
Abstract
Burnout syndrome received increased scientific attention in the wake of the Coronavirus-19 (COVID-19) pandemic. Globally, burnout prevalence rates increased, but there is limited published data on this phenomenon in the English-speaking Caribbean. The objective of this study was to determine the prevalence of the burnout syndrome among doctors and nurses (termed healthcare-workers) in a hospital in Tobago during the COVID-19 pandemic. The study also sought to identify potential associated factors, and to assess coping strategies. This was a cross-sectional study of 102 doctors and nurses selected using convenience sampling. The Maslach Burnout Inventory, Pandemic Experiences and Perceptions Survey (PEPS) and the Brief Coping Orientation to Problems Experienced (COPE) screening tools were administered through a self-administered questionnaire hosted on the Google Forms online platform. Binomial logistic regression was applied to evaluate potential predictive variables of burnout in healthcare workers. The overall prevalence of burnout during the COVID-19 pandemic was 33.3%, with approximately 10% reporting severe levels of burnout. Lifestyle factors such as use of sleeping pills (p = 0.002) and time spent doing relaxing activities (p = 0.015) were found to have a statistically significant association with burnout. A healthcare worker using sleeping pills was demonstrated to have increased odds of developing burnout (OR: 12.667; 95% CI: 2.359, 68.015) as compared to persons who did not use this substance. Acceptance and religion were the most utilized coping strategies. Behavioural disengagement was demonstrated to have a significant relationship with burnout (p < 0.001). Burnout syndrome was a significant concern during the COVID-19 pandemic among healthcare-workers serving under the Tobago Regional Health Authority. Both organizational and individual interventions are necessary to reduce negative outcomes to the affected staff and the patients they serve.
Similar content being viewed by others
Introduction
The burnout syndrome phenomenon, though extensively studied over the last four decades, received increased scientific attention during the stressful chronicity of the Coronavirus-19 (COVID-19) pandemic. Burnout is classified as a syndrome resulting from prolonged emotional, situational and interpersonal stressors in one’s occupation1, in a context where “chronic workplace stress…. is not effectively handled”2. Burnout syndrome spans three core domains which are Emotional Exhaustion (EE), Depersonalisation (DP) and diminished Personal Accomplishment (PA). EE refers to the experience of fatigue or energy depletion, DP describes feelings of cynicism or detachment towards one’s job, and diminished PA relates to reduced professional effectiveness2.
Social psychologist Christina Maslach and colleagues conducted extensive research detailing the burnout syndrome which led to the creation of its first quantitative assessment tool, The Maslach Burnout Inventory (MBI)3. The MBI possesses good reliability and validity, and remains widely used across varying populations4. A systematic review of thirty studies of burnout using the MBI Inventory within the COVID-19 pandemic found an overall burnout prevalence of 52% among healthcare-workers (HCWs) [95% CI 40–63%], with the highest levels recorded among physicians and nurses5. This rate exceeded figures found in studies over the past two decades (32% and 34% respectively). A systematic review and meta-analysis of sixteen studies exploring burnout in nurses during the COVID-19 pandemic found an overall prevalence of 34.1% (95% CI: 22.5–46.6%)6. Notably, there was a demonstrable six-year period of decline in reported burnout among American doctors before the start of the pandemic in December, 2020, with a sharp increase noted by the end of 2021, with figures of 62.0% in 2021, relative to 38.2% in 20207. Nurses themselves also felt the strain. In 2019, only 15.6% of American nurses reported feelings of being burnt out, which rose to 62% at the onset of the pandemic8.
Past studies have shown that burnout is a significant prognosticator of poor health outcomes in employees9. Increased turnover of staff coupled with the presence of a debilitated existing workforce may lead to sub-optimal patient care. This may contribute to increased patient morbidity and mortality, and consequent financial burden caused by high litigation costs and staff turnover expenses for affected healthcare organizations9. Unfortunately, there has been little published research surrounding burnout syndrome in healthcare-workers (HCWs) and their coping strategies in the English-speaking Caribbean during the COVID-19 pandemic.
