
Abstract
Breast cancer’s primary site diversity may influence distant metastasis, yet research is scant. This study explores primary site impacts on metastasis and patient survival. We included 240,943 female breast cancer patients in the Surveillance, Epidemiology, and End Results Program (SEER) data between 2010 and 2019. The primary sites were classified as upper-inner quadrant (UIQ, C50.2), lower-inner quadrant (LIQ, C50.3), upper-outer quadrant (UOQ, C50.4), lower-outer quadrant (LOQ, C50.5), axillary tail (C50.6), overlapping region (C50.8), and the central and nipple portion (TCNP, C50.0–C50.1). The distant metastatic organs include bone, brain, liver, and lung. Chi-square tests were used to compare patient characteristics, logistic regression for identifying predictive factors. Cox regression was utilized to compare the survival among patients with different primary sites and different metastatic sites. Breast cancer’s primary site affects distant metastasis patterns and survival. Compared to the UOQ, tumors located in the axillary tail are associated with a higher risk of bone metastasis (P = 0.003) and lung metastasis (P = 0.006); tumors in the UIQ are linked to a lower risk of bone metastasis (P = 0.028), while TCNP presents a higher risk of both bone metastasis (P < 0.001) and liver metastasis (P = 0.001). Moreover, metastatic patterns affect patient survival, with brain metastasis generally indicating a poorer prognosis compared to bone metastasis (P < 0.001). When metastasis occurs in the same organ, the impact of primary site on survival prognosis becomes less significant (P > 0.05). Differences in the primary site of breast cancer shows variations in the patterns of metastasis to distant organs, which may assist in focusing attention and implementing preventive measures on organs more susceptible to distant metastasis at the early stage of breast cancer diagnosis.
Similar content being viewed by others

Introduction
Female breast cancer has surpassed lung cancer as the most commonly diagnosed cancer, with an estimated 2.3 million new cases. Its incidence and mortality rates continue to rise, posing a serious threat to women’s health and lives1. It is reported that 20–30% of breast cancer patients may develop metastasis during diagnosis and treatment2, with bone metastasis being the most common (75%), followed by metastasis to the lungs, liver, and brain2. The 5-year overall survival rate for breast cancer patients without metastasis exceeds 80%3. However, distant metastasis can lead to a dramatic reduction of this rate, dropping to only approximately 25%4. Therefore, understanding the factors influencing metastasis and its incidence in breast cancer patients is of critical importance for assessing prognosis and survival outcomes.
The primary site of cancer within the same organ can influence its metastatic pattern, thereby affecting patient prognosis. For example, proximal gastric cancer is more likely to metastasize to the liver, while distal gastric cancer tends to spread to the peritoneum5; patients with lower esophageal cancer are more prone to develop liver metastasis, while those with upper esophageal cancer are more likely to develop lung metastasis6. Previous studies have shown that breast cancer patients exhibit similar probabilities of distant organ metastasis regardless of whether the primary tumor is located in the left or right breast7, however, this study did not investigate the detailed anatomical subsite of the tumor. Further research indicates that, akin to other malignancies, the primary site within the breast may similarly impact metastatic patterns and patient prognosis8. For instance, compared to breast cancers in other regions, tumors located in the axillary tail demonstrate a higher propensity for metastasis to axillary lymph nodes9. Compared to UOQ, patients with TCNP demonstrate a higher rate of axillary lymph node positivity10, which may be associated with an increased risk of distant organ metastasis. These findings imply that breast cancers originating from different primary sites may exhibit distinct metastatic propensities, thereby influencing patient prognosis11,12. It has also been confirmed that the primary site is one of the strongest predictive factors for survival in breast cancer patients13. The above studies indicate that different primary sites of breast cancer may affect patient prognosis by influencing the risk of distant organ metastasis. However, the specific differences in distant organ metastatic patterns among different primary sites still lack in-depth investigation. In fact, breast cancer can arise from various primary sites within the breast, including the upper-outer quadrant (UOQ), lower-outer quadrant (LOQ), upper-inner quadrant (UIQ), lower-inner quadrant (LIQ), axillary tail, overlapping region, the central and nipple portion (TCNP). Furthermore, breast cancer patients exhibit significant variation in tumor histology, size, hormone receptor status, and other factors, which in turn affect metastasis and survival outcomes14. Therefore, this study aims to explore the potential association between the primary site of breast cancer and distant organ metastasis, and further analyze the impact of this association on patient survival.
To investigate the impact of different primary sites of breast cancer on distant organ metastasis, it is crucial to utilize a large, well-structured database that offers standardized data recording, strict parameter classification, and long-term follow-up. The Surveillance, Epidemiology, and End Results (SEER) database is particularly valuable in this regard, as it spans a long period, includes a large sample size, and provides detailed records of key factors influencing metastasis, such as patient age and molecular subtypes. Importantly, the SEER database precisely distinguishes between the primary sites of breast cancer (C50.0-C50.6, C50.8). Since 2010, it has included detailed information on metastasis of distant organs such as bone, brain, liver, and lung. Given these advantages, we have chosen the SEER database for this study. Our goal is to analyze the association between different primary sites and distant organ metastasis, thereby providing solid data support for extending survival and improving the prognosis of breast cancer patients.
