
Abstract
Obstructive sleep apnea (OSA) and smoking are both prevalent and impactful health risks. While smoking may contribute to OSA through inflammatory and neuromuscular pathways, population-based evidence on this relationship remains limited and inconsistent. A sample (N = 1,206) from the population-based Study of Health in Pomerania with complete overnight polysomnography and smoking assessment was investigated in a cross-sectional study for an association between OSA and former as well as recent smoking status. Regression models adjusted for Age and BMI were applied. Current smoking was significantly associated with increased apnea-hypopnea-index (AHI) severity (OR = 1.75, 95% CI [1.27; 2.41], p < .001), with stratified analyses confirming the effect across younger and older participants. Former smokers also showed significantly elevated AHI severity compared to never-smokers (OR = 1.76, 95% CI [1.27; 2.43], p < .001). Both current and former smoking were significantly associated with greater OSA severity in this population-based sample, even after accounting for age and BMI. The findings underscore the long-term respiratory consequences of smoking and highlight the need for integrated approaches in smoking cessation and OSA screening.
Similar content being viewed by others

Introduction
Obstructive sleep apnea (OSA) is characterized by intermittent episodes of partial or complete upper airway blockage during sleep, resulting in a cessation of airflow and a marked decrease in oxygen saturation. Much like smoking, sleep apnea is widely acknowledged to exert a considerable detrimental effect on health, both in the short and the long term1,2. Similar to smoking, OSA increases the risk for cardiovascular and metabolic diseases, stroke, and overall mortality substantially2. Like smoking, it is endemic – worldwide, an estimated one billion people are at risk, with 425 million most likely affected, resulting in a substantial economic burden on healthcare systems and society at large (e.g., the economic damage in Italy alone is estimated to range from €13.8 to €41.3 billion per annum)3,4. In the adult population in Pomerania, Germany, observed in this study, 46% of the tested participants were at risk and 6% fulfilled the diagnostic criteria for obstructive sleep apnea syndrome (OSAS) based on an increased apnea-hypopnea-index (AHI, the number of obstructions per hour during sleep) and self-reported daytime sleepiness5. Smoking may contribute to the onset and progression of OSA by altering sleep architecture, impairing upper airway neuromuscular reflexes, and causing upper airway inflammation6. A bidirectional effect is also possible: OSA may contribute to depression and reduced quality of life, which may, in turn, increase the likelihood of smoking initiation or hinder cessation efforts6,7.
In a recent meta-analysis by Zeng et al. a stable association between current smoking and OSA relying on overnight polysomnography (PSG) was found, which did not appear to be alleviated by smoking cessation8. However, this finding is not uniformly supported. For example, in a large patient study (N = 3,718) in Sao Paulo, Brazil, it was found that former smokers were less affected by OSA9. In some patient studies, the association between a history of smoking and OSA could not be substantiated at all10,11,12,13. A retrospective study with 3,791 patients of a sleep clinic in Thessaloniki, Greece, and another study with 733 patients of a sleep clinic in Changhua, Taiwan, found an elevated AHI in smokers, but the association became non-significant after adjustment for age, body-mass-index (BMI) and other confounders11,12. Population-based studies on this topic remain scarce. Using data from the Korea National Health and Examination Survey, an association between the STOP-Bang questionnaire (a screening instrument for OSA14 and smoking was observed15. Because of the absence of PSG this study lacks exact AHI values, which limits its interpretability.
The present study aimed to address the lack of population-based evidence regarding the relationship between smoking and OSA. We used data on smoking behavior, polysomnography (PSG), and relevant covariates from the TREND-0 cohort of the Study of Health in Pomerania (SHIP), a population-based survey conducted in northeastern Germany16. The primary objective was to examine whether current or former smoking is associated with OSA severity, as measured by AHI, while adjusting for key confounders age and BMI.
Methods
Sample
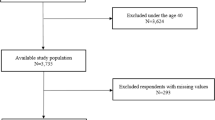
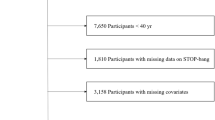
The study sample was a subsample of SHIP, a population-based cohort study aimed at monitoring health status in the West Pomerania region of Germany16. All participants gave informed consent in writing. The study was approved by the local ethics committee. As part of the initial assessment of the SHIP-TREND cohort (2008–2012), participants were invited to undergo overnight PSG in a sleep laboratory17. Out of the 4,420 individuals in the SHIP-TREND-0 cohort, 1,264 agreed to participate. Complete data on Apnea-Hypopnea Index (AHI) was obtained for 1,209 individuals. Of these 1,206 completed the smoking interview. No further exclusion criteria were applied - all 1,206 individuals with complete data on AHI and on smoking status were included in the analysis.
