
Abstract
One intrinsic characteristic of Triple Negative Breast Cancer (TNBC) is its high plasticity, resulting in heterogeneous cancer cell subpopulations with distinct interactions with the immune system. To address TNBC plasticity, we set to model the dynamics of tumor cell subpopulations derived from the murine TNBC-like 4T1 cell line, by developing a system of ordinary differential equations (ODEs) based on experimental results, distinguishing between Sca1⁺ (Stem Cell Antigen 1) and Sca1⁻ cells and identifying chemotherapy-resistant populations. The model incorporates interactions with immune cells, including natural killer (NK) cells, T lymphocytes, and myeloid-derived suppressor cells (MDSCs). We investigated the effects of chemotherapy and anti-MDSC immune-boosting agent—methotrexate (MTX) and Abequolixron, respectively—through various treatment regimens and combinations. Simulations were conducted to explore different treatment initiation times and variations in immune cell killing rates. Our findings suggest treatment timing and administration order as key determinants of therapeutic outcome. Initiating chemotherapy in synchrony with immune-killer cell oscillations—near their local peak—promoted tumor elimination, whereas mistimed treatment led to tumor escape. An optimal chemotherapy exposure window was required for elimination; exposures that were too short or prolonged favored escape of MTX-sensitive and MTX-resistant cells, respectively. Longer MTX-free intervals shifted tumors from dormancy toward elimination, suggesting reduced recurrence risk. Administering immune-boosting therapy before chemotherapy broadened the effective therapeutic window, and combination treatment with Abequolixron and MTX further improved outcomes. These results provide, for the first time a quantitative mathematical framework based on experimental data, leveraging TNBC cell plasticity for optimizing combined chemo-immunotherapy scheduling in TNBC.
Similar content being viewed by others


Introduction
Triple-Negative Breast Cancer (TNBC) is an aggressive, highly metastatic breast cancer subtype lacking estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2), making it unresponsive to targeted therapies1. TNBC is primarily treated with chemotherapy and recurs in approximately 30–40% of cases as metastatic disease, due to the development of drug resistance2,3. One of the key factors contributing to TNBC’s aggressive nature is tumor plasticity, the ability of cancer cells to dynamically switch between different phenotypic and functional states. This adaptability allows TNBC cells to resist therapy, enhance metastatic potential, and evade immune response4. A murine marker associated with tumor plasticity is Stem Cell Antigen-1 (Sca-1), a cell surface protein implicated in regulating cellular heterogeneity and promoting metastatic behavior5. Elevated Sca-1 expression has been linked to a stem cell like state, increased tumorigenicity, enhanced resistance to therapy, and greater adaptability of cancer cells6,7, suggesting it may play a potential role in TNBC progression.
The immune system plays a central role in controlling tumor growth and metastasis through the action of cytotoxic immune cells8. Natural killer (NK) cells and cytotoxic T lymphocytes (CTLs) are key effectors for anti-tumor immunity, recognizing and eliminating cancer cells through cytotoxic mechanisms9,10. However, tumors can evade immune surveillance by recruiting immunosuppressive cells such as myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Tregs), which inhibit NK and T cell activity through cytokine secretion and direct cell–cell interactions11. These immunosuppressive mechanisms contribute to tumor immune escape and resistance to immune-based therapies12.
Treatments of TNBC include radiotherapy, chemotherapy and, more recently, immunotherapy13. Chemotherapy remains a cornerstone of TNBC treatment, reducing tumor burden by inhibiting tumor growth14. Methotrexate (MTX), modeled in this study, is a well-characterized antimetabolite that inhibits dihydrofolate reductase (DHFR), thereby disrupting DNA synthesis and inducing tumor cell death15. Historically part of the CMF regimen (cyclophosphamide, methotrexate, and 5-fluorouracil), MTX was among the first effective breast cancer treatments16,17. Although no longer a first-line agent, because anthracyclines, taxanes, and platinum-based regimens generally show superior efficacy, it retains clinical relevance in specific settings—such as in frail patients not tolerating more aggressive regimens and in palliative settings —and remains mechanistically pertinent to the high proliferative rate of TNBC cells18,19. In addition to its cytotoxic activity, MTX induces myelosuppressive effects that can influence immune cell production and recruitment to the tumor site20,21, an aspect incorporated into our analysis. Immunotherapy, on the other hand, is an increasingly relevant strategy in cancer treatment, leveraging the immune system to target tumors. Immune checkpoint inhibitors, cancer vaccines, and immune-modulating agents have shown promise in improving outcomes8,22. Abequolixron (RGX-104) is a synthetic small-molecule immunomodulator identified in recent preclinical and early clinical studies as a potent enhancer of antitumor immunity. By activating the liver X receptor (LXR) pathway, it induces depletion of myeloid-derived suppressor cells (MDSCs), thereby alleviating tumor-associated immune suppression23,24. Given the pivotal role of MDSCs in mediating immune evasion and therapeutic resistance in TNBC25,26, we selected RGX-104 as a representative immune-activating compound with reported effects on MDSC populations24. The combinations of chemotherapy and immunotherapy may have a beneficial effect, maximizing the treatment efficacy and reducing the likelihood of tumor escape and recurrence13.
One of the critical challenges in TNBC treatment is drug resistance. It develops under the selective pressure of frequent drug exposure, enabled by tumor cell plasticity27. Adaptive therapy, a novel treatment strategy, seeks to control tumor progression by optimizing treatment timing and dosages based on tumor dynamics and immune responses to maintain long-term tumor control while preventing the emergence of resistant cancer cell populations28,29. Based on the immunoediting concept, which describes cancer evolution through tumor-immune interactions, cancer progression can follow three potential trajectories: elimination, where immune cells successfully eradicate tumor cells; equilibrium (dormancy), where immune surveillance constrains tumor growth without complete eradication; and escape, where tumor cells develop mechanisms to evade immune control and proliferate unrestricted30. Drawing on concepts from adaptive therapy and immunoediting, the optimized treatment plan aims to prevent the emergence of drug-resistant subpopulations while simultaneously reducing the formation of dormant tumor cells—both of which are key contributors to cancer recurrence.
Ordinary differential equations (ODEs) are widely used to model tumor-immune dynamics and treatment responses. Their simplicity makes them computationally efficient and analytically tractable for analysis of the biological systems such as tumor-immune system dynamics. This advantage has led to their extensive use in cancer modeling31,32,33,34,35.
In contrast to the extensive mathematical modeling of chemotherapy effects on tumors, the modeling of the impact of combined immune and chemotherapy on TNBC remains largely unexplored. Existing studies primarily focus on chemotherapy alone36,37,38, overlooking how immune therapies can significantly enhance treatment efficacy. Additionally, TNBC’s heterogeneity and resistance to chemotherapy remain key challenges, contributing to poor treatment outcomes and prognosis.
To address these gaps, we developed an ODE-based model, validated by experimental results, to simulate murine TNBC-immune system interactions and assess treatment strategies. Our model incorporates various treatment plans of RGX-104 and MTX to analyze their effects on tumor growth, immune suppression, and drug resistance. By optimizing treatment timing based on immune system dynamics, we explore how combination therapy may enhance the efficacy of the treatment to eliminate the tumor. Additionally, we examine how varying immune cell killing rates influence tumor progression, providing insights into the benefits of personalized treatment strategies. Our findings indicate that chemotherapy exposure duration and resting intervals, synchronization with immune activity, treatment sequencing, and combination strategies collectively shape therapeutic response, highlighting key parameters for treatment optimization and providing a framework for improving TNBC management and reducing recurrence driven by dormant drug-resistant cells.