Methods
Variables
Data for this retrospective cohort study were extracted from the Surveillance, Epidemiology, and End Results (SEER) database (https://seer.cancer.gov/). The specific SEER dataset used, released in April 2024 (based on data submitted in November 2023), covers cases from 2000 to 2021 across 17 population-based cancer registries, with detailed demographic and clinical characteristics recorded. Demographic information includes age, year of diagnosis, race, and marital status. Clinical characteristics encompass grade, primary site, laterality, metastatic sites, breast subtype, tumor size, lymph node status, survival time, treatment modalities (surgery, chemotherapy, and radiotherapy), and vital status. Regarding the determination of the primary site of breast cancer, based on the ICD-O-3 coding system (https://seer.cancer.gov/icd-o-3/) and previous literature15, we restricted the sites to the seven most common and well-defined anatomical quadrants: upper-inner quadrant (UIQ, C50.2), lower-inner quadrant (LIQ, C50.3), upper-outer quadrant (UOQ, C50.4), lower-outer quadrant (LOQ, C50.5), axillary tail (C50.6), overlapping region (C50.8), and the central and nipple portion (TCNP, C50.0–C50.1). No significant inconsistencies across years were observed in the demographic and clinical characteristics of breast cancer patients, except for tumor grade. For tumor grading, we merged the “Grade Recode (thru 2017)” and the “Derived Summary Grade 2018 (2018 +)” to obtain the final grade. Due to variations in the classification descriptions across different periods, we harmonized the grade classifications according to the SEER-based coding guidelines16 (page 18)17 (page 33–34 and page 114), as shown in Table 1.
Inclusion and exclusion criteria
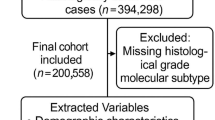
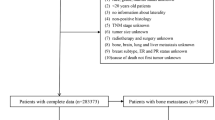
Based on the following inclusion criteria, we identified potential eligible patients: female gender, age between 18 and 80 years, years of diagnosis from 2010 to 2019, and an International Classification of Diseases for Oncology (ICD-O), 3rd Edition codes of 8500/3, indicating an infiltrating ductal carcinoma (IDC) as the pathological type. We excluded patients with breast cancer as a non-first primary tumor, cases derived from autopsy or death certificate only, and those lacking relevant clinical information (Fig. 1).

The patient selection flowchart.
Statistical analysis
Breast cancer specific survival (BCSS) was defined as the interval from the date of diagnosis to the date of death due to breast cancer. Overall survival (OS) was defined as the interval from the date of diagnosis to the date of death from any cause. The results were reported using hazard ratios (HRs) with 95% CIs. We used X-tile to determine the optimal cut-off point of age as 72 years old. We categorized the continuous variable of age into two levels: < 72 years old and ≥ 72 years old (Supplementary Fig. 1). Similarly, we determined the optimal cut-off point of tumor size as 29 mm, and categorized the continuous variable of tumor size into two levels: < 29 mm and ≥ 29 mm (Supplementary Fig. 2). Chi-square tests were used to compare the differences in clinical characteristics between patients with bone, brain, liver, and lung metastasis and those without metastasis. Logistic regression analysis was conducted to explore the impact of different primary sites on distant organ metastasis. The Cox proportional hazards regression model was used to compare survival between different metastatic sites and primary sites. Statistical analyses were performed using SPSS version 26.0. Two-sided tests were applied, with P < 0.05 considered statistically significant.
Results
Patient characteristics
A total of 240,943 female breast cancer patients were included in this study, among which 5,009 had bone metastasis, 509 had brain metastasis, 2,178 had liver metastasis, and 2,406 had lung metastasis. The baseline characteristics of the patients are shown in Table 2. The analysis results also revealed that patients with distant metastasis had a median survival time shorter than the overall median survival time. Among the overall population, the median survival time was approximately 65 months (95% CI: 39.09, 97.97). For patients with bone, brain, liver, and lung metastasis, the median survival times were approximately 32 months (95% CI: 14.36, 53.59), 12 months (95% CI: 3.37, 30.23), 25 months (95% CI: 8.52, 46.80), and 25 months (95% CI: 9.60, 45.59), respectively. Furthermore, patients with distant metastasis were younger, mostly white, unmarried, and mostly had the HR + /HER2- molecular subtype, followed by HR + /HER2 + and TNBC, with HR-/HER2 + being the least common. The majority of patients with distant metastasis have their primary site in the UOQ, primarily on the left side, with a higher grade, larger tumor size, and more frequent positive regional lymph nodes. In terms of treatment, a higher proportion of patients across all groups underwent surgery for the primary tumor; however, after metastasis, there was a marked decrease in the number of patients receiving surgical treatment. For radiotherapy, patients with brain metastasis were more likely to receive radiotherapy, whereas patients with bone, liver, and lung metastasis were less inclined to undergo radiotherapy. Regarding chemotherapy, a higher proportion of patients with distant organ metastasis received chemotherapy compared to those who did not.
