
Abstract
Acute aortic dissection (AAD) is a life-threatening emergency without established effective monitoring biomarkers. This study aimed to explore biomarkers to optimize the diagnosis of AAD. AAD related genes were screened by spatial transcriptomics experiments, and their encoded proteins were validated in aortic tissues. We measured plasma levels of candidate proteins in 302 participants (173 AAD cases, 129 controls), finding higher PTMA, ADAMTS8, and CD36 in AAD. Case-control analysis revealed that elevated levels of those proteins along with d-dimer, increased systolic blood pressure (SBP), height and smoking history were risk factors for AAD. A multi-marker score comprising d-dimer, ADAMTS8, height, SBP, and age was developed for AAD diagnosis, achieving an AUC of 0.921 (95%CI 0.889–0.952), with 77.5% sensitivity and 96.5% specificity. We further validated the diagnostic performance of the multi-marker score in an independent validation set including healthy controls and patients with chest pain. Our findings indicate that PTMA, ADAMTS8, and CD36 are potential biomarkers associated with AAD. The multi-marker score effectively discriminates AAD from both healthy controls and non-AAD acute chest pain conditions, and may serve as a rapid, cost-effective auxiliary diagnostic tool.
Similar content being viewed by others


Introduction
As a life-threatening cardiovascular disease, acute aortic dissection (AAD) is a rapidly fatal clinical emergency, with high rates of mortality. According to the International Register of Aortic Dissection Studies data1, the annual incidence of AAD in European or American countries is about 3–5 cases per 100,000 individuals. In accordance with the prediction of the UK’s Office for National Statistics population projections, the number of the incident dissection events will increase from 3892 in 2010 to 6893 in 20502. In addition, the overall global death rates from AAD have increased during the past two decades and it seems to be more evident in developing countries. Despite important advances in diagnostic and therapeutic interventions, the burden of AAD treatment remains clinically high challenging3. The untreated mortality is approximately 1%–2% per hour following symptom onset, and it remains high even after surgical intervention4,5. Therefore, early identification and confirmation of a suspected AAD diagnosis, along with timely and appropriate intervention, are crucial in reducing mortality rates6. Currently, the diagnosis of AAD mainly relies on imaging techniques including ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI)7. However, these methods, while recommended for screening in high-risk populations and for assessing patients at the onset of symptoms, are not suitable for early screening in the general population3,8,9. Consequently, there is a pressing need to identify specific biomarkers for AAD in both clinical practice and research, due to the concealment of the disease.
Biomarkers are helpful to diagnose and determine the risk of AAD in a timely and easily available manner3,10. Currently, potential biomarkers have been focusing on those associated with pathophysiologic changes in aortic wall, such as smooth muscle markers, which reflect the disintegration and release of medial smooth muscle cellular components into the circulation during dissection11,12. Similarly, extracellular matrix proteins (ECM), inflammatory response and markers are also released into the circulation10. More biomarkers including cardiac stress or damage, thrombosis or fibrinolysis and inherited predisposition are being researched. d-dimer reflects the dynamic coagulation state and is recognized as an exclusion biomarker for pulmonary embolism. It has a clinically relevant role in suspected AAD and is highly sensitive to AAS. Several studies have shown that d-dimer has a clinically relevant role in suspected AAD13,14. However, the specificity of d-dimer ranges from 40 to 100%6,15 which may be lower in patients with false lumen thrombosis, less extensive disease and younger age individuals16. Moreover, the negative d-dimer test result is not sufficient to exclude AAD, and other meaningful indicators need to be combined to optimize the diagnosis.
The emerging paradigm of precision medicine highlights the importance of quantitative portray of molecular features during disease onset and progression. Dynamic markers, especially the circulating proteins, may help to capture the disease trajectory and to offer precise prognostication for AAD patients17. In our previous studies, we have collected AAD tissues and conducted an initial exploration of AAD-related genes by spatial transcriptomics (ST)18. To study how genes affect health and disease, and to find novel biomarkers, it is essential to further investigate the expression of proteins encoded by these genes in dissection tissues and blood circulation.
Leveraging the AD resources using ST, we sought to (1) screen the AAD related genes, (2) validate the protein expression encoded by these genes in tissues, (3) confirm protein expression in blood circulation in larger clinical blood samples, (4) develop diagnostic panels to differentiate AAD from healthy controls, and (5) explore the discriminative efficacy in patients with chest pain. We also included an independent validation set to verify the diagnostic performance of the developed panels. We hope that these identified candidate proteins can assist in the clinical diagnosis of AAD and ultimately improve the treatment strategies for this condition.
Materials and methods
Study design and patients’ enrollment
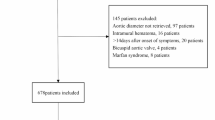
The overall experimental design is summarized in Fig. 1. The human aortic samples used for ST analysis and protein validation were collected from patients undergoing vascular replacement surgery. Control tissues were from organ donation patients. The clinical research is comprised a retrospective discovery set and a validation set. In the discovery set, 173 patients diagnosed with AAD through computed tomography angiography from December 2021 to December 2023 and 129 healthy control patients were included to evaluate the diagnostic performance of candidate molecules in distinguishing AAD from the normal population. In order to further validate the diagnostic value of the screened biomarkers, we designed an independent validation set, including suspected acute AAD patients with chest pain who visited the emergency department from March 2025 to March 2026. Finally, confirmed pulmonary embolism patients (PE) (42 patients), confirmed AAD patients (130 patients), patients with acute myocardial infarction (AMI) (99 patients), along with 122 healthy control patients. Human subjects with the Marfan syndrome, Ehlers-Danlos syndrome, bicuspid aortic valve, malignant tumor, pregnancy and trauma were excluded. Baseline characteristics including medical history, physical examination biochemical data and surgical information were obtained through medical records. All clinical specimens were recruited from the First Affiliated Hospital of Xinjiang Medical University and the People’s Hospital of Xinjiang Uygur Autonomous Region.

The overall experimental design.
Written informed consent forms were obtained from the patients or the donors’ families. The research protocol conforms to the ethical guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (20150006-8) and the Ethics Committee of People’s Hospital of Xinjiang Uygur Autonomous Region (KY2022072259).
ST experiments and data analysis
ST detection of AAD is our previous study18. The detailed collection and preparation of aortic samples and the following 10x Genomics and ST sequencing experiments were described in our previous studies18. In short, spatial gene expression library was constructed on Illumina’s NOVA 6000 platform. The Seurat package (version 3.1.3) implemented in R software19 was used to analyze the gene-spot matrices derived from ST data processing and Visium samples. Perform subsequent analysis using principal component analysis (PCA) and ICA methods, and cluster each point based on K-nearest neighbor algorithm. A spatial cluster gene list was generated for all genes differentially expressed in ST clusters (average logFC > 0.25, P value < 0.05, and only retained positively regulated genes). Compare the expression of each gene from one cluster to the spots of all other clusters with the average expression. The DEGs with the largest changes in expression in each cluster were ranked. Cell Marker database20, clusterProfiler (version 3.12.0)21, and Human Cell Landscape (HCL) database were helped to classify the cell subpopulations and identify the Cell types of different locations.