Polysomnography
An attended, laboratory-based overnight PSG was conducted in accordance with the American Academy of Sleep Medicine (AASM)18 guidelines, using ALICE 5 PSG devices (Philips Respironics, Eindhoven). Recordings included six electroencephalogram (EEG) channels, two electrooculogram (EOG) channels, three electromyogram (EMG) channels (at the chin and tibialis muscles of each leg), one electrocardiogram (ECG), respiratory inductive plethysmography, a nasal pressure sensor, pulse oximetry, a snoring microphone, and a body position sensor. Sleep stages, respiratory events, and arousals were scored according to the same AASM guidelines18.
Smoking
Smoking behavior was assessed through a structured interview with a specific focus on cigarette consumption19. Among other things, participants were asked if they ever smoked a cigarette and if applicable whether they are currently smoking, how many cigarettes they smoke per day, whether they ever smoked on a regular basis, or at what age they started or quit smoking. Smoking hiatus was not recorded - only a start date and potentially an end date were collected.
Study variables
Variables of interest
Two variables of interest were introduced in separate models. For the first variable of interest “smoker”, participants were divided in current regular smokers (N = 208) and non-smokers as well as occasional smokers (N = 998, including former smokers, see below). Current regular smokers smoked at least one cigarette per day. For the second variable of interest “former smoker” current non-smoking participants were divided in former smokers (N = 190, excluding short term quitters, see below) and never-smokers (N = 495). Former smokers were defined as regular smokers for at least ten years that had quit smoking one year or longer ago20. Current smokers were excluded from all analyses concerning the variable “former smoker”.
Confounders
Age. In Germany, smoking behavior varies across different age groups21. As participants age they have more opportunity to start and eventually quit smoking and there is a minimum age where participants could have stopped smoking for 10 years or longer. Age is also an established factor in sleep apnea and is associated with musculoskeletal changes in the pharynx22. The regular smokers had a mean age of m = 45 years (SD = 13, range: 20–78) while the non-smokers and occasional smokers had a mean age of m = 54 years (SD = 14, range: 22–81). The former smokers had a mean age of m = 59 years (SD = 11, range: 25–80) while the never-smokers had a mean age of m = 53 years (SD = 14, range: 21–81).
BMI. Smoking as well as AHI is associated with BMI23,24. The regular smokers had a mean BMI of m = 27.5 (SD = 4.7, range: 18.5–41.8) while the non-smokers and occasional smokers had a mean BMI of m = 28.7 (SD = 5.0, range: 18.4–52.8). The former smokers had a mean BMI of m = 30.4 (SD = 4.6, range: 20.3–52.1) while the never-smokers had a mean BMI of m = 28.4 (SD = 5.0, range: 18.4–50.1).
Outcome
AHI. The regular smokers had a mean AHI of m = 10.3 (SD = 15.1, range: 0–85.9) while the non-smokers and occasional smokers had a mean AHI of m = 10.7 (SD = 14.2, range: 0–91.8). The former smokers had a mean AHI of m = 15.1 (SD = 15.9, range: 0–72.7) while the never-smokers had a mean AHI of m = 9.4 (SD = 12.9, range: 0–89.1).
Table 1 provides an overview of the descriptive statistics for the study sample.
Data analysis
For data analysis and visualization R Statistics25 with the packages haven26, dplyr27, MASS28, ggplot229, brant30, car31, splines32, tableone33, and gvlma34 were utilized. Separate planned linear regressions were computed for an immediate and a long-term model with the confounders age and BMI. In case model assumption were violated, additional tests were conducted to validate the robustness of the results.
Results
Visualization
Linear associations between AHI and age for the non-obese and the obese participants (BMI ≥ 30 kg/m²) were visualized for the smokers and non-smokers (Fig. 1) as well as the former smokers and the never-smokers (Fig. 2) separately.

AHI according to age for smokers (red) and non-smokers (blue) for the non-obese participants (a) and the obese participants (b).

AHI according to age for the former smokers (red) and the never-smokers (blue) for the non-obese participants (a) and the obese participants (b).
