S. & N. J., H. A comparison of conservative treatment and fenestration for thoracolumbar intervertebral disc disease in the dog. J. Small Anim. Pract. 24, 721–729. https://doi.org/10.1111/j.1748-5827.1983.tb00360.x (1983).
Maeda, S., Shibata, S., Chimura, N. & Fukata, T. House dust mite major allergen Der f 1 enhances proinflammatory cytokine and chemokine gene expression in a cell line of canine epidermal keratinocytes. Vet. Immunol. Immunopathol. 131, 298–302. https://doi.org/10.1016/j.vetimm.2009.04.012 (2009).
Satoh, J. et al. TMEM119 marks a subset of microglia in the human brain. Neuropathology 36, 39–49. https://doi.org/10.1111/neup.12235 (2016).
Goldmann, T. et al. Origin, fate and dynamics of macrophages at central nervous system interfaces. Nat. Immunol. 17, 797–805. https://doi.org/10.1038/ni.3423 (2016).
Kobatake, Y. et al. Localization of a mutant SOD1 protein in E40K-heterozygous dogs: Implications for non-cell-autonomous pathogenesis of degenerative myelopathy. J. Neurol. Sci. 372, 369–378. https://doi.org/10.1016/j.jns.2016.10.034 (2017).
Aikawa, T., Fujita, H., Kanazono, S., Shibata, M. & Yoshigae, Y. Long-term neurologic outcome of hemilaminectomy and disk fenestration for treatment of dogs with thoracolumbar intervertebral disk herniation: 831 cases (2000–2007). J. Am. Vet. Med. Assoc. 241, 1617–1626. https://doi.org/10.2460/javma.241.12.1617 (2012).
Guarda, G. et al. Differential expression of NLRP3 among hematopoietic cells. J. Immunol. 186, 2529–2534. https://doi.org/10.4049/jimmunol.1002720 (2011).
Shao, B. Z., Xu, Z. Q., Han, B. Z., Su, D. F. & Liu, C. NLRP3 inflammasome and its inhibitors: a review. Front. Pharmacol. 6, 262. https://doi.org/10.3389/fphar.2015.00262 (2015).
Meissner, F., Molawi, K. & Zychlinsky, A. Mutant superoxide dismutase 1-induced IL-1beta accelerates ALS pathogenesis. Proc. Natl. Acad. Sci. U S A. 107, 13046–13050. https://doi.org/10.1073/pnas.1002396107 (2010).
Iyer, S. S. & Cheng, G. Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Crit. Rev. Immunol. 32, 23–63. https://doi.org/10.1615/critrevimmunol.v32.i1.30 (2012).
Fuentes, M. E. et al. Controlled recruitment of monocytes and macrophages to specific organs through transgenic expression of monocyte chemoattractant protein-1. J. Immunol. 155, 5769–5776 (1995).
Shi, C. & Pamer, E. G. Monocyte recruitment during infection and inflammation. Nat. Rev. Immunol. 11, 762–774. https://doi.org/10.1038/nri3070 (2011).
Zhang, R. et al. MCP-1 chemokine receptor CCR2 is decreased on circulating monocytes in sporadic amyotrophic lateral sclerosis (sALS). J. Neuroimmunol. 179, 87–93. https://doi.org/10.1016/j.jneuroim.2006.06.008 (2006).
Henkel, J. S. et al. Presence of dendritic cells, MCP-1, and activated microglia/macrophages in amyotrophic lateral sclerosis spinal cord tissue. Ann. Neurol. 55, 221–235. https://doi.org/10.1002/ana.10805 (2004).
Zondler, L. et al. Peripheral monocytes are functionally altered and invade the CNS in ALS patients. Acta Neuropathol. 132, 391–411. https://doi.org/10.1007/s00401-016-1548-y (2016).