Histological analysis
The aorta samples were quickly washed with cold saline solution immediately after surgical resection, then frozen in liquid nitrogen for protein extraction or fixed in 4% paraformaldehyde for 24 h. Following the standard paraffin embedded, cross sections were prepared at 5 μm for immunohistochemical (IHC) staining. The antibodies were as follows: cluster of differentiation 36 molecule (CD36, 1:100, Novus Biologicals, NB400-144), a disintegrin and metalloproteinase with thrombospondin motifs 8 (ADAMTS8, 1:100, Abnova, PAB18816) and prothymosin α (PTMA, 1:200, ABGENT, AP11770a). The images were captured using a Leica microscope system. For quantitative analysis, Image-Pro Plus 6.0 software was used to evaluate the area and the integrated optical density (IOD) value of each IHC sections and calculate the mean density.
Protein extraction and western blot analysis
Extract total protein from human aortas using the Minute™ Total Protein Extraction Kit for Blood Vessels (SA-03-BV, Invent Biotechnologies). Standard sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) protocols and PVDF membranes were employed to detect target protein expression. The following primary antibodies were used: CD36 (1:1000, Abcam, ab252923), ADAMTS8 (1:300, Abnova, PAB18816) and PTMA (1:1000, ABGENT, AP11770a). Glyceraldehyde-3-phosphate dehydrogenase (GAPDH, 1:1000, Cell Signaling, 5174s) was used as loading control.
Collection of plasma samples and measurements of target proteins
Blood samples were obtained from participants and collected from AAD patients before surgery. After centrifuged, plasma was immediately processed and stored at − 80 °C before measured. Circulating target proteins were measured using ELISA double antibody sandwiched method (Jianglai Bio., Shanghai, China) according to the manufacturer’s instructions. To ensure accuracy, all samples were analyzed in duplicate, and both intra- and inter-assay coefficients of variation were maintained at less than 10%.
Clinical data collection
We collected the clinical information from patients’ electronic medical records, including age, gender, symptom, body mass index, blood pressure, heart rate, history of smoking, hyperlipidemia and hypertension. Biochemical and hematological data were also recorded.
Statistical analysis
Continuous variables were expressed as mean with standard deviation (SD) or median with interquartile range (IQR) for skewed variables. We used the unpaired Student’s t-test or the Mann-Whitney U test to compare variables between groups. Categorical variables are presented as frequencies and percentages and were conducted with chi-square test. Univariate and multivariate Logistic regression analyses were performed to identify independent risk factors for AAD. Results were presented as odds ratio (OR) with 95% confidence interval (CI).
PCA was utilized to figure out the distribution pattern of epidemiological risk factors between healthy subjects or AAD patients, while identifying the most important variables contributing to different patterns (ranked by PCA loadings). For all proteins and clinical parameters, we selected biomarkers to develop the AAD diagnostic multi-marker score system through PCA loadings, according to the optimal predictive thresholds from receiver operating characteristic (ROC) analysis and practice guidelines: d-dimer ≥ 500 ng/mL22, ADAMTS8 ≥ 802.5 pg/mL, Height ≥ 166.5 cm, SBP ≥ 140 mmHg2,23 and Age ≥ 65 years3,6. 1 point was assigned to each selected biomarker described above and multiple biomarker scores was generated from 0 to 5. We used regression curves with restricted cubic spline analysis to check the relationship between multi-marker score as a continuous variable and AAD events. ROC curve and area under the curve (AUC) were calculated and compared to assess the diagnostic performance and predictive capability of the multi-marker score.
Statistical analyses were performed in SPSS (version 26.0) and R statistical software version 4.0.3 (R Foundation). Differences were considered as significant for P values < 0.05.
Results
Screening for novel candidate genes related to AAD
In our previous studies involving ST experiments of AAD, a spatial cluster gene list was generated for differentially expressed in ST clusters (average logFC > 0.25, P value < 0.05, and only retained positively regulated genes) (Supplemental: Table S1). To identify novel genes related to AAD, we employed the following selection criteria: (1) expression in the artery and the heart, (2) encoding of a secretory protein, (3) association with pathological mechanisms of AAD such as inflammation, cell apoptosis, or vascular homeostasis regulation, and (4) few reported by literature search. Utilizing these criteria, we ultimately selected three candidate genes ADAMTS 8 (encoding ADAMTS8), CD36 (encoding CD36), and PTMA (encoding PTMA) (Fig. 2A).

Selection of candidate proteins related to AAD. (A) Spatial distribution maps of three candidate genes PTMA, CD36 and ADAMTS8 selected by spatial transcriptomics (ST) experiments in each section (n = 6). (B) Cellular composition in ten spots exhibiting the highest gene expression. EC, endothelial cell; Fb, fibroblasts; Mp, macrophages; MSC, mesothelial cell or mesenchymal-stromal cell; NK, natural killer cell; SMC, smooth muscle cell; T, T cells.
Considering the varied expression of ADAMTS8, CD36, and PTMA in different cell types, in order to clarify the cell types with high expression regions of ADAMTS8, CD36, and PTMA, we further analyzed ten spots exhibiting the highest gene expression to assess cellular composition. Combined with the cell marker database24, clusterProfiler tool, and AAD related cell markers, such as VSMC marker α-smooth muscle actin (α-SMA), endothelial cell marker cluster of differentiation 31 (CD31), macrophage marker cluster of differentiation 68 (CD68)25, etc. the cell markers at the sites were identified. This analysis identified several cell types associated with each gene, and the results showed that the cell composition of ADAMTS8, CD36, and PTMA high expression sites mainly included fibroblasts, vascular smooth muscle cells (VSMCs), mesenchymal stromal cells, macrophages, and endothelial cells (Fig. 2B). The above results indicate that ADAMTS8, CD36, and PTMA may participate in the occurrence and development of AAD by regulating the functions of multiple cell types, including VSMCs, fibroblasts, and macrophages.
