
Abstract
Migration to Europe has been rising in recent years and is associated with higher HIV vulnerability due to overlapping social and structural barriers. New cases among migrants have been steadily increasing, and for the first time in Portugal, there were more cases among migrants than among non-migrants in 2023. This study aims to compare sociodemographic, behavioural, clinical, and viral genomic characteristics of non-migrant and migrant MSM newly diagnosed with HIV-1 in Portugal (2023–2024), as well as the composition of Transmission Clusters (TC) to which they belong. Between June 2023 and December 2024, 60 MSM were recruited upon HIV-1 reactive screening in a community centre in Lisbon. Sociodemographic and behavioural data were collected through a questionnaire. A blood sample was collected for viral load measurement and HIV-1 genomic sequencing. TC were identified using a branch support ≥ 90% and iterating between 1.5%, 2.5%, 3.5%, 4.5%, 5.5% and 6.5% genetic distances. Among the 60 MSM newly diagnosed with HIV in our 2023–2024 community-based sample, 70% were migrants, of whom 60% were from Latin America and 10% from other regions. The results showed significant differences in age at diagnosis, district of residence, and HIV-1 subtype between non-migrants and migrants, while sexual behaviours, testing patterns, and STI prevalence were similar across the two groups. No difference between the proportion of non-migrant and migrant MSM in TC was found. Notably, phylogenetic analysis suggests that migrant MSM are mainly related to other migrant MSM and outside Portugal. In contrast, non-migrant MSM were more frequently found in mixed clusters. All Surveillance drug resistance mutations (SDRM) in TC were related to migrant MSM. Findings from this single community-based centre suggest that recent HIV-1 epidemiology among MSM has shifted towards an increased proportion of migrants in MSM HIV diagnosis, who are primarily involved in sexual networks with other migrants. To effectively address these current dynamics, Portugal should explore strategies to improve early and accessible PrEP, STI, and HIV testing for the migrant MSM communities.
Similar content being viewed by others


Introduction
In 2023, 1.3 million people were infected with HIV, above the UNAIDS target of ≤ 370,000 new infections by 20251. The EU/EEA incidence was 5.3 per 100,0002, while Portugal reported a higher rate of 8.2 cases per 100,000 (876 new cases)3. HIV-1 new diagnosis in the EU/EEA were similar among men who have sex with men (MSM) and heterosexual men and women (46.7% and 46.1% of diagnoses with a known mode of transmission, respectively)2. Between 2014 and 2023, diagnoses among EU/EEA-born MSM have decreased by 51%, while diagnoses among migrant MSM increased by 37.7%2. In Portugal, MSM accounted for 41.7% of new diagnoses and heterosexuals for 49%. From 2014 to 2023, MSM cases rose (32.2% to 41.7%), while heterosexual transmission decreased (59% to 49%)3. Although no data is available for migrant MSM in Portugal in 2023, the report shows a reduction among all non-migrants (59%), and a significant increase in cases among all migrants from Latin America (147%)(2014–2023)3. In 2023, for the first time, new cases among migrants (466) exceeded those among Portuguese non-migrants (410)3. Migration to Europe, including Portugal, has risen in recent years4,5, with greater HIV vulnerability linked to social and structural barriers that limit access to care and prevention6,7.
Integrating HIV-1 surveillance with genomic data to identify transmission clusters (TCs) helps trace how HIV-1 spreads and reveals hidden dynamics8,9. One study found 40.6% of infections among Brazilian migrants linked to Portuguese partners10. Another Portuguese study found no differences between non-migrant and migrant MSM inside and outside TC, suggesting comparable involvement in transmission networks11. However, to our knowledge, no studies have explored HIV TC among MSM in Portugal to assess differences between migrants and non-migrants or their transmission links.
In this context, this study aims to compare sociodemographic, behavioural, clinical, and viral genomic characteristics of non-migrant and migrant MSM newly diagnosed with HIV-1 in Portugal (2023–2024), and analyses the composition of TC to which they belong.
Materials and methods
Ethics
The study was approved by the Ethics Review Board of the Institute of Hygiene and Tropical Medicine, NOVA University of Lisbon (IHMT/UNL)(Approval No. 7.23). Potential participants were informed about the study in the visit to confirm the reactive HIV screening result and were invited to participate. The participants provided written informed consent to take part in this study. All procedures were performed in accordance with relevant guidelines/regulations. All data collected were anonymized.
Research sample
In a community centre in Lisbon, between June 2023 and December 2024, 60 MSM were recruited upon HIV-1 reactive screening, were ≥ 18 years old, and drug-naïve. This MSM community-based centre offers free screening for HIV and other sexually transmitted infections (STIs), counselling, and healthcare referral12.
Data collection
Sociodemographic and behavioural data were collected through a questionnaire administered by a registered nurse. 5 ml of blood was collected for viral load measurement and viral genomic analysis, and the plasma was separated by centrifugation and frozen at -80 °C. Data was anonymised using an alphanumeric code.