Materials and methods
Schematic representation of interactions between cell populations of the model
The interactions between five populations used in our model are illustrated in Fig. 1a. These populations are as follows: 4T1 Sca-1− and 4T1 Sca-1+ tumor cells (\({\text{C}}^{-}\) and \({\text{C}}^{+}\)), chemotherapy-selected 4T1 Sca-1+ tumor cells (\({\text{C}}_{\text{p}}^{+}\)), immune killer cells (I), and myeloid-derived suppressor cells (MDSCs, M). All interactions were simulated using murine-derived data. In reference to the study from which we obtained data on cell population interactions, the term MDSCs specifically refers to the tumor-educated \(\text{G}\text{r}1^+\text{C}\text{D}11\text{b}^+\) cell population5.

Schematic representations of the model structure and treatment protocols used in this study. (a) Interactions between modeled cell populations. Arrows indicate an increase in the population of the cells they point to, while red inhibitory bars represent a decrease in cell numbers. (b) RGX monotherapy treatment plan. (c–d) Treatment cycles used in MTX and MTX-RGX plans. Both periods of each treatment cycle were variable, ranging from 0.165 to 80 days.
Model assumptions
The following assumptions were applied to model the interactions of the cell populations:
-
The recruitment, expansion, and activation of MDSCs are solely induced by tumor cells.
-
The immune killer cell population (I) consists of natural killer (NK) cells, CD8+ and CD4+ T lymphocytes as they are the main immune cells responsible for eliminating tumor cells39,40,41.
-
Tumor cells inactivate immune killer cells indirectly through the recruitment of MDSCs.
-
NK cells, which belong to the innate immune system, remain consistently active and present within tissues, representing a constant source of cytotoxic cells—even when tumor cells are not present.
Developing model using ordinary differential equations
A set of ordinary differential equations (ODEs) was established to simulate the dynamics of the 4T1 tumor cells and the immune system. The used variables are: \({\text{C}}^{-}\), \({\text{C}}^{+}\), \({\text{C}}_{\text{p}}^{+}\), I, M, q (recruitment rate of I cells), and αm (recruitment rate of M cells). Different terms in the equations indicate distinct conditions or treatment effects. Terms corresponding to the base model (no drug treatment) are unmarked, terms representing the MTX treatment effect are labeled “MTX,” and the term representing the RGX-104 effect is labeled “RGX. For simplicity, RGX-104 will be referred to as RGX from this point onward. Also, all terms used in the equations are based on the law of mass action, meaning that the rate of change for each term is proportional to the respective populations involved. The dynamics of the cell populations are modeled as follows, where all parameters are described in Table 1.
Sca-1− tumor cells (\({\text{C}}^{-}\)):
Sca-1+ tumor cells (\({\text{C}}^{+}\)):
Chemotherapy-selected Sca-1+ tumor cells (\({\text{C}}_{\text{p}}^{+}\)):
A logistic growth term was chosen due to its best fit to the experimental data5 with \({a}_{1}\) and \({a}_{2}\) as growth rates. To model the intrinsic \({C}^{-}\leftrightarrow{C}^{+}\) conversion, \(\lambda{C}^{-}\) and \(\gamma{C}^{+}\) terms were introduced with \(\lambda\) and \(\gamma\) representing the coefficients of related conversions. The MDSC and self-induced \(\text{f}\text{o}\text{r}\text{m}\text{a}\text{t}\text{i}\text{o}\text{n}\text{ o}\text{f}\) \({C}^{+}\) cells are modeled using a Michaelis-Menten function, with \(\epsilon\) and \(r\) as coefficients. The induction of \({C}^{-}\) ◊ \({C}^{+}\) conversion by MDSCs5 has direct relationship with \({\text{s}\text{c}\text{a}-1}^{+}\) cancer cells (\({C}^{+}\text{ and }{C}_{p}^{+}\)) based on experimental data presented in the study by Peyvandi et al.5. The parameters \({i}_{M}\) and \({i}_{C}\), as indicated in Table 1, respectively represents the ratio of MDSCs and the ratio of Sca-1 antigen-positive cancer cells to the total cancer cell population. The use of cell population ratios instead of absolute cell counts accounts for the concentration of probable secretions that stimulate the cells. The reduction in tumor cell subpopulations due to the activity of immune killer cells is shown in the \("\tau IC"\) term. During MTX exposure, \({C}^{-}\) and \({C}^{+}\) cells are killed at rate \(\mu\). Also \({C}_{p}^{+}\) subpopulation of cancer cells emerges from \({C}^{+}\) cells by selection at rate \(\omega\).
Immune killer cells (I):
The parameter s (cells·day⁻¹) represents a constant recruitment rate of immune killer cells into the bloodstream under homeostatic conditions, indicating a steady inflow. The rest of immune killer cells are recruited to the tumor site by a Michaelis-Menten term, with k and q as coefficients of the recruitment. The other terms in Eq. 4 stands for the reduction of immune killer cells due to their natural death or their inactivation by MDSCs33. The effect of MTX on the recruitment of Immune killer cells (I) and MDSCs (M) populations to the tumor site was considered and is reflected in the following equations; however, this effect was not explicitly incorporated into the parameter s because of the lack of reliable data. This limitation could be addressed in future work by introducing a dose-dependent modulation of leukocyte production by MTX to capture MTX-induced leukopenia more accurately.
Myeloid-derived suppressor cells (MDSCs) (M):
The first termindicates the recruitment of MDSCs to the tumor site, while the second term, represents the natural death of MDSCs33. The last term stands for the RGX killing effect on MDSCs at rate g.
The recruitment rates of I cells (\(q\)) and M cells (\({\alpha}_{m}\)) vary over time, as shown in Eqs. 6 and 7.
I cells’ recruitment rate (\(q\)):
M cells’ recruitment rate (\({\alpha}_{m}\)):
As shown in Table 1, the parameters A (0 or 0.12) and B (0 or 0.22) vary depending on the condition. When the mouse is treated with MTX, both values are set to 0 to simulate the decrease in \(q\) and \({\alpha}_{m}\). The variation in these values stops once they reach 0. In the absence of MTX exposure, A and B are set to 0.12 and 0.22, respectively, reflecting the recruitment rates in the study of Mehdizadeh et al.33. This explains the gradual post-treatment recovery of the q and \({\alpha}_{m}\) recruitment rates until they reach their maximum values. Also, The change in the values of q and \({\alpha}_{m}\) is directly related to the values of death rates of immune killer cells’ (n) and MDSCs (\(\beta\)).
Model parameter fitting
Some of the model parameters were obtained from previous works33. To estimate the remaining coefficients, two approaches were used. For parameters where the system could be handled computationally, the lsqcurvefit function in MATLAB R2023b was applied to fit the model to the experimental data5,24. For parameters associated with more complex ODEs, where the fitting process became computationally demanding due to system stiffness, we employed a sequential manual fitting strategy. Parameters were first estimated from datasets with the fewest unknowns, and additional parameters were then introduced step by step. This fitting cycle was repeated until parameter values stabilized. A detailed description of all coefficients is provided in Table 1.
