
Abstract
This paper examines the recently formed Movement for Change and Social Justice (MCSJ) in the township of Gugulethu, in Cape Town, South Africa. MCSJ is a health and social justice movement that has an unusual trajectory—guided by the political principles and strategies of South Africa AIDS activism, inspired but also frustrated by the contemporary progressive public health activism, and catalysed by a university research partnership at the University of Cape Town (UCT) that focused on innovative ways of using health information to spur community and health system action to respond to issues of men, masculinity and HIV.
This paper synthesises findings from participant observation, qualitative process evaluations of MCSJ’s work, and reflections from the UCT-based research team to develop a number of lessons about the challenges and opportunities in efforts to foster a healthy public for men and HIV. MCSJ’s approach builds on current modes and models of public health thinking while also pushing for more responsive, more inclusive, more sustained, and more locally rooted forms of practice. The paper identifies a range of enabling conditions for MCSJ’s work, describes the often delicate balancing act MCSJ has to manage in its work, and outlines some of the key strategies of this community–university partnerships that guided efforts to develop a healthy public for men and HIV. Lessons learned from this case study will be helpful for other efforts to promote and sustain engaged and impactful university–community collaborations to support the emergence of healthy publics.
Similar content being viewed by others

Introduction: fostering healthy publics to address men and HIV
In the last few years, global public health discourse and action has begun to focus attention on the problem of men and HIV. While the global majority of the HIV prevalence burden—as well as the HIV care burden—falls on women, men generally do worse than women in most aspects of HIV prevention, treatment and care (Auld et al., 2015; Cornell et al., 2017; Tsai and Siedner, 2015; Lurie et al., 2019). In 2017, UNAIDS published ‘Blind Spot—Reaching Out to Men and Boys’ (2017), a milestone report on the HIV-related challenges facing men and boys around the world. In the following year, the MenStar Coalition was announced at the International AIDS Conference in Amsterdam with the goal of focusing funding, research and intervention to better support men in HIV prevention and treatment (MenStar Coalition, 2018). While this new focus on men includes men who have sex with men (MSM), it extends beyond this well-identified category to include all men, but with a prominent focus on the preventable HIV burden among heterosexual men in sub-Saharan Africa. A cascade of further policy development, funding, research and advocacy around this issue is continuing to build at both local and global levels.
Despite the recency of these prominent global health developments, the public health challenge of men and HIV is not a new or an unknown problem. Evidence of men’s poor outcomes along the HIV treatment cascade has been available for years—from prevention and testing, to treatment initiation and viral suppression, men not only fare worse than women, but also far worse than they have to (UNAIDS, 2017). Research has described a range of factors driving this preventable and inequitable HIV burden among men, including masculine gender norms, the gendered structure of labour and economic contexts, and the ways in which the design and delivery of the health services themselves can present numerous barriers to men’s access (Colvin, 2019).
A small group of public health researchers and activists have been writing about this issue for a number of years (Cornell, 2013; Cornell et al., 2015; Higgins et al., 2010; Barker et al., 2010), although without gaining obvious traction. For reasons that are both beyond the scope of this article as well as still unclear, the problem of men and HIV is now, however, starting to gain both considerable attention and tangible resources. For those interested in fostering the engagement of political, academic and community actors around this issue, there is now a real opportunity to do so.
But there are also significant questions around how best to go about these efforts. How should we frame the ‘problem’ of men and HIV so that we can recruit those who might be sceptical of focusing on a group that enjoys significant gendered social power and is often framed as perpetrators of violence and the source of many social problems? How might we avoid an approach that blames individual men for their poor health and HIV outcomes and expects them to work on their own to overcome the powerful social and structural drivers behind these outcomes? How might researchers engage with key community, professional and political actors around the question of men and HIV in ways that promote a more coordinated and effective response that is also consistent with feminist and human rights principles? In the terms of the article that inspired this special collection (Hinchliffe et al., 2018), how might we as researchers support the development of a ‘healthy public’ engaged in new ways of thinking about and addressing the problem of men and HIV?
These questions about how to foster healthy publics operate—and may look different—at different scales, from the global political and policy spheres, to national governments and issues of citizen and scientific engagement, down to local communities, activists, academics and healthcare staff working at the ‘coalface’ of public health challenges. This paper examines a local-level effort in Cape Town, South Africa to foster the growth of a healthy public in relation to men and HIV. It describes the emergence of the Movement for Change and Social Justice (MCSJ) in one community in Cape Town as part of that effort and reviews some of the lessons learned about what is required to create and sustain an impactful public response to inequities in men’s experiences and outcomes in HIV care.
iALARM: using information to catalyse coordination and mobilisation for a healthy public
The work of MCSJ is closely linked to a 5-year, NIH-funded research project on men and HIV based at the University of Cape Town (UCT) and partnering with Brown University called ‘iALARM: using information to align services and link and retain men in the HIV cascade’. The iALARM project and MCSJ are closely interconnected and each has played a distinct role in the process of promoting a healthy public around men and HIV.