RNA extraction, PCR amplification, sequencing, and genome assembly
Viral RNA was extracted with QIAamp Viral RNA Kit and amplified with Taq Platinum High Fidelity enzyme. The regions for amplification included Protease (PR) (amino acid 1–99 (HXB2: 2253–2549)), Reverse Transcriptase (RT) (amino acid 1-238 (HXB2: 2550–3263)), and Integrase (INT) (amino acid 1-267 (HXB2: 4230–5030)). PCR product verification by electrophoresis (PR/RT: 1112 bp and IN: 1254 bp) was performed, and purified using AMPure XP beads (Beckman Coulter, USA). DNA concentrations were normalised to 80 ng/µL for each fragment (PR, RT, IN). DNA Libraries were prepared using Ligation Sequencing Kit (SQK-NBD114.24) and Non-migrant Barcoding Expansion 1–24 Kit (R10.4.1), both from Oxford Nanopore Technologies. Sequencing was carried out on a MinION Mk1C device. Reads were mapped and aligned to sample-specific reference sequences (pol-PR/RT/IN regions) using Geneious Prime v2024.0.5. One consensus nucleotide sequence per isolate was generated. Codons with mixed nucleotides ≥ 5% of the viral population were labelled using IUPAC ambiguity codes.
HIV-1 subtyping
HIV-1 subtype analyses were performed using three algorithms (REGA V.3.013, Comet13 and Scuel14. The assigned subtype was based on the concordance of the three algorithms. If there was no agreement, the majority assignment (≥ 2 algorithms) was considered.
Analysis of transmitted drug resistance (TDR)
The consensus FASTA file was submitted to the Calibrated Population Resistance tool at HIV Drug Resistance Database, Stanford University (https://hivdb.stanford.edu/cpr/) to evaluate surveillance drug resistance mutations (SDRM) to nucleotide reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), and integrase strand transfer inhibitors (INSTIs).
Recent infection
Recent infection was defined according to Croxford et al. (2022)15, who updated the 2011 consensus definition16. Participants with a last negative test within 12 months of diagnosis or clinical evidence of acute infection were classified as recent infection. For MSM participants who did not meet these criteria, classification as recent or late diagnosis was not possible due to the unavailability of CD4 count data.
Transmission cluster analysis
Only HIV-1 subtype B pol sequences (n = 39) were used to identify TC. Control sequences (n = 56267) were extracted from the Los Alamos database (https://www.hiv.lanl.gov/content/sequence/HIV/mainpage.html). All subtype B sequences available from Europe (n = 25304), Africa (n = 248) and Latin America (n = 30715) were included. Three subtype C sequences were used as an outgroup. Using VIRULIGN17, the dataset was aligned against the global background dataset. Sequences with ≤ 1050 nucleotides and ≤ 90% nucleotide calls were excluded. For phylogenetic reconstruction, codon associated with drug resistance were removed18. Duplicates were removed with the Seqkit and Los Alamos tools. The final polifasta file included 50,969 sequences. Maximum likelihood phylogenies were constructed using FastTree19 with the generalised time-reversible model. Statistical support of clades was assessed using the Shimodaira-Hasegawa-like test (SH-test). Putative TC were identified using ClusterPicker20 v1.2.3 and defined as clades with branch support ≥ 90% and iterative genetic distance thresholds (≤ 1.5%, ≤ 2.5%, ≤ 3.5%, ≤ 4.5%, ≤ 5.5% and ≤ 6.5%)21,22.
Transmission clusters inferred from HIV-1 sequences are used as proxies for epidemiological linkage, and their interpretation depends on the genetic distance threshold used. A sensitivity analysis across different thresholds was therefore conducted to evaluate the robustness of the clustering patterns and results. The analysis of consistency across thresholds is used to assess wether the the findings reflect the transmission dynamics rather than an artefact of a single clustering cut-off23.
Cluster composition
TCs were characterised according to the proportional representation of migrant and non-migrant MSM within each cluster. Clusters composed entirely (100%) of migrant or non-migrant MSM were classified as exclusively involving that group. In mixed TC, the group representing ≥ 66.6% of individuals was considered the predominant group within the cluster. When no group reached this threshold (< 66.6%), the cluster was classified as having no predominant group. Additionally, clusters containing ≥ 66% control sequences from other countries were classified as clusters with predominant international representation, consistent with previous methodological approaches10.
No assumptions regarding transmission directionality were inferred from cluster composition.
Statistical analysis
We estimated medians and proportions for continuous and qualitative variables, respectively, with 95% confidence intervals for proportions and interquartile ranges for medians. To compare non-migrant and migrant MSM characteristics and TC composition, we used the Wilcoxon rank sum test, Fisher’s exact test and Pearson’s Chi-squared test.
The alpha level was 5%. Analyses were performed in R(v4.3.1) and plots generated in Python (v3.11).