Validation of candidate proteins in tissues
To confirm the expression levels of the coding proteins ADAMTS8, CD36 and PTMA corresponding to the candidate genes screened above, we utilized aorta tissues from AAD patients for both IHC and Western blot detection. The IHC results of the aorta showed that compared with the healthy control group, the positive staining area and average optical density of PTMA, ADAMTS8, and CD36 in the AAD aorta were significantly increased ( all P < 0.05) (Fig. 3A–D). The Western blot results of the aorta showed that compared with the healthy control group, the relative expression levels of these three candidate proteins in AAD aorta were significantly upregulated ( all P < 0.05) (Fig. 3E, F). These results suggest that PTMA, ADAMTS8 and CD36 are abnormally overexpressed in the aortic wall of AAD lesions, and their expression changes may be closely related to the occurrence and development of AAD.

Validation of candidate proteins related to AAD in aortic tissues. Candidate protein expression was validated by immunohistochemistry (IHC) and Western blot (WB) detection. (A-D) Representative IHC results of PTMA, CD36, and ADAMTS8 in aortic tissues from AAD patients and normal controls respectively. (n = 4/group). Scale bars are 50 µm and 20 µm for the zoom image. (E, F) Representative Western blot images and quantification of PTMA, CD36, ADAMTS8, and GAPDH in AAD tissues and normal aortic tissues (n = 4/group).
Clinical synopsis and proteins distribution in plasma
A total of 302 participants participated were enrolled in this discovery set, comprising 173 AAD cases and 129 controls (Table 1). The mean age of AAD patients was 53.79 ± 10.35 years, which was comparable to the mean age of 53.47 ± 12.45 years in controls (P = 0.808). Men were accounted for 79.8% in AAD patients and for 69.9% in controls (P = 0.052). The AAD patients exhibited significantly higher levels of the independent risk factors including systolic blood pressure (SBP), smoking, hypertension, standing height and d-dimer levels. Subsequently, the circulating levels of PTMA, ADAMTS8, and CD36 were measured in plasma samples from patients with AAD and healthy control subjects. Plasma concentrations of all three candidate proteins were significantly elevated in the AAD group compared with healthy controls. ADAMTS8 levels were elevated at 898.00 pg/mL (median, IQR: 575.50–1241.00) vs. 484.00 pg/mL (median, IQR: 392.00–726.50) (P < 0.0001); CD36 levels were elevated at 17.59 ng/mL (median, IQR: 10.72–24.39) vs. 6.25 ng/mL (median, IQR: 4.54–8.91) (P < 0.0001); and PTMA levels were elevated at 0.76 ng/mL (median, IQR: 0.46–1.28) vs. 0.57 ng/mL (median, IQR: 0.48–0.74) (P = 0.004). (Fig. 4A–C). These results suggest significant differences in the expression of these three candidate molecules in peripheral blood, which can serve as potential molecular markers for AAD diagnosis and prediction.

Exploration of protein distribution in plasma and development of a multi-marker score. (A-C) The expression levels of PTMA, ADAMTS8, and CD36 proteins were significantly higher in AAD patients than in control subjects. ADAMTS8 levels were elevated to 898.00 pg/mL (median, IQR: 575.50 – 1241.00 vs. 484.00 pg/mL (median, IQR: 392.00 – 726.50) in healthy controls (P < 0.0001), CD36 levels were elevated to 17.59 ng/mL (median, IQR: 10.72 – 24.39) vs. 6.25 ng/mL (median, IQR: 4.54 – 8.91) in healthy controls (P < 0.0001), and PTMA levels were elevated to 0.76 ng/mL (median, IQR: 0.46 – 1.28) vs. 0.57 ng/mL (median, IQR: 0.48 – 0.74) in healthy controls (P = 0.004). (D-F) ROC curve analysis of individual proteins: ADAMTS8 (AUC=0.782, 95%CI: 0.733-0.831), CD36 (AUC=0.881, 95%CI: 0.842-0.920), and PTMA (AUC=0.596, 95%CI: 0.527-0.665). (G) PCA plot based on the top two principal components distinguishing AAD group from healthy controls. (H) Selection of five core predictive factors (D-dimer, ADAMTS8, height, SBP and age) based on PCA loading values. (I) Optimal cut-off values of the five core factors for multi-marker score construction: D-dimer ≥ 500 ng/mL, ADAMTS8 ≥ 802.5 pg/mL, height ≥ 166.5 cm, SBP ≥ 140 mmHg, age ≥ 65 years. (J) Multi-marker scores were significantly higher in the AAD patients than in the controls. (K) ROC curve analysis of the multi-marker score for AAD diagnosis (AUC = 0.921, 95%CI: 0.889 - 0.952; sensitivity 77.5%, specificity 96.5%). (L) Restricted cubic spline regression showing the relationship between multi-marker score and AAD events, with exponentially increased AAD risk when the score ≥ 3 points.
Plasma ADAMTS8, CD36 and d-dimer are independent risk factors for AAD
Univariate logistic regression analysis identified that plasma protein markers such as ADAMTS8 and CD36, clinical characteristics such as sex, height, SBP, and smoking history, and laboratory indicators such as white blood cells, d-dimer, and high-density lipoprotein cholesterol (HDL-C) were significantly correlated with the risk of AAD (all P < 0.05). Among these, ADAMTS8 (OR = 6.774, 95% CI 3.421–13.142, P < 0.0001), CD36 (OR = 1.316, 95% CI 1.233–1.405, P < 0.0001), and d-Dimer (OR = 1.011, 95% CI 1.008–1.014, P < 0.0001) were identified as independent risk factors for AAD, whereas HDL-C (OR = 0.042, 95% CI 0.013–0.129, P < 0.0001) was a protective factor. Multivariate logistic regression analysis further demonstrated that after adjustment for potential confounders including sex, SBP, heart rate, smoking history, white blood cell, serum creatinine, and triglycerides, ADAMTS8 (aOR = 4.596, 95% CI 1.250–19.890, P = 0.022), CD36 (aOR = 1.521, 95% CI 1.244–1.860, P < 0.0001), and d-dimer (aOR = 1.013, 95% CI 1.007–1.019, P < 0.0001) remained independent risk factors for AAD. In contrast, HDL-C (aOR = 0.001, 95% CI 0.001–0.028, P = 0.002) remained an independent protective factor. These details were summarized in Table 2.
Diagnostic value of plasma proteins in AAD
Based on the genomic and protein validations related to AAD in tissues and plasma, we aimed to search for identify specific protein combinations as potential diagnostic panels for AAD. To assess the accuracy of the three candidate proteins as diagnostic biomarkers, the ROC analysis was conducted to evaluate their sensitivity and specificity individually. The AUC values were 0.765 (95%CI 0.710–0.819), 0.881 (95%CI 0.842–0.920) and 0.596 (95%CI 0.527–0.666) for ADAMTS8, CD36 and PTMA, respectively (Fig. 4D–F). Candidate proteins with an AUC > 0.7 may be considered as diagnostic biomarkers for AAD.