Most of the iALARM research project staff are based in the Division of Social and Behavioural Sciences (DSBS) at UCT’s School of Public Health and Family Medicine. Its field research site is in Gugulethu, a peri-urban township community in Cape Town of about 100,000 people (Stats, 2011). iALARM’s original focus was on using novel forms of health information to improve the alignment and coordination of services between the NY3 Clinic (a local public primary care clinic) and the Men’s Wellness Centre, an initiative run on the clinic grounds by Sonke Gender Justice, a prominent South African gender, health and human rights non-governmental organisation (NGO). iALARM’s core intervention was the creation of a ‘Linkage and Retention in Care Task Team’, also known as the iALARM Task Team, composed of local clinic and NGO staff. The iALARM Task Team meets regularly to review key health information and academic research about men and HIV in the area and use this information to identify service gaps and transmission hotspots and develop better ways of designing, coordinating and delivering services for men attending the clinic and Men’s Wellness Centre.
Soon after the start of the project, though, we realised our original focus on one clinic and one NGO project was too narrow, and we expanded iALARM’s scope to include the broader surrounding community of Gugulethu, as well as the encompassing health sub-district of Klipfontein (of which Gugulethu is part). This brought a broader group of stakeholders into the iALARM Task Team, including staff and managers from other health facilities and from the local government’s sub-district offices, as well as representatives from several local NGOs and community structures. The NGOs involved included ones focusing on child and adolescent wellness, youth sports, parenting and community health, food security, disability, and more. In addition to setting up the Task Team, the initial stages of iALARM also included a retrospective cohort study to better understand how well men were performing in the HIV cascade in Klipfontein (Lurie et al., 2019), as well as formative qualitative research to better understand the local factors shaping men’s engagement in HIV services (Colvin et al., 2018). Once the Task Team meetings were under steam, we also began conducting qualitative and quantitative process evaluations to understand how local actors engaged with and made use of health information (van Pinxteren, 2020).
In some respects, iALARM is designed as a fairly conventional research project supported by mainstream research funding (the NIH in the US, the South African Medical Research Council, and the National Research Foundation in South Africa). It includes quantitative and qualitative studies run by academic researchers and their postgraduate students designed to establish and then evaluate a new intervention to address a well-defined health problem. At this level, iALARM does not really challenge the kind of established—and often limiting—methods for conducting and using public health research described by Hinchliffe et al. (2018) in their framing piece for this collection.
In other ways, though, iALARM has some unique design features that are important for understanding how it helped lay the foundation for the development of MCSJ and a different kind of healthy public for men and HIV. The first element is the fact that the Task Team is intentionally designed to bring people together from across different levels, and from both the health system and community contexts. The Task Team aims to foster new kinds of interactions and relationships both horizontally (between the health system and community organisations) as well as vertically across levels of social and organisational hierarchy (e.g. by including community members, community health workers and NGO volunteers as well as health system managers, NGO directors, and local political and opinion leaders). Both kinds of engagement—across the health system–community divide and across the hierarchies within each—are unusual in this context.
Another unique and, for this case study, critical feature of iALARM is the fact that the ‘intervention’ being developed and evaluated was simply the creation of the iALARM Task Team and the engagement that followed. We did not have a specific biomedical, behavioural or structural intervention for men and HIV in mind. We essentially set out to host a regular meeting for a group of interested actors, prime their deliberations with locally relevant health information about men and HIV, and then see what happened. We of course hoped that through these engagements, health system and community actors would reflect critically on their services, and find ways of better refining, redirecting and coordinating their efforts. But exactly what direction these discussions and new practices took was left entirely open at the start of the project.
A final element of iALARM’s success has been its ability to recruit staff on to the project who have deep knowledge about and relationships within the local context. These staff understand the social and cultural contexts and complexities in Gugulethu and have been able to engage, recruit and mobilise from within both the community and health system. Mandla Majola, hired initially as iALARM’s ‘community engagement coordinator’ was born in Gugulethu, worked for many years in the Treatment Action Campaign (TAC) as an AIDS activist, and has led the effort to grow and sustain the iALARM Task Team. He also became a key figure in the founding and development of MCSJ.
The rest of this paper charts the birth and growth of MCSJ and considers some of the lessons learned in MCSJ’s efforts to engage a healthy public around the issue of men and HIV in Gugulethu. The reflections in this case study are synthesised from the findings of several sub-studies within iALARM—including the primary qualitative process evaluation of the Task Team and MCSJ led by Myrna van Pinxteren as part of her Ph.D. (Pinxteren, 2020) and a number of Masters-level research projects on MCSJ’s work—as well as participant-observation and numerous, ongoing discussions within the broader research team about MCSJ and its work. All research was approved by the UCT’s Faculty of Health Sciences Human Research Ethics Committee (#802/2014) and informed consent was obtained from all participants.
Birth and growth of MCSJ
Exactly how MCSJ started, who started it, and how MCSJ is related to iALARM has been the subject of some (friendly) debate among those involved. There is a consensus that MCSJ is organised as a network of actors interested in urgent public health issues in Gugulethu. It is deliberately not aligned to any political party but it does have a relatively coherent, progressive political perspective. Its membership includes local NGOs, UCT’s DSBS, and Sonke Gender Justice. It does not have formal health system representatives in its membership but MCSJ is a regular participant in iALARM Task Team meetings that include health system staff. Individual MCSJ staff also have close connections with key figures in the local health system. Mandla Majola’s role in MCSJ has been critical but also complex. He was and remains a full-time UCT staff member on the iALARM project but is often identified as the founder of MCSJ (a status he sometimes reluctantly acknowledges) and spends much of his time working on MCSJ initiatives. UCT as an organisation is also in an unusual—and sometimes complicated—role of being both a founding member and active contributor to the network (a presumed equal among many other groups) as well as a funder and researcher of the network’s activities (which in turn puts it in a unique position).