Watanabe, Y. et al. Mouse motor neuron disease caused by truncated SOD1 with or without C-terminal modification. Brain Res. Mol. Brain Res. 135, 12–20. https://doi.org/10.1016/j.molbrainres.2004.11.019 (2005).
Ogawa, M. et al. Immunohistochemical observation of canine degenerative myelopathy in two Pembroke Welsh Corgi dogs. J. Vet. Med. Sci. 73, 1275–1279 (2011).
Liddelow, S. A. et al. Neurotoxic reactive astrocytes are induced by activated microglia. Nature 541, 481–487. https://doi.org/10.1038/nature21029 (2017).
Ukawa, H. et al. Negative Selection on a SOD1 Mutation Limits Canine Degenerative Myelopathy While Avoiding Inbreeding. Genome Biol. Evol. 16 https://doi.org/10.1093/gbe/evad231 (2024).
Chang, H. S. et al. Genotyping assays for the canine degenerative myelopathy-associated c.118G > A (p.E40K) mutation of the SOD1 gene using conventional and real-time PCR methods: a high prevalence in the Pembroke Welsh Corgi breed in Japan. J. Vet. Med. Sci. 75, 795–798 (2013).
Roels, E. et al. Assessment of CCL2 and CXCL8 chemokines in serum, bronchoalveolar lavage fluid and lung tissue samples from dogs affected with canine idiopathic pulmonary fibrosis. Vet. J. 206, 75–82. https://doi.org/10.1016/j.tvjl.2015.06.001 (2015).
Appelbaum, T., Santana, E. & Aguirre, G. D. Strong upregulation of inflammatory genes accompanies photoreceptor demise in canine models of retinal degeneration. PLoS One. 12, e0177224. https://doi.org/10.1371/journal.pone.0177224 (2017).
Toedebusch, C. M. et al. Lumbar spinal cord microglia exhibited increased activation in aging dogs compared with young adult dogs. Geroscience 42, 169–182. https://doi.org/10.1007/s11357-019-00133-8 (2020).
Goulart, M. R., Pluhar, G. E. & Ohlfest, J. R. Identification of myeloid derived suppressor cells in dogs with naturally occurring cancer. PLoS One. 7, e33274. https://doi.org/10.1371/journal.pone.0033274 (2012).
Fahnestock, M. et al. BDNF increases with behavioral enrichment and an antioxidant diet in the aged dog. Neurobiol. Aging. 33, 546–554. https://doi.org/10.1016/j.neurobiolaging.2010.03.019 (2012).
Peng, Y., Li, P., Hu, W., Shao, Q. & Wen, H. Mechanisms by which spinal cord stimulation intervenes in atrial fibrillation: The involvement of the endothelin-1 and nerve growth factor/p75NTR pathways. Open. Med. (Wars). 18, 20230802. https://doi.org/10.1515/med-2023-0802 (2023).
Acknowledgements
The authors would like to acknowledge Kazuhiro Watanabe and Shingo Miyawaki for sharing the experimental equipment, as well as Yuuta Nozue and Haruka Iseri for cooperation in sample collection.
Funding
This work was supported by an intramural research fund (President discretionary expenses) from Gifu university and JSPS KAKENHI Grant Number 19K15978.
Author information
Authors and Affiliations
Contributions
Shunya, Yui, Naohito and Satoshi designed the study. Shunya, Yui, Hiroaki, Kohei and Junya collected the experimental samples and the clinical data. Yui and Kei provided technical assistance. Osamu and Shinichiro conducted genetic test. Hiroki and Jun made diagnosis of DM by histopathological examination. Shunya collected and analyzed the experimental data and wrote the original draft of manuscript. All authors provided editorial input during manuscript editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yokota, S., Kobatake, Y., Yoshida, K. et al. Analysis of immune-related alterations in blood and spinal cord of canine degenerative myelopathy, a spontaneous model of amyotrophic lateral sclerosis. Sci Rep 16, 13494 (2026). https://doi.org/10.1038/s41598-026-43838-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-43838-5