Results
Sociodemographic characteristics
Overall, 30% (95% CI [19%, 43%]) of MSM were non-migrant and 70% (95% CI [57%, 81%]) were migrant, of which 60% (95% CI [47%, 72%]) from Brazil and 10% (95% CI [4.1%, 21%]) from other origins. The median age at diagnosis was 33 (IQR: 27–37), with the majority of MSM in the 25–34 years old (48.3%, 95% CI [35%, 61%]) and 35–44 years old (35%) [23%, 48%] intervals. Most migrants (57.1%, 95% CI [41%, 72%]) were diagnosed between 25 and 34 years, compared to non-migrants (27.8%, 95% CI [11%, 54%]). Non-migrants showed a more distributed age, with more diagnoses at older ages, with 16.7% (95% CI [4.4%, 42%]) diagnosed between 45 and 64 years, compared to migrants (2.4%, 95% CI [0.12%, 14%])(Table 1).
Sexual behavioural characteristics
Most MSM (93.3%, 95% CI [83%, 98%]) had sex only with men, while 6.7% (95% CI [2.2%, 17%]) had sex with men and women. A high proportion had unprotected anal sex (97%, 95% CI [87%, 99%]). None of the sexual behaviours differed significantly between non-migrants and migrants (Table 2).
Behavioural towards HIV testing and prophylaxis
One-third either tested for HIV more than once per year (31.7%, 95% CI [21%, 45%]), once per year (31.7%, 95% CI [21%, 45%]), or less than once per year (31.7%, 95% CI [21%, 45%]), although 5% (95% CI [1.3%, 15%]) had never been tested at the time of diagnosis. Regarding the last negative HIV test, 52% (95% CI [39%, 65%]) of MSM reported it was within the past year and 48% (95% CI [35%, 61%]) more than a year ago. For pre-exposure prophylaxis (PrEP), 13% (95% CI [6.3%, 25%]) reported having used it at least once in the past. None of the behaviours towards testing and prophylaxis were significantly different between non-migrants and migrants (Table 3).
Clinical and viral genomic data
Overall, 53% (95% CI [40%, 66%]) reported STI history, 39% (95% CI [22%, 58%]) in the previous 12 months and 61% (95% CI [42%, 78%]) more than 12 months ago. The most prevalent STI was syphilis (72%, 95% CI [53%, 86%]), followed by gonorrhea (41%, 95% CI [24%, 59%]), chlamydia (16%, 95% CI [5.9%, 34%]). No significant difference was found between non-migrants and migrants (Table 4).
HIV-1 subtype B was the most prevalent (65%, 95% CI [52%, 77%]), in 76.2% of migrants (95% CI [60%, 87%]) and 38.9% (95% CI [18%, 64%]) of non-migrants. The proportion of HIV-1 subtype B in migrants was significantly higher than in non-migrants (Table 4).
Overall, 58% of MSM (95% CI [45%, 71%]) were classified with recent HIV-1 infection, with no significant difference between non-migrants and migrants (Table 4).
SDRMs were present in 15% of MSM (95% CI [7.5%, 27%]), similar among non-migrants (16.7%, 95% CI [4.4%, 42%]) and migrants (14.3%, 95% CI [5.9%, 29%]). The most prevalent SDRM was K103N (10%, 95% CI [4.1%, 21%]). NNRTI resistance was more prevalent (12%, 95% CI [5.2%, 23%]), with comparable proportions in both groups. No resistance to INSTI was detected(Table 4).
Transmission clusters analysis
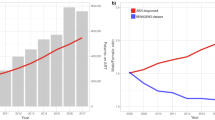
The proportion of MSM included in TC (HIV-1 subtype B) increased with genetic distance thresholds: 10.3% (95% CI [3.3%, 25%]) at 1.5%, 28.2% (95% CI [16%, 45%]) at 2.5%, 35.9% (95% CI [22%, 53%]) at 3.5%, 53.8% (95% CI [37%, 70%]) at 4.5%, 61.5% (95% CI [45%, 76%]) at 5.5%, and 66.7% (95% CI [50%, 80%]) at 6.5%. The proportion of non-migrant and migrant MSM included in TC did not differ significantly at any threshold. However, the composition of TC changed with increasing genetic distance: the proportion of migrants rose steadily from 9.4% (95% CI [2.5%, 26%]) at 1.5% to 72% (95% CI [53%, 86%]) at 6.5%. In contrast, the proportion of non-migrants remained relatively stable, ranging from 14% (95% CI [0.75%, 58%]) at 1.5% to 43% (95% CI [12%, 80%]) at distances of 3.5%, but remaining constant (43%, 95% CI [12%, 80%]) at 4.5%, 5.5% and 6.5% thresholds (Fig. 1).

– Transmission clusters analysis (Subtype B) – MSM inside TC.
Cluster composition (100% Migrants or 100% Non-migrants)
Across all thresholds, part of our sample migrant MSM were in migrant-only TC: 67% (95% CI [13%–98%]) at 1.5%, 44% (95% CI [15%, 77%]) at 2.5%, 36% (95% CI [12%, 68%]) at 3.5%, 22% (95% CI [7.4%, 48%]) at 4.5%, 9.5% (95% CI [1.7%, 32%]) at 5.5%, and 0% (95% CI [0%, 18%]) at 6.5%.