Regression analyses
Smoker vs. non-smokers. To test the association between the dichotomous variable of interest Smoker (smoker / non-smoker) and AHI, a linear regression model with the continuous confounders Age (in years) and BMI (in kg/m²) was computed. In this linear regression model the variable of interest Smoker was significantly associated with the outcome AHI, β = 3.11 [CI 1.13; 5.10], p = .002, however, a non-linear distribution of residuals indicated that assumptions of the model might be violated. Therefore, an ordinal logistic regression model with the same variable of interest and confounders on the AHI severity (AHI < 5: normal, 5 ≤ AHI < 15: mild, 15 ≤ AHI < 30: moderate, AHI ≥ 30: severe) was computed. Smoking status remained significantly associated with higher AHI severity categories, OR 1.75 [CI 1.27; 2.41], p < .001. However, a Brand-Wald-test indicated that the assumption of proportional odds might be invalidated for the model. A closer inspection of Fig. 1 reveals that smokers and non-smokers might have different centroids concerning the variable Age. Therefore, participants were split into two age groups roughly at the median (younger: age in years < 54, older: age in years ≥ 54, see Table 2) and the ordinal logistic regression was repeated for both age groups separately, yielding significant results for the variable of interest Smoker for the younger participants, OR 1.56 [CI 1.03; 2.35], p = .036, and the older ones, OR 1.75 [CI 1.27; 2.41], p < .001, as before. Keeping all other factors stable, being a regular smoker increases the chance of having a higher severity grade of sleep apnea by 56% for the younger participants and respectively by 75% for the older ones.
Former smoker vs. never-smoker. Similarly to analysis of smoker vs. non-smoker, a linear regression model with the continuous confounders Age (in years) and BMI (in kg/m²) on AHI (apnea and hypopnea events/h) for the dichotomous variable of interest Former Smoker (former smoker / never-smoker) was computed. The variable of interest Former Smoker was significantly associated with the outcome AHI, β = 3.13 [CI 0.99; 5.28], p = .004, but a non-linear distribution of residuals indicated that assumptions of the model might not be fulfilled. Therefore, an ordinal logistic regression model on the AHI severity (AHI < 5: normal, 5 ≤ AHI < 15: mild, 15 ≤ AHI < 30: moderate, AHI ≥ 30: severe) for the same predictor and confounders as before was computed, resulting in a significant association between Former Smoker and AHI severity, OR 1.76 [CI 1.27; 2.43], p < .001, indicating that compared to the never-smoker a former smoker had a 76% higher chance of reaching a higher severity grade of sleep apnea, given both other factors were held stable. To allow for an analogue interpretation groups were split as for the smokers vs. non-smokers at the median age (younger: age in years < 57, older: age in years ≥ 57, see Table 3). For the younger participants, the association between AHI and former smoker status failed the conventional level of significance OR 1.49 [CI 0.89; 2.49], p = .13, whereas in the older participants the association was significant, OR 1.91 [CI 1.26; 2.91], p = .002, resulting in a higher relative risk of 49% or of 91% being in the group with the higher severity grade.
Discussion
Concerning current smokers, our findings align with the current meta-analysis by Zeng et al.8, as we found a substantial association with OSA with an increased relative risk of a higher severity grade of 56% for the younger and 75% for the older participants. Likewise, our findings are in line with the meta-analysis regarding former smokers with a nearly identical relative risk of 76%. Looking at the relative risk for age groups separately, a relative higher risk of 49% is found in the younger and of 91% in the older participants.
These findings are in line with several pathophysiological mechanisms explaining the association between smoking and increased OSA severity. Cigarette smoke promotes upper airway inflammation and oxidative stress, narrowing the airway and increasing its collapsibility during sleep35,36. Structural changes elevate airway resistance and exacerbate upper airway obstruction in smokers with OSA37. Moreover, smoking amplifies OSA related hypoxia, promoting systemic inflammation and further airway dysfunction38.
Strength and limitations
This study is based on a large population-based cohort with objective assessment of OSA using full-night polysomnography, reducing selection bias and improving generalizability in contrast to patient samples. Participation in polysomnography was voluntary, and individuals with sleep-related symptoms such as snoring may be overrepresented; however, there is no indication that this resulted in systematic bias in AHI distribution5,39. Detailed smoking data allowed differentiation between current, former, and never smokers. Adjustment for key confounders and using alternative modeling approaches support the robustness of the findings. Analyses of former versus never smokers may have been underpowered duo to limited number of the later. Residual and unmeasured confounding cannot be excluded. The cross-sectional design precludes causal inference.