Association between patient characteristics and distant metastasis sites
As can be seen from the aforementioned table, among all patients with distant metastasis, those with primary sites in the UOQ of the breast were the most numerous. In bone metastases, 36% of cases originated from the UOQ. Similarly, 36% of brain metastases, 38% of liver metastases, and 36% of lung metastases originated from the UOQ (Fig. 2). Then, we observed the ratio of tumor metastases to the number of patients with tumors originating from different primary sites; the results are shown in Fig. 3. Overall, the axillary tail region and TCNP region are more prone to metastasis, while regardless of the primary site, bone metastasis was the most common, followed by lung metastasis and liver metastasis, and brain metastasis.

Proportion of primary sites in different distant organ metastases. UOQ, upper-outer quadrant; LOQ, lower-outer quadrant; UIQ, upper-inner quadrant; LIQ, lower-inner quadrant; overlapping, overlapping region; TCNP, the central and nipple portion. The percentages represent the proportion of patients from each primary site among those with metastasis to a specific organ.

Probability of distant organ metastasis in breast cancer by different primary sites. UOQ, upper-outer quadrant; LOQ, lower-outer quadrant; UIQ, upper-inner quadrant; LIQ, lower-inner quadrant; overlapping, overlapping region; TCNP, the central and nipple portion. The percentages represent the proportion of patients with metastasis to each distant organ among those with a specific primary site.
To further investigate the factors that may influence distant organ metastasis, we first performed univariate logistic regression analysis on patients with metastasis (Supplementary Table 1). The results showed that race, marital status, breast subtype, primary site, tumor grade, tumor size, and lymph node status were potential factors influencing bone metastasis. Brain, liver, and lung metastasis were primarily affected by age, race, marital status, breast subtype, primary site, tumor grade, tumor size, and lymph node status.
We included variables with a P < 0.05 from the univariate logistic regression analysis into the multivariate logistic regression analysis (Table 3). The results are as follows:
Bone Metastasis: Marital status, breast subtype, primary site, tumor grade, tumor size, and lymph node status were independent predictors of bone metastasis. Compared to the UOQ, the risk of bone metastasis was higher in the LIQ (OR = 1.150; 95% CI, 1.004–1.318; P < 0.05), axillary tail (OR = 1.718; 95% CI, 1.209–2.440; P < 0.05), overlapping region (OR = 1.220; 95% CI, 1.134–1.313; P < 0.05), and TCNP (OR = 1.486; 95% CI, 1.325–1.666; P < 0.05), while the risk of bone metastasis was lower in the UIQ (OR = 0.889; 95% CI, 0.800–0.987; P < 0.05).
Brain metastasis: Age, marital status, breast subtype, tumor grade, tumor size, and lymph node status were independent predictive factors for brain metastasis. Compared to the UOQ, TCNP (OR = 1.484; 95% CI, 1.054–2.090; P < 0.05) is more likely to develop brain metastasis.
Liver metastasis: Marital status, breast subtype, primary site, tumor grade, tumor size, and lymph node status are independent predictive factors for liver metastasis. Compared to the UOQ, the risk of liver metastasis is higher in the overlapping region (OR = 1.165; 95% CI, 1.048–1.296; P < 0.05) and TCNP (OR = 1.333; 95% CI, 1.123–1.583; P < 0.05). The risk of liver metastasis is lower in the UIQ (OR = 0.762; 95% CI, 0.648–0.895; P < 0.05).
Lung metastasis: Age, race, marital status, breast subtype, primary site, tumor grade, tumor size, and lymph node status were independent predictive factors for lung metastasis. Compared to the UOQ, the risk of lung metastasis is higher in the LIQ (OR = 1.247; 95% CI 1.033–1.505; P < 0.05), LOQ (OR = 1.207; 95% CI 1.209–1.415; P < 0.05), axillary tail (OR = 1.903; 95% CI 1.204–3.008; P < 0.05), overlapping region (OR = 1.265; 95% CI 1.142–1.402; P < 0.05), and TCNP (OR = 1.322; 95% CI 1.118–1.563; P < 0.05).
Our study results suggest that the primary site of breast cancer is a significant factor influencing distant organ metastasis in female patients with invasive ductal carcinoma (IDC). Overall, for bone, liver, and lung metastasis, the overlapping region and TCNP are the most common regions for metastasis, while the axillary tail is more likely to metastasize to the bone and lung.