Non-migrant-only TC were identified only at 3.5%, 4.5% and 5.5% genetic distances and included 33% (95% CI [1.8%, 87%]) MSM for all 3 thresholds (Fig. 2).

Proportion of MSM in 100% migrant or non-migrant clusters by genetic distance.
Cluster composition across genetic distance thresholds
Among non-migrant MSM, cluster composition varied across genetic distance (GD) thresholds. At 1.5% GD, clusters involving non-migrants did not meet criteria for a predominant group. At 2.5% GD, 50% (95% CI [9.5%, 91%]) of non-migrant MSM were observed in clusters predominantly composed of migrants. At 3.5% and 4.5% GD, equal proportions (33%, 95% CI [1.8%, 87%]) of non-migrant MSM were identified in clusters predominantly composed of non-migrants and in clusters predominantly composed of migrants. At 5.5% and 6.5% GD, non-migrant MSM were distributed in equal proportions across clusters predominantly composed of non-migrants, predominantly composed of migrants, and clusters with predominant international representation (33%, 95% CI [1.8%, 87%]).
Among migrant MSM, individuals were consistently observed in clusters predominantly composed of migrants across all GD thresholds, and less frequently in clusters with predominant international representation. Migrants identified in clusters predominantly composed of non-migrants were less frequent, with no such clusters observed between 1.5% and 4.5% GD. At 5.5% and 6.5% GD, 9.5% (95% CI [1.7%, 32%]) and 8.7% (95% CI [1.5%, 30%]) of migrant MSM, respectively, were identified in clusters predominantly composed of non-migrants (Fig. 3).

Heatmap of assortative mixing by origin across genetic distance thresholds.
TCs were characterised according to the proportional representation of migrant and non-migrant MSM within each cluster. Clusters composed entirely (100%) of migrant or non-migrant MSM were classified as exclusively involving that group. In mixed TC, the group representing ≥ 66.6% of individuals was considered the predominant group within the cluster. When no group reached this threshold (< 66.6%), the cluster was classified as having no predominant group. Additionally, clusters containing ≥ 66% control sequences from other countries were classified as clusters with predominant international representation, consistent with previous methodological approaches10.
Transmitted drug resistance in TC (Subtype B)
There were 6 MSM (15%, 95% CI [6.4%, 31%]) with SDRMs included in the TC analysis (Subtype B; n = 39): 1 (14%, 95% CI [0.75%, 58%]) non-migrant (n = 7) and 5 (16%, 95% CI [5.9%, 34%]) migrants (n = 32). From those 6 MSM, 2 MSM (33%, 95% CI [6.0%, 76%]) at 1.5 and 2.5% GD thresholds and 3 MSM (50%, 95% CI [19%, 81%]) at 3.5% to 6.5% GD thresholds, clustered in TC. All MSM with SDRM belonging to TC were migrants at all GD thresholds (Table 5). The one non-migrant MSM with SDRM did not cluster. With SDRM, 2 TC were identified at 1.5% and 2.5% GD, and 3 TC at 3.5% to 6.5% (Table 5). From 1.5% to 5.5% GD, there was 1 TC with SDRM with 2 tips, including the same 2 MSM (from our sample). At 6.5%, these 2 MSM were included in a TC with 9 tips. From 3.5% to 5.5%, there was a second TC with SDRM with 4 tips, including the 1 MSM (from our sample). At 6.5%, this 1 MSM was included in a TC with 20 tips (Table 5).
Discussion
This study analysed sociodemographic, sexual behavioural, testing, STI, clinical and viral genomic characteristics of MSM diagnosed with HIV-1 in Portugal (2023–2024), in a Lisbon community centre, comparing non-migrant and migrant MSM, and analysing TC identified at six genetic distance thresholds.
Among the 60 newly diagnosed MSM, 70% were migrants, of whom 60% were from Latin America and 10% from other regions, highlighting the relevance of the migrant MSM in current HIV-1 transmission dynamics. The latest national report shows foreign-born individuals now constitute the majority of new HIV-1 diagnoses in Portugal with 53.1% overall, and 54.7% migrants among MSM in 20233. Denmark’s HIV surveillance report (2023) shows a similar migrant proportion (64%) among MSM24. In contrast, in the MSM population in Portugal, a 2014–2019 Portuguese study reported only 28% migrants among new MSM diagnoses25. Although the 70% in this 2023–2024 community sample may reflect a specific network, exceeding national averages, these results suggest a greater role of migrants in MSM HIV diagnoses. To address this trend, Portugal should consider policies to enhance early and accessible HIV testing and PrEP for migrants.
The overall median age at diagnosis was 33 (IQR (27, 37)), consistent with other studies in Portugal11 and other European countries26. Although the median age between non-migrants and migrants was comparable, significantly more migrants (57.1%) were diagnosed at younger ages (25–34), while non-migrants had a more dispersed age distribution. Migration is often youth-driven, with people most likely migrating for work, study, or refuge to be young adults27. This naturally leads to a younger age distribution among migrants living in high-income countries, which is reflected in HIV diagnoses.