AAD risk pattern recognition and variable screening
To achieve precise identification of AAD risk patterns and screen for core diagnostic variables, this study integrated molecular markers with significant differential expression at both tissue and plasma levels, and combined key clinical indicators to construct an AAD specific diagnostic model. PCA was performed using independent predictors of AAD validated by logistic regression, including ADAMTS8, d-dimer, and related clinical variables, with varimax orthogonal rotation for component extraction. The results showed that the variance contribution rate of principal component 1 was 83.9%, and that of principal component 2 was 15.7%. The cumulative variance contribution rate of the top two principal components reached 99.6%, indicating that these two components captured 99.6% of the effective information from the original variables and adequately reflect the core risk characteristics of AAD pathogenesis (Supplemental: Fig. 1).
PCA plots based on principal components 1 and 2 can clearly distinguish the AAD group from healthy controls (Fig. 4G). These findings further validate that the PCA model incorporating ADAMTS8, d-dimer, and clinical variables can effectively identify AAD risk patterns, confirming the discriminatory value of the selected key variables for AAD.
Develop multi-marker score for AAD
Based on the two principal component analysis results with a cumulative variance contribution rate of 99.6%, the five core predictive factors with the highest contribution to the AAD risk model were selected according to the PCA load value, including two biomarkers: d-dimer, ADAMTS8, and three clinical variables: height, systolic blood pressure, and age (Fig. 4H). The optimal threshold determined based on clinical diagnosis and treatment guidelines and experimental data is set as follows: d-dimer ≥ 500 ng/mL, ADAMTS8 ≥ 802.5 pg/mL, height ≥ 166.5 cm, SBP ≥ 140 mmHg (according to the diagnostic criteria for hypertension), and age ≥ 65 years old. The total score range of this scoring system is 0–5 points, with higher scores indicating a higher risk of AAD in the research subjects (Fig. 4I).
The multi-marker score was significantly higher in AAD patients than in controls (Fig. 4J). The sensitivity and specificity of multi-marker score for AAD diagnosis were 77.5% and 96.5% with an AUC of 0.921 (95%CI 0.889–0.952) (Fig. 4K). Regression analysis with restricted cubic spline described the relationship between multi-marker score as a continuous variable and AAD events, suggesting that the likelihood of AAD events increased with the multi-marker score, and the risk increased exponentially when the score reached ≥ 3 points (Fig. 4L).
Validation of multi-marker score in validation set
To validate the diagnostic and predictive value of the multi-marker score for AAD, we established an independent validation set comprising 393 participants: 271 patients with acute chest pain (130 AAD cases, 99 AMI cases, and 42 PE cases) and 122 healthy controls. Baseline characteristics are presented in Table 3.
In the first case-control comparison, both ADAMTS8 levels and multi-marker scores were significantly higher in the AAD group than in healthy controls (Fig. 5A, B). For ADAMTS8, the AUC for differentiating AAD from healthy controls was 0.788 (95% CI 0.733–0.842), with a sensitivity of 57.7% and a specificity of 83.6% (Fig. 5C). For the multi-marker score, the AUC was 0.928 (95% CI 0.897–0.959), with a sensitivity of 79.2% and a specificity of 95.1% (Fig. 5D).

Validation of the ADAMTS8 levels and the multi-marker score in the independent validation set. (A, B) ADAMTS8 levels and multi-marker scores were significantly elevated in AAD group compared with healthy controls (ADAMTS8, median [IQR]: 913.33 [733.86, 1067.66] pg/mL vs. 504.03 [394.40, 838.89] pg/mL, P < 0.0001). (C) ROC curve of ADAMTS8 for differentiating AAD from healthy controls (AUC = 0.788, 95% CI: 0.733–0.842). (D) ROC curve analysis of the multi-marker score for discriminating AAD from healthy controls (AUC = 0.928, 95% CI: 0.897–0.959). (E, F) ADAMTS8 levels and multi-marker scores were significantly higher in AAD patients than in non-AAD acute chest pain patients (ADAMTS8, median [IQR]: 913.33 [733.86, 1067.66] pg/mL vs. 626.30 [462.80, 732.34] pg/mL, P < 0.0001). (G) ROC curve of ADAMTS8 for discriminating AAD from non-AAD acute chest pain patients (AUC = 0.788, 95% CI: 0.732–0.843). (H) ROC curve of ADAMTS8 for discriminating AAD from non-AAD acute chest pain patients (AUC = 0.887, 95% CI: 0.848–0.926). (I, J) ADAMTS8 levels and multi-marker scores were significantly higher in the AAD group than in AMI patients. (ADAMTS8, median [IQR]: 913.33 [733.86, 1067.66] pg/mL vs. 504.03 [394.40, 838.89] pg/mL, P < 0.0001). (K, L) For differentiating AAD from AMI, ADAMTS8 had an AUC of 0.803 (95% CI: 0.747–0.859), while the multi-marker score reached an AUC of 0.913 (95% CI: 0.877–0.949). (M, N) ADAMTS8 levels and multi-marker scores were significantly higher in the AAD group than in PE patients. (ADAMTS8, median [IQR]: 913.33 [733.86, 1067.66] pg/mL vs. 660.48 [524.13, 760.44] pg/mL, P < 0.0001). (O, P) For differentiating AAD from PE, ADAMTS8 had an AUC of 0.752 (95% CI: 0.671–0.833), while the multi-marker score reached an AUC of 0.825 (95% CI: 0.756–0.894).
In the second case-control design aimed at distinguishing AAD from non-AAD acute chest pain conditions (AMI and PE), ADAMTS8 levels in AAD patients were 913.33 pg/mL (median, IQR: 733.86–1067.66), which were significantly higher than the 626.30 pg/mL (median, IQR: 462.80–732.34) observed in non-AAD chest pain patients (P < 0.0001) (Fig. 5E). The multi-marker score was also markedly elevated in AAD patients(Fig. 5F). For discriminating AAD from all non-AAD acute chest pain patients, ADAMTS8 yielded an AUC of 0.788 (95% CI 0.732–0.843), with 75.4% sensitivity and 77.3% specificity, whereas the multi-marker score achieved an AUC of 0.887 (95% CI 0.848–0.926), with 79.2% sensitivity and 86.5% specificity (Fig. 5G, H). Further stratified analyses showed that for differentiating AAD from AMI, ADAMTS8 had an AUC of 0.803 (95% CI 0.747–0.859; 73.8% sensitivity, 80.8% specificity), while the multi-marker score reached an AUC of 0.913 (95% CI 0.877–0.949; 79.2% sensitivity, 89.9% specificity) (Fig. 5I–L). For distinguishing AAD from PE, ADAMTS8 exhibited an AUC of 0.752 (95% CI 0.671–0.833; 64.6% sensitivity, 88.1% specificity), and the multi-marker score had an AUC of 0.825 (95% CI 0.756–0.894; 79.2% sensitivity, 78.6% specificity) (Fig. 5M–P). Thus, the multi-marker score exhibited superior overall diagnostic performance in differentiating AAD from other conditions presenting with sudden-onset severe chest pain encountered in the emergency department.