To assess the robustness of the findings, we constructed two additional models (Supplementary Table 2). The first was a multivariate logistic regression model adjusted only for demographic variables (Model 1). The second was a multivariate logistic regression model adjusted for all variables, with the cut-off points for age and tumor size modified to clinically more common thresholds (age cut-off point set to 50 years; tumor size cut-off point set to 20 mm) (Model 3). The results across these four models, the two newly constructed models along with the univariate and original multivariate logistic models, were largely consistent. In the model before modifying the cut-off points for age and tumor size (Model 2), compared to the UOQ, the LIQ showed a higher risk of bone metastasis, while the overlapping region did not show a higher risk of brain metastasis. In contrast, after modifying the cut-off points (Model 3), LIQ no longer demonstrated a higher risk of bone metastasis compared to UOQ, while the overlapping region showed a higher risk of brain metastasis. All other statistical results remained consistent across models. These sensitivity analyses confirm that our findings are robust.
Development of nomograms for predicting distant organ metastasis
To facilitate the clinical use of patient characteristics in predicting the risk of distant organ metastasis, we integrated multiple variables to construct nomograms for predicting distant organ metastasis in breast cancer patients (Supplementary Fig. 3). Based on variables with independent predictive value from the aforementioned multivariate logistic analysis, we ultimately selected key factors including age, race, marital status, breast subtype, primary site, grade, lymph node status, and tumor size for inclusion in the nomograms. These integrated models are presented graphically, allowing for quantification of individualized metastasis risk for each patient. These will assist clinicians in rapidly identifying high-risk patients, enabling more proactive and targeted follow-up strategies and interventions, thereby achieving more precise prevention and management.
Impact of primary site on distant organ metastasis in different breast subtypes
We then performed a subgroup analysis based on the molecular subtypes of the patients. The results are shown in Supplementary Table 3. Regardless of the molecular subtype, the UIQ was less likely to develop distant organ metastasis compared to the UOQ. In contrast, the axillary tail, overlapping region, and TCNP had a higher tendency for distant metastasis, consistent with the overall study findings.
Impact of site and number of different organ metastases on patient survival
We further analyzed the OS of patients with metastasis to different organs (Table 4). Among the 240,943 patients included, those with isolated bone metastasis had significantly better survival (Median OS 38.00 months) than those with isolated metastasis to other distant organs (P < 0.05), especially those with brain metastasis (Median OS 13.00 months, HR = 3.024; 95% CI 2.392–3.822; P < 0.05). Overall, the more distant metastasis sites, the worse the prognosis. The BCSS results were consistent with the overall survival results (Supplementary Table 4).
Survival differences in metastatic breast cancer patients with different primary sites
We further investigated the prognosis of breast cancer patients with different primary sites. First, we analyzed whether the primary site affects the overall survival (OS) of IDC patients with metastasis to the same distant organ. Kaplan–Meier survival curves analysis (Supplementary Fig. 4) revealed that, except for patients with brain metastasis, there were no significant differences in overall survival (OS) or breast cancer-specific survival (BCSS) among different primary sites for patients with metastasis to other distant organs (bone, liver, lung) (P > 0.05). Further multivariate Cox regression analysis (Table 5) demonstrated similar results. Only among patients with brain metastasis, compared to those with a primary site in the UOQ, patients with their primary site in the UIQ had worse OS, whereas patients with primary site in other regions showed similar OS. Similarly, among patients with metastasis to other distant organs (bone, liver, lung), the primary site showed no significant impact on OS. The results for BCSS are presented in Supplementary Table 5, indicating no significant influence of primary site on BCSS in patients with bone, brain, liver, or lung metastasis. These findings suggest that when breast cancer patients develop metastasis to the same distant organ, the impact of primary site on survival is limited.
Finally, we studied whether metastasis to different distant organs from the same primary site affects the OS of IDC patients (Table 6). For patients with a primary site in the UOQ, those with brain or lung metastasis had worse overall survival compared to those with bone metastasis. In patients with a primary site in the UIQ, those with brain metastasis (HR = 7.279; 95% CI 4.074–13.006; P < 0.05) had significantly poorer overall survival compared to those with bone metastasis. For patients with a primary site in the LIQ, those with lung metastasis had worse overall survival than those with bone metastasis. For Patients with a primary site in the overlapping region, compared to those with bone metastasis, those with brain, liver, or lung metastasis had poorer overall survival, especially those with brain metastasis (HR = 5.841; 95% CI 3.534–9.656; P < 0.05) . No significant differences in overall survival were observed for other groups. The BCSS results were consistent with the OS results (Supplementary Table 6). This result suggests that, among breast cancer patients with metastasis to different distant organs from the same quadrant, those with brain metastasis have significantly poorer survival compared to those with metastasis to other distant organs.
Discussion
This study, based on a large-scale, retrospective cohort, shows that breast cancer has the highest incidence in the UOQ and the lowest incidence in the axillary tail. These results are consistent with previous studies14,18. There is a strong correlation between different primary sites of breast cancer and distant organ metastasis. Regardless of the primary site, breast cancer patients are most likely to develop bone metastasis. Compared to the UOQ, the UIQ is less prone to distant metastasis, while other regions are more likely to develop bone, brain, liver, and lung metastasis. The survival analyses indicated that the more distant metastasis sites, the worse their OS. Once metastasis occurs, the primary site has minimal impact on survival. Among patients with metastasis to the bone, brain, liver, or lung, those with bone metastasis tended to have a longer survival period compared to patients with metastasis to other organs.