Our findings reveal extremely high-risk sexual behaviours among MSM, consistent with patterns reported in other studies. The near-universal proportion of unprotected anal sex (97%) is higher than typically observed in MSM surveys, but still aligns with evidence that a majority of MSM engage in condomless sex. A German clinic-based study found 73.6% of MSM had recent sex without condoms28, and a European survey of high-risk MSM reported 84% had condomless sex with multiple partners29. However, interpretation of condomless sex in contemporary prevention contexts requires nuance. HIV transmission risk is substantially modified by other strategies, including PrEP and antiretroviral therapy with sustained viral suppression (U = U). Therefore, condomless intercourse in our sample may not uniformly represent uncontrolled HIV transmission risk, although it remains epidemiologically relevant. Importantly, condomless sex continues to confer significant risk for STIs, regardless of PrEP use or viral suppression. In fact, over half (53%) of the MSM reported a history of STI, most commonly syphilis and gonorrhoea, in line with the heavy STI burden documented among MSM in other studies28,30. This highlights that even in the era of biomedical HIV prevention, STI transmission remains a major public health concern. Our study emphasises the need for STI control policies within MSM-focused programs that ensure comprehensive STI screening and treatment are integrated and offered alongside HIV services31.
Additionally, our finding of low pre-exposure prophylaxis (PrEP) uptake (13%) reflects patterns of inadequate global PrEP coverage32. Around 2020, only about 18.3% of MSM in Brazil and 21.5% in Portugal reported using PrEP (28). In countries with more mature PrEP programs, uptake has increased, yet many high-risk individuals remain unreached (in the Netherlands, only one-third of at-risk MSM were on PrEP (2021))33. Public health agencies should identify barriers to PrEP uptake among eligible MSM and address them by reducing cost, simplifying access, improving multilingual information, training providers to proactively offer PrEP without judgment, integrating PrEP into routine care, and removing structural and administrative barriers to acessing national health system32,34.
Guidelines recommend annual screening, and every 3–6 months for those at ongoing risk35. Our data show suboptimal HIV testing frequency, despite confidential, broad access in Portugal through self-testing, healthcare services, NGOs, and pharmacies36. These results align with other studies among MSM in Portugal37 and across Europe38,39,40. That many MSM test infrequently despite widespread testing access suggests other underlying factors. HIV testing among MSM is affected by intertwined psychosocial barriers, including antecipated stigma, fear of judgment, low-risk perception, negative treatment attitudes, and avoidance of distressing information41,42.
Migrant MSM were predominantly infected with subtype B (76.2%), significantly different from non-migrant MSM with 38.9% subtype B and 61.1% non-B (including A1, F1, G, C and CRFs). In Europe, Non-B and/or CRF clades were introduced mostly through waves of migration from regions in which they are prevalent43. The Brazilian HIV epidemic is largely subtype B, reaching 90% in some regions. By contrast, Portuguese MSM appear to have acquired viruses from a wide mix of sources. Consistently, recent Portuguese data show ~ 58% subtype B among MSM overall, with the remainder including substantial A1, F1, C and G subtypes11.
Across all distance thresholds used to identify TC among HIV-1 subtype B sequences, migrants in TCs were mostly related to other migrants, consistent with assortative mixing by country of birth (Figs. 2 and 3). Non-migrants were distributed across clusters predominantly composed of non-migrants, migrants, or sequences from other countries, indicating more heterogeneous mixing patterns. Another Portuguese study found 50% of clusters composed only of non-migrant MSM, whereas 16% included exclusively migrants11. Thus, our results may be specific to the MSM attending this community centre. Our findings of homogeneous migrant TC suggest strong assortative mixing by country of birth. The segregation of migrant networks may stem from sociocultural factors, as migrants often socialise within co-ethnic circles for support and due to language or cultural familiarity44. The dominance of migrant-to-migrant mixing among MSM highlights a need for targeted HIV prevention. Public health programs should engage migrant MSM through community‐based organisations and peer networks, using culturally and linguistically appropriate messaging34,45,46. Ensuring equitable access to HIV services regardless of immigration status, is essential7. National HIV/AIDS strategies should explicitly identify migrants as a priority population, with tailored objectives for increasing testing and reducing late diagnosis in this group6.
The prevalence of TDR mutations was 15%, with no significant difference between non-migrant (16.7%) and migrant (14.3%) MSM. The overall prevalence is considerably higher than that found in a previous MSM study in Portugal (8.2%)11, France (10.8%)47 and the UK (7.5%)48. In Brazil, higher prevalences have been reported, between 12%49 and 16.3%50. The high TDR prevalence found may be explained by the high proportion of MSM from Brazil in our sample and the high proportion of migrant MSM mixing with other migrants in Portugal or outside Portugal (Fig. 3). Importantly, like in Portugal, European studies generally report no significant difference in TDR rates between non-migrant and migrant patients11,51.