While the idea of developing some kind of local health activist network had been discussed by various people involved in iALARM research team and Task Team, and the Gugulethu community more broadly, the moment that catalysed the establishment of the movement was an appeal from one of Mandla’s childhood acquaintances. He was living with epilepsy and was unable, over the course of several days, to obtain the medication he needed from the pharmacy at a local ‘day hospital’ (large public clinic). Mandla collected the relevant information from his acquaintance, discussed the situation with fellow activists and NGOs in the area, and then set up a meeting with the local facility manager, also a friend from childhood. Though the facility manager acknowledged the struggles within the pharmacy service to provide a consistent service, he was surprised that this patient, whom he knew, had had to wait several days before getting his medication. Mandla, other activists, and the facility manager sat down with a higher-level manager within the sub-district and lobbied for an extra pharmacist for the day hospital. In the end, they were successful (in the short term, at least) in getting an extra pharmacist in the facility and helping this man access the medication he required. That marked the beginning of what would become MCSJ.
Most of MCSJ’s activities have been organised around ‘campaigns’ that have taken a similar form to that described above. A local and urgent health or social problem is brought to the attention of MCSJ members (often through social or organisational networks), and they then gather the relevant information, consult with local stakeholders and activists, engage with the relevant public services and political authorities, and then advocate for a workable solution. Once a campaign is deemed successful, MCSJ moves on to the next identified problem. Subsequent campaigns have focused on improving: the local dental services at the NY3 Clinic, ARV delays and stockouts at the day hospital, condom distribution in local high schools, public understanding of the local emergency room’s (ER) triage system and human resource constraints, safety and security at this same ER, safety at a local primary school, and gender-based violence (GBV).
Not all of these campaigns have been as seemingly easy, successful or sustainable as the pharmacy service campaign but MCSJ has been credited with bringing about significant improvements in the public services in Gugulethu. Their approach almost always starts with careful collection of information (sometimes in the form of a community-driven audit, gathering testimonies, or similar techniques), strategic networking among other local stakeholders, and an initial collaborative and supportive approach to the public sector management. MCSJ members are clear, though, that they are focused on pushing the state to fulfil its obligations and are careful not to be co-opted into providing such services themselves. They have escalated their approach when necessary to larger public protests and other campaigns to put pressure on local authorities. Throughout these efforts, they are also careful to maintain a distinction between the broader state’s abstract responsibility to fulfil its human rights obligations, and the bureaucratic dilemmas and resource constraints that most managers and civil servants face working on the frontline.
Though MCSJ’s approach has generally been to be responsive to locally expressed needs, rather than develop its own specialist niche and identity, its close connection to iALARM has also led to a concerted effort within MCSJ to address the issue of men and HIV. They set up a ‘Men’s Forum’ initiative to coordinate a range of activities related to men and HIV, including large community meetings on GBV, Men’s Dialogues to discuss HIV and other men’s health issues, support for men’s participation in ART adherence clubs, training in leadership, gender transformation and GBV for emerging community leaders, a Men’s Health Summit, and initiatives with local football clubs to engage boys and young men in issues of HIV, health and GBV.
The MCSJ Men’s Forum has also supported a range of networking and mobilisation efforts to disseminate some of the lessons learned from the iALARM project. These activities include hosting a city-wide networking event for NGOs working with men and boys, two annual Research Indabas (large community meetings) to bring iALARM findings to the broader Gugulethu community, an initiative to distribute findings through the local ‘street committees’ (important community structures that operate at the level of the street one lives on), and sending a representative to the International AIDS Conference in July 2019 in Mexico City to share MCSJ’s work at a special “Men & HIV Forum” pre-conference meeting.
Achieving and sustaining MCSJ’s rapid growth and busy schedule of activities has often not been easy. It has some funding through UCT for part of Mandla’s time as the iALARM community engagement coordinator, and for some public events. MCSJ has also secured some funding from overseas donors like Acacia Global and interested private individuals. Its long-term funding remains uncertain, however, and insufficient for its ambitions. It has also struggled to develop a solid internal capacity and infrastructure for running the movement, notwithstanding the devoted inner circle of unpaid volunteers that make up its executive committee.
Despite these constraints, MCSJ is widely perceived within Gugulethu as a real success and as a trusted player in local issues. Many residents and local NGOs see it as a new locus for community organising around urgent health and social problems. There are frequent requests for MCSJ to open up new branches outside of Gugulethu and to partner with other groups on political campaigns. It has also been approached to provide services for larger NGOs that need to deliver programs or otherwise mobilise community members in the area (e.g. a recent request to deliver a community-based HIV testing campaign). This interest in MCSJ and its potential local impact are driven by a range of perceptions, including the idea that Gugulethu has always been bypassed by the more prominent HIV activist efforts that are rooted in other Cape Town townships like the much larger Khayelitsha, that the global decline in HIV funding has left many communities short of critical resources and expertise, and a sense that political factions within the community, city and country are leading to destructive political in-fighting that prevents important advocacy and service delivery work from getting done.
This quick sketch of the birth and growth of MCSJ necessarily leaves out many details but is designed to convey enough background information for the reader to understand the range of lessons learned described in the rest of this article. The lessons below are organised into three categories: enabling conditions, balancing acts, and overall strategies.