Conclusion
Although the detrimental effects of smoking are well established, the present findings might paradoxically be interpreted as discouraging cessation, potentially fostering a fatalistic attitude that the damage is already done once smoking becomes habitual. However, it is important to note here that our results concern long term smokers after an indeterminable time (but at least a year) of non-smoking. Shorter smoking histories and longer periods of cessation might lead to more beneficial outcomes. Furthermore, our current study and most studies included in aforementioned meta-analysis were retrospective or cross-sectional in nature, limiting a causal interpretation that smoking contributes to the development or progression of OSA. Given the lower odds ratios observed in the younger participants, one might cautiously speculate that this age group exhibits greater resilience concerning OSA in smokers or hope for more regenerative capacity in response to the long-term effects of smoking on OSA. Taking into account that continued smoking is detrimental to other health factors, too, of which at least some are partially reversible, there seems to be no reason to not recommend smoking cessation1,20,40. Yet, there is a problem. Smoking cessation might lead to weight gain, which in turn increases cardiovascular risk41. But for OSA, weight-loss management is recommended to reduce the AHI and the cardiovascular risks associated with obesity (and OSA for that matter)42,43. While smoking cessation and weight management should both be considered key components of care in smokers with OSA, addressing both simultaneously may be overwhelming for patients. Prioritization should therefore be guided by individual patient circumstances and preferences44. The only way to win this game is to not start smoking in the first place.
Data availability
The data that support the findings of this study are available from the Transferstelle für Daten- und Biomaterialienmanagement [Office for transfer of data and bio materials] of the University Medicine Greifswald, Study of Health in Pomerania (SHIP: https://transfer.ship-med.uni-greifswald.de/FAIRequest/). Access is restricted and needs approval of the board.
References
Bonnie, R. J., Stratton, K. & Kwan, L. Y. The effects of tobacco use on health. Public health implications of raising the minimum age of legal access to tobacco products. National Academies Press (US) (2015).
Wang, Q. et al. Association between obstructive sleep apnea and multiple adverse clinical outcomes: evidence from an umbrella review. Front. Med. 12, 1497703. https://doi.org/10.3389/fmed.2025.1497703 (2025).
Benjafield, A. V. et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respiratory Med. 7, 687–698. https://doi.org/10.1016/S2213-2600(19)30198-5 (2019).
Borsoi, L. et al. The invisible costs of obstructive sleep apnea (OSA): Systematic review and cost-of-illness analysis. PLoS ONE. 17, e0268677. https://doi.org/10.1371/journal.pone.0268677 (2022).
Fietze, I. et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences – Results of SHIP-Trend. J. Sleep Res. 28, e12770. https://doi.org/10.1111/jsr.12770 (2019).
Krishnan, V., Dixon-Williams, S. & Thornton, J. D. Where There Is Smoke… There Is Sleep Apnea. Chest 146, 1673–1680. https://doi.org/10.1378/chest.14-0772 (2014).
Vogler, K. et al. Quality of life in patients with obstructive sleep apnea: Results from the study of health in Pomerania. J. Sleep Res. 32, e13702. https://doi.org/10.1111/jsr.13702 (2023).
Zeng, X. et al. Association Between Smoking Behavior and Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. Nicotine Tob. Res. 25, 364–371. https://doi.org/10.1093/ntr/ntac126 (2023).
Conway, S. G. et al. Effect of smoking habits on sleep. Braz J. Med. Biol. Res. 41, 722–727. https://doi.org/10.1590/S0100-879X2008000800014 (2008).
Shao, C. et al. Smoking history and its relationship with comorbidities inpatients with obstructive sleep apnea. Tob. Induc. Dis. 18 https://doi.org/10.18332/tid/123429 (2020).
Hsu, W-Y. et al. The association between cigarette smoking and obstructivesleep apnea. Tob. Induc. Dis. 17 https://doi.org/10.18332/tid/105893 (2019).
Ioannidou, D. et al. Smoking and Obstructive Sleep Apnea: Is There An Association between These Cardiometabolic Risk Factors?—Gender Analysis. Medicina 57, 1137. https://doi.org/10.3390/medicina57111137 (2021).
Esen, A. D. & Akpinar, M. Relevance of obstructive sleep apnea and smoking: Obstructive sleep apnea and smoking. Fam. Pract. 38, 180–185. https://doi.org/10.1093/fampra/cmaa112 (2021).