The NNRTI mutation K103N dominated (10%). In contrast, no INSTI-resistance mutations were detected. K103N is a non-polymorphic mutation conferring high-level resistance to NVP and EFV, and it is the most common TDR52. Consistently, NNRTI resistance (e.g. K103N) remains the predominant form of transmitted resistance in Brazil50. Although NNRTI-associated TDR, especially K103N, is still commonly observed in Europe and Brazil, its clinical impact has become less important as both regions now use INSTI-based first-line regimens (e.g. dolutegravir with two NRTIs)53,54. Transmitted INSTI resistance remains very low in Europe. A 2018–2021 survey found only 0.3% of new cases with INSTI SDRMs, and virtually none with resistance to second-generation INSTI54. As in Europe, transmitted INSTI resistance is rare in Brazil54. INSTI resistance remains minimal because INSTI (especially second-generation agents like dolutegravir and bictegravir) have a high genetic barrier to resistance, and were only recently introduced, limiting the time for resistant strains to emerge55,56.
Although TDR prevalence between non-migrant and migrant MSM was not significantly different, all clustered SDRM cases were among migrants (Table 6), suggesting active resistance transmission within migrant networks. This signals a need to target prevention in those networks and continue to trace how resistant strains move through populations and across borders using phylogenetic analysis approach.
This study has some limitations. There is a potential selection bias associated with a single community-based testing site. MSM testing in this centre may over-represent migrants and younger MSM. Therefore, data may not represent MSM diagnosed in hospitals or other settings. The small sample size may impact statistical power and generalisability. Most migrants were from Portuguese-speaking countries, limiting applicability to origins with linguistic differences. Self-reported behavioural data may include memory and social desirability biases. Finally, different genetic distance thresholds can impact cluster identification and transmission pattern interpretation, although multiple thresholds were tested for robustness.
Conclusion
Findings from this single community-based centre suggest that recent HIV-1 epidemiology among MSM has shifted, with migrants representing a growing proportion of new diagnoses, mainly within sexual networks with other migrants. To address this trend, strategies should enhance early and accessible PrEP, STI, and HIV testing for migrant MSM. Ending the HIV-1 epidemic requires closing testing gaps, increasing prevention, and defining programmes to reach migrant communities.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
UNAIDS. global AIDS report — The Urgency of Now: AIDS at a Crossroads [Internet]. Geneve https://www.unaids.org/sites/default/files/media_asset/2024-unaids-global-aids-update_en.pdf (2024).
WHO. WHO Regional Office for Europe. European Centre for Disease Prevention and Control. HIV/AIDS surveillance in Europe 2024–2023 data. Copenhagen; (2024).
DGS; INSA. Infeção por VIH em Portugal 2024 (Lisboa, 2024).
Eurostat. Population on 1 January by age group, sex and country of birth (Data set code: migr_pop3ctb) https://ec.europa.eu/eurostat/databrowser/product/page/migr_pop3ctb (2025).
Pachankis, J. E. et al. Anti-LGBT and Anti-immigrant Structural Stigma: An Intersectional Analysis of Sexual Minority Men’s HIV Risk When Migrating to or Within Europe. JAIDS J Acquir Immune Defic Syndr [Internet]. 76 356–366 https://api.semanticscholar.org/CorpusID:3423606. (2017).
ECDC. HIV and migrants in the EU/EEA. Monitoring implementation of the Dublin Declaration on partnership to fight HIV/AIDS in Europe and Central Asia: 2024 progress report (European Centre for Disease Prevention and Control, 2024).
Nöstlinger, C. et al. HIV among migrants in precarious circumstances in the EU and European Economic Area. lancet HIV. 9 (6), e428–e437 (2022).
Oster, A. M. et al. Identifying Clusters of Recent and Rapid HIV Transmission Through Analysis of Molecular Surveillance Data. J. Acquir. Immune Defic. Syndr. 79 (5), 543–550 (2018).
Miller, R. L. et al. Phylogenetic prioritization of HIV-1 transmission clusters with viral lineage-level diversification rates. Evol. Med. public. Heal. 10 (1), 305–315 (2022).
Pimentel, V. F. et al. Differential patterns of postmigration HIV-1 infection acquisition among Portuguese immigrants of different geographical origins. AIDS 36 (7), 997–1005 (2022).
Abrantes, R. et al. Determinants of HIV-1 transmission clusters and transmitted drug resistance in men who have sex with men: A multicenter study in Portugal (2014–2019). Int. J. Infect. Dis. https://www.sciencedirect.com/science/article/pii/S1201971225001110 (2025).
GAT - Grupo de Ativistas em Tratamentos. GAT CheckpointLx [Internet] https://www.checkpointlx.com/ (2022).
Pineda-Peña, A. C. et al. Automated subtyping of HIV-1 genetic sequences for clinical and surveillance purposes: Performance evaluation of the new REGA version 3 and seven other tools. Infect. Genet. Evol. 19 (100), 337–348 (2013).
Delport, W., Poon, A. F. Y., Frost, S. D. W. & Kosakovsky Pond, S. L. Datamonkey 2010: a suite of phylogenetic analysis tools for evolutionary biology. Bioinformatics 26 (19), 2455–2457 (2010).