Enabling conditions
While MCSJ cannot of course take sole credit for the progress that has been made in promoting the emergence of a healthy—or at least healthier—public for men and HIV in Gugulethu, it has been a significant contributor to and catalyser of these developments. Below we review some of the important enabling conditions for MCSJ to play this role effectively. This is not an exhaustive list but rather represents some of the most critical and distinctive factors that have been central in enabling MCSJ’s work.
The first, and perhaps least surprising, enabling factor has been the availability of sufficient funding and human resources. MCSJ’s executive committee and other members largely work on a volunteer basis and have done a huge amount of work without remuneration. Most of its membership and executive are also unemployed and their willingness to contribute their labour despite their own unmet needs is a critical success factor (as well as a source of inevitable tension and complexity within the movement (Trafford et al., 2018)). A movement does not happen without more direct financial resources, though, at the very least for activities and for enough core human resources to sustain momentum within the movement. Financial support from iALARM, Acacia Global and others for Mandla’s time and for MCSJ’s many activities have been crucial to their success.
The flexibility of this funding is also crucial. The lack of complex funding applications and onerous financial management requirements have allowed this funding to be spent effectively and efficiently. This has allowed MCSJ to move quickly in response to events on the ground and manage access to and spending of funds without an elaborate internal infrastructure. This flexibility has allowed MCSJ to work without the kind of professionalised (and expensive) management and administration infrastructure that many NGOs are increasingly required to have in a neoliberal funding context in order to access external funding (Kamat, 2004).
The experience, networks and local knowledge of key MCSJ members have been just as critical in the movement’s success. Perhaps most important has been the long experience of Mandla and few other MCSJ members in the trenches of AIDS activism since the early 2000s. Mandla was a prominent leader within the TAC, the country’s most important political movement since the end of apartheid, from shortly after its inception. Other MCSJ members like Ncedisa Qabazi and Tantaswa Ndlelana have equally long-standing engagement and leadership in AIDS activism. This work gave them extensive training, knowledge and experience in principles of community mobilising, political activism, engaging with the media and government officials, and managing the sheer magnitude of logistical challenges in pulling off complex events like protest marches and large community meetings in very resource and capacity-constrained contexts.
While the task of mobilising for a healthy public must include a wide range of stakeholders and activities, and must acknowledge that many kinds of knowledge and expertise have a role to play, this work is also a specialist skill that requires solid training and experience. The necessary expertise does not only involve logistical, financial and other technical skills (although these are crucial) but also social, cultural and political forms of expertise that can guide strategies and tactics for the movement and ensure that the emerging healthy public is as inclusive and legitimate as possible. The capacity to understand and effectively negotiate local social dynamics and political contexts has proven over and over to be crucial to MCSJ’s success.
Importantly, and in relation to a key argument in Hinchliffe’s framework, MCSJ’s approach to the social, cultural and political complexities in Gugulethu does not frame these complexities as barriers to more rational or apolitical forms of intervention. Rather, these complexities are understood as inevitable (in any context), and as the place from which to begin understanding where people are coming from, what their needs, interests and agendas might be, and where the opportunities are for aligning interests and coordinating efforts while avoiding the conventional lines of division and conflict that structure everyday life. MCSJ’s success in this approach is evident in the frequent participation in its events of NGOs and community structures that are aligned to, for example, conflicting political parties and that rarely work together. A ‘non-aligned’ movement like MCSJ can never fully avoid accusations that it might represent one group’s or the other’s interests—whether these different groups are political parties or genders or ethnicities—but MCSJ had proven quite adept at navigating these tensions. The insight and capacity to do so should be understood as a critical form of expertise that develops over long experience in this kind of work.
Finally, MCSJ’s mobilisation of diverse forms of health information in its work to promote a healthy public has been crucial in guiding its strategy and also in meeting a frequently expressed need on the part of community members and organisations for more information about the health and social problems they face. Some of this information has come from iALARM and other academic partners in the form of epidemiological profiles, local census data, health systems and policy information, and the findings from qualitative research conducted in Gugulethu, as well as synthesised from the broader literature. This information has been distributed in a wide array of forms and fora, including iALARM Task Team meetings, written summaries and reports, pamphlets, video documentaries, and in large community meetings like the Annual Research Indabas (see https://ialarm.org.za for some examples). The distribution of this information has consistently been met with enthusiastic engagement on the part of local residents who seem eager to not only access and internalise this knowledge, but also challenge, reflect on, and then make active use of it, often as part of the ‘way forward’ section that ends nearly every community meeting.
MCSJ has also been active in producing their own forms of information as part of its work. Myrna van Pinxteren’s Ph.D. work on MCSJ contains numerous examples of the creative ways in which MCSJ produced their own bodies of evidence when academic knowledge was unavailable or inaccessible, and/or when state-produced knowledge conflicted with their understanding of what was happening on the ground. A good example of this was the qualitative and quantitative data MCSJ activists collected on the failure of dental services at the NY3 clinic to meet community need. MCSJ members spent several early mornings collecting quantitative data on the number of people queueing for the dental service as well as the numbers turned away each day due to capacity constraints. They also collected names, addresses and ID numbers of those waiting, to ensure MCSJ could not be accused of inventing patients. At the same time, they collected testimonies from many of the waiting people about service delivery failures and brought a notebook filled with these testimonies to meetings with sub-district management.