The study results indicate that bone metastasis remains the most common form of metastasis in breast cancer, which is consistent with previous research findings19,20. A study by Liu et al. also found that, even when distant lymph node metastasis was included, bone was the most frequent metastatic site (42.5%), followed by the lung (19.8%), distant lymph nodes (18.4%), liver (15.4%), and brain (3.9%)21. Moreover, the primary site of breast cancer influences the pattern of distant metastasis. Tumors located in TCNP and the axillary tail of the breast are more likely to develop distant organ metastasis compared to those in the UOQ, whereas tumors in the UIQ are less likely to metastasize distantly than those in the UOQ.
The exact reasons for the distinct patterns of distant organ metastasis across different primary sites remain unclear. The association between the primary site and distant metastasis likely originates from a multilevel, interrelated biological framework, in which the ultimate metastatic risk results from a complex interplay between local tumor characteristics and host physiological status22.
First, the relationship between the primary site of breast cancer and distant metastasis may be closely related to the anatomical location of the primary tumor. The axillary tail region is adjacent to the thoracic wall vasculature23, which may facilitate the spread of tumor cells via the vascular system, thereby increasing the risk of metastasis to other organs from this region. This may explain why breast cancer located in the axillary tail exhibit a higher metastatic propensity.
Second, the pattern of lymphatic drainage from the primary site may also affect the risk of distant metastasis. The axillary lymph nodes are generally considered as the primary sentinel lymph nodes for the entire breast24. The distance and pathway from the primary site to the axillary sentinel lymph node thus become one of the key factors influencing lymph node metastasis and, subsequently, distant organ metastases25,26.Studies have suggested that the shorter the distance from the primary site to the sentinel lymph node, the higher the likelihood of lymph node metastasis27. Therefore, patients with invasive breast cancer originating in the axillary tail demonstrate a higher risk of axillary lymph node positivity25, which may subsequently lead to a higher risk of distant metastasis. This finding is consistent with our results. Similarly, since the sentinel lymph nodes for breast cancers in the UIQ are also predominantly located in the axilla24,28, the lymphatic vessels from the UIQ must traverse the lymphatic network of the UOQ before reaching the axilla29. Therefore, compared to the more direct route from the UOQ, the longer and less efficient drainage pathway from the UIQ may result in a slower and less extensive spread of tumor cells to distant organs, thereby contributing to a lower metastatic risk. In summary, the distance between the primary site and the axillary sentinel lymph nodes may partially explain our findings: compared to the UOQ, tumors in the UIQ are associated with a lower risk of distant organ metastasis, while those in the axillary tail carry a higher risk.
Finally, Several studies have found that inflammation also plays a crucial role in the development and metastasis of breast cancer30,31. Some research has shown that blocking inflammatory feed-forward loops can inhibit the occurrence of breast cancer and its metastasis to the liver and lung32. Additionally, studies have suggested that certain areas may be more prone to inflammation, such as periductal mastitis (PDM), which is more common in the central areola region, and granulomatous lobular mastitis (GLM), which primarily affects the peripheral quadrants of the breast33,34. Therefore, the increased incidence of inflammation in these regions may explain why breast cancer patients in the axillary tail and TCNP are more likely to develop bone, brain, liver, and lung metastasis. Our study also found that elderly patients are more likely to develop lung metastasis, which could be associated with the higher prevalence of chronic pulmonary inflammation, such as chronic obstructive pulmonary disease (COPD), in older patients35. Several studies have suggested that in mouse models, the potential mechanism involving inflammatory cells, particularly neutrophils, supports the initiation of metastasis and promotes the awakening of dormant cancer cells in the lungs36,37. Moreover, the microenvironment in distant organs may be more susceptible to metastasis due to the presence of a pro-tumor inflammatory environment, which suppresses immune defenses in the microenvironment2. This may contribute to the increased likelihood of distant organs being affected by metastasis.
The aforementioned mechanisms may collectively influence distant metastasis of tumors. This integrated multi-line reasoning framework provides a more comprehensive and profound biological explanation for understanding the findings of this study and their clinical relevance.
In this study, we further analyzed the relationship between the primary site and distant organ metastasis across different molecular subtypes of breast cancer. Our findings reveal that, for patients with triple-negative breast cancer (TNBC), the risk of metastasis to bone, brain, liver, and lung differs according to the primary site. A study by Raghavendra AS et al. suggested that TNBC patients show a higher risk of brain metastasis38, which is consistent with our results. However, another study on TNBC found that the primary site had no effect on the metastasis to bone, brain, liver, or lung39, which is inconsistent with our findings. This discrepancy may be attributed to the fact that our study exclusively included patients with IDC. It is noteworthy that the risk of metastasis is generally higher in the axillary tail and TCNP compared to the UOQ. Given that metastasis is the leading cause of breast cancer-related mortality40, this could potentially impact patient survival prognosis41,42.