Simulations
All the simulations were conducted using MATLAB R2023b with the ODE45 solver. According to the immunoediting theory, tumors can undergo one of three fates following interaction with the immune system: elimination (eradication of cancer cells), dormancy (where net growth is zero due to the immune response, but the cancer cell population is not fully eradicated), or escape (uncontrolled tumor growth).
Simulation results were categorized into one of the following states:
-
Elimination occurs if the total number of cancer cells falls below 10.
-
Escape occurs if the total number of cancer cells exceeds 109.
-
In all other cases, the tumor enters the dormancy phase.
The initial set up of simulations are mentioned in Table 2.
Simulations were conducted under three distinct therapeutic conditions:
-
1.
Monotherapy with RGX.
-
2.
Monotherapy with MTX.
-
3.
Dual therapy with MTX and RGX.
In all mentioned therapeutic conditions, treatment began at three different starting points (days 11, 19, and 25), with simulations conducted using three distinct values of τ (\(1.1\times{10}^{-7}\), \(1.6\times{10}^{-7}\) and \(2.86\times{10}^{-7}\)).
Monotherapy with RGX
Based on experimental protocols for RGX, a daily administration for up to 60 days is recommended for tumor treatment in mice24. Therefore, it assumed to be effective continuously during the simulation time. The treatment plan for the RGX monotherapy is shown in Fig. 1b.
Treatment regimens for monotherapy with MTX and dual therapy with RGX and MTX
The treatment regimens for both MTX monotherapy and MTX-RGX dual therapy were simulated as repetitive cycles. Each cycle consisted of an MTX treatment period, representing the duration of drug effect following administration, followed by a drug-free interval. The MTX monotherapy cycles were repeated five times, with a subsequent 150-day drug-free period to confirm the tumor’s final state. In the dual therapy regimen, the key difference was the continuous effect of RGX during the cycles, while MTX followed the same pattern. The shortest period MTX could remain active in the body was determined by seven plasma half-lives (33.8 min each44) ensuring the concentration fell below 1% of the initial dose, corresponding to roughly 0.165 days. At the end of each simulation, tumor status was recorded as escape, dormancy, or elimination. All treatment cycles for both regimens are illustrated in Fig. 1c and d.
Evaluation of tumor non-escape probability under different treatment regimens and τ variations
To compare the results of different simulations on tumor escape prevention—whether through elimination or dormancy—the percentages of the respective tumor fates were calculated from the relevant figures. This analysis was performed using MATLAB 2023b’s built-in functions for figure manipulation and pixel analysis. In the first set of analysis (varying τ values from \(1.1\times{10}^{-7}\) to \(2.86\times{10}^{-7}\)), all figures corresponding to each distinct τ value were included. In the second set of analysis (comparison of MTX monotherapy results to dual therapy), all figures for the three τ values (\(1.1\times{10}^{-7}\), \(1.6\times{10}^{-7}\) and \(2.86\times{10}^{-7}\)) were considered.
Sensitivity analysis
To evaluate the robustness of our model, a sensitivity analysis was performed on the parameters listed in Table 3, all of which were estimated and optimized in this study rather than obtained from the literature. These parameters were held constant in the baseline simulations; however, for the sensitivity analysis, each was independently varied by ± 5% from its optimized value to assess its impact on model outcomes.
For each parameter perturbation, the resulting changes in tumor fate—classified as elimination, dormancy, or escape—were quantified. The relative variations in the percentage of each outcome are summarized in Table 3. All simulations were conducted under identical conditions, using 2.86 × 10⁻⁷ and a dual-therapy regimen with MTX and RGX initiated on day 25. The baseline scenario used for comparison corresponds to the results shown in Fig. 5e.
Results and discussion
Model parameter estimation and validation against experimental data
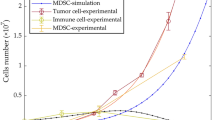
The model parameters are estimated as described in the Materials and Methods based on the in vivo and in vitro data5. Fitting the model to the related experimental data is shown in Fig. 2. The fitted simulations closely reproduced the experimentally observed dynamics of 4T1 tumor subpopulations, as well as the effects of immunotherapy with RGX and chemotherapy with MTX on cell populations (Fig. 2). Incorporating MDSC-mediated induction of C⁻→C⁺ conversion, modeled as a function of the Sca-1⁺ cell fraction within the tumor population, was essential to reproduce co-culture dynamics, consistent with experimental evidence that tumor-educated myeloid cells promote cancer cell plasticity5. Also, MTX treatment was simulated, as detailed in the Materials and Methods, by increasing the death of sensitive cells (\({C}^{-}\) and \({C}^{+}\)) and selecting for the \({C}_{P}^{+}\) subpopulation (resistant group) from \({C}^{+}\) cells. Accordingly, Fig. 2g shows a late increase in this group, reflecting treatment-driven enrichment of resistant phenotype.

Fitting the model simulations to experimental data. (a) In vitro data on the growth of 4T1 cells (C- and C+)5 and the related simulation (estimating the a1 parameter). (b) In vitro data on the growth of \({C}_{p}^{+}\) cells5 and the corresponding simulation (estimating the a2 parameter). (c) In vitro data on the conversion of C⁻ ⇌ C⁺ cells5 and the related simulation (estimating λ and γ parameters under in vitro conditions). Only the dynamics of the C⁻ population are shown, as C⁻ and C⁺ fractions are complementary. Including both would not provide additional information and would make the figure less readable. (d) In vitro data on the C⁻ ⇌ C⁺ conversion in co-culture with MDSCs5, along with the corresponding simulation (estimating the ε parameter). The plotted data represent the C⁻ fraction, with complementary C⁺ dynamics omitted for clarity. (e) In vivo data on the conversion of C⁻ ⇌ C⁺ cells5 and the related simulation (optimizing λ and γ parameters under in vivo conditions along with estimating the r parameter). As above, only the C⁻ fraction is shown for clarity. (f) In vitro data of MDSC’s population reduction after RGX treatment24 and the corresponding simulation (estimating the g parameter). (g) In vitro data on the decrease of total 4T1 tumor cells following MTX treatment5 and the corresponding simulation (estimating the µ and ꞷ parameters) [left panel]. The simulated curve in the left panel, representing the sum of all 4T1 subpopulations, is further broken down into subpopulations, showing the death of C⁻ and C⁺ cells and the emergence of Cₚ⁺ cells through selection from C⁺ cells [right panel]. (h) In the same study5, Selected cells from part G were cultured in MTX-free medium, showing a decrease in the fraction of Sca-1⁺ 4T1 cells (estimating the µ and ꞷ parameters) and the corresponding simulation [left panel]. The dynamics of all 4T1 cell subpopulations are shown, with all subpopulations expanding over time, while the relative fraction of Sca-1⁺ cells decreases. This arises from the equilibrium between C⁻ and C⁺ populations, which favors C⁻, combined with the comparatively slower expansion of the Cₚ⁺ population. [right panel].
Together, these results demonstrate that the model quantitatively captures experimentally observed tumor–immune–treatment interactions and provides a validated basis for exploring treatment timing and scheduling.
Different tumor fates defined in the model
Based on immunoediting theory, simulated tumor outcomes were classified as escape, dormancy, or elimination as introduced in the introduction section. Figure 3 illustrates the characteristic cell population dynamics associated with each fate under specific treatment conditions.