At one of these meetings with health staff and managers, City officials argued back that their service was in fact more than exceeding targets set by the City and was even serving patients from outside Gugulethu. Managers and staff were largely unaware of the volume of patients being turned away, however, and it became clear that the City’s definition of ‘appropriate service delivery’ was based on annually set targets, and on what an appropriate load would be for the existing staff (who were indeed performing admirably under difficult conditions). MCSJ’s definition was instead based on the existing and unmet need in the community. In this case, they did not have conflicting numbers per se, but conflicting approaches to how to define and assess unmet needs. This engagement, rooted in discussion of both the human costs of lack of access to healthcare as well as the differing ways of quantifying this unmet need, resulted in the City adding capacity to the dental clinic and was another important, early success for MCSJ.
Balancing acts on the road to engaged healthy publics
Funding, expertise and knowledge have been important enabling conditions for MCSJ in its work to foster a healthy public around men and HIV. Just as important have been a range of ‘balancing acts’, as one member described it, that MCSJ has had to negotiate as it pursues this work. We review here three key areas in which MCSJ has had to balance competing agendas, priorities, interests and politics.
The first balance MCSJ has had to strike is in its definition of the conceptual and spatial boundaries of its work. Observers, and even some MCSJ members, have expressed confusion and uncertainty around what MCSJ’s focus is and where it works. This ambiguity grows primarily out of the organisation’s flexible and responsive approach to engaging with local health needs and its refusal to define itself in a more conventional and limiting fashion (e.g. as an HIV or a gender movement per se). This ambiguity is also a product of a vacuum in community-based political leadership in many Cape Town communities and the widespread desire for effective and legitimate actors to step into the gap.
MCSJ’s continued focus on men and HIV—as a critical but not defining thread of its work—is partly the result of its close links to iALARM and partly an expression of an independent consensus among its members, and much of the broader Gugulethu community, that ‘men are a problem’ that needs attention. The creation of the Men’s Forum within MCSJ structures was one way to strike this balance, ensuring a consistent focus on men and HIV while leaving the broader organisation to be responsive to a variety of emergent needs. This does not resolve all of the tensions, however, since the iALARM and NRF funding is earmarked for work with men and HIV, and many of the partner organisations in MCSJ have more traditionally defined and narrower scopes of work (such as parenting skills or GBV). This tension also emerged during planning for the second Annual Research Indaba where the decision was to identify men and HIV as a broad focus of the event while also expanding the range of presentations to include ones on fatherhood, pregnancy and HIV, and livelihood strategies for young families.
This kind of questioning of the scope and objectives of work to build healthy publics may be to some extent unavoidable. The social determinants of health are all deeply inter-connected. Any holistic and responsive approach to addressing health needs that looks upstream and considers social and structural drivers of ill health will inevitably have to deal with this inter-connectedness. This will likely prompt questions like those heard in community meetings and debates such as, ‘why aren’t we focusing on poverty or jobs or housing instead of just HIV?’, or ‘why are we focusing only on men, when women and children are also affected by HIV’?
MCSJ has also had to strike balances around the geographic reach of its work and the nature of its engagement in the community. Almost as soon as it was established, MCSJ started receiving requests to expand its operations and open up branches in surrounding townships. Some members have been enthusiastic about growing the movement, and MCSJ has sometimes responded to these requests in order to address these other needs and expand its network and visibility. It is not clear, however, that this growth has always been strategic or sustainable. When hosting a march, it is very useful to be able to call on the numerous, experienced comrades from Khayelitsha to raise the numbers on the street but MCSJ often struggles to maintain the regular functioning of its own core executive committee and local branches, much less these farther flung branches. The impulse to respond to needs and opportunities outside of Gugulethu sits in constant tension, therefore, with the fact that MCSJ, for the time being at least, has quite limited capacity, is rooted in Gugulethu, and indeed relies on the skills and resources of a few key members to keep it running.
There are similar balances to be struck when considering requests to play a more service delivery—as opposed to advocacy and oversight—role for outside NGOs or government departments that may value MCSJ for its local networks of staff and community relationships. This was the case when MCSJ was approached by a large South African NGO to deliver HIV testing in Gugulethu. There was considerable internal debate within the executive about whether on the one hand, this request took MCSJ too far outside its activist role and identity, and on the other hand, whether a struggling new movement full of unemployed volunteers could really afford to turn down 3 months of paid work for many of its members. They ended up taking the work but strategized throughout about how to maintain an activist and human rights-oriented posture as an organisation.
Again, these are likely to be common dilemmas confronting any effort to constitute a new healthy public. These efforts must continually consider what the boundaries of this public are (or should be), and how to avoid the pitfalls of co-optation by both the state and non-profit sectors as service providers and facilitators of (shallow) ‘consultation’.
Second, MCSJ has had to balance a wide range of competing institutional and political identities, interests, agendas, and expertises. We have mentioned the presence of political factions with Gugulethu and the importance of MCSJ’s careful efforts to navigate these. We have also described the inclusive and supportive stance they try to take in their engagements with the health system. This approach requires another delicate balance between wanting to support the health system (and especially its most vulnerable and least powerful members who actually provide the services) while also holding it accountable for delivering quality services that meet the community’s needs.