Chung, F. et al. STOP Questionnaire: A Tool to Screen Patients for Obstructive Sleep Apnea. Anesthesiology 108, 812–821. https://doi.org/10.1097/ALN.0b013e31816d83e4 (2008).
Chung, Y. & Kim, J-S. Association between health-related behaviors and obstructive sleep apnea among Korean adults. Sci. Rep. 14, 21244. https://doi.org/10.1038/s41598-024-72401-3 (2024).
Völzke, H. et al. Cohort Profile Update: The Study of Health in Pomerania (SHIP). Int. J. Epidemiol. dyac034 https://doi.org/10.1093/ije/dyac034 (2022).
Stubbe, B. et al. Polysomnography in a Large Population Based Study-the Study of Health in Pomerania Protocol. J. Sleep. Disord Manag. 2 https://doi.org/10.23937/2572-4053.1510010 (2016).
Sateia, M. J. International Classification of Sleep Disorders-Third Edition. Chest 146, 1387–1394. https://doi.org/10.1378/chest.14-0970 (2014).
Völzke, H. et al. Prevalence Trends in Lifestyle-Related Risk Factors. Deutsches Ärzteblatt international. Published Online First: 13 March. https://doi.org/10.3238/arztebl.2015.0185 (2015).
Hahad, O. et al. Chronic cigarette smoking is associated with increased arterial stiffness in men and women: evidence from a large population-based cohort. Clin. Res. Cardiol. 112, 270–284. https://doi.org/10.1007/s00392-022-02092-1 (2023).
Zeiher, J., Kuntz, B. & Lange, C. Smoking among adults in Germany. J. Health Monit. 2, 57–63. https://doi.org/10.17886/RKI-GBE-2017-043 (2017).
Silva, M., Poyares, S. & Silva, D. Associations of the Severity of Obstructive Sleep Apnea With Age-Related Comorbidities: A Population-Based Study. Front. Neurol. 13 https://doi.org/10.3389/fneur.2022.802554 (2022).
Chao, A. M. et al. Tobacco Smoking, Eating Behaviors, and Body Weight: a Review. Curr. Addict. Rep. 6, 191–199. https://doi.org/10.1007/s40429-019-00253-3 (2019).
Ong, C. W. et al. The reciprocal interaction between obesity and obstructive sleep apnoea. Sleep Med. Rev. 17, 123–131. https://doi.org/10.1016/j.smrv.2012.05.002 (2013).
R Core Team. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, 2024).
Wickham, H., Miller, E. & Smith, D. haven: Import and Export SPSS, Stata and SAS Files. https://cran.r-project.org/web/packages/haven/index.html (2023).
Wickham, H. et al. dplyr: A Grammar of Data Manipulation. https://cran.r-project.org/web/packages/dplyr/index.html (2023).
Ripley, B. et al. MASS: Support Functions and Datasets for Venables and Ripley’s MASS. https://cran.r-project.org/web/packages/MASS/index.html (2024).
Wickham, H. et al. ggplot2: Create Elegant Data Visualisations Using the Grammar of Graphics. https://cran.r-project.org/web/packages/ggplot2/index.html (2024).
Schlegel, B. & Steenbergen, M. brant: Test for Parallel Regression Assumption. https://CRAN.R-project.org/package=brant (2020).
Fox, J. et al. Ccar: Companion to Applied Regression. https://cran.r-project.org/web/packages/car/index.html (2023).
Bates, D. M. & Venables, W. N. Regression Spline Functions and Classes. https://cran.r-project.org/doc/manuals/r-patched/packages/splines/refman/splines.html
Yoshida, K. et al. Tableone: Create Tables 1 to Describe Baseline Characteristics with or without Propensity Score Weights. https://cran.r-project.org/web/packages/tableone/index.html (2022).
Pena, E. A., Slate, E. H. & gvlma Global Validation of Linear Models Assumptions. https://cran.r-project.org/web/packages/gvlma/index.html (2019).
Cohen, O. et al. Pharyngeal Inflammation on Positron Emission Tomography/Magnetic Resonance Imaging Before and After Obstructive Sleep Apnea Treatment. Annals ATS. 20, 574–583. https://doi.org/10.1513/annalsats.202207-594oc (2023).
Jang, Y. S. et al. Association between smoking and obstructive sleep apnea based on the STOP-Bang index. Sci. Rep. 13 https://doi.org/10.1038/s41598-023-34956-5 (2023).