Croxford, S. et al. Late diagnosis of HIV: An updated consensus definition. HIV Med. 23 (11), 1202–1208 (2022).
Antinori, A. et al. Late presentation of HIV infection: a consensus definition. HIV Med. 12 (1), 61–64 (2011).
Libin, P. J. K., Deforche, K., Abecasis, A. B. & Theys, K. VIRULIGN: Fast codon-correct alignment and annotation of viral genomes. Bioinformatics 35 (10), 1763–1765 (2019).
Lemey, P. et al. Molecular footprint of drug-selective pressure in a human immunodeficiency virus transmission chain. J. Virol. 79 (18), 11981–11989 (2005).
Price, M. N., Dehal, P. S. & Arkin, A. P. FastTree: computing large minimum evolution trees with profiles instead of a distance matrix. Mol. Biol. Evol. 26 (7), 1641–1650 (2009).
Ragonnet-Cronin, M. et al. Automated analysis of phylogenetic clusters. BMC Bioinform. 14 (1), 317 (2013).
Wertheim, J. O. et al. Social and Genetic Networks of HIV-1 Transmission in New York City. PLoS Pathog. 13 (1), 1–19 (2017).
Novitsky, V. et al. Empirical comparison of analytical approaches for identifying molecular HIV-1 clusters. Sci. Rep. 10 (1), 1–11 (2020).
Kosakovsky Pond, S. L., Weaver, S., Leigh Brown, A. J. & Wertheim, J. O. HIV-TRACE (TRAnsmission Cluster Engine): a Tool for Large Scale Molecular Epidemiology of HIV-1 and Other Rapidly Evolving Pathogens. Mol. Biol. Evol.https://doi.org/10.1093/molbev/msy016 (2018).
Statens Serum Institut (Denmark). HIV 2023 Report https://en.ssi.dk/surveillance-and-preparedness/surveillance-in-denmark/annual-reports-on-disease-incidence/h/hiv-2023 (2024).
Abrantes, R. et al. Determinants of HIV late presentation among men who have sex with men in Portugal (2014–2019): who’s being left behind? Front. public. Heal. 12, 1336845 (2024).
ECDC/WHO. HIV/AIDS surveillance in Europe 2024–2023 data (WHO Regional Office for Europe, 2024).
Milasi, S. What Drives Youth’s Intention to Migrate Abroad? Evidence from International Survey Data. IZA J. Dev. Migr. https://api.semanticscholar.org/CorpusID:220634179 (2020).
Jansen, K. et al. STI in times of PrEP: high prevalence of chlamydia, gonorrhea, and mycoplasma at different anatomic sites in men who have sex with men in Germany. BMC Infect. Dis. https://doi.org/10.1186/s12879-020-4831-4 (2020).
Iniesta, C. et al. Awareness, knowledge, use, willingness to use and need of Pre-Exposure Prophylaxis (PrEP) during World Gay Pride 2017. PLoS One. 13 (10), 1–10 (2018).
Kojima, N. & Klausner, J. D. An Update on the Global Epidemiology of Syphilis. Curr. Epidemiol. Rep. 5 (1), 24–38 (2018).
Wilson, J. S18.2 Bridging the gap {\textendash} best practice global examples of integration of HIV and STI services. Sex Trans. Infect. https://sti.bmj.com/content/95/Suppl_1/A29.2 (2019).
Bavinton, B. R. & Grulich, A. E. HIV pre-exposure prophylaxis: scaling up for impact now and in the future. Lancet Public. Heal. 6 (7), e528–e533 (2021).
Evers, Y. J., Goense, C. J. D., Hoebe, C. J. P. A. & Dukers-Muijrers, N. H. T. M. Newly diagnosed HIV and use of HIV-PrEP among non-western born MSM attending STI clinics in the Netherlands: a large retrospective cohort study. Front. Public. Heal. 11 (June), 1–8 (2023).
Tieosapjaroen, W. et al. Improving access to oral pre-exposure prophylaxis for HIV among international migrant populations. Lancet Public Heal. https://api.semanticscholar.org/CorpusID:259375098 (2023).
World Health Organization. Consolidated guidelines on differentiated HIV testing services [Internet]. Geneva: World Health Organization. https://iris.who.int/bitstream/handle/10665/378162/9789240096394-eng.pdf?sequence=1 (2024).
DGS; INSA. Infeção por VIH em Portugal – 2022 (Lisboa, 2022).
Abrantes, R. et al. Determinants of HIV late presentation among men who have sex with men in Portugal (2014–2019): who’s being left behind? Front. Public. Heal ;12. (2024).
European Centre for Disease Prevention and Control. EMIS-2017: The European men-who-have-sex-with-men internet survey: Key findings from 50 countries. https://www.ecdc.europa.eu/en/publications-data/emis-2017-european-men-who-have-sex-men-internet-survey (2019).
Leenen, J. et al. HIV testing behaviour and associated factors in men who have sex with men by level of urbanisation: a cross-sectional study in the Netherlands. BMJ Open. 12 (1), e049175 (2022).