With this in mind, the primary aim of this research was to establish the degree of burnout and its associated factors in HCWs during the COVID-19 pandemic under the institution responsible for healthcare in the island of Tobago, the Tobago Regional Health Authority (TRHA). The secondary aim was to explore individual protective coping techniques that may have mitigated the experience of burnout and its adverse consequences in this population.
Methods
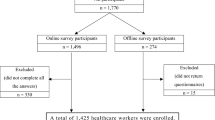
This was a cross-sectional study of doctors and nurses working in Scarborough General Hospital under the Tobago Regional Health Authority (TRHA) in Tobago. Convenience sampling was used for a three-month period from the 20th of December 2022 to the 20th of March, 2023.
Written informed consent was obtained from participants through a electronic consent form at the beginning of the survey that was hosted on the Google Forms online platform. Participants could not access the survey if they did not give consent (through clicking the ‘No’ button) at the end of the consent form.
Ethical approval was granted by the Campus Research Ethics Committee of the University of the West Indies on the 17th August, 2022. (Ethical Approval ID CREC-SA1616/06/2022). Ethical approval was also granted by the Research Ethics Committee (REC) of the Tobago House of Assembly (THA) and the Tobago Regional Health Authority (TRHA) on (Ethical Approval ID THAREC: 022/10/2022). All methods were conducted in full accordance with relevant guidelines and regulations.
The Maslach Burnout Inventory-Human Services Survey (MBI-HSS), Pandemic Experiences and Perceptions Survey (PEPS) and the Brief Coping Orientation to Problems Experienced (COPE) were the validated measurement tools implemented through a self-administered questionnaire hosted on the Google Forms online platform. The MBI-HSS comprises of twenty-two (22) items evaluating the respondents’ attitudes to work that coorelate to the three domains of burnout Emotional Exhaustion (EE), Depersonalisation (DP) and Personal Accomplishment (PA)3. Each item is scored from a Likert Scale ranging from never (0) to every day (6). Descriptive statistics were used to classify the marks of the participants in all three burnout sub-elements. These scores coorelated to varying degrees of burnout severity, which were evaluated as low, moderate, and high based on already established scores. A low degree of EE is a score of < 17, a moderate level of EE is a score of 18–29, and severe level of EE a score more than 30. A low degree of DP is a score < 5, a moderate degree of DP 6–11, and a high degree of DP a score more than 12. A low degree of PA < 33, a moderate degree of PA 34–39 and a high degree of PA being a score > 40. High scores in the the EE and DP domains and low scores in the PA coorelate to burnout.
The PEPS is 35-item assessment tool developed by one of the authors of the MBI to identify employees’ unique experiences and perspectives while working during the COVID-19 pandemic in five key areas, namely Work Disruption, Resources, Risk Perception, Impact on Worklife Areas and Perceptions of Leadership, with open-text items identifying potential support mechanisms and sources of hope for employees10. The Brief COPE scale is the 28-item abbreviated version of the original form of the COPE questionnaire that measures respondents’ coping styles during stressful experiences11. Responses are rated on a four-point Likert scale, with scores in each domain calculated to assess for fourteen adaptive and maladaptive coping mechanisms.
Responses ranged from the statements like “I usually don’t do this at all’ to “I do this a lot”. The scores ranged from a minimum score of 1, to a maximum of 4, and scores were used to assess the popularity of the coping mechanism. An unanswered statement related was treated as absent. All data from the questionnaires were analysed with the Statistical Product and Service Solutions (SPSS) (IBM SPSS Statistics for Windows, Version 28.0, Armonk, NY).
Descriptive statistics were used to show the respondents’ attributes with regards to socio-demographics, employment information, lifestyle factors and coping techniques in terms of frequencies and percentages. Burnout point prevalence and severe burnout prevalence were stated as percentages. The Cronbach’s α coefficient was evaluated for the three dimensions of the MBI-HSS (MP), as well as the five PEPS tools and the fourteen coping strategies in the Brief COPE.
Pearson’s χ2 and Fisher’s exact tests were used to find univariate associations between categorical independent variables and the dependent variable ‘burnout’ (yes/no), as well as relationships between categorical independent variables and the individual burnout elements. Fisher’s exact test was used for expected frequencies in at least 20% of cells in cross-tabulations. These tests’ scores were used to select informative variables only to avoid dimensionality.