Defined tumor fates in the model. In all subfigures, treatment initiated on day 19. Each cycle (see Materials and Methods) was repeated five times, followed by 150 days without treatment to confirm outcome stability. (a) Tumor Escape (treatment cycle: 40 days MTX-RGX followed by 20 days RGX). No treatment also results in escape with different cell dynamics (not shown). Note that tumor escape occurs around day ~ 120 when the tumor cell population exceeds 10⁹. The subsequent part of the simulation was only followed to confirm the stability of the escape state and does not carry additional biological meaning. (b) Tumor Dormancy (treatment cycle: 15 days MTX-RGX followed by 20 days RGX). (c) Tumor Elimination (treatment cycle: 2 days MTX-RGX followed by 20 days RGX).
In panels A and B, the C⁻ and C⁺ populations decline and remain near zero for the remainder of the simulation, and their curves are therefore not visible at later times.
Simulation of tumor’s fate under varying initial conditions
The outcomes of tumor fate simulations were assessed following three distinct drug regimens: monotherapy with RGX, monotherapy with MTX, and dual therapy combining both drugs. In each scenario, the therapeutic regimen was initiated at three different time points (days 11, 19 and 25) and repeated for three distinct values of τ (1.1 × 10⁻⁷, 1.6 × 10⁻⁷, and 2.86 × 10⁻⁷).
Monotherapy with RGX
All monotherapy regimens with RGX led to tumor escape. In these simulations, reduction of MDSCs partially relieved immune suppression but was insufficient to eliminate tumor cells in the absence of direct cytotoxic pressure. Supplemental Fig. 1 illustrates the dynamics of the cells during RGX monotherapy for one specific plan as a case.
Monotherapy with MTX
Tumor response to MTX monotherapy was strongly dependent on both treatment initiation time and immune killing rate τ. When τ was set to its lowest value (1.1 × 10⁻⁷), tumor escape occurred across all treatment schedules, regardless of treatment initiation time (Supplemental Fig. 2d). Similarly, initiating treatment on day 25 (latest tested time) led to escape for all τ values, indicating that delayed chemotherapy could not overcome established tumor–immune suppression (Supplemental Fig. 2 d).
In contrast, earlier initiation (day 11 or day 19) combined with higher τ values yielded subsets of treatment plans resulting in tumor dormancy or elimination (Supplemental Fig. 2a–c). The most favorable MTX-only outcomes were observed when therapy began on day 19 with τ = 2.86 × 10⁻⁷ (Fig. 4). The apparent advantage of initiating treatment on day 19, rather than at the earliest tested time point or at later initiation times, is elucidated in later sections through a detailed analysis of the cell population dynamics.

Tumor fate following MTX monotherapy initiated on day 19 with τ set to 2.86 × 10⁻⁷.
Dual therapy with MTX and RGX
The tumor’s response to various dual therapy cycles—each defined by a specific combination of dual-therapy duration and RGX effect duration—was simulated. Combining MTX treatment with a continuous RGX therapeutic effect throughout the treatment plan improved outcomes by reducing tumor escape region. When treatment was initiated on day 11 with τ set to 1.1 × 10⁻⁷ or 1.6 × 10⁻⁷, tumor elimination or dormancy was observed in only a subset of plans, as shown in Supplemental Fig. 3a-b. In contrast, increasing τ to 2.86 × 10⁻⁷ led to a greater number of non-escape outcomes (Fig. 5a). When treatment was started on day 19, all tested τ values produced some successful plans leading to tumor elimination, as shown in Fig. 5b–d, indicating a broad therapeutic window. However, initiating treatment on day 25 with τ values of 1.1 × 10⁻⁷ or 1.6 × 10⁻⁷ resulted in tumor escape across all therapy cycles (Supplemental Fig. 3c). Importantly, raising τ to 2.86 × 10⁻⁷ allowed tumor elimination despite late treatment initiation on day 25, where monotherapy was ineffective (Fig. 5e). Later sections further evaluate the advantages of dual therapy and MDSC targeting through detailed analyses of cell population dynamics.

Tumor fate following MTX–RGX dual therapy across different τ values and treatment initiation times. (a) τ = 2.86 × 10⁻⁷, treatment initiated on day 11. (b–d) τ = 1.1 × 10⁻⁷, 1.6 × 10⁻⁷, and 2.86 × 10⁻⁷, respectively, all with treatment initiated on day 19. (e) τ = 2.86 × 10⁻⁷, treatment initiated on day 25.
The white grid points marked in panels represent specific treatment plans under the corresponding conditions, which were subsequently used to generate the simulations of cell population dynamics shown in Fig. 6.

Dynamics of cell populations under various treatment plans and initial conditions. (a–c) Dynamics during treatment initiation at different time points (τ = 1.1 × 10⁻⁷; treatment cycle: 12 days MTX–RGX followed by 20 days RGX-only). Treatment was initiated on day: (a) 11, (b) 19, and (c) 25. (d–e) Dynamics under different τ values (treatment cycle: 5 days MTX–RGX followed by 15 days RGX-only). (d) τ = 1.1 × 10⁻⁷; (e) τ = 2.86 × 10⁻⁷. (f–g) Comparison between MTX–RGX combination and MTX monotherapy (τ = 2.86 × 10⁻⁷). (f) MTX monotherapy: 10 days MTX followed by 20 days drug-free; (g) MTX–RGX: 10 days MTX–RGX followed by 20 days RGX-only. (h–i) Dynamics under MTX–RGX treatment with varying chemotherapy exposure durations (τ = 1.6 × 10⁻⁷). (h) Longer MTX exposure: 35 days MTX–RGX followed by 30 days RGX-only; (i) Shorter MTX exposure: 25 days MTX–RGX followed by 30 days RGX-only.
Cell population dynamics underlying treatment outcomes
To elucidate the mechanisms driving the treatment outcomes presented earlier, we examined the cell population dynamics that lead to those outcomes (Fig. 6). We focus on five variables identified as key determinants of treatment outcomes: (1) treatment initiation time, (2) chemotherapy exposure duration, (3) chemotherapy resting period, (4) τ value, and (5) combination therapy versus monotherapy. The panels in Fig. 6 show specific points selected from Figs. 5 and 2, and Supplemental Figs. 2 and 3.
Notably, the oscillatory patterns in our simulations reflect biologically documented immune–tumor feedback dynamics. A time delay model demonstrated Hopf bifurcation–driven oscillations consistent with nonmonotonic tumor growth45, and another immune–tumor interaction model reproduced post-therapy prostate-specific antigen (PSA) bounce behavior through feedback dynamics46. Likewise, clinical studies report rhythmic oscillations in immune–tumor activity: Coventry et al. observed cyclical fluctuations in immune biomarkers47, and Xiao et al. reported periodic changes in hematopoietic populations48. Moreover, Tubin et al. and Leontovich et al. showed that treatment outcomes improve when therapy is synchronized with immune activation phases49,50. Collectively, these findings confirm that oscillatory immune–tumor dynamics are biologically grounded and arise from intrinsic feedback between immune activation and tumor-induced suppression.
The results of our study confirms that ineffective therapeutic regimens promote tumors to escape immune control51. Ineffective short durations of drug exposure primarily result in tumor escape characterized by the dominance of C⁻ cells. This phenomenon arises from the natural balance between C⁺ cells (Sca-1 antigen-positive) and C⁻ cells, which tends to favor C⁻ cells5. Conversely, inefficient treatment regimens with prolonged drug exposure confer a competitive advantage to the resistant cell population (Cₚ⁺), leading to tumor escape that is largely driven by these resistant cells.