Grigoriou, I. et al. Smoking History and Nicotine Dependence Alter Sleep Features in Patients with Obstructive Sleep Apnea-Hypopnea Syndrome. Healthcare 13, 49. https://doi.org/10.3390/healthcare13010049 (2024).
Wuttiumporn, K. et al. Associations between Airway Inflammation and Indices of Sleep Apnea Severity in Obstructive Sleep Apnea Patients. Srinagarind Med. J. 32, 102–106 (2018).
Krüger, M. et al. Socioeconomic factors do not predict sleep apnea in a population sample from Mecklenburg-Western Pomerania, Germany. Sleep. Breath. 27, 459–467. https://doi.org/10.1007/s11325-022-02614-1 (2023).
Tomiyama, H. et al. Continuous Smoking and Progression of Arterial Stiffening. J. Am. Coll. Cardiol. 55, 1979–1987. https://doi.org/10.1016/j.jacc.2009.12.042 (2010).
Wang, X. et al. Smoking Cessation, Weight Gain, Cardiovascular Risk, and All-Cause Mortality: A Meta-analysis. Nicotine Tob. Res. 23, 1987–1994. https://doi.org/10.1093/ntr/ntab076 (2021).
Messineo, L. et al. Obstructive sleep apnea and obesity: A review of epidemiology, pathophysiology and the effect of weight-loss treatments. Sleep Med. Rev. 78, 101996. https://doi.org/10.1016/j.smrv.2024.101996 (2024).
John, U. Smoking status, obesity and hypertension in a general population sample: a cross-sectional study. QJM 99, 407–415. https://doi.org/10.1093/qjmed/hcl047 (2006).
Oțelea, M. R. et al. Smoking Obstructive Sleep Apnea: Arguments for a Distinctive Phenotype and a Personalized Intervention. JPM 12, 293. https://doi.org/10.3390/jpm12020293 (2022).
Acknowledgements
The Study of Health in Pomerania (SHIP) is part of the Community Medicine Research Network of the University Medicine Greifswald, which is supported by the German Federal State of Mecklenburg-West. AI tools were used to assist with language refinement and formatting.
Funding
Open Access funding enabled and organized by Projekt DEAL. No specific funding was received for the analysis or preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
MK: Conceptualization, Methodology, Formal analysis, Visualization, Writing - original draft. CP: Formal analysis, Visualization, Writing - review & editing. HJ: Writing - review & editing. AW: Writing - review & editing. C-JB: Writing - review & editing. CS: Writing - review & editing. TB: Writing - review & editing. RE: Writing - review & editing, Data curation. AO: Writing - review & editing, Data curation. TP: Writing - review & editing, Data curation. IF: Writing - review & editing, Data curation. BK: Writing - review & editing. TK: Writing - review & editing. RB: Writing - review & editing. HV: Writing - review & editing. AD: Writing - review & editing, Conceptualization.
Corresponding author
Ethics declarations
Competing interests
TP reports consulting fees from Cerebra and Takeda; speaker honoraria from Jazz Pharmaceuticals and Idorsia; travel support from Philips and Sleepimage; advisory board participation for Takeda (personal) and Bayer (institutional); leadership roles in the German Sleep Society (past president) and World Sleep Society (president-elect, unpaid); shares in Advanced Sleep Research and The Siestagroup GmbH; and receipt of devices from Neurovirtual and Sleepimage. RE reports research support from Löwenstein Medical; grants and/or lecture honoraria from Janssen Germany, OMT Germany, AOP, Boehringer Ingelheim, and Berlin Chemie; consulting fees from AOP Germany and Janssen Germany; travel support from Novartis Germany and Janssen Germany; and advisory board roles with AOP Germany and Janssen Germany. All authors affirm that they received no financial support related to this work other than as disclosed above. The tobacco and nicotine delivery industry had no involvement in this work.
Ethical approval
Data retrospectively examined in this study is part of the population-based Study of Health in Pomerania (SHIP) approved by the ethics committee of the University Medicine Greifswald and in full compliance with ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Consent for publication
The authors take full responsibility for the accuracy, interpretation, and integrity of the content presented in this research.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Krüger, M., Pink, C., Jiang, H. et al. Breathing bad: increased risk for obstructive sleep apnea in current and former smokers. Sci Rep 16, 13382 (2026). https://doi.org/10.1038/s41598-026-48908-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-48908-2