For the variables EE and DP, the ‘low’ and ‘moderate’ classifications were brought together to form a ‘low/moderate’ category against ‘high’. For the PA variable, ‘moderate’ and ‘high’ categories were merged into ‘moderate/high’ against ‘low’ outcome. This allowed binomial logistic regression to be used in calculating the strength of associations with odds ratios (OR) and 95% confidence intervals (CI) and identifying possible predictive factors for burnout, where the explanatory variables were the statistically significant variables from the univariate analyses.
Because of non-normally distributed data, coping techniques were described as medians and interquartile ranges (IQRs), while PEPS tool scores were presented as means and standard deviations. The relationship between burnout and popular coping mechanisms were assessed with the non-parametric Mann-Whitney U test.
Burnout and PEPS tool scores were assessed using independent samples test. Spearman’s rank correlation coefficient was used to correlations between PEPS tool scores and coping styles. Statistical significance was set at p < 0.05.
Results
Socio-demographics and occupational characteristics
There was a total of 102 participants, 49 nurses (48%) and 53 physicians (52%). The socio-demographic and occupational characteristics are presented in Table 1. Most participants were in the 31–40 age group (n = 52, 51%). Among the two occupations, 49% of nurses were in the 31–40 age group, while most physicians were also in this age group (n = 28, 52.8%). Most participants were female (n = 82, 80.4%), which was also observed in both professions.
There was a notable gender difference among professions, with 32.1% of physicians being male, as compared to 6.1% of nurses. Most persons were of African descent (n = 79, 77.5%). Among both occupations, the nurses (n = 43, 87.8%) and physicians (n = 36, 67.9%) were predominantly of African descent. Most participants were single (n = 55, 53.9%). Among the two occupations, most nurses (n = 27, 55.1%) were married, while most physicians (n = 37, 69.8%) were single. The largest proportion of participants did not have any children living with them (n = 47, 46.1%), with most physicians (n = 37, 69.8%) not having any children living with them. Most participants held an undergraduate degree (n = 52, 51%), which was seen in both occupations.
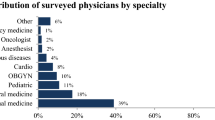
Overall, the largest proportion of participants worked in the Psychiatry department (n = 24, 23.5%). Among nurses, 30.6% worked in the Psychiatry department, while 17% of physicians worked in the Adult Medical Ward and Psychiatry department.Almost all the participants were employed full-time (n = 101, 99%). A total of 32.4% of participants have been working in health for less than five years. Among both occupations, 42.9% of nurses had 11–20 years in experience in healthcare, while 39.6% of physicians had 5–10 years of primary care experience. Some participants worked over 10 h each day at the RHA (n = 16, 15.7%).
The highest proportion of participants worked more than six night shifts (8pm–8am) each month (n = 35, 34.3%). Among nurses, 38.8% did not have any night shifts each month, while most physicians (n = 28, 52.8%) had more than six night shifts each month. Most participants (n = 81, 79.4%) worked in close contact with confirmed or suspected COVID-19 patients, which was observed in both occupations. Most participants (n = 53, 52%) also had training in managing patients with COVID-19. Most nurses (n = 28, 57.1%) did not have training in managing patients with COVID-19, while most physicians (n = 32, 60.4%) received such training.
Prevalence of burnout and associated socio-demographic, occupational and lifestyle factors
The three dimensions of burnout, were each scored separately and were then grouped into categories delineated as ‘low’, ‘moderate’, and ‘high’. The numbers of participants meeting these cut-offs - are shown in Table 2. The scale evinced good to excellent internal consistency, as Cronbach’s α coefficients for each subscale of the MBI-HSS (MP) were calculated to be EE = 0.904, DP = 0.739, and PA = 0.740. Using the criteria of high EE and high DP for the presence of burnout, 23.5% met this measure. Severe burnout was categorized as high EE, high DP, with low PA scores, where 9.8% met this criterion. The overall prevalence of burnout during the COVID-19 pandemic was then 33.3%, with approximately 10% reporting severe levels of burnout. For additional evaluation, participants were segregated into groups that had burnout and those who did not. Pearson’s χ2 and Fisher’s exact tests for categorical independent variables were used to establish factors relevant to burnout.