Consistent with other studies, our research found that among patients with metastasis to a single organ, those with brain metastasis had the shortest survival, while those with bone metastasis had relatively longer survival and better prognosis43,44,45. Our study also found that patients with metastasis to more organs had a shorter survival compared to those with fewer metastatic sites. Furthermore, we observed that any involvement of the brain in distant metastasis was associated with a generally poorer prognosis, even worse than in patients with multiple metastases that did not involve the brain. This conclusion is similar to the results of previous research45,46.
We also assessed the survival of female breast cancer patients with different primary tumor sites and distant metastasis locations. According to previous studies, factors such as older age, TNBC, and higher grade are considered risk factors for survival14. However, the impact of different primary tumor sites on the survival of patients with metastasis has not been extensively studied. We first evaluated the effect of different primary sites on survival in patients with metastasis to the bone, brain, liver, and lung. The results indicated that once metastasis occurs to the same distant organ, the impact of primary site on survival is minimal. This suggests that predicting the metastasis pattern in breast cancer patients is particularly important. We further analyzed survival differences in patients with the same primary site but different distant metastasis organs. We found that for patients with primary sites in the UIQ, UOQ, and overlapping region, those with brain metastasis had significantly poorer survival compared to those with bone metastasis. This aligns with previous conclusions that brain metastasis is associated with the worst survival outcomes46. However, for patients with a primary site in the LIQ, those with lung metastasis had the worst survival, rather than brain metastasis.
The findings of this study suggest that during the diagnosis and treatment process, special attention should be given to early screening for breast cancer, as well as the prediction of distant organ metastasis during disease progression, as these factors may significantly impact patient survival. However, this study has several unavoidable limitations: 1. Although the SEER database is subject to quality control and integrity assessment, due to its large scale, certain potential confounding factors are not incorporated into the analysis, including dietary patterns, physical activity habits, smoking and alcohol consumption, accessibility to medical resources, treatment adherence, variations in adjuvant treatment regimens, and psychological stress levels, and other factors. 2. The data used in this study are only updated through 2019, which may not fully reflect the latest advances in breast cancer treatment. 3. We lack validation from multi-center datasets. Therefore, future studies need to incorporate multi‑center, large‑sample, prospective cohort data to verify the reliability of the findings. 4. The data in this study originate from the United States. Due to differences across countries in ethnicity, diet, climate, geographic environment, and other factors, we recommend that readers interpret and reference these results with prudence, and remain attentive to future relevant research data derived from other populations for validation.
Conclusion
The aim of this study was to explore the relationship between the primary site in breast cancer and distant organ metastasis, as well as its impact on prognosis. Our findings suggest that the primary site of breast cancer is a significant factor influencing the occurrence of distant organ metastasis. Breast cancer located in the axillary tail, overlapping region, and TCNP is more likely to metastasize to distant organs. Regardless of the molecular subtype, the overlapping and TCNP are more prone to metastasis to the bone, brain, liver, and lung. Metastasis to different distant organs affects patient survival, but once metastasis to a particular organ occurs, the primary site no longer plays a significant role in survival outcomes. Additionally, the number of distant metastasis sites is inversely correlated with survival; patients with more metastasis sites generally have shorter survival. However, once brain metastasis occurs, patients have the poorest survival outcomes.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Sung, H., Ferlay, J. & Siegel, R. L. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 71(3), 209–249 (2021).
Liang, Y. et al. Metastatic heterogeneity of breast cancer: Molecular mechanism and potential therapeutic targets. Semin. Cancer Biol. 60, 14–27 (2020).
Guo, L. et al. Breast cancer heterogeneity and its implication in personalized precision therapy. Exp. Hematol. Oncol. 12(1), 3 (2023).
Coleman, M. P. et al. Cancer survival in five continents: A worldwide population-based study (CONCORD). Lancet Oncol. 9(8), 730–756 (2008).
Wang, L. et al. Subsite-specific metastatic organotropism and risk in gastric cancer: A population-based cohort study of the US SEER database and a Chinese single-institutional registry. Cancer Med. 12(19), 19595–19606 (2023).
Ai, D. et al. The effect of tumor locations of esophageal cancer on the metastasis to liver or lung. J. Thorac. Dis. 11(10), 4205–4210 (2019).
Kazemzadeh, F. & Snoek, J. A. A. Association of metastatic pattern in breast cancer with tumor and patient-specific factors: A nationwide autopsy study using artificial intelligence. Breast Cancer 31(2), 263–271 (2024).
Wei, Y. et al. Analysis of the relationship between primary tumor site and clinicopathological characteristics and survival prognosis of breast cancer patients based on SEER database. Clin. Breast Cancer 24(8), 728–745 (2024).
Qian, F. et al. Establishment of a logistic regression model nomogram for clinicopathological characteristics and risk factors with axillary lymph node metastasis in T1 locally advanced breast cancer: A retrospective study. Gland Surg. 13(6), 871–884 (2024).