Discussion
In the current study, we identified PTMA, ADAMTS8 and CD36 as genes related to AAD and evaluated cell types in the high expression sites of genes. Compared to the controls, AAD patients showed increased expression of these encoded proteins in the aortic arteries and blood circulation. Through case-control analysis, we demonstrated that elevated SBP, taller standing height and smoking as major epidemiologic risk factors for AAD. We further developed a multi-marker score integrating d-dimer, ADAMTS8, age, height, and SBP. The model was validated in a large independent validation set of 393 subjects, including AAD, AMI, PE, and healthy controls, and showed excellent ability to distinguish AAD not only from healthy individuals but also from non-AAD acute chest pain etiologies. This panel may facilitate early and differential diagnosis of AAD in the emergency setting.
Despite the lethality of AAD, the determinants are still largely unknown. The aortic wall, comprising dynamic cell populations and ECM, responds to biomechanical changes by modulating structure and function, thereby strengthening the aortic wall and meeting hemodynamic demands26. Compromised aortic integrity is a fundamental component of the underlying pathology of AAD. While degeneration mechanisms include progressive SMCs depletion, ECM destruction and inflammation, the precise AAD trigger remains elusive. The ST experiments helped us search for novel genes related to AAD. Finally, PTMA, ADAMTS8 and CD36 were selected as candidate proteins for discriminating AAD from controls.
PTMA is a small, widely distributed acidic nuclear protein with cytoplasmic and extracellular localization under specific physiological or pathological conditions27,28. Studies have shown that the major intracellular role of PTMA is associated with cell proliferation28. Extracellularly, it plays a role in immunomodulation via a pleiotropic mode by stimulating a variety of immune cells28. PTMA is also involved in fibrosis by regulating the expression ECM-related markers and the downstream genes of transforming growth factor beta1 (TGF-β1) pathway29. Relevant studies have further clarified the regulatory role of PTMA in vascular diseases: it has been identified as a key mediator in vascular remodeling during transplant arteriosclerosis, where it modulates estrogen receptor transcriptional activity and promotes cyclin D1‑dependent vascular cell proliferation30. Given that vascular remodeling and abnormal cell proliferation are core pathological features of AAD, the regulatory effect of PTMA on vascular cell proliferation and intimal hyperplasia, as reported in the literature, strongly suggests its potential involvement in aortic wall remodeling and AAD progression, which is consistent with our findings that PTMA is abnormally overexpressed in AAD tissues and plasma.
CD36 is a scavenger receptor densely expressed on the surface of macrophages. Its role in immunity, metabolism and atherosclerosis has been widely studied. CD36 mediates oxidized low-density lipoprotein uptake leading to foam cell formation and inhibits macrophage migration that promotes the trapping of lipid-laden macrophages in the arterial intima31. Emerging evidence also indicates that CD36 drives fatty acid-induced ferroptosis in CD4+ T cells in acute type A AD, leading to immune dysfunction and vascular inflammation, excessive reactive oxygen species accumulation, and vascular inflammation32. Combined with our findings that CD36 is significantly upregulated in AAD tissues and plasma, and its loss can inhibit VSMC proliferation and regulate contractile protein expression, these literature-based mechanistic insights further confirm that CD36 participates in AAD pathogenesis by linking metabolic disturbance, immune dysregulation, and vascular structural instability. CD36 may contribute to aortic aneurysm development by affecting fatty acid transport and adventitia degradation in the aortic wall. The loss of CD36 has been proven to significantly inhibit VSMC proliferation, increase the expression of TGF-β1 and the contractile proteins including calponin 1 and smooth muscle α actin33. These observations collectively suggest that CD36 links metabolic disturbance, immune dysregulation, and structural instability in AAD.
ADAMTS family members, including ADAMTS8, are crucial in vascular homeostasis and vasculopathy, influencing cell proliferation, adhesion, migration and signaling34,35,36. ADAMTS8 is proven to increase SMC proliferation and degrade proteoglycans to promote ECM remodeling37. It also induces endothelial dysfunction and matrix metalloproteinase activation in an autocrine/paracrine manner34. In line with our present findings in AAD, Levula et al. 38 demonstrated that ADAMTS8 expression was significantly higher in ascending AD tissues than in aortic aneurysm (AA) tissues, accompanied by prominent medial inflammation and active vascular remodeling. Similarly, Duma et al.39 reported that ADAMTS8 expression was markedly elevated in the aneurysmal sac of abdominal aortic aneurysm (AAA) compared with non-aneurysmal border segments, supporting a role for ADAMTS8 in localized pathological matrix degradation40. However, a study focused on macrophage transcriptomics and plasma proteomics in AAA patients, found a slight reduction in ADAMTS8 (ratio 0.9) in macrophages and plasma relative to peripheral arterial occlusion controls41. This discrepancy may reflect differences in disease subtype (AAD vs. AAA), sample source (tissue vs. macrophage vs. plasma), disease stage, or cellular origin. Moreover, the latest genome-wide association study based on the Million Veteran Program suggests ADAMTS8 may be a putative causal gene for AAD42. Although the exact pathogenic mechanisms of these proteins in AAD are not fully understood, their roles in ECM remodeling and cellular function indicate their potential significance in AAD pathogenesis34. Despite variable expression patterns across studies, dysregulated ADAMTS8 whether upregulated or downregulated consistently disrupts ECM homeostasis and compromises aortic wall stability, a core pathological mechanism shared by both aortic dissection and aneurysm. Collectively, our results and existing clinical evidence strongly support that ADAMTS8 is closely implicated in the pathogenesis of AAD. Given the heterogeneous expression profiles and limited mechanistic insights, ADAMTS8 represents a biologically relevant and valuable target for further in-depth investigation in aortic diseases.
When focusing on the dynamics of aortic cells, SMCs are the primary component of the aortic wall and play a central role in maintaining aortic functions and homeostasis26. Other cell types including endothelial cells, fibroblasts and myofibroblasts also play vital roles in maintaining the structure and integrity of the aortic wall. Additionally, various inflammatory cells, such as lymphocytes, macrophages, mast cells and neutrophils, actively participate in tissue injury, repair and remodeling43,44. In our study, the analysis of cell composition at high expression positions of related genes revealed that the cell types at these positions were concentrated in fibroblasts, SMCs, mesenchymal–stromal cells, macrophages and endothelial cells. These results are consistent with the identified cellular roles in AAD pathogenesis and support the potential of the three candidate proteins as pathogenic molecules in AAD. Despite advancements in understanding the dynamics of cell populations and ECM remodeling in aortic physiology and pathology, the specific trigger of aortic dissection remains elusive. Future research efforts are needed to determine whether these three molecules are pathogenic and to elucidate their mechanisms of action.