Significant associations were not observed between socio-demographic characteristics and burnout (p > 0.05), and between occupational variables with burnout (p > 0.05). Lifestyle factors such as use of sleeping pills (p = 0.002) and time spent doing relaxing activities (p = 0.015) were found to have a statistically significant association with burnout (refer to Table 3). There were no demonstrable significant relationships with any other lifestyle characteristics, and they were not found to have a statistically significant association (p > 0.05). Binomial logistic regression was applied to observe the strength of associations of lifestyle characteristics with burnout. The odds ratios (OR) are also presented in Table 3.
HCWs using sleeping pills were demonstrated to have increased odds of developing burnout (OR: 12.667; 95% CI: 2.359, 68.015) as compared to persons who did not use this substance. However, participants taking 1–2 hours for relaxing activities had lowered odds of developing burnout (OR: 0.258; 95% CI: 0.085, 0.788) as compared to persons taking less than one hour. Acceptance and religion were the most utilized coping strategies. Behavioural disengagement was demonstrated to have a significant relationship with burnout (p < 0.001).
Coping styles
Fourteen individual coping strategies were evaluated by the Brief COPE questionnaire. Table 4 shows the median and IQR of the various coping strategies. Acceptance and religion were found to be the most used of the fourteen coping strategies. Behavioural disengagement was demonstrated to have a significant relationship with burnout (p < 0.001), as participants in the burnout group had significantly higher scores in that particular style.
Pandemic experiences and perceptions
A total of 98% of participants indicated that they had been in unmediated contact with COVID-19 positive cases. Additionally, A total of 96.1% participants indicated that they had requisite preparation and ancillary infrastructure necessary to manage the COVID-19 virus. Most participants (98%) expressed some worry of contagion and that the virus presented a potential hazard to them (refer to Table 5).
Discussion
The overall prevalence of burnout during the COVID-19 pandemic was 33.3%, with around 10% of HCWs reporting severe levels of burnout. This was significantly lower than levels seen in studies conducted in high income countries and moderately lower than rates reported in low to middle income countries that ranged from 43% to 48% respectively12. Also, there were no significant differences between burnout levels between doctors and nurses in this study which is similar to some studies13,14, however the literature points to nurses being more predisposed to burnout15,16,17. According to the Job Demands-Resources Model (JD-R) by Demerouti and colleagues, an imbalance between various job aspects and occupational and personal resources can influence health outcomes like burnout in employees18. Most doctors and nurses in this study shared the increased job demand of working in direct contact with COVID-19 positive cases as expressed in the PEPS tool, however, the majority (96.1%) reported that they had the necessary preparation and supportive framework to manage the COVID-19 virus. As per the JD-R model, this balance may have mediated the extent of burnout felt by the study’s respondents, despite high levels of worry (96.1%) of viral contagion.
Gender was not a predictor of burnout in this study. Chinese studies performed during the COVID-19 pandemic by Liu X et al.19 and Li et al.20 similarly found no significant association between burnout and the gender variable, and this was also observed in previous studies21,22,23,24. A meta-analysis of the relationship between gender and burnout showed similarly that there was no male-female difference in burnout, but that women were slightly more emotionally exhausted than men25.
This finding may suggest that workload expectations, job responsibilities and support during the pandemic were equitable between males and females in this healthcare institution, moderating any effect of the gender variable.
Age and position level were not critical predictors of burnout among HCWs. Contrastingly, many studies have shown that both doctors and nurses with low seniority and who were below the age of 40 years have a higher level of job burnout26,27,28. Younger junior HCWs may be more vulnerable to burnout as they have less work experience and have more work tasks assigned to them as well. Possible fairer distribution of workload and individual personality traits may account for the conflicting finding in this study.