The following sections examine determinants of effective tumor elimination, beginning with treatment-timing parameters and followed by factors related to drug administration order. Together, the findings suggest that successful outcomes can be achieved without administering additional drugs that target resistant Cₚ⁺ cells (which often carry substantial side effects). By optimizing therapeutic regimens to align with immune-killer cell dynamics and by augmenting immune activity, the resistant Cₚ⁺ population can be eradicated, resulting in tumor elimination.
Treatment timing: considering immune system dynamics enables optimization of treatment initiation for tumor elimination
Increasing the number of cancer cells has a dual impact on immune killer cells; Firstly, a direct immune stimulating effect by promoting the recruitment of the immune killer cells to the tumor site and secondly, an indirect immunosuppressive effect by promoting the recruitment of MDSCs. Thus, tumor growth may modulate the immune killer cell response depending on the balance between recruitment and suppression. The dynamics of these effects were analyzed under various conditions. As shown in Fig. 6b, the optimal condition for the effective immune response occurs in this scenario (therapy start at day 19) compared to starting therapy on previous or following days (day 11 and 25 respectively) (Fig. 6a and c). In this case, a larger tumor cell population at day 19, compared to a smaller population at day 11, recruits a greater number of immune killer cells, enabling the immune system to control the tumor during chemotherapy. In other words, the higher tumor cell numbers stimulate a stronger and more effective immune response, also seen in Arabameri and Arab’s model52.
Explaining the optimal control of tumor growth by starting the treatment on day 19, the dynamic of the immune killer cells (I) on this time point, is represented (Fig. 7) with and without treatment, corresponding to Fig. 6b.

Schematic dynamics of the immune killer cells’ population on day 19 following MTX-RGX or RGX alone treatment.
It can be observed that when immune killer cells reach their local maximum and are about to decline, the initiation of chemotherapy alters the dynamics, causing an upward trend. This is due to a significant reduction in tumor cells during chemotherapy, which decreases the recruitment of MDSCs. The reduced immune suppression allows an increase in active immune killer cells, resulting in a more effective antitumor response.
When chemotherapy starts earlier on day 11 (Fig. 6a), the tumor cell population is smaller, leading to fewer immune killer cells being recruited to the tumor site. Consequently, the immune killer cells have not reached their peak at the onset of chemotherapy and starting treatment cycles at this point damps the local peak of the immune response. So, the dropped immune killer cell population in the local peak compared to Fig. 6b is unable to eliminate the tumor cells.
On the other hand, when chemotherapy begins on day 25 (Fig. 6c), the immune killer cell population has already declined and is far from its local maximum. The delay allows the tumor to grow aggressively, and the chosen treatment regimen fails to control its growth. The decline in immune cell numbers is attributed to increased tumor growth followed by enhanced immune suppression caused by MDSCs.
The exact timing of the therapy based on the immune response is supported by clinical evidence53,54,55. Although previous studies have primarily focused on how the circadian rhythm affects the immune system in cancer patients, our model suggests a dynamically optimized treatment schedule that needs to be experimentally investigated. While the early therapy start after diagnosis is generally preferred56, the exact starting point of chemotherapy may be optimized based on the state of immune response as also indicated in the modeling reported by Ghanizadeh et al.42.
Treatment timing: optimized chemotherapy timing avoids higher doses that promote resistant cancer cell subpopulations
The duration of chemotherapy effect significantly influences treatment outcomes. MTX reduces both \(C^-\) and \(C^+\) tumor populations, while also supporting the immune system in eliminating tumors. However, prolonged chemotherapy can lead to the expansion of the resistant\(C_p^+\) population, creating conditions that favor their uncontrolled proliferation. Additionally, MTX suppresses the immune system by limiting the recruitment of killer cells to the tumor site over time. Ultimately, excessive chemotherapy durations may allow the tumor to escape elimination, driven by the proliferation of resistant cells. As shown in Fig. 6h and i an optimized chemotherapy plan is not necessarily achieved by higher doses or dose-dense chemotherapy, which may result in the development of chemotherapy resistant cancer cell subpopulations. In contrast, under specific conditions, shorter chemotherapy exposure can control drug-resistant cells more efficiently by eliminating their competitive advantage over other tumor subpopulations. Meanwhile, the only factor affecting all tumor subpopulations—immune killer cells—will gradually contribute to the complete eradication of the tumor. Although the rapid initial tumor size reduction is usually seen in high dose or dose-dense treatments, other optimized plans facilitate more effective tumor elimination by controlling drug-resistant tumor subpopulations and help prevent recurrence. This phenomenon is consistent with what observed with adaptive therapy approach57,58.
Eliminating the competitive advantage of the resistant subpopulation leads to a reduction in its population, resulting in a decreased \({i}_{c}\) value (the fraction of Sca-1⁺ cells relative to the total cancer cell population). In our model, based on experimental data5, the rate of MDSC-induced \(C\)⁻ \(\to C\)⁺ conversion is directly correlated with \({i}_{c}\). Thus, a reduction in \({i}_{c}\) leads to a decrease in \(C^+\) cells, which serve as precursors for Cₚ⁺ cells. This, in turn, further limits the expansion of the \(C_p^+\) population. By optimizing therapy to reduce \({i}_{c}\), the conversion process could be slowed.
Notably, the effect of \({i}_{c}\) (Sca-1⁺ cells) on MDSC-induction suggests that the interactions between \(C^-\), \(C^+\) cells, and MDSCs may differ. Therefore, further research is needed to explore the communication pathways between \(C^-\) and \(C^+\) cells and MDSCs, which could help identify novel therapeutic targets.
Treatment timing: the duration of chemotherapy resting period determines the treatment outcome
As it appears from Fig. 6e, the longer MTX-free period appears to increase the probability of tumor elimination. In contrast, prolonged duration of dual therapy durations consistently leads to tumor escape. These findings suggest that extending the rest period between treatments may be more beneficial as may prevent the tumor recurrence, and that shorter intervals between chemotherapy sessions are not universally advantageous for all patients. This concept remains somewhat controversial, as clinical evidence on dose-dense versus standard chemotherapy has shown mixed results, with some studies reporting improved outcomes59 and others finding no significant difference60.However, in the context of combined chemotherapy and immunotherapy, some studies support the idea of longer breaks before initiating immunotherapy61. Therefore, further clinical research is needed to better understand the role of rest periods in cancer treatment.
Drug administration order: immunotherapy before chemotherapy may increase the probability of successful treatment in patients
As demonstrated in the results, increasing τ from 1.1 × 10− 7 to 2.86 × 10− 7 reduces tumor escape regions by 18.95% as expected. Therefore, our simulations suggest that improving immune response to the tumor by immunotherapies (modeled by increasing τ) reduces the dependency on precise chemotherapy timing and duration, making tumor elimination more feasible. As shown in Fig. 6d, if chemotherapy begins when the tumor cell count is still very low, only a few immune killer cells are recruited, and the treatment fails. In contrast, in Fig. 6e, the higher killing efficiency of the population of immune killer cells compensates for its lower count, ultimately eliminating the tumor.
These simulations suggest that when a detailed analysis of tumor-immune system dynamics is not easily accessible or timing of therapy cannot be optimized (e.g., in newly diagnosed patients), pre-treatment with anticancer immune-boosting agents can enhance the effectiveness of chemotherapy in achieving tumor elimination. Though therapeutic protocols usually suggest concurrent chemotherapy with immunotherapy or immunotherapy after chemotherapy cycles13,62, our results propose that administering immunotherapy may be beneficial before chemotherapy cycles as they increase the probability of complete tumor elimination in patients. This is supported by observations in the study by Kwon et al.63. More clinical investigations are required to optimize the timing of chemo- and immunotherapy combinations.