Chen, K. et al. Development of nomograms to predict axillary lymph node status in breast cancer patients. BMC Cancer 17(1), 561 (2017).
Li, Y. et al. Prognostic significance of molecular subtype, metastatic site and primary tumor surgery for survival in primary metastatic breast cancer: A SEER-based study. Medicine 100(27), e26619 (2021).
Nam, Y. H. A study on the factors and prediction model of triple-negative breast cancer for public health promotion. Diagnostics https://doi.org/10.3390/diagnostics13223486 (2023).
Abdalnabi, N. & Adebiyi, A. Impact of tumor location on predicting early-stage breast cancer patient survivability using explainable machine learning models. JCO Clin. Cancer Inform. 9, e2400178 (2025).
Wei, Y. et al. Analysis of the relationship between primary tumor site and clinicopathological characteristics and survival prognosis of breast cancer patients based on SEER database. Clin. Breast Cancer https://doi.org/10.1016/j.clbc.2024.08.021 (2024).
Milano, A. F. Breast cancer: 20-Year comparative mortality and survival analysis by age, sex, race/ethnicity, stage, grade, disease duration, selected ICD-O-3 oncophenotypes, and cohort entry time-period. J. Insur. Med. 50(2), 80–122 (2023).
Seer, E.C.o. SEER RESEARCH DATA RECORD DESCRIPTION: Nov 2020 Submission. 2021; Available from: https://seer.cancer.gov/data-software/documentation/seerstat/nov2020/TextData.FileDescription.pdf
Jennifer Ruhl, M., RHIT, CCS, ODS-C, NCI SEER Jim Hofferkamp, ODS-C, NAACCR. Grade Coding Instructions and Tables v3.3. 2025; Available from: https://www.naaccr.org/wp-content/uploads/2025/12/Version-3.3.Grade-Manual.pdf?v=1769531043
Hwang, K. T. et al. Poor prognosis of lower inner quadrant in lymph node-negative breast cancer patients who received no chemotherapy: A study based on nationwide Korean Breast Cancer Registry Database. Clin. Breast Cancer 17(4), e169–e184 (2017).
Yu, X. & Zhu, L. Nanoparticles for the treatment of bone metastasis in breast cancer: Recent advances and challenges. Int. J. Nanomed. 19, 1867–1886 (2024).
Pang, L. et al. Bone metastasis of breast cancer: Molecular mechanisms and therapeutic strategies. Cancers https://doi.org/10.3390/cancers14235727 (2022).
Liu, K. et al. Patterns of distant metastasis and survival outcomes in de novo metastatic breast cancer according to age groups. Front Endocrinol. (Lausanne) 15, 1385756 (2024).
Diamantopoulou, Z. & Castro-Giner, F. The metastatic spread of breast cancer accelerates during sleep. Nature 607(7917), 156–162 (2022).
Pluguez-Turull, C. & Del Toro, C. Pseudoaneurysm in the axillary tail of the breast after a core needle biopsy. Eur. J. Breast Health 20(4), 313–315 (2024).
Machado, P. & Liu, J. B. Anatomy versus physiology: Is breast lymphatic drainage to the internal thoracic (internal mammary) lymphatic system clinically relevant?. J. Breast Cancer 26(3), 286–291 (2023).
Cordeiro, M. R. & Gante, I. Intramammary tumor location and ipsilateral lymphatic spread in early breast cancer patients using one-step nucleic acid amplification (OSNA) assay. Breast J. 2024, 4864443 (2024).
Zhang, M. et al. Patterns and prognostic implications of distant metastasis in breast cancer based on SEER population data. Sci. Rep. 15(1), 26717 (2025).
Xia, S. et al. Super-resolution ultrasound imaging of intranodal lymphatic sinuses for predicting sentinel lymph node metastasis in breast cancer: A preliminary study. Eur. Radiol. 35(10), 6079–6088 (2025).
Coroneos, C. J. et al. Anatomy and physiology of the sentinel lymph nodes of the upper extremity: Implications for axillary reverse mapping in breast cancer. J. Surg. Oncol. 123(4), 846–853 (2021).
Johnson, A. R. et al. The all but forgotten mascagni-sappey pathway: Learning from immediate lymphatic reconstruction. J. Reconstr. Microsurg. 36(1), 28–31 (2020).
Yofe, I. & Shami, T. Spatial and temporal mapping of breast cancer lung metastases identify TREM2 macrophages as regulators of the metastatic boundary. Cancer Discov. 13(12), 2610–2631 (2023).
Domínguez-Cejudo, M. A., Gil-Torralvo, A. & Cejuela, M. Targeting the tumor microenvironment in breast cancer: Prognostic and predictive significance and therapeutic opportunities. Int. J. Mol. Sci. 24(23), 16771 (2023).
Lu, Z. et al. Simultaneous inhibition of breast cancer and its liver and lung metastasis by blocking inflammatory feed-forward loops. J. Control Release 338, 662–679 (2021).