There was no demonstrable correlation with specialty departments and burnout levels. A pre-pandemic study by Rodrigues et al. reported a high variability of prevalence across various studies with high prevalence seen in mostly surgical specialties such as general surgery and obstetrics/gynaecology, moderate prevalence in fields such as internal medicine and paediatrics, and low prevalence seen in the otolaryngology and neurology specialties29. During the COVID-19 pandemic, prevalence across specialties varied across countries30,31,32. Probable adaptation processes and enhanced control over work tasks at the approximately three-year mark of the pandemic may have accounted for reduced burnout33.
Sleeping pills usage was associated with burnout in this study. Studies showed a bi-directional relationship between sleep disorders and burnout during the COVID-19 pandemic34,35,36,37. Shecter et al. found that poor sleep was linked with the EE dimension of burnout in a sample of medical professionals in an emergency department38.
The causal-effect relationship between sleeping pill use and burnout in HCWs is inconclusive in the literature, however, due to HCWs’ medical knowledge and access to sleep medication, persons affected by burnout may be more likely to self-medicate to cope or resolve fatigue39,40. The duration of time spent doing relaxing activities was a significant variable in this study, with 1–2 hours, or more than two hours for relaxing activities corresponding to reduced chance of burnout development, compared to those who spent less than one hour. A review of existing literature did not reveal set leisure times that relate to burnout levels, however, less time spent doing relaxing activities relative to time spent working may correlate to work-life imbalance in polled healthcare-workers.41.
Behavioural disengagement, a form of avoidant coping style, was correlated with burnout in this study. Participants reporting high EE had higher scores in the use of different coping styles, more seen in the categories of problem focused coping (use of informational support, positive reframing, planning) and avoidant coping (self-distraction, denial, substance use and behavioural disengagement). Only two emotion-focused coping styles (venting and self blame) were associated with EE. Howlett et al. found that task-oriented coping corresponded with less risk of burnout, while emotion-oriented coping had an elevated risk42.
The use of convenience sampling may have led to several drawbacks such as selection bias, which may have contributed to the over-representation of respondents from the Psychiatry Department. The sampling technique also may limit generalizability to other populations, however, appropriate statistical procedures would have been applied for convenience sampling i.e. non parametric approaches in this research to mitigate effects.
Conclusion
Although the small sample size and sampling technique restricts its generalizability to all populations, the study highlights the need for greater awareness and critical evaluation of the burnout phenomenon during large scale emergencies, such as pandemics. Organizational meaures that may be effective are adequate staffing, training for both doctors and nurses and availability of necessary equipment as seen in this study. Inclusion of HCWs in adjusting on-call hours, equitable distribution of work hours, and access to professional support may reduce sleeping pill use among HCWS, which was a significant factor associated with burnout in this study. Work schedules that provide adequate opportunities to achieve restful sleep that spans six to eight hours have been shown to mitigate burnout rates among HCWs43. From this study, the amount of time engaged in restful activity was shown to be important, and as such, HCWs should ideally engage in relaxation activities for more than one hour to alleviate symptoms of burnout. Scheduled off-days can also be a beneficial measure that can allow for engaging in relaxation activities that may lead to improved productivity levels and job satisfaction in the workplace. Furthermore, leisure activities that allow mastery of a skill and include physical activity can decrease fatigue and enhance personal accomplishment44.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus-19
- COPE:
-
Brief Coping Orientation to Problems Experienced
- TRHA:
-
Tobago Regional Health Authority
References
Maslach, C. & Leiter, M. P. The truth about burnout (Jossey-Bass, 1997).
World Health Organization (WHO). Burn-out an occupational phenomenon: International Classification of Diseases. Available at https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases. Accessed on 25th January, 2023.
Maslach, C. & Jackson, S. E. The measurement of experienced burnout. J. Occup. Behav. 2 (2), 99–113. https://doi.org/10.1002/job.4030020205 (1981).
Schonfeld, I. S., Verkuilen, J. & Bianchi, R. Inquiry into the correlation between burnout and depression. J. Occup. Health Psychol. 24 (6), 603616. (2019). https://doi.org/10.1037/ocp0000151 PMID 30945922. S2CID 92997542.
Ghahramani, S. et al. A systematic review and meta-analysis of burnout among healthcare workers during COVID-19. Front. Psychiatry. 12, 758849 (2021).