As highlighted in demographic studies, approximately 65% of AAD patients are male, with the condition most commonly occurring in their seventies (mean age 63 years)10,45,46. While African American patients with AAD tend to be younger (mean age 54.6 ± 12.8 years) compared to white individuals (mean age 64.2 ± 15.2 years; P < 0.001), and are more likely to have histories of cocaine abuse, hypertension and diabetes47. This is consistent with our case-control analysis, in which AAD patients presented at a relatively younger age and exhibited a high prevalence of hypertension. Women are less frequently affected by AAD, comprising about 32% of all patients in the IRAD48. Observational studies have identified smoking, hyperlipidemia, hypertension and standing height as independent risk factors for AAD development. In observational studies, smoking, hyperlipidemia, hypertension and standing height have been suggested as independent risk factors associated with the development of AAD42,49. In our case-control, AAD patients demonstrated higher standing heights and SBP, and a greater prevalence of smoking and hypertension compared to controls. Univariate analysis also indicated that hypertension, smoking, standing height and SBP are associated with an increased risk of AAD, which is consistent with the epidemiologic literature42,50.
d-dimer is a degradation product of crosslinked fibrin and a well-established biomarker of coagulation and fibrinolysis51. Elevated d-dimer may play an important role in the formation and development of various cardiovascular diseases, especially in pulmonary embolism disease. Multiple studies have shown that exposure of tissue factors in the arterial smooth muscle layer of AAD patients activates exogenous coagulation pathways and increases blood d-dimer levels52. Therefore, d-dimer also plays an important role in the diagnosis of aortic dissection. Given the complexity of AAD pathophysiology, single biomarkers are insufficient for reliable diagnosis. We therefore constructed a multi-marker score combining d-dimer, ADAMTS8, age, height, and SBP. In an independent validation set of 393 participants, this score achieved an AUC of 0.928 for distinguishing AAD from healthy controls, which was significantly superior to the single biomarker ADAMTS8 (AUC = 0.788), confirming the stability and reproducibility of the model and ruling out accidental results. More importantly, the three life-threatening acute chest pain conditions (AAD, AMI, and PE) have highly similar clinical symptoms, leading to high misdiagnosis rates in emergency settings. Our multi-marker score exhibited excellent performance in differentiating AAD from other acute chest pain etiologies, with an AUC of 0.887 for distinguishing AAD from all non-AAD chest pain patients. Specifically, it achieved an AUC of 0.913 for differentiating AAD from AMI and 0.825 for distinguishing AAD from PE. Although ADAMTS8 itself had a certain discriminatory ability, the combined score significantly improved diagnostic efficacy, which is of great practical significance for rapid triage in the emergency department and avoiding fatal misdiagnosis. The superiority of the multi-marker score over single indicators lies in the fact that single biomarkers such as ADAMTS8 have limited specificity and sensitivity in complex chest pain etiologies, while the combination of molecular biomarkers and clinical risk factors comprehensively captures the multi-faceted pathophysiological characteristics of AAD, resulting in a substantial improvement in AUC and stable performance in the independent validation set, indicating strong robustness of the model.
A prospective population-based study revealed that only 67.3% of the patients were on antihypertensive medication during the 5 years prior to dissection. Proportion analysis of blood pressure data showed that 61.9% of subsequent blood pressure readings were > 140/90 mmHg, despite most patients receiving combined antihypertensive therapy53,54. Various risk factors have been shown to predispose the aorta to become fragile to increase the risk of AAD. Mechanistically, factors such as older age, dyslipidemia, elevated apolipoprotein levels and arterial hypertension can accelerate atherosclerotic degeneration of the aorta. This degeneration manifests as intimal thickening, fibrosis, calcification, extracellular fatty acid deposition and ECM degradation, all of which impair the aortic wall’s elasticity, leading to aortic wall fragility55,56. Hypertension also exerts increased pressure on the aortic wall, potentially initiating an intimal tear. It may further stimulate the production of pro-inflammatory cytokines and matrix metalloproteinases, leading to excessive ECM degradation56.
Collectively, our findings demonstrate that this multi-marker score, validated in a large independent validation set, enables early and differential diagnosis of AAD and supports timely referral, surgical intervention, or emergency operation. Its ability to distinguish AAD from AMI and PE is particularly valuable in acute care settings. Key strengths of this study include the identification of novel AAD-associated biomarkers (PTMA, CD36, and ADAMTS8), a two-stage design involving model development in a discovery set and rigorous validation in a large independent validation set, excellent performance in differentiating AAD from other life-threatening causes of chest pain, and potential for rapid triage in the emergency department. Further investigation into molecular mechanisms and prospective multicenter studies will help optimize clinical therapeutic strategies and improve patient outcomes.
Study limitations
This study has several limitations. First, all samples were from two hospitals, but both located in the same region, which may limit the generalizability of our findings. Expanded sample sizes and multi-regional, multi-center study designs are needed to improve statistical power and external validity and to further confirm the diagnostic reliability of our model. Second, although we validated our multi-marker score in a large independent set of 393 subjects, including patients with AAD, AMI, PE, and healthy controls, which strengthened its reliability and clinical applicability, the overall sample size still restricted in-depth subgroup analyses, especially among patients with complex comorbidities. Further multi-center prospective cohorts are therefore required to improve the applicability and robustness of this scoring system. Third, the potential value and biological roles of other candidate biomarkers not included in our diagnostic panel should not be overlooked. In particular, further mechanistic studies, including functional assays and animal models, are needed to clarify the causal roles of PTMA, CD36, and ADAMTS8 in the pathogenesis of AAD. Fourth, protein quantification may vary across different analytical platforms, which could influence the stability of the proposed cutoff values. Targeted proteomic assays may be utilized to improve measurement precision in future investigations. Finally, clinical imaging remains the gold standard for AAD diagnosis, and our scoring model should be used as an adjunctive tool rather than a replacement. Currently, we have designed a multi-center prospective study that is under registration, to further validate the model in diverse populations.
Conclusions
We identified PTMA, ADAMTS8, and CD36 as novel biomarkers associated with AAD. We developed and validated a five-biomarker risk score that can effectively distinguish AAD patients from healthy controls. More importantly, this multi-marker score shows excellent performance in the differential diagnosis of life-threatening acute chest pain syndromes, including AAD, AMI, and PE. It represents a rapid, sensitive, and cost-effective auxiliary tool for early risk stratification and timely triage in the emergency department. Our findings may provide evidence-based insights for early identification, accurate diagnosis, and optimized clinical management of AAD.