There are also sometimes challenging balances to manage between academic and activist roles and expertises in the organisation. When Mandla was being interviewed for the iALARM project position, he made a point to say, ‘Please remember, I am an activist, not an academic’. He expressed a sincere desire to work with UCT to help bring the value of academic knowledge to his community. But he was reminding the staff at UCT that he was an activist at heart, and would think and act as such. UCT staff members have on many occasions made analogous declarations, expressing a real commitment to the political principles and objectives of MCSJ but also clarifying that their distinctive contribution and expertise is not as activists but as knowledge producers. Whatever degree of overlap, ambiguity and boundary-work there may be to disrupt this clean distinction, it has nonetheless remained an important and useful distinction within MCSJ. It brings with it inevitable tensions, but ones that can be productively managed in the right context.
MCSJ has also had to think about how to negotiate tensions and disconnects at home, among a highly fragmented and NGO-ised (Sheppard, 2009) landscape of civil society organisations in Gugulethu. Whatever the particular commitments and interests of individual NGO staff members might be, they are all bound up in a political economy of NGO-driven community engagement that is characterised by neoliberal forms of mission definition, funding competition, and financial accountability. Many activities and programmes are siloed off from other organisations and sectors, and are shaped by a focus on narrow outcome indicators, heavy reporting requirements, precarious funding, and short funding cycles. None of these problems are new in South Africa, or indeed much of the global South (Hearn, 1998). They do represent, however, a considerable challenge to the project of fostering a healthy public that is able to engage cooperatively across sectors and institutional identities, and work in the longer-term towards more durable solutions.
Finally, and especially in relation to its work on men and HIV, MCSJ has had to balance ‘gender-sensitive’ and ‘gender-transformative’ approaches (Barker et al., 2010) to the question of men, and gender more broadly. On the one hand, most MCSJ members support what would be understood as a conventional progressive and feminist approach to gender equity and the need for transformation in the underlying gender norms and practices in Gugulethu (and South Africa more generally). The critique of patriarchy, in the abstract at least, is widely accepted and there is little in MCSJ’s work or its member’s attitudes that suggest the kind of regressive politics of ‘men’s rights’ organisations in the US and elsewhere (Messner, 2016). On the other hand, members’ attitudes about exactly what this change should look like, how it should be brought about, and how quickly this should (and can) happen vary considerably. This reflects, unsurprisingly, a broader community sentiment that readily identifies men as a ‘problem’ but as often as not, recommends a return to traditions of male power and authority as the solution to this problem.
MCSJ members express a desire to challenge traditionalist defences of men’s gendered power but they are also sensitive to the fact that this desire is not always widely shared in Gugulethu and that conversations need to ‘meet people where they are’. Importantly, however, they typically do not frame these intended changes as ‘cultural’ changes or simplistically assign gender beliefs to ‘Xhosa culture’. This link between Xhosa culture and patriarchal gender beliefs is often articulated by both outside observers as well as internal, traditionalist defenders of male power in Xhosa-speaking communities. MCSJ members recognise and speak about the existence and persistence of patriarchal beliefs and practices in the places where they live, but they almost always do so in a way that avoids reified notions of local or ‘African’ culture, and that does not see culture as something to be overcome.
Strategies for engaging healthy publics
This last section on lessons learned surveys some of the broader strategies that have guided MCSJ’s work in fostering a health public for men and HIV. The first strategy involves the ways in which MCSJ engages with and includes the various sub-groups and communities within Gugulethu. As a community-based activist organisation, MCSJ works to include marginalised voices and groups in its work in ways that are not merely and thinly consultative or consumerist in orientation (Hinchliffe et al., 2018, p. 7). This is not difficult given MCSJ’s rootedness in Gugulethu and its ideological commitments. More challenging, however, has been its work to craft a mode of engagement that does not invent or reinforce siloed sub-group identities and agendas. MCSJ has worked instead to provide various groups in Gugulethu a non-threatening space in which to explore how their own distinct interests and agendas—e.g. older people, disability, cancer, food insecurity, gender—might be understood within a broader political economic framework. This allows a wide variety of small organisations and sub-groups, who typically experience engagement outside their closed networks as full of competition for attention, resources and legitimacy, to come together and feel like they are part of a larger and shared project. Even if MCSJ cannot undertake campaigns to address all of the needs in Gugulethu, they have developed a political language and method for engagement that makes people and groups from a wide array of sectors feel like participating in MCSJ is part of something bigger that they could have an interest in supporting.
Building an inclusive and broad-minded space for engaging diverse local stakeholders has been important for the internal coherence of the movement. MCSJ has also worked in creative ways to engage with the conventional antagonists of activism, in this case, the state. Many of its strategies for engaging the state are borrowed from the recent experience of AIDS activism (and many of these strategies are, in turn, borrowed from apartheid activist methodologies (Mbali, 2013)). One such strategy involves mobilising the political support of academics and academic institutions as well as the power of knowledge produced in the academy. Just as TAC enlisted prominent academics and made very effective use of technical knowledge in its legal, media and community-based activism (Colvin, 2014), MCSJ has also mobilised its ties to academics, and the specialist forms of knowledge they can provide, to bring legitimacy, attention and support to its campaigns.