Galanis, P., Vraka, I., Fragkou, D., Bilali, A. & Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: a systematic review and meta-analysis. J. Adv. Nurses. 77 (8), 3286–3302 (2021). 21.
7. Shanafelt TD, West CP, Dyrbye LN, Trockel M, Tutty M, Wang H, Carlasare LE, Sinsky C. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin. Proc. J. 97 12 2248–2258 (2022).
Sullivan, D., Sullivan, V., Weatherspoon, D. & Frazer, C. Comparison of nurse burnout, before and during the COVID-19 pandemic. Nurs. Clin. North. Am. J. 57 (1), 79–99 (2022).
Salvagioni, D. A. J. et al. Physical, psychological and occupational consequences of job burnout: a systematic review of prospective studies. PLoS One. 12 (2017).
Pandemic, E. & Perceptions Survey (PEPS) - Assessments, Tests | Mind Garden - Mind Garden. https://www.mindgarden.com/346-pandemic-experiences-perceptions-survey
Brief, C. O. P. E. Coping Orientation Problems Experienced Inventory. https://novopsych.com/assessments/formulation/brief-cope/
Dugani, S., Afari, H. & Hirschhorn, L. R. Prevalence and factors associated with burnout among frontline primary health care providers in low- and middle-income countries: a systematic review. Gates Open. Res. 2, 4 (2018).
Yuguero, O., Ramon Marsal, J., Esquerda, M., Vivanco, L. & Soler-González, J. Association between low empathy and high burnout among primary care physicians and nurses in Lleida, Spain. Eur. J. Gen. Pract. 23 (1), 4–10 (2017). 22.
Hu, Z. et al. Burnout in ICU doctors and nurses in mainland China–a national cross-sectional study. J. Crit. Care. 62, 265–270 (2021).
Dyrbye, L. N., Shanafelt, T. D. & Johnson, P. O. A cross-sectional study exploring the relationship between burnout, absenteeism, and job performance among American nurses. BMC Nurs. 18, 57 (2019).
Hu, Z. et al. Burnout in ICU doctors and nurses in mainland China-a national cross-sectional study. J. Crit. Care. 62, 265–270 (2021).
Gunawan, J., Aungsuroch, Y., Fisher, M. L., Marzilli, C. & Liu, Y. Factors related to the clinical competence of registered nurses: systematic review and meta-analysis. J. Nurs. Scholarsh. 52, 623–633 (2020).
Demerouti, E., Bakker, A. B., Nachreiner, F. & Schaufeli, W. B. The job demands-resources model of burnout. J. Appl. Psychol. 86 (3), 499–512 (2001).
Liu, X. et al. COVID-19 outbreak can change the job burnout in health care professionals. Front. Psychiatry. 11, 563781 (2020).
Li, X., Jiang, T. & Sun, J. The relationship between occupational stress, job burnout and quality of life among surgical nurses in Xinjiang, China. BMC Nurs. 20, 181. (2021). https://doi.org/10.1186/s12912-021-00703-2
Wu, Y. et al. A comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan, China. J. Pain Symptom Manag. 60(1). (2020).
Pu, J. et al. Gender differences in psychological morbidity, burnout, job stress and job satisfaction among Chinese neurologists: a national cross-sectional study. Psychol. Health Med. 22 (6), 680–692 (2017).
Popa, F. et al. Occupational burnout levels in emergency medicine–a stage 2 nationwide study and analysis. J. Med. Life. 3 (4), 449–453 (2010).
SitiHajar, R. & Huda, B. Z. Burnout and its associated factors among nurses in a tertiary hospital, Malaysia. Int. J. Public. Health Clin. Sci. (2018).
Purvanova, R. & Muros, J. Gender differences in burnout: a meta-analysis. J. Vocat. Behav. 77, 168–185. (2020). https://doi.org/10.1016/j.jvb.2010.04.006
Chen, S. C. & Chen, C. F. Antecedents and consequences of nurses’ burnout. Manag. Decis. 56, 777–792 (2018).