Data availability
All supporting data are included within the main article and its supplementary files.
Abbreviations
- AAD:
-
Acute aortic dissection
- ADAMTS8:
-
A disintegrin and metalloproteinase with thrombospondin motifs 8
- AUC:
-
Area under the curve
- AMI:
-
Acute myocardial infarction
- α-SMA:
-
α-smooth muscle actin
- CD31:
-
Cluster of differentiation 31
- CD68:
-
Cluster of differentiation 68
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- ECM:
-
Extracellular matrix proteins
- GAPDH:
-
Glyceraldehyde-3-phosphate dehydrogenase
- HCL:
-
Human cell landscape
- IHC:
-
Immunohistochemical
- IOD:
-
Integrated optical density
- MRI:
-
Magnetic resonance imaging
- OR:
-
Odds ratio
- PCA:
-
Principal component analysis
- PE:
-
Pulmonary embolism patients
- PTMA:
-
Prothymosinα
- ROC:
-
Receiver operating characteristic
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- SDS-PAGE:
-
Standard sodium dodecyl sulfate polyacrylamide gel electrophoresis
- SMCs:
-
Smooth muscle cells
- ST:
-
Spatial transcriptomics
- TGF-β1:
-
Transforming growth factor beta1
- VSMCs:
-
Vascular smooth muscle cells
References
Hagan, P. G. et al. The international registry of acute aortic dissection (irad): new insights into an old disease. JAMA 283, 897–903 (2000).
Howard, D., Sideso, E., Handa, A. & Rothwell, P. Incidence, risk factors, outcome and projected future burden of acute aortic dissection. Annals Cardiothorac. Surg. 3, 278–284 (2014).
Bossone, E. & Eagle, K. Epidemiology and management of aortic disease: aortic aneurysms and acute aortic syndromes. Nat. Rev. Cardiol. 18, 331–348 (2021).
Hagan, P. et al. The international registry of acute aortic dissection (irad): new insights into an old disease. JAMA 283, 897–903 (2000).
Elsayed, R., Cohen, R., Fleischman, F. & Bowdish, M. Acute type a aortic dissection. Cardiol. Clin. 35, 331–345 (2017).
Nienaber, C. et al. Aortic dissection. Nat. Rev. Dis. Primers. 2, 16053 (2016).
Isselbacher, E. et al. 2022 acc/aha guideline for the diagnosis and management of aortic disease: a report of the american heart association/american college of cardiology joint committee on clinical practice guidelines. Circulation 146, e334–e482 (2022).
Wang, Y. et al. Magnitude of soluble st2 as a novel biomarker for acute aortic dissection. Circulation 137, 259–269 (2018).
Zhang, H. et al. The potential value of the neutrophil to lymphocyte ratio for early differential diagnosis and prognosis assessment in patients with aortic dissection. Clin. Biochem. 97, 41–47 (2021).
Erbel, R. et al. 2014 esc guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the european society of cardiology (esc). Eur. Heart J. 35, 2873–2926 (2014).
Zeng, T. et al. Cytokines in aortic dissection. Clin. Chim. Acta. 486, 177–182 (2018).
Li, Y. et al. Single-cell transcriptome analysis reveals dynamic cell populations and differential gene expression patterns in control and aneurysmal human aortic tissue. Circulation 142, 1374–1388 (2020).
Asha, S. & Miers, J. A systematic review and meta-analysis of d-dimer as a rule-out test for suspected acute aortic dissection. Ann. Emerg. Med. 66, 368–378 (2015).
Suzuki, T. et al. Diagnosis of acute aortic dissection by d-dimer: the international registry of acute aortic dissection substudy on biomarkers (irad-bio) experience. Circulation 119, 2702–2707 (2009).
Singh, K. et al. Intra- and interobserver variability in the measurements of abdominal aortic and common iliac artery diameter with computed tomography. The tromsø study. Eur. J. Vasc. Endovasc. Surg. 25, 399–407 (2003).
Ranasinghe, A. & Bonser, R. Biomarkers in acute aortic dissection and other aortic syndromes. J. Am. Coll. Cardiol. 56, 1535–1541 (2010).
Hao, X., Cheng, S., Jiang, B. & Xin, S. Applying multi-omics techniques to the discovery of biomarkers for acute aortic dissection. Front. Cardiovasc. Med. 9, 961991 (2022).
Li, Y. et al. Visualization and analysis of gene expression in stanford type a aortic dissection tissue section by spatial transcriptomics. Front. Genet. 12, 698124 (2021).
Butler, A., Hoffman, P., Smibert, P., Papalexi, E. & Satija, R. Integrating single-cell transcriptomic data across different conditions, technologies, and species. Nat. Biotechnol. 36, 411–420 (2018).
Zhang, X. et al. Cellmarker: a manually curated resource of cell markers in human and mouse. Nucleic Acids Res. 47, D721–D728 (2019).
Yu, G., Wang, L., Han, Y. & He, Q. Clusterprofiler: an r package for comparing biological themes among gene clusters. Omics: J. Integr. biology. 16, 284–287 (2012).
Peiman, N. et al. Diagnostic accuracy of the aortic dissection detection risk score plus d-dimer for acute aortic syndromes: the advised prospective multicenter study. Circulation 137, 250–258 (2017).
Chukwu, M. et al. Acute stanford type a aortic dissection: a review of risk factors and outcomes. Cureus 15, e36301 (2023).
Ibrahim, A. & Christoph, A. N. Prediction of aortic dissection. Heart ;106 870–871 (2020).
Yanming, L. et al. Single-cell transcriptome analysis reveals dynamic cell populations and differential gene expression patterns in control and aneurysmal human aortic tissue. Circulation, 142 1374–1388 (2020).
Shen, Y. et al. Aortic aneurysms and dissections series. Arterioscler. Thromb. Vasc. Biol. 40, e37–e46 (2020).
Kijogi, C. et al. Subcellular dissemination of prothymosin alpha at normal physiology: immunohistochemical vis-a-vis western blotting perspective. BMC Physiol. 16, 2 (2016).
Kumar, A. et al. Overexpression of prothymosin-α in glioma is associated with tumor aggressiveness and poor prognosis. Bioscience reports ;42 BSR20212685 (2022).
Wang, J. et al. Ptma, a new identified autoantigen for oral submucous fibrosis, regulates oral submucous fibroblast proliferation and extracellular matrix. Oncotarget 8, 74806–74819 (2017).
Simone, A. J. et al. Genetic profiling of aortic allografts: prothymosin alpha as potential target? Transpl Int ;181010–1015 (2005).