While our simulations capture key tumor–immune dynamics, they assume all tumor subpopulations are equally susceptible to immune-mediated killing (i.e., a constant τ). This is most relevant for early-stage tumors (e.g., those detected by mammography) or residual tumor cells following surgical removal. For more advanced tumors, future work should allow τ to vary across subpopulations to capture heterogeneity and also consider patients with multiple lesions at different stages, thereby complicating therapy timing. Addressing these scenarios will require detailed clinical and biological data and represents an important direction for future studies.
Drug administration order: RGX alone failed to eliminate tumors, while in combination with MTX it boosted the chances of successful treatment
The results show that while treatment with RGX alone failed to control the tumor, combining it with MTX reduces tumor escape regions by up to 10.7%. This underscores the significance of using anti-MDSC therapies alongside direct tumor-targeting treatments.
RGX kills MDSCs, indirectly strengthening the immune system and enabling the elimination of treatment-resistant tumor population (Cₚ⁺ cells). Previous studies13,64,65 similarly highlight the benefits of combining immunotherapy with traditional cancer treatments. Particularly, the results of Shariatpanahi et al. model64 are consistent with our simulations and shows that directly targeting MDSCs or altering the tumor microenvironment to disrupt their function can enhance the effectiveness of existing cancer therapies.
The most significant improvement is observed when comparing the scenario with a τ of 2.86 × 10− 7, treatment initiated on day 25, and MTX monotherapy, to a similar setup that instead utilizes dual therapy (Fig. 6e). In the monotherapy case, tumor escape occurs across all tested conditions. In contrast, the dual-therapy can lead under certain conditions to complete tumor elimination, highlighting the broader range of effective treatment outcomes achieved with the combined therapy approach. As shown in Fig. 6f and g, adding RGX to treatment changes the dynamics of immune killer cells. In both cases, treatment begins at the same starting point (day 25). As demonstrated, the MTX monotherapy results in the expansion of the MDSC population during MTX-free intervals, driven by tumor growth and increased MDSC recruitment to the tumor site. This expansion subsequently leads to the suppression of immune killer cells. Whereas in the dual-therapy plan, RGX effectively controls MDSC expansion during MTX-free periods. This, combined with the increased recruitment of immune killer cells driven by tumor growth (without MDSC’s suppression effect), results in a higher immune killer cell count and improved tumor growth control. The encouraging results from our simulations suggest that MDSC-targeted immunotherapies, such as RGX-104, merit further experimental and clinical investigation in TNBC.
Comparing mono- versus dual-therapy plans as described, highlights the well-established advantages of combination therapy. Notably, the observed lack of efficacy in all monotherapy regimens for RGX and certain methotrexate treatment protocols contrasted with the emergence of effective tumor-eliminating regimens by combination therapies, indicates that resistance against monotherapy by different drugs does not necessarily implicate complete treatment efficacy. So combination therapies with other seemingly ineffective agents must be considered in such cases, as the agents may cross-potentiate each other’s efficacy, which may result in the desired treatment effect as seen in66. This approach may be considered for drug development programs. The efficacy assessment of a drug candidate must be investigated not just as a single agent but also in different combinations with other agents.
Sensitivity analysis
The outcomes of the sensitivity analysis are summarized in Table 3. Each model parameter was independently varied by ± 5% from its optimized value, and the resulting percentage-point changes in tumor elimination, dormancy, and escape relative to the baseline simulation (Fig. 2e) were computed. For clarity, Table 3 also reports the maximum absolute percentage-point change among these outcomes for each parameter.
Among all parameters, \({\text{a}}_{1}\)exhibited the strongest influence on tumor fate, with up to ~ 46%-point variation when increased by + 5% from its optimized value of 0.7616. This strong response likely arises because the baseline value lies close to a critical threshold where small perturbations dramatically alter system behavior. Notably, this relatively high growth rate is consistent with the aggressive nature of TNBC, which typically exhibits faster intrinsic proliferation than many other solid tumor types and commonly used murine tumor models14. In contrast, parameters \({\text{a}}_{2}\), \(g\), and \(\mu\) produced moderate effects (1.5–3.5 pp), while the remaining parameters caused only minor (< 1 pp) shifts, indicating that the model is largely robust to small perturbations.
To further explore the sensitivity to \({\text{a}}_{1}\), its value was systematically varied from − 20% to + 20% of the baseline (Fig. 8b). The figure shows a sharp transition near \({\text{a}}_{1}\)≈ 0.78, where elimination and dormancy fractions drop to nearly zero while the escape fraction rises steeply to 100%. Below this threshold, all three fates coexist, with escape being dominant (~ 60%) and elimination and dormancy occurring in ~ 20–30% of cases. When the tumor growth rate approaches or exceeds approximately 0.79 day⁻¹, tumor control becomes markedly more difficult, suggesting that tumors with even higher proliferative capacity may require additional or complementary therapeutic strategies.

Sensitivity of model outcomes and experimental fit to variations in parameter a₁. (a) Model fit to 4T1 tumor growth data for the baseline a₁ and ± 5% perturbations. (b) Tumor fate distributions as a₁ varies from − 20% to + 20% of its optimized value (0.7616).
Figure 8a shows the influence of parameter \({\text{a}}_{1}\) on simulated 4T1 tumor growth compared with experimental data. The baseline simulation (a₁ = 0.7616) closely matches the observed tumor growth, whereas altering \({\text{a}}_{1}\) by ± 5% produces clear deviations. The + 5% increase leads to overestimation of cell counts, exceeding the experimental error bars by day 3, while the − 5% case underestimates growth throughout. These results confirm that the fitted value of \({\text{a}}_{1}\) provides a precise match to experimental data and that even small perturbations in this parameter noticeably affect the model’s predictive accuracy. Despite the aggressive growth characteristics reflected by this parameter value, the evaluated treatment strategies were still able to effectively control tumor progression within the modeled conditions.
In conclusion, our study is, to our knowledge, the first to integrate experimentally validated dynamics of stem cell like TNBC cell subpopulations with immune components (NK, T cells and MDSC). We also incorporated the effects of a novel anti-MDSC agent (RGX-104) alongside methotrexate to explore chemo–immunotherapy interactions. Our results demonstrate that the initiation time, sequence, duration and resting periods in chemotherapy cycles play a critical role in determining treatment outcomes. Synchronizing chemotherapy with initiation of immune killer cells peak during their oscillation appears as a key factor in preventing the development of drug-resistant tumor cell subpopulation. Chemotherapy regimens initiated either too early or too late, as well as those with a too short or too long exposure period, favor the emergence of drug-resistant tumor cells and tumor progression. Longer MTX-free periods in a range of chemotherapy regimens have been shown to bypass cancer dormancy and promote tumor elimination. Moreover, the combination of RGX-104 with MTX boosted the treatment outcomes. An important prediction of our model is that administration of an immune-boosting therapy before chemotherapy is more effective in eradicating all cancer subpopulations and broadens their therapeutic time window.
Code availability
The code used in this study is openly available on Zenodo at: https://doi.org/10.5281/zenodo.15723767. The corresponding GitHub repository can be accessed at: https://github.com/Mobina-Daneshparvar/cancer-immune-dynamics.