Wu, H. et al. Factors related to burnout among Chinese female hospital nurses: cross-sectional survey in Liaoning Province of China. J. Nurs. Adm. Manag. 22, 621–629 (2014).
Yang, G. et al. Burnout and resilience among transplant nurses in 22 hospitals in China. Transplantation Proceedings. ;50:2905–2910. 24 (2018).
Rodrigues, H. et al. Burnout syndrome among medical residents: a systematic review and meta-analysis. PLoS One ;13(11) (2018).
Gramaglia, C. et al. The mental health impact of 2019-nCOVID on healthcare workers from north-eastern piedmont, Italy. Focus on burnout. Front. Public. Health. 9, 667379 (2021).
Hwang, S. et al. Correlates of burnout among healthcare workers during the COVID-19 pandemic in South Korea. Sci. Rep. 13 (1), 3360 (2023).
Wu, Y. et al. A comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan, China. J. Pain Symptom Manage. 60(1). (2020).
Zerbini, G., Ebigbo, A., Reicherts, P., Kunz, M. & Messman, H. Psychosocial burden of healthcare professionals in times of COVID-19 - a survey conducted at the University Hospital Augsburg. Ger. Med. Sci. 18. (2020).
Fu, W. et al. Psychological health, sleep quality, and coping styles to stress facing the COVID-19 in Wuhan, China. Transl Psychiatry. 10, 225 (2020).
Nazari, N., Sadeghi, M., Samusenkov, V. & Aligholipour, A. Factors associated with insomnia among frontline nurses during COVID-19: a cross-sectional survey study. BMC Psychiatry. 22 (1), 1–9 (2022).
Becker, P. M. Overview of sleep management during COVID-19. Sleep. Med. 91, 211–218 (2022).
Lin, Y. N. et al. Burden of sleep disturbance during COVID-19 pandemic: a systematic review. Nat. Sci. Sleep. 13, 933–966 (2021).
Shechter, A. et al. Sleep disturbance and burnout in emergency department health care workers. JAMA Netw. Open. 6 (11), e2341910. https://doi.org/10.1001/jamanetworkopen.2023.41910 (2023).
Hsieh, M. L. et al. Sleep disorder in Taiwanese nurses: a random sample survey. Nurs. Health Sci. 13, 468–474 (2011).
Yazdanshenas, M. et al. The association between life satisfaction and the extent of depression, anxiety and stress among Iranian nurses: a multicenter survey. Iran. J. Psychiatry. 11, 120–127 (2016).
ThimmapuramJR et al. Factors influencing work-life balance in physicians and advance practice clinicians and the effect of heartfulness meditation conference on burnout. Global Adv. Health Med. 8, 2164956118821056 (2019).
Howlett, M., Doody, K. & Murray, J. Burnout in emergency department healthcare professionals is associated with coping style: a cross-sectional survey. Emerg. Med. J. 32, 722–727 (2015).
Wisetborisut, A. et al. Shift work and burnout among health care workers. Occup. Med. (Lond.) 64 (4), 279–286 (2014).
Shamblaw, A. L., Rumas, R. L. & Best, M. W. Coping during the COVID-19 pandemic: Relations with mental health and quality of life. Can. Psychol. 62 (1), 92–100 (2021).
Acknowledgments
The co-author GA acknowledges Brendon Bhagwandeen, Lecturer, Department of Mathematics and Statistics, University of the West Indies, St. Augustine Campus for his statistical consultation on this research.
Funding
This research was self-funded.
Author information
Authors and Affiliations
Contributions
NB approved the research’s concept and design, supervised the interpretation of the data and research’s revision. GA conceptualised the research’s concept, draft, design and revisions, and substantially contributed to the data acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interests
The authors declare no competing interests.
Ethical approval
Ethical approval was granted by the Campus Research Ethics Committee of the University of the West Indies, the Research Ethics Committee (REC) of the Tobago House of Assembly (THA) and the Tobago Regional Health Authority (TRHA).
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Baboolal, N., Alexander, G. Burnout syndrome among Tobagonian healthcare-workers during the COVID-19 pandemic. Sci Rep 16, 14417 (2026). https://doi.org/10.1038/s41598-026-46230-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-46230-5