Chen, Y. et al. Mitochondrial metabolic reprogramming by cd36 signaling drives macrophage inflammatory responses. Circul. Res. 125, 1087–1102 (2019).
Hui, L. et al. Cd36-mediated ferroptosis destabilizes cd4(+) t cell homeostasis in acute stanford type-a aortic dissection. Cell Death Dis ;15 669 (2024).
Yue, H. et al. Cd36 enhances vascular smooth muscle cell proliferation and development of neointimal hyperplasia. Arterioscler. Thromb. Vasc. Biol. 39, 263–275 (2019).
Omura, J. et al. Adamts8 promotes the development of pulmonary arterial hypertension and right ventricular failure: a possible novel therapeutic target. Circul. Res. 125, 884–906 (2019).
Chelladurai, P., Seeger, W. & Pullamsetti, S. Matrix metalloproteinases and their inhibitors in pulmonary hypertension. Eur. Respir. J. 40, 766–782 (2012).
Rodríguez-Manzaneque, J., Fernández-Rodríguez, R., Rodríguez-Baena, F. & Iruela-Arispe, M. Adamts proteases in vascular biology. Matrix Biol. J. Int. Soc. Matrix Biol. 44 38–45 (2015).
Collins-Racie, L. et al. Adamts-8 exhibits aggrecanase activity and is expressed in human articular cartilage. Matrix biology: J. Int. Soc. Matrix Biology. 23, 219–230 (2004).
Mari, L. et al. A disintegrin and metalloprotease – 8 and – 15 and susceptibility for ascending aortic dissection. Scand J. Clin. Lab. Invest ;71 515–522 (2011).
Aleksandra, A-D. et al. Expression gradient of metalloproteinases and their inhibitors from proximal to distal segments of abdominal aortic aneurysm. J Appl. Genet ;62 499–506 (2021).
Kurt, F. et al. Alterations in phenotype and gene expression of adult human aneurysmal smooth muscle cells by exogenous nitric oxide. Exp Cell. Res ;384 111589 (2019).
Nicolas, L. et al. Profile of macrophages in human abdominal aortic aneurysms: A transcriptomic, proteomic, and antibody protein array study. J Proteome Res ;9 3720–3729 (2010).
Klarin, D. et al. Genome-wide association study of thoracic aortic aneurysm and dissection in the million veteran program. Nat. Genet. 55, 1106–1115 (2023).
Dale, M., Ruhlman, M. & Baxter, B. Inflammatory cell phenotypes in aaas: their role and potential as targets for therapy. Arterioscler. Thromb. Vasc. Biol. 35, 1746–1755 (2015).
Piacentini, L. et al. Genome-wide expression profiling unveils autoimmune response signatures in the perivascular adipose tissue of abdominal aortic aneurysm. Arterioscler. Thromb. Vasc. Biol. 39, 237–249 (2019).
Evangelista, A. et al. Insights from the international registry of acute aortic dissection: a 20-year experience of collaborative clinical research. Circulation 137, 1846–1860 (2018).
Mussa, F. et al. Acute aortic dissection and intramural hematoma: a systematic review. JAMA 316, 754–763 (2016).
Bossone, E. et al. Acute aortic dissection in blacks: insights from the international registry of acute aortic dissection. Am. J. Med. 126, 909–915 (2013).
Nienaber, C. et al. Gender-related differences in acute aortic dissection. Circulation 109, 3014–3021 (2004).
Isselbacher, E. Thoracic and abdominal aortic aneurysms. Circulation 111, 816–828 (2005).
Pape, L. et al. Aortic diameter > or = 5.5 cm is not a good predictor of type a aortic dissection: observations from the international registry of acute aortic dissection (irad). Circulation 116, 1120–1127 (2007).
Deli, W. et al. The diagnostic and prognostic value of d-dimer in different types of aortic dissection. J Cardiothorac. Surg ;17 194 (2022).
Zexiang, X. et al. Changes of serum d-dimer, nt-probnp, and troponin i levels in patients with acute aortic dissection and the clinical significance. Evid Based Complement Alternat Med 2022 (2022).
Zhou, Z., Cecchi, A., Prakash, S. & Milewicz, D. Risk factors for thoracic aortic dissection. Genes 13 1814 (2022).
Howard, D. et al. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the oxford vascular study. Circulation 127, 2031–2037 (2013).
Landenhed, M. et al. Risk profiles for aortic dissection and ruptured or surgically treated aneurysms: a prospective cohort study. J. Am. Heart Association. 4, e001513 (2015).
Yin, H. & Pickering, J. Cellular senescence and vascular disease: novel routes to better understanding and therapy. Can. J. Cardiol. 32, 612–623 (2016).
Acknowledgements
The authors sincerely thank the Key Laboratory of Cardiovascular Disease Research of the First Affiliated Hospital of Xinjiang Medical University and the Department of Medical Research and Translational Management of the People’s Hospital of Xinjiang Uygur Autonomous Region for providing excellent experimental platforms for this study.
Funding
This study was supported by National Natural Science Foundation of China [grant number 82570503], Natural Science Foundation of Xinjiang Uygur Autonomous Region [grant number 2022D01D22], Natural Science Foundation of Xinjiang Uygur Autonomous Region [grant number 2024D01C108], Tianchi Talent Cultivation Program Project of Xinjiang Uygur Autonomous Region [2025013], and Youth Project of Medicine and Technology of Health Commission of Xinjiang Uygur Autonomous Region [WJWY-201419].
Author information
Authors and Affiliations
Contributions
All authors made a significant contribution to the work reported. TT and LZ designed project, performed the experiments and wrote manuscript. TT, LZ, XXT and QZ (Qiang Zhao) prepared and analyzed patient datasets and clinical samples. QZ (Qian Zha), FL, JL and YL contributed through data curation and revising the manuscript. XL and YY designed project, edit manuscript and supervised the project. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
41598_2026_51121_MOESM2_ESM.tiff (download TIFF )
Supplementary Material 2. Figure S1. Determination of PCA models and composition of each PCA component. (A) Based on the scree plot, the first two principal components were retained. The contribution of the first two principal components to the total variance was 83.9% and 15.7%, respectively, and together they explained approximately 99.6% of the total cumulative variance. (B, C) Contribution of each variable to the first two principal components (Dim-1, Dim-2): candidate proteins (CD36, ADAMTS8, PTMA) and clinical risk factors or laboratory indicators showed different contribution degrees, with ADAMTS8 and D-dimer having the highest contribution to Dim-1 and Dim-2.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tian, T., Zhao, L., Tian, X. et al. A d-dimer and ADAMTS8 based multi-marker score for the diagnosis of acute aortic dissection. Sci Rep 16, 14679 (2026). https://doi.org/10.1038/s41598-026-51121-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-51121-w