Zhou, F. & Liu, L. Periductal mastitis, a disease with distinct clinicopathological features from granulomatous lobular mastitis. J. Inflamm. Res. 17, 3815–3823 (2024).
Jiang, L. et al. Clinicopathological features of granulomatous lobular mastitis and mammary duct ectasia. Oncol. Lett. 19(1), 840–848 (2020).
Cosio, M. G., Cazzuffi, R. & Saetta, M. Is chronic obstructive pulmonary disease a disease of aging?. Respiration 87(6), 508–512 (2014).
Albrengues, J. & Shields, M. A. Neutrophil extracellular traps produced during inflammation awaken dormant cancer cells in mice. Science 361(6409), 4227 (2018).
Wculek, S. K. & Malanchi, I. Neutrophils support lung colonization of metastasis-initiating breast cancer cells. Nature 528(7582), 413–417 (2015).
Raghavendra, A. S. & Ibrahim, N. K. Breast cancer brain metastasis: A comprehensive review.. JCO Oncol. Pract. 20(10), 1348–1359 (2024).
Zhao, S. et al. Clinicopathologic features and prognoses of different histologic types of triple-negative breast cancer: A large population-based analysis. Eur. J. Surg. Oncol. 44(4), 420–428 (2018).
Kos, K. et al. Tumor-educated T(regs) drive organ-specific metastasis in breast cancer by impairing NK cells in the lymph node niche. Cell Rep. 38(9), 110447 (2022).
Gou, Z. C. et al. Decreased survival in patients with carcinoma of axillary tail versus upper outer quadrant breast cancers: A SEER population-based study. Cancer Manag. Res. 10, 1133–1141 (2018).
Siotos, C. et al. Tumor site and breast cancer prognosis.. Clin. Breast Cancer 18(5), e1045–e1052 (2018).
Li, C. et al. Novel models by machine learning to predict prognosis of breast cancer brain metastases.. J. Transl. Med. 21(1), 404 (2023).
Ivanova, M. & Porta, F. M. Breast cancer with brain metastasis: Molecular insights and clinical management. Genes 14(6), 1160 (2023).
Ibragimova, M. K. & Tsyganov, M. M. Organ-specificity of breast cancer metastasis. Int. J. Mol. Sci. 24(21), 15625 (2023).
Lin, C. et al. Subdivision of M1 stage for de novo metastatic breast cancer to better predict prognosis and response to primary tumor surgery. J. Natl. Compr. Canc. Netw. 17(12), 1521–1528 (2019).
Funding
This work was supported by Fundamental Research Funds for the Central public welfare research institutes (ZZ15-YQ-063), Henan Provincial College Students’ Innovation Training Program Project (202510472026), Henan Provincial Selective Research Funding Program for Returned Scholars Studying Abroad (HNLX202620) and Natural Science Foundation of Henan (Grant No. 252300423181).
Author information
Authors and Affiliations
Contributions
Haijun Zhu: Writing—Review & Editing, Writing—Original Draft. Mengxue Wang: Methodology, Writing—Review & Editing, Writing—Original Draft. Mengran Chen: Formal analysis, Methodology, Validation. Peipei Cai: Data Curation, Resources, Software. Jiaxin Mao: Investigation, Funding acquisition. Yonghui Zhao: Data Curation, Formal analysis, Investigation. Pengwei Wang: Project administration, Supervision. Ruixin Cao: Formal analysis, Methodology, Validation. Lili Zang: Conceptualization, Resources, Software. Lilin Wang: Formal analysis, Investigation, Methodology. Jun Su: Conceptualization, Software, Visualization. Pengfei Yang: Data Curation, Funding acquisition, Project administration, Supervision, Writing—Review & Editing. Dandan Liu: Funding acquisition, Conceptualization
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The data for this study was sourced from the Surveillance, Epidemiology, and End Results (SEER) public database, which is openly accessible. Patient information has been de-identified, thus exemption approval was granted by the ethics committee of Xinxiang Medical University. This research complies with the Helsinki Declaration.
Consent to Participate
Participate consent was waived due to the approval of using a publicly accessible database and the retrospective nature of the research.
Informed consent
Due to the approval of using a publicly accessible database and the retrospective nature of the research, informed consent was waived.
Research involving human participants and/or animals
This article does not contain any research conducted by the authors on human participants or animals.
Clinical significance
This large-scale cohort study identified significant associations between primary site in breast cancer and patterns of distant metastasis, with bone metastasis being the most prevalent. Notably, our findings suggest that the inflammatory tumor microenvironment may facilitate metastasis. Predicting metastatic sites holds critical clinical value for guiding targeted therapies and improving patient prognosis.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhu, H., Wang, M., Chen, M. et al. Differences in distant metastasis risk of breast cancer originating from various primary sites: a retrospective analysis based on the SEER database. Sci Rep 16, 14474 (2026). https://doi.org/10.1038/s41598-026-44790-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-44790-0