References
Aysola, K. et al. Triple negative breast cancer–an overview. Hereditary Genet. 2013(Suppl 2), 001 (2013).
Ma, T. et al. Predictive markers of rapid disease progression and chemotherapy resistance in triple-negative breast cancer patients following postoperative adjuvant therapy. Sci. Rep. 15(1), 386 (2025).
Won, K.-A. & Spruck, C. Triple-negative breast cancer therapy: Current and future perspectives. Int. J. Oncol. 57(6), 1245–61 (2020).
Guo, Z. & Han, S. Targeting cancer stem cell plasticity in triple-negative breast cancer. Explor. Target. Antitumor Ther. 4(6), 1165 (2023).
Peyvandi, S., Bulliard, M., Yilmaz, A., Kauzlaric, A., Marcone, R., Haerri, L., et al. Tumor-educated Gr1 + CD11b+ cells drive breast cancer metastasis via OSM/IL-6/JAK–induced cancer cell plasticity. J. Clin. Invest. 134(6) (2024).
Upadhyay, G. et al. Stem cell antigen-1 enhances tumorigenicity by disruption of growth differentiation factor-10 (GDF10)–dependent TGF-β signaling. Proc. Natl. Acad. Sci. U. S. A. 108(19), 7820–7825 (2011).
Velasco-Velázquez, M. A., Popov, V. M., Lisanti, M. P. & Pestell, R. G. The role of breast cancer stem cells in metastasis and therapeutic implications. Am. J. Pathol. 179(1), 2–11 (2011).
Mukherjee, A. G. et al. Role of immune cells and receptors in cancer treatment: an immunotherapeutic approach. Vaccines 10(9), 1493 (2022).
Shaver, K. A., Croom-Perez, T. J. & Copik, A. J. Natural killer cells: The linchpin for successful cancer immunotherapy. Front. Immunol. 12, 679117 (2021).
Vojdani, A. et al. Natural killer cells and cytotoxic T cells: Complementary partners against microorganisms and cancer. Microorganisms 12(1), 230 (2024).
Spranger, S. & Gajewski, T. F. Mechanisms of tumor cell–intrinsic immune evasion. Annu. Rev. Cancer Biol. 2(1), 213–228 (2018).
Haist, M., Stege, H., Grabbe, S. & Bros, M. The functional crosstalk between myeloid-derived suppressor cells and regulatory T cells within the immunosuppressive tumor microenvironment. Cancers 13(2), 210 (2021).
Sordo-Bahamonde, C. et al. Chemo-immunotherapy: A new trend in cancer treatment. Cancers 15(11), 2912 (2023).
Xiong, N., Wu, H. & Yu, Z. Advancements and challenges in triple-negative breast cancer: A comprehensive review of therapeutic and diagnostic strategies. Front. Oncol. 14, 1405491 (2024).
Huennekens, F. The methotrexate story: A paradigm for development of cancer chemotherapeutic agents. Adv. Enzyme Regul. 34, 397–419 (1994).
Colleoni, M. et al. Classical cyclophosphamide, methotrexate, and fluorouracil chemotherapy is more effective in triple-negative, node-negative breast cancer: Results from two randomized trials of adjuvant chemoendocrine therapy for node-negative breast cancer. J. Clin. Oncol. 28(18), 2966–73 (2010).
Munzone, E., Curigliano, G., Burstein, H., Winer, E. & Goldhirsch, A. CMF revisited in the 21st century. Ann. Oncol. 23(2), 305–311 (2012).
Bocci, G., et al. Cyclophosphamide-methotrexate ‘metronomic’chemotherapy for the palliative treatment of metastatic breast cancer. A comparative pharmacoeconomic evaluation. Annals Oncol. 16(8), 1243–1252 (2005).
Colleoni, M. et al. Low-dose oral methotrexate and cyclophosphamide in metastatic breast cancer: Antitumor activity and correlation with vascular endothelial growth factor levels. Ann. Oncol. 13(1), 73–80 (2002).
Lora, M. et al. Low dose methotrexate has divergent effects on cycling and resting human hematopoietic stem and progenitor cells. Clin. Transl. Sci. 18(5), e70233. https://doi.org/10.1111/cts.70233 (2025).
Pannacciulli, I., Massa, G., Bogliolo, G., Ghio, R. & Sobrero, A. Effects of high-dose methotrexate and leucovorin on murine hemopoietic stem cells. Cancer Res. 42(2), 530–534 (1982).
Ling, S. P. et al. Role of immunotherapy in the treatment of cancer: A systematic review. Cancers 14(21), 5205 (2022).
Lim, E., et al. Abstract CT146: RGX-104, a first-in-class immunotherapy targeting the liver-X receptor (LXR): initial results from the phase 1b RGX-104 plus docetaxel combination dose escalation cohorts. Cancer Res. 80(16_Supplement), CT146-CT (2020).
Tavazoie, M. F. et al. LXR/ApoE activation restricts innate immune suppression in cancer. Cell 172(4), 825–40. e18 (2018).
Serrano García, L. et al. Patterns of immune evasion in triple-negative breast cancer and new potential therapeutic targets: a review. Front. Immunol. 15, 1513421 (2024).
Cha, Y. J. & Koo, J. S. Role of tumor-associated myeloid cells in breast cancer. Cells 9(8), 1785 (2020).
Nedeljković, M. & Damjanović, A. Mechanisms of chemotherapy resistance in triple-negative breast cancer—How we can rise to the challenge. Cells 8(9), 957 (2019).
Gatenby, R. A., Silva, A. S., Gillies, R. J. & Frieden, B. R. Adaptive therapy. Cancer Res. 69(11), 4894–903 (2009).
Gluzman, M., Scott, J. G. & Vladimirsky, A. Optimizing adaptive cancer therapy: Dynamic programming and evolutionary game theory. Proc. R. Soc. B Biol. Sci. 287(1925), 20192454 (2020).
Pandya, P. H., Murray, M. E., Pollok, K. E. & Renbarger, J. L. The immune system in cancer pathogenesis: Potential therapeutic approaches. J. Immunol. Res. 2016(1), 4273943 (2016).
Panetta, J. C. A mathematical model of drug resistance: Heterogeneous tumors. Math. Biosci. 147(1), 41–61 (1998).
Chisholm, R. H., Lorenzi, T. & Clairambault, J. Cell population heterogeneity and evolution towards drug resistance in cancer: Biological and mathematical assessment, theoretical treatment optimisation. Biochim. Biophys. Acta Gen. Subj. 1860(11), 2627–45 (2016).
Mehdizadeh, R., Shariatpanahi, S. P., Goliaei, B. & Rüegg, C. Targeting myeloid-derived suppressor cells in combination with tumor cell vaccination predicts anti-tumor immunity and breast cancer dormancy: An in silico experiment. Sci. Rep. 13(1), 5875 (2023).
Mehdizadeh, R., Shariatpanahi, S. P., Goliaei, B., Peyvandi, S. & Rüegg, C. Dormant tumor cell vaccination: A mathematical model of immunological dormancy in triple-negative breast cancer. Cancers 13(2), 245 (2021).
Mohammad Mirzaei, N. et al. A mathematical model of breast tumor progression based on immune infiltration. J. Pers. Med. 11(10), 1031 (2021).
Davenport, A. A. et al. Mathematical model of triple-negative breast cancer in response to combination chemotherapies. Bull. Math. Biol. 85(1), 7 (2023).