In a similar fashion, MCSJ often works closely, though often quietly, with key allies in the public health and education services in Gugulethu, including doctors and nurses, higher-level managers and school headmasters. This too is a strategy that was frequently deployed by TAC and is designed to leverage the internal support offered by individual allies in the state’s employ, while also helping to reinforce the idea that activists are not attacking those on the frontline of service provisions but are rather trying to put pressure on the broader apparatus of the state to better fulfil its obligations. In several cases, facility managers or other staff have grown frustrated raising resources or capacity problems with their own line managers. They have asked MCSJ if it could bring some pressure to bear on the facility in a more public fashion and thereby provide these internal allies with some additional leverage to improve their services.
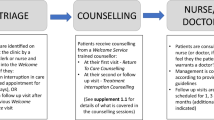
In another case, doctors and nurses within the local ER had grown frustrated with community members’ lack of understanding of the ER triage system, a gap that would lead to loud and sometimes violent conflicts within the hospital about who should be seen first (Pinxteren, 2020). The ER staff asked MCSJ to broker a meeting with community members to better explain the triage system and ask them to spread the word about this system. ER staff also shared with community members information about their staffing shortages and workloads that, while not confidential, are not usually shared with members of the public. This helped community members better understand the pressure healthcare workers laboured under and also gave them valuable information to bring to their ongoing advocacy with the state for better services. This kind of creative and two-sided engagement across conflict between community and state services is rare and is an indication of the valuable trust MCSJ has been able to garner among both groups.
Finally, we would like to point to a few research-related strategies that have been important in MCSJ’s work. The first is an effort to institutionalise some key elements of a longer-term research cycle. The reality is that, like most research projects, the funded research work coming from DSBS at UCT is likely to continue to be short-term and dependent on funder agendas. The Division has committed, however, to continue hosting its Annual Research Indaba in Gugulethu as long as funding allows. These are large events—much larger than conventional research dissemination activities—and have been attended by several hundred to more than a thousand people. Their cost is relatively small, though, especially in relation to the scale of many public health research projects. Even if we have to reduce the size of this annual meeting, we have been told that committing to a regular cycle of feedback marks a critical step in the relationship between the community and the university. We have also committed to continuing the regular iALARM Task Team meetings even when formal funding for these ends in 2020. Again, these relatively small commitments in terms of time and money appear to have an outsized impact on how community members in Gugulethu feel about their relationships with researchers and their ability to ask for, engage with, and make use of health research in their own efforts to build a healthy public.
A related strategy by UCT has been efforts to link its ongoing stream of incoming Masters in Public Health students to research needs that have been identified by MCSJ and other community members. We have provided some short-term support for MCSJ staff to serve as research assistants for these students and take more of a lead in helping students to shape locally relevant research projects. We are also working on developing short courses for MCSJ and other NGO staff who want to build their own capacity for both engaging with and using academic research as well as producing their own research within their organisations. These are all efforts to sustain an ongoing research-related engagement with MCSJ without relying on more conventional, large sources of research funding for ‘community engagement’.
Conclusion: where to from here for MCSJ and the problem of men and HIV?
In the space of a few short years, and with relatively little funding and infrastructure, MCSJ has enjoyed some significant successes in its efforts to build a healthy public around men and HIV, as well as around a broader range of health and social concerns. It has done this by working outside of conventional public health approaches that see communities as passive recipients—sometimes ‘complicated’ by culture and politics—of research projects and technical interventions to improve population health.
MCSJ has also challenged some of the conventional forms of progressive public health activism in South Africa by eschewing narrow problem-based approaches and identities (refusing to be identified as, for example, ‘AIDS activists’ or ‘disability activists’) as well as taking a tight focus on locally expressed needs and locally situated responses (and avoiding too many long asides on the evils on neoliberalism and the corruption of national political leadership). One of Mandla Majola’s guiding ideas in the early days of MCSJ was to shift his previously close engagement with prominent national-level health activists and progressive health NGOs in the country and instead ‘just focus on Gugulethu’ and try to achieve ‘just one small thing’ at a time. If we can get that one thing done, he said, then we can move on to the next problem or perhaps the next community.
This approach was in many ways quite different from the mindset and strategies of the TAC and the People’s Health Movement, both high-profile activist groups in South Africa. This shift in perspective did not mean Mandla was disavowing the importance of working for large-scale structural change or was unaware of the dangers of globally dominant ideas and practices of neoliberal political economics. Rather, he has emphasising something about the need for a complementary focus on the distinctive and difficult task of building healthy publics at a more local level, where the link between community members, activists, academics and other stakeholders can be closer, more sustained and more substantive.
Despite MCSJ’s success in this area, its work remains fragile. Not being tied to conventional institutions and mainstream sources of funding is both its greatest strength as well as the source of its greatest vulnerability. The funding for iALARM ends in 2020 and may or may not be replaced with a similar research project based at UCT. MCSJ also currently depends quite heavily on the experience and expertise of Mandla and a small group of other leaders who bring a unique skillset that is not easily or quickly transferred to new activists. And as with all social movements, there are ongoing internal and external political dilemmas it will have to navigate.
MCSJ, along with the DSBS at UCT, have committed to continuing the Research Indabas and Task Team meetings as long as they are able. And we are hoping to leverage the continuing ‘problematisation’ of men and HIV in global public health discourse to raise money for ongoing research and activist initiatives. Our longer-term research agenda includes a series of theory-generating case studies of strategies for mobilising individuals, the health services, and communities to build healthy publics that better support men and women living with HIV. This is in turn part of our ongoing effort to extend conventional public health approaches that emphasise knowledge about ‘what works’ by adding crucial complementary knowledge about how it works, for whom it works and for how long (Colvin, 2019; Krieger, 2011).