Moseng, B. U. & Bjørnshagen, V. Are there any differences between different testing sites? A cross-sectional study of a Norwegian low-threshold HIV testing service for men who have sex with men. BMJ Open. 7 (10), 1–7 (2017).
Kobrak, P. et al. Motivations and Barriers to Routine HIV Testing Among Men Who Have Sex with Men in New York City. AIDS Behav. https://doi.org/10.1007/s10461-022-03679-5 (2022).
Dibble, K. E. et al. Associations between HIV testing and multilevel stigmas among gay men and other men who have sex with men in nine urban centers across the United States. BMC Health Serv. Res. 22 (1), 1179 (2022).
Beloukas, A. et al. Molecular epidemiology of HIV-1 infection in Europe: An overview. Infect. Genet. Evol. https://www.sciencedirect.com/science/article/pii/S156713481630257X. (2016).
Stella, F. & Gawlewicz, A. Social networks, language and identity negotiations among queer migrants in Scotland. J. Ethn. Migr. Stud. 47(11) 2537–55. https://doi.org/10.1080/1369183X.2020.1863203 (2021).
Lee, J. J. et al. Culturally Tailored Social Media Content to Reach Latinx Immigrant Sexual Minority Men for HIV Prevention: Web-Based Feasibility Study. JMIR Form Res. https://api.semanticscholar.org/CorpusID:246996410 (2022).
Sánchez, J., Rosa, M. R. D., La, Serna, C. A., Project & Salud Efficacy of a community-based HIV prevention intervention for Hispanic migrant workers in south Florida. AIDS Educ. Prev. 25 5 363–75. https://api.semanticscholar.org/CorpusID:38023455 (2013).
Visseaux, B. et al. Surveillance of HIV-1 primary infections in France from 2014 to 2016: Toward stable resistance, but higher diversity, clustering and virulence? J. Antimicrob. Chemother. 75 (1), 183–193 (2020).
Tostevin, A. et al. Recent trends and patterns in HIV-1 transmitted drug resistance in the United Kingdom. HIV Med. 18 (3), 204–213 (2017).
Tanaka, T. S. O. et al. HIV-1 Molecular Epidemiology, Transmission Clusters and Transmitted Drug Resistance Mutations in Central Brazil. Front Microbiol. https://www.frontiersin.org/journals/microbiology/articles/https://doi.org/10.3389/fmicb.2019.00020 (2019).
Ferreira, A. C. G. et al. Transmitted drug resistance in patients with acute/recent HIV infection in Brazil. Brz. J. Infect. Dis. 21(4) 396–401. https://bjid.org.br/en-transmitted-drug-resistance-in-patients-articulo-S1413867016303300 (2017).
Pineda-Peña, A. C. et al. Trends and Predictors of Transmitted Drug Resistance (TDR) and Clusters with TDR in a Local Belgian HIV-1 Epidemic. PLoS One [Internet]. https://doi.org/10.1371/journal.pone.0101738 (2014).
HIV Drug Resistance Database. - Stanford University [Internet]. https://hivdb.stanford.edu/dr-summary/comments/NNRTI/ (2025).
Diaz, R. S. et al. Dolutegravir-associated resistance mutations after first-line treatment failure in Brazil. BMC Infect. Dis. 23 (1), 347 (2023).
de Salazar, A. et al. Transmitted Drug Resistance to Integrase-Based First-Line Human Immunodeficiency Virus Antiretroviral Regimens in Mediterranean Europe. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciac972 (2023).
Chu, C. et al. Prevalence of Emergent Dolutegravir Resistance Mutations in People Living with HIV: A Rapid Scoping Review. Viruses [Internet].https://www.mdpi.com/1999-4915/16/3/399 (2024).
Zhao, A. V. et al. A clinical review of HIV integrase strand transfer inhibitors (INSTIs) for the prevention and treatment of HIV-1 infection. Retrovirology [Internet]. https://doi.org/10.1186/s12977-022-00608-1 (2022).
Acknowledgements
We would like to thank the GAT-Checkpoint team for your support during data collection.
Funding
This work is funded by national funds through FCT – Fundação para a Ciência e a Tecnologia, I.P., under the R&D unit Global Health and Tropical Medicine (UID/04413/2025) and the Associated Laboratory in Translation and Innovation Towards Global Health REAL (LA/P/0117/2020).
Author information
Authors and Affiliations
Contributions
RA, VP, MROM, MP, and AA: conceptualization, methodology, writing original draft, reviewing and editing. RA, VP, CS: formal analysis and reviewing. AA: funding acquisition, project administration, and supervision. AM, LP, LM: resources, data collection, reviewing and approval of the publication contents. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Abrantes, R., Pimentel, V., Sebastião, C.S. et al. Men who have sex with men newly diagnosed with HIV-1 in Portugal (2023–2024): a comparative analysis of transmission clusters between migrants and non-migrants. Sci Rep 16, 10911 (2026). https://doi.org/10.1038/s41598-026-45367-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-45367-7