Shen, J., Li, L., Howlett, N. G., Cohen, P. S. & Sun, G. Application of a biphasic mathematical model of cancer cell drug response for formulating potent and synergistic targeted drug combinations to triple negative breast cancer cells. Cancers 12(5), 1087 (2020).
López-Alvarenga, J. C. et al. A mathematical model to optimize the neoadjuvant chemotherapy treatment sequence for triple-negative locally advanced breast cancer. Mathematics 11(11), 2410 (2023).
Gonzalez, H., Hagerling, C. & Werb, Z. Roles of the immune system in cancer: From tumor initiation to metastatic progression. Genes Dev. 32(19–20), 1267–1284 (2018).
Speiser, D. E., Ho, P.-C. & Verdeil, G. Regulatory circuits of T cell function in cancer. Nat. Rev. Immunol. 16(10), 599–611 (2016).
Donadon, M. et al. Increased infiltration of natural killer and T cells in colorectal liver metastases improves patient overall survival. J. Gastrointest. Surg. 21(8), 1226–1236 (2017).
Ghanizadeh, M., Shariatpanahi, S. P., Goliaei, B. & Rüegg, C. Mathematical modeling approach of cancer immunoediting reveals new insights in targeted-therapy and timing plan of cancer treatment. Chaos Solitons Fractals 152, 111349 (2021).
He, D., Xu, W., Li, X. & Xu, J.-X. A prognostic immunotherapy model for 4T1 breast cancer with combined cyclophosphamide and TLR agonist. J. Biol. Syst. 28(01), 65–90 (2020).
Lobo, E. D. & Balthasar, J. P. Pharmacokinetic–pharmacodynamic modeling of methotrexate-induced toxicity in mice. J. Pharm. Sci. 92(8), 1654–64 (2003).
Rihan, F. A., Rahman, D. A., Lakshmanan, S. & Alkhajeh, A. A time delay model of tumour–immune system interactions: Global dynamics, parameter estimation, sensitivity analysis. Appl. Math. Comput. 232, 606–23 (2014).
Yamamoto, Y. et al. Tumour and immune cell dynamics explain the PSA bounce after prostate cancer brachytherapy. Br. J. Cancer 115(2), 195–202 (2016).
Coventry, B. J. et al. CRP identifies homeostatic immune oscillations in cancer patients: A potential treatment targeting tool?. J. Transl. Med. 7(1), 102 (2009).
Xiao, Z., Hao, Y., Qin, T. & Han, Z. Periodic oscillation of blood leukocytes, platelets, and hemoglobin in a patient with chronic eosinophilic leukemia. Leuk. Res. 27(1), 89–91 (2003).
Tubin, S., Ashdown, M. & Jeremic, B. Time-synchronized immune-guided SBRT partial bulky tumor irradiation targeting hypoxic segment while sparing the peritumoral immune microenvironment. Radiat. Oncol. 14(1), 220 (2019).
Croghan, A. & Markovic, S. N. Fluctuation of systemic immunity in melanoma and implications for timing of therapy Alexey A. Leontovich2, Roxana S. Dronca3, Vera J. Suman2, Martin L. Ashdown4, Wendy K. Nevala1, Michael A. Thompson1, Andrew Robinson5, Lisa A. Kottschade3, Judith S. Kaur3, Robert R. McWilliams3, Leonid V. Ivanov6, Gary. Front. Biosci. 4, 958–75 (2012).
Maeda, H. & Khatami, M. Analyses of repeated failures in cancer therapy for solid tumors: Poor tumor-selective drug delivery, low therapeutic efficacy and unsustainable costs. Clin. Transl. Med. 7, 1–20 (2018).
Arabameri, A. & Arab, S. Understanding the interplay of CAR-NK cells and triple-negative breast cancer: Insights from computational modeling. Bull. Math. Biol. 86(2), 20 (2024).
Fortin, B. M. et al. Circadian control of tumor immunosuppression affects efficacy of immune checkpoint blockade. Nat. Immunol. 25(7), 1257–1269 (2024).
El-Tanani, M. et al. Circadian rhythms and cancer: implications for timing in therapy. Discov. Oncol. 15(1), 767 (2024).
Zeng, Y., Guo, Z., Wu, M., Chen, F. & Chen, L. Circadian rhythm regulates the function of immune cells and participates in the development of tumors. Cell Death Discov. 10(1), 199 (2024).
Liao, D. Z. et al. Association of delayed time to treatment initiation with overall survival and recurrence among patients with head and neck squamous cell carcinoma in an underserved urban population. JAMA Otolaryngol. Head Neck Surg. 145(11), 1001–1009 (2019).
West, J. et al. Towards multidrug adaptive therapy. Cancer Res. 80(7), 1578–1589 (2020).
Gatenby, R. A. & Brown, J. S. Integrating evolutionary dynamics into cancer therapy. Nat. Rev. Clin. Oncol. 17(11), 675–686 (2020).
Petrelli, F. et al. Adjuvant dose-dense chemotherapy in breast cancer: a systematic review and meta-analysis of randomized trials. Breast Cancer Res. Treat. 151, 251–259 (2015).
Lorigan, P. et al. Randomized phase III trial of dose-dense chemotherapy supported by whole-blood hematopoietic progenitors in better-prognosis small-cell lung cancer. J. Natl. Cancer Inst. 97(9), 666–674 (2005).
Kang, D.H. et al. The rest period between chemotherapy and immunotherapy influences the efficacy of immune checkpoint inhibitors in lung cancer. Thorac Cancer. 13(16), 2346–2354 (2022).
Peyvandi, S., Lan, Q., Lorusso, G. & Rüegg, C. Chemotherapy-induced immunological breast cancer dormancy: a new function for old drugs?. JCMT 5, N/A-N/A (2019).
Kwon, M., Jung, H., Nam, G.-H. & Kim, I.-S. The right timing, right combination, right sequence, and right delivery for cancer immunotherapy. JCR 331, 321–334 (2021).
Shariatpanahi, S. P., Shariatpanahi, S. P., Madjidzadeh, K., Hassan, M. & Abedi-Valugerdi, M. Mathematical modeling of tumor-induced immunosuppression by myeloid-derived suppressor cells: Implications for therapeutic targeting strategies. J Theor Biol 442, 1–10 (2018).
Lai, X. & Friedman, A. Combination therapy of cancer with cancer vaccine and immune checkpoint inhibitors: A mathematical model. PLoS One 12(5), e0178479 (2017).
Mokhtari, R. B. et al. Combination therapy in combating cancer. Oncotarget 8(23), 38022 (2017).
Acknowledgements
This work was supported by a grant from the Swiss National Science Foundation (310030_208136) to CR.
Author information
Authors and Affiliations
Contributions
M.D.: Conceptualization, simulation data collection, data analysis, and manuscript draft preparation. M.G.: Conceptualization, simulation data collection, and manuscript draft preparation and revision. S.P.S.: Project supervision, conceptualization, and manuscript revision. B.G.: Project administration and project supervision. R.M.: Manuscript revision. C.R.: Project supervision and manuscript revision. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Daneshparvar, M., Ghanizadeh, M., Shariatpanahi, S.P. et al. Modeling optimal timing of immunotherapy and chemotherapy to prevent resistance and recurrence in triple-negative breast cancer. Sci Rep 16, 15450 (2026). https://doi.org/10.1038/s41598-026-44611-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-44611-4