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Auld AF, Shiraishi RW, Mbofana F, Couto A, Fetogang EB, El-Halabi S et al. (2015) Lower levels of antiretroviral therapy enrollment among men with HIV compared with women—12 Countries, 2002–2013. Morb Mortal Wkly Rep 64(46):1281–1286. https://doi.org/10.15585/mmwr.mm6446a2
Barker G, Ricardo C, Nascimento M, Olukoya A, Santos C (2010) Questioning gender norms with men to improve health outcomes: evidence of impact. Glob Public Health 5(5):539–553. https://doi.org/10.1080/17441690902942464
Colvin CJ (2014) Evidence and AIDS activism: HIV scale-up and the contemporary politics of knowledge in global public health. Glob Public Health 9(1–2):57–72. https://doi.org/10.1080/17441692.2014.881519
Colvin CJ (2019) Strategies for engaging men in HIV services. Lancet HIV 6(3):e191–e200. https://doi.org/10.1016/S2352-3018(19)30032-3
Colvin CJ, Pinxteren Mv, Schmidt B-M, Cornell M, Leon NH, Lurie M et al. (2018) Health Information as a catalyst for community health system engagement. South Afr Health Rev 2018:135–139
Cornell M (2013) Gender inequality: Bad for men’s health. South Afr J HIV Med 14(1):12–14. https://doi.org/10.7196/SAJHIVMED.894
Cornell M, Cox V, Wilkinson L (2015) Public health blindness towards men in HIV programmes in Africa. Trop Med Int Health 20(12):1634–1635. https://doi.org/10.1111/tmi.12593
Cornell M, Johnson LF, Wood R, Tanser F, Fox MP, Prozesky H et al. (2017) Twelve-year mortality in adults initiating antiretroviral therapy in South Africa. J Int AIDS Soc 20(1):21902. https://doi.org/10.7448/IAS.20.1.21902
Hearn J (1998) The ‘NGO-isation’ of Kenyan society: USAID & the restructuring of health care. Rev Afr Political Econ 75:89–100
Higgins JA, Hoffman S, Dworkin SL (2010) Rethinking gender, heterosexual men, and women’s vulnerability to HIV/AIDS (Review). Am J Public Health 100(3):435–445. https://doi.org/10.2105/AJPH.2009.159723
Hinchliffe S, Jackson MA, Wyatt K, Barlow AE, Barreto M, Clare L et al. (2018) Healthy publics: enabling cultures and environments for health. Palgrave Commun 4:57. https://doi.org/10.1057/s41599-018-0113-9
Kamat S (2004) The privatization of public interest: theorizing NGO discourse in a Neoliberal Era. Rev Int Political Econ 11(1):155–176. http://www.jstor.org/stable/4177492
Krieger N (2011) Epidemiology and the people’s health: theory and context. Oxford University Press, New York
Lurie MN, Kirwa K, Callaway J, Cornell M, Boulle A, Bengtson AM, et al. (2019) Quantifying the HIV treatment cascade in a South African health sub-district by gender: retrospective cohort study. Trop Med Int Health. https://doi.org/10.1111/tmi.13334
Mbali M (2013) South African AIDS activism and global health politics. Palgrave Macmillan, Hampshire, Houndmills, Basingstoke
MenStar Coalition (2018) Global partners pledge over $1.2 billion to launch the MenStar Coalition. MenStar Coalition. http://www.menstarcoalition.org/menstar.pdf
Messner MA (2016) Forks in the road of men’s gender politics: men’s rights vs feminist allies. Int J Crime Justice Soc Democr 5(2):6–20
Pinxteren, Mv (2020) Tracing ‘paper’, discovering people: three ethnographic case studies exploring the use of health information to improve health services in Gugulethu. University of Cape Town
Sheppard ES (2009) A world of difference: encountering and contesting development. Guilford Press, New York
Stats SA (2011) City of Cape Town census data. Statistics South Africa, S. SA. Pretoria, South Africa
Trafford Z, Swartz A, Colvin CJ (2018) “Contract to Volunteer”: South African community health worker mobilization for better labor protection. New Solut 27(4):648–666. https://doi.org/10.1177/1048291117739529
Tsai AC, Siedner MJ (2015) The missing men: HIV treatment scale-up and life expectancy in Sub-Saharan Africa. PLoS Med 12(11):e1001906. https://doi.org/10.1371/journal.pmed.1001906
UNAIDS (2017) Blind Spot: reaching out to men and boys. UNAIDS, Geneva. www.unaids.org/sites/default/files/media_asset/blind_spot_en.pdf
Acknowledgements
This work was supported by grants from the National Institute of Mental Health (NIMH) and the South African Medical Research Council (#R01MH106600), from the Fogarty International Center (FIC) and the National Institute of Mental Health (NIMH) (#D43TW011308) and from the National Research Foundation of South Africa (grant #: 118533). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the South African Medical Research Council or the National Research Foundation. We are also very grateful for our ongoing engagements with the members of the Movement for Change and Social Justice in Gugulethu, Cape Town.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Colvin, C.J., van Pinxteren, M., Majola, M. et al. Fostering a healthy public for men and HIV: a case study of the Movement for Change and Social Justice (MCSJ). Palgrave Commun 6, 25 (2020). https://doi.org/10.1057/s41599-020-0402-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-020-0402-y
